
Abstract
Purpose
To document the range and the most common strategies for the management of the parturient with inadvertent durai puncture (DP) during labour epidural analgesia.
Methods
A confidential survey form was mailed to 46 academic units in Canada and USA. The responses were compiled into Canadian, US and joint North American databases.
Results
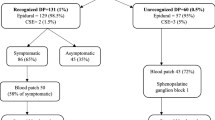
Thirty-six centres (78%) responded, representing 137,250 annual deliveries. The reported incidence of DP was 0.04–6%. The most common initial response to DP was re-siting the catheter at another level, Most centres made little change in routine practice regarding epidural top-ups and infusion rates after DP. Unrestricted mobilisation was advocated by 86% of centres following delivery; enhanced oral hydration was encouraged by 61%. Prophylactic epidural blood patch (PEBP) was recommended by 37% of centres, with twice as many US as Canadian centres doing so. In the presence of PDPH, EBP was offered most commonly at or within 24 hr of diagnosis. Complications were common after EBP: 86% of centres reported patch failures; 44% reported persistent headache after ≥2 EBP. Despite this, centres remained optimistic about EBP success, quoting cure rates >90% in 58% of centres.
Conclusion
There is little difference between the practices reported by Canadian or US centres. The expressed optimism regarding the efficacy of EBP is not supported by the evidence available and may be unwarranted. More research is needed to define the issue better.
Résumé
Objectif
Documenter l’étendue du problème et les stratégies les plus utilisées pour traiter la parturiente avec ponction accidentelle de la dure-mère (PDM) durant l’analgésie pour le travail.
Méthodes
Une enquête confidentielle a été adressée par la poste à 46 départements académiques au Canada et aux États-Unis. Les réponses ont été compilées dans les bases de données canadienne, américaine et nordaméricaine conjointe.
Résultats
Trente-six centres (78%) ont répondu, ce qui représentait 137,250 accouchements. Lincidence rapportée de PDM était de 0,04–6%. La réaction initiale la plus fréquente à une PDM était de reprendre la technique à un autre niveau. La plupart des centres ne modifiaient pas leur routine concernant les vitesse d’infusion et les bolus après PDM. La mobilisation à volonté à la suite de l’accouchement était prônée par 86% des centres; 61 % encourageaient une hydratation orale accrue. Le pansement de sang épidural (PSE) prophylactique était recommandé par 37% des centres, et ce deux fois plus souvent aux USA qu’au Canada. En présence de céphalée post-ponction de la dure-mère (CPPDM), le PSE était offert le plus souvent au moment du diagnostic ou dans les 24 heures subséquentes. Les complications sont fréquentes après PSE : 86% des centres rapportent des échecs; 44% rapportent des céphalées persistantes après ≥2PSE. Malgré ceci, les centres demeurent optimistes quant au succès du PSE, 58% des centres rapportent des taux de succès de >90%.
Conclusion
Il y a peu de différence entre la pratique au Canada et aux États-Unis. Loptimisme démontré quant à l’efficacité du PSE n’est pas corroboré par les données disponibles et est peut-être injustifié. Des recherches additionnelles pour quantifier ce problème sont nécessaires.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Okell RW, Sprigge JS. Unintentional durai puncture. A survey of recognition and management. Anaesthesia 1987; 42: 1110–3.
Stride PC, Cooper GM. Durai taps revisited. A 20-year survey from Birmingham Maternity Hospital. Anaesthesia 1993; 48: 247–55.
Suzuki N, Koganemaru M, Onizuka S, Takasaki M. Durai puncture with a 26-gauge spinal needle affects spread of epidural anesthesia. Anesth Analg 1996; 82: 1040–2.
Leach A, Smith GB. Subarachnoid spread of epidural local anaesthetic following durai puncture. Anaesthesia 1988; 43: 67–4.
Wagner DL. Total spinal anesthesia during cesarean section hours after previous unintentional durai puncture. Anesthesiology 1994; 81: 260–1.
Carbaat PAT, van Crevel H. Lumbar puncture headache: controlled study on the preventive effect of 24 hours’ bed rest. Lancet 1981; 2: 1133–5.
Cook PT, Davies MJ, Beavis RE. Bed rest and postlumbar puncture headache. The effectiveness of 24 hours’ recumbency in reducing the incidence of postlumbar puncture headache. Anaesthesia 1989; 44: 389–91.
Jones RJ. The role of recumbency in the prevention and treatment of postspinal headache. Anesth Analg 1974; 53: 788–96.
Costigan SN, Sprigge JS. Durai puncture: the patients’ perspective. A patient survey of cases at a DGH maternity unit 1983–93. Acta Anaesthesiol Scand 1996; 40: 710–4.
Dieterich M, Brandt T. Incidence of post-lumbar puncture headache is independent of daily fluid intake. Eur Arch Psychiatry Clin Neurolsci 1988; 237: 194–6.
Sechzer PH, Abel L. Post-spinal anesthesia headache treated with caffeine. Evaluation with the demand method. Part 1. Curr Ther Res 1978; 24: 307–12.
Jarvis AP, Greenawalt JW, Tagraeus L. Intravenous caffeine for postdural puncture headache (Letter). Anesth Analg 1986; 65: 316.
Camann WR, Murray RS, Mushlin PS, Lambert DH. Effects of oral caffeine on postdural puncture headache. A double-blind, placebo-controlled trial. Anesth Analg 1990; 70: 181–4.
Sajjad T, Ryan TDR. Current management of inadvertent durai taps occurring during the siting of epidurals for pain relief in labour. A survey of maternity units in the United Kingdom. Anaesthesia 1995; 50: 156–61.
Loeser EA, Hill GE, Bennett GM, Sederberg JH. Time vs success rate for epidural blood patch. Anesthesiology 1978; 49: 147–8.
Palahniuk RJ, Camming M. Prophylactic blood patch does not prevent post lumbar puncture headache. Can Anaesth Soc J 1979; 26: 132–3.
Quaynor H, Corbey M. Extradural blood patch —why delay? Br J Anaesth 1985; 57: 538–40.
Ackerman WE, Colchugh GW. Prophylactic epidural blood patch: the controversy continues (Letter). Anesth Analg 1987; 66: 913.
Colonna-Romano P, Shapiro BE. Unintentional durai puncture and prophylactic epidural blood patch in obstetrics. Anesth Analg 1989; 69: 522–3.
Trivedi NS, Eddi D, Shevde K. Headache prevention following accidental durai puncture in obstetric patients. J Clin Anesth 1993; 5: 42–5.
Bart AJ, Wheeler AS. Comparison of epidural saline placement and epidural blood placement in the treatment of post-lumbar-puncture headache. Anesthesiology 1978; 48: 221–3.
Thomas DI, Suresh MS, Stride PC, Wilkey AD. Prophylaxis of durai headache-epidural saline bolus versus infusion. Anesth Analg 1992; 74: S319.
Abvuleish E, de la Vega S, Blendinger I, Tio T-O. Long-term follow-up of epidural blood patch. Anesth Analg 1975; 54: 459–63.
Yaivainen T, Fitkänen M, Tuominen M, Rosenberg PH. Efficacy of epidural blood patch for postdural puncture headache. Acta Anaesthesiol Scand 1993; 37: 702–5.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Berger, C.W., Crosby, E.T. & Grodecki, W. North American survey of the management of durai puncture occurring during labour epidural analgesia. Can J Anaesth 45, 110–114 (1998). https://doi.org/10.1007/BF03013247
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03013247