
Abstract
Purpose
To compare two airway management techniques, face mask (FM) with oropharyngeal airway and laryngeal mask airway (LMA), with respect to the effectiveness of positive pressure ventilation and airway maintenance.
Methods
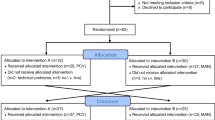
After induction of anaesthesia, two airway management techniques (FM or LMA) and three peak pressures (20, 25 and 30 cm H2O) were randomly applied during controlled ventilation in 60 patients. Data collected included inspiratory and expiratory volumes and presence of gastro-oesophageal insufflation. Leak was calculated by subtracting the expiratory from the inspiratory volume, expressed as a fraction of the inspiratory volume.
Results
Expiratory volumes (mean ± SD) at 20, 25 and 30 cm H2O for LMA ventilation were 893 ± 260, 986 ± 276 and 1006 ± 262 respectively, and for FM ventilation 964 ± 264, 1100 ± 268 and 1116 ± 261. Leak fractions at 20, 25 and 30 cm H2O for LMA ventilation were 0.21 ± 0.15, 0.24 ± 0.18 and 0.26 ± 0.18 respectively, and for FM ventilation 0.14 ± 0.09, 0.14 ± 0.09 and 0.12 ± 0.08. The frequency of gastro-oesophageal insufflation was 1.6%, 5% and 5% for the LMA and 5%, 15% and 26.6% for the FM for ventilation pressures of 20, 25 and 30 cm H2O respectively which was greater with LMA use.
Conclusion
Ventilation was adequate in all patients using both techniques. Leak was pressure dependent and greater with LMA use. Most of the leak was vented to the atmosphere via the pharynx. Gastro-oesophageal insufflation was more frequent with ventilation using the face mask. LMA use with positive pressure ventilation would appear to be a better airway management method than the face mask.
Résumé
Objectif
Comparer deux techniques de maintien des voies aériennes, le masque facial (MF) avec canule oropharyngée et le masque laryngé (ML) quant à l’efficacité de la ventilation à pression positive et du maintien des voies aériennes.
Méthodes
Après induction de l’anesthésie, on a utilisé de façon aléatoire chez 60 patients 2 méthodes de contrôle des voies aériennes (MF ou ML) et 3 pressions de pointe (20, 25 et 30 cm H2O) durant la ventilation contrôlée. Comme données on a colligé les volumes inspiratoires et expiratoires et la présence d’insufflation gastro-oesophagienne. La fuite a été calculée en soustrayant le volume expiré du volume inspiré et a été exprimée comme une fraction du volume inspiré.
Résultats
Pour la ventilation avec ML, les volumes expirés (moyenne ± Écart type) mesurés à 20, 25 et 30 cm H2O étaient respectivement de 893 ± 260, 986 ± 276 et 1006 ± 262, alors que pour la ventilation avec MF les volumes étaient respectivement de 964 ± 264, 1100 ± 268 et 1116 ± 261. La fraction de fuite à 20, 25 et 30 cm H2O a été pour la ventilation avec ML respectivement de 0,21 ± 0,15, 0,24 ± 0,18 et 0,25 ± 1,18, alors qu’avec le MF elle atteignait 0,14 ± 0,09, 0,14 ± 0,09 et 0,12 ± 0,08. La fréquence de l’insufflation gastro-oesophagienne se situait respectivement à 1,6%, 5% et 5% pour le ML et à 5%, 15% et 26,6% pour le MF pour des pressions de ventilation de 20,25 et 30 cm H2O.
Conclusion
La ventilation a été adéquate chez tous les patients en utilisant l’une ou l’autre technique. La fuite était plus grande avec le ML, dépendait de la pression et était en grande partie évacuée dans l’atmosphère par le pharynx. Linsufflation gastro-oesophagienne était plus fréquente avec l’utilisation du MF Lutilisation du ML lors de ventilation à pression positive semble une meilleure méthode de maintien des voies aériennes que l’utilisation du masque facial.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Brodrick PM, Webster NR, Nunn JF. The laryngeal mask airway. A study of 100 patients during spontaneous breathing. Anaesthesia 1989; 44: 238–41.
Kumar CM. Laryngeal mask airway for inadequate reversal (Letter). Anaesthesia 1990; 45: 792.
Brain AIJ. Three cases of difficult intubation overcome by the laryngeal mask airway. Anaesthesia 1985; 40: 353–5.
Practice guidelines for management of the difficult airway. A report by the American Society of Anesthesiologists task force on management of the difficult airway. Anesthesiology 1993; 78: 597–602.
Maltby JR, Loken RG, Watson NC. The laryngeal mask airway: clinical appraisal in 250 patients. Can J Anaesth 1990; 37: 509–13.
Verghese C, Brimacombe JR. Survey of laryngeal mask airway usage in 11,910 patients: safety and efficacy for conventional and nonconventional usage. Anesth Analg 1996; 82: 129–33.
Fisher JA, Ananthanarayan C, Edelist G. Role of laryngeal mask in airway management (Editorial). Can J Anaesth 1992; 39: 1–3.
Benumof JL. Laryngeal mask airway. Indications and contraindications (Editorial). Anesthesiology 1992; 77: 843–6.
Pennant JH, White PF. The laryngeal mask airway. Its uses in anesthesiology. Anesthesiology 1993; 79: 144–63.
Asai T, Morris S. The laryngeal mask airway: Its features, effects and role. Can J Anaesth 1994; 41: 930–60.
Warner MA, Warner ME, Weber JG. Clinical significance of pulmonary aspiration during the perioperative period. Anesthesiology 1993; 78: 56–62.
Brain AIJ. The laryngeal mask - a new concept in airway management. Br J Anaesth 1983; 55: 801–5.
Payne J. The use of the fibreoptic laryngoscope to confirm the position of the laryngeal mask (Letter). Anaesthesia 1989; 49: 865.
John RE, Hill S, Hughes TJ. Airway protection by the laryngeal mask. A barrier to dye placed in the pharynx. Anaesthesia 1991; 46: 366–7.
Devitt JH, Wenstone R, Noel AG, O’Donnell MP. The laryngeal mask airway and positive-pressure ventilation. Anesthesiology 1994; 80: 550–5.
Griffin RM, Hatcher IS. Aspiration pneumonia and the laryngeal mask airway. Anaesthesia 1990; 45: 1039–40.
Nanji GM, Maltby JR. Vomiting and aspiration pneumonitis with the laryngeal mask airway. Can J Anaesth 1992; 39: 69–70.
Devitt JH, Brooks DA, Oakley PA, Webster PM. Mask lung ventilation by ambulance personnel: a performance assessment. Can J Anaesth 1994; 41: 111–5.
Anonymous. Guidelines for cardiopulmonary resuscitation and emergency cardiac care. Emergency Cardiac Care Committee and Sub Committees, American Heart Association. Part III: Adult advanced cardiac life support. JAMA 1992; 268: 2199–241.
Weiler N, Latorre F, Eberle B, Goedecke R, Heinrichs W. Respiratory mechanics, gastric insufflation pressure, and air leakage of the laryngeal mask airway. Anesth Analg 1997; 84: 1025–8.
Vanner RG, O’Dwyer JP, Pryle BJ, Reynolds F. Upper oesophageal sphincter pressure and the effect o4f cricoid pressure, Anaesthesia 1992; 47: 95–100.
Lawes EG, Campbell I Mercer D. Inflation pressure, gastric insufflation and rapid sequence induction. Br J Anaesth 1987; 59: 315–8.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ho-Tai, L.M., Devitt, J.H., Noel, A.G. et al. Gas leak and gastric insufflation during controlled ventilation: face maskversus laryngeal mask airway. Can J Anaesth 45, 206–211 (1998). https://doi.org/10.1007/BF03012903
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03012903