
Abstract
Purpose
To compare the hemodynamic effects of sevoflurane when used for induction and maintenance of anesthesia with a total intravenous technique in patients with known coronary artery disease (CAD).
Methods
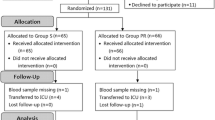
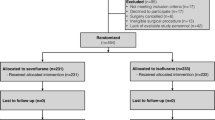
Thirty patients undergoing elective coronary artery bypass graft (CABG) were randomly allocated to receive either sevoflurane (S group, n = 15) at a minimal concentration of 4% in oxygen for induction and at 0.5-2 MAC end-tidal concentration for maintenance, or a total intravenous technique (T group, n = 15) consisting of midazolam for induction and propofol for maintenance. In both groups, anesthesia was supplemented with sufentanil and muscle relaxation with cis-atracurium. Hemodynamic measurements included systemic and pulmonary pressures, heart rate, mixed venous oxygen saturation and cardiac output at the following times: pre-induction, 7 and 25 min post-induction, chest closure, one hour after surgery and pre and post tracheal extubation.
Results
More patients in the S group (8/15) presented bradycardia in the induction period (T:2/15) (P = 0.05). During maintenance of anesthesia, treatment of hypertension was more frequent in the T group (12/15) than in the S group (6/15) (P = 0.025). All other parameters were comparable.
Conclusion
Induction of anesthesia in patients with CAD, VCRII with sevoflurane supplemented by sufentanil provided hemodynamic responses comparable with those of TIVA although bradycardia was observed more often with sevoflurane. Intraoperative control of systemic blood pressure was achieved with fewer interventions with a sevoflurane/sufentanil maintenance than with a propofol/sufentanil technique in CABG surgery.
Résumé
Objectif
Comparer les effets hémodynamiques d’une anesthésie exclusivement intraveineuse (AEI) à une technique utilisant le sévoflurane durant la chirurgie de revascularisation myocardique.
Méthode
Trente patients programmés pour une chirurgie de revascularisation myocardique (PAC) ont été répartis de façon aléatoire pour recevoir soit du sévoflurane (groupe S, n = 15) à une concentration minimale de 4% dans l’oxygène pour l’induction et à une concentration en fin d’expiration de 0.5-2 MAC pour le maintien, soit une technique TIVA (groupe T, N= 15) comprenant du midazolam pour l’induction et du propofol pour le maintien. Dans les deux groupes, l’anesthésie était complétée avec du sufentanil et du cis-atracurium. Les mesures hémodynamiques comprenaient les pressions systémiques et pulmonaires, la fréquence cardiaque, la saturation en oxygène du sang veineux mêlé et le débit cardiaque aux moments suivants: pré-induction, 7 et 25 min post-induction, à la fermeture du sternum, une heure après la fin de la chirurgie, avant et après l’extubation.
Résultats
Plus de patients du groupe S (8/15) vs groupe T (2/15) ont présenté de la bradycardie durant l’induction (P = 0,05). Durant le maintien, le traitement de l’hypertension a été plus fréquent dans le groupe T (12/15) que dans le groupe S (6/15) (P = 0,025) pour contrôler la réponse hémodynamique (± 20% valeurs de base). Tous les autres paramètres étaient comparables.
Conclusion
Pour l’induction de l’anesthésie chez des patients coronariens, l’induction VCRII avec du sévoflurane, supplémentée avec du sufentanil, offre une réponse hémodynamique comparable à une technique AEI. Cependant une incidence de bradycardie est observée plus souvent avec la première. Lors de la chirurgie, le contrôle intraopératoire de la pression sanguine est obtenue avec moins d’intervention avec la technique sevoflurane/sufentanil.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Sloan MH, Conard PF, Karsunky PK, Gross JB. Sevoflurane versus isoflurane: induction and recovery characteristics with single-breath inhaled inductions of anesthesia. Anesth Analg 1996; 82: 528–32.
Muzi M, Robinson BJ, Ebert TJ, O’Brien TJ. Induction of anesthesia and tracheal intubation with sevoflurane in adults. Anesthesiology 1996; 85: 536–43.
Goresky GV, Muir J. Inhalational induction of anaesthesia (Editorial). Can J Anaesth 1996; 43: 1085–9.
McGinley J, Briggs L, Carey M. Inhalational induction with sevoflurane (Letter). Can J Anaesth 1997; 44: 1218.
Ebert TJ, Kharasch ED, Rooke GA, Shroff A, Muzi M, and the Sevoflurane Ischemia. Study Group. Myocardial ischaemia and adverse cardiac outcomes in cardiac patients undergoing noncardiac surgery with sevoflurane and isoflurane. Anesth Analg 1997; 85: 993–9.
Yurino M, Kimura H. Efficient Inspired concentration of sevoflurane for vital capacity rapid inhalational induction (VCRII) technique. J Clin Anesth 1995; 7: 228–31.
Yurino M, Kimura H. A comparison of vital capacity breath and tidal breathing techniques for induction of anaesthesia with high sevoflurane concentrations in nitrous oxide and oxygen. Anaesthesia 1995; 50: 308–11.
Muzi M, Colinco MD, Robinson BJ, Ebert TJ. The effects of premedication on inhaled induction of anesthesia with sevoflurane. Anesth Analg 1997; 85: 1143–8.
Routsi C, Vincent J-L, Bakker J, et al. Relation between oxygen consumption and oxygen delivery in patients after cardiac surgery. Anesth Analg 1993; 77: 1104–10.
Magilligan DJ Jr, Teasdall R, Eisinminger R, Peterson E. Mixed venous oxygen saturation as a predictor of cardiac output in the postoperative cardiac surgical patient. Ann Thorac Surg 1987; 44: 260–2.
Fredman B, Nathanson MH, Smith I, Wang J, Klein K, White PF. Sevoflurane for outpatient anesthesia: a comparison with propofol. Anesth Analg 1995; 81: 823–8.
Frink EJ Jr, Malan TP, Atlas M, Dominguez LM, DiNardo JA, Brown BR Jr. Clinical comparison of sevoflurane and isoflurane in healthy patients. Anesth Analg 1992; 74: 241–5.
Ebert TJ, Muzi M, Lopatka CW. Neurocirculatory responses to sevoflurane in humans. Anesthesiology 1995; 83: 88–95.
Kersten JR, Brayer AP, Pagel PS, Tessmer JP, Warltier DC. Perfusion of ischemic myocardium during anesthesia with sevoflurane. Anesthesiology 1994; 81: 995–1004.
Ebert TJ, Harkin CP, Muzi M. Cardiovascular responses to sevoflurane: a review. Anesth Analg 1995; 81: S11–22.
Ramsay JG, DeLima LGR, Wynands JE, O’Connor JP, Ralley FE, Robbins GR. Pure opioid versus opioidvolatile anesthesia for coronary artery bypass graft surgery: a prospective, randomized,double-blind study. Anesth Analg 1994; 78: 867–75.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gravel, N.R., Searle, N.R., Taillefer, J. et al. Comparison of the hemodynamic effects of sevoflurane anesthesia induction and maintenancevs TIVA in CABG surgery. Can J Anesth 46, 240–246 (1999). https://doi.org/10.1007/BF03012603
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03012603