
Abstract
Purpose
The purpose of this study was to assess the effects of increased intra-abdominal pressure due to CO2 insufflation on the mechanical characteristics of the respiratory system and arterial blood gases during and after laparoscopic cholecystectomy.
Methods
Respiratory mechanics and arterial blood gases were examined in 12 patients undergoing laparoscopic cholecystectomy with CO2 insufflation. Respiratory mechanics were continuously monitored with in-line spirometry. In the recovery room, PaCO2 was measured in this group at 30 min and compared with PaCO2s in 23 patients who had undergone open cholecystectomy retrospectively, to evaluate the effects of insufflation on CO2 elimination.
Results
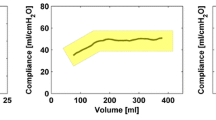
Minute ventilation was decreased by about 500 ml·min−1 during abdominal insufflation. Dynamic lung compliance decreased from 49.6 ± 4.7 to 30.7 ±2.3 (mean ± SEM) ml·cmH2O−1 with abdominal insufflation (P < 0.005), and returned to 45.1 ±3.1 after the release of pneumoperitoneum. Peak inspiratory pressure increased from 15.9 ± 0.9 to 18.9 ± 1.0 cmH2O with abdominal insufflation (P < 0.05). Arterial blood gas determinations indicated a decrease in arterial pH, with CO2 retention during insufflation and in the recovery room (P < 0.05). PaCO2 of the laparoscopic patients was higher than that of the open patients in the recovery room.
Conclusion
The results indicate that respiratory acidosis was caused during CO2 insufflation for laparoscopic cholecystectomy, that was due to (1) decreased compliance, (2) increased CO2 load and (3) insufficient ventilation. Accumulated CO2 during laparoscopic cholecystectomy increased PaCO2 level in the recovery room.
Résumé
Objectif
Evaluer les effets de l’augmentation de pression intraabdominale provoquée par l’insufflation de CO2 sur les caractéristiques du système respiratoire et des gaz du sang artériel pendant et après la cholécystectomie laparoscopique.
Méthode
La mécanique respiratoire et les gaz du sang artériels ont été étudiés chez 123 patients soumis à une cholé-cystectomie laparoscopique avec insufflation de CO2. La mécanique respiratore a été monitorée en continu par spirométrie. A la salle de réveil, la PaCO2 a été mésurée à la 30e min de l’admission et comparée rétrospectivement à la PaCO2 de 23 patients qui avaient subi une cholécystectomie ouverte, dans le but d’évaluer les effets de l’insufflation sur l’élimination du CO2.
Résultats
La ventilation minute a diminué d’environ 500 ml·min−1 pendant l’insufflation abdominale. La compliance dynamique pulmonaire diminuait de 49,6 ± 4,7 à 30,7 ± 2,3 (moyenne ± SEM) ml·cmH2O−1 avec l’insufflation (P < 0,005) et revenait à 45,1 ± 3,1 après le relâchement du pneumopéritoine. L’analyse des gaz artériels a révélé une diminution du pH artériel avec rétention de CO2 pendant l’insufflation et à la salle de réveil (P < 0,005). La PaCO2 des patients opérés sous laparoscopie était plus élevée que celle des patients opérés par chirurgie ouverte.
Conclusion
Ces résultats indiquent que l’insufflation de CO2 pour la cholécystectomie laparoscopique provoque de l’acidose respiratoire causée 1) par la baisse de la compliance, 2) l’augmentation du volume de CO2 et 3) l’insuffisance ventilatoire. L’accumulation du CO2 pendant la cholécystectomie laparoscopique augmente la PaCO2 à la salle de réveil.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Rose DK, Cohen MM, Soutter DI, Laparoscopic cholecystectomy: the anaesthetist’s point of view. Can J Anaesth 1992; 39: 809–15.
Cunningham AJ, Brull SJ, Laparoscopic cholecystectomy: anesthetic implications. Anesth Analg 1993; 76: 1120–33.
Bardoczky GI, Engelman E, Levarlet M, Simon P. Ventilatory effects of pneumoperitoneum monitored with continuous spirometry. Anaesthesia 1993; 48: 309–11.
Blobner M, Felber AR, Gögler S, et al. Zur resorption von kohlendioxid aus dem pneumoperitoneum bei laparoskopischen cholezystektomien. Anaesthesist 1993; 42: 288–94.
Bardockzy GI, d’Hollander A. Continuous monitoring of the flow-volume loops and compliance during anesthesia. J Clin Monit 1992; 8: 251–2.
Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986; February 8: 307–10.
Desmond J, Gordon RA. Ventilation in patients anaesthetized for laparoscopy. Can Anaesth Soc J 1970; 17: 378–87.
Ohlgisser M, Sorokin Y, Heifetz M. Gynecologic laparoscopy. A review article. Obstet Gynecol Surv 1985; 40: 385–96.
Wahba RWM, Béïaue F, Kleiman SJ. Cardiopulmonary function and laparoscopic cholecystectomy. Can J Anaesth 1995;42: 51–63.
Benumof JL. Anesthesia for pulmonary surgery. 1991 Annual ASA Refresher Course Lectures 1991; 225: 1–7.
Dubois F, Icard P, Berthelot G, Levard H. Coelioscopic cholecystectomy. Ann Surg 1990; 211: 60–2.
Reddick EJ, Olsen DO. Outpatient laparoscopic laser cholecystectomy. Am J Surg 1990; 160: 485–7.
Luiz T, Huber T, Hartung H-J. Veränderungen der ventilation während laparoskopischer cholezystektomie. Anaesthetist 1992; 41: 520–6.
Yamanaka MK, Sue DY. Comparison of arterial-end-tidal PCO2 difference and dead space/tidal volume ratio in respiration failure. Chest 1987; 92: 832–5.
Liu S-Y, Leighton T, Davis I, Klein S, Lippmann M, Bongard F. Prospective analysis of cardiopulmonary responses to laparoscopic cholecystectomy. J Laparoendosc Surg 1991; 1: 241–6.
Wittgen CM, Andrus CH, Fitzgerald SD, Baudendistel LJ, Dahms TE, Kaminski DL. Analysis of the hemodynamic and ventilatory effects of laparoscopic cholecystectomy. Arch Surg 1991; 126: 997–1001.
McMahon AJ, Russel IT, Baxter JN, et al. Laparoscopic versus minilaparotomy cholecystectomy: a randomized trial. Lancet 1994; 343: 135–8.
Joris I, Cigarini M, Legrand M, et al. Metabolic and respiratory changes after cholecystectomy performed via laparotomy or laparoscopy. Br J Anaesth 1992; 69: 341–5.
Erice F, Fox GS, Salib YM, Romano E, Meakins JL, Magder SA. Diaphragmatic function before and after laparoscopic cholecystectomy. Anesthesiology 1993; 79: 966–75.
Couture JG, Chartrand D, Gagner M, Bellemare F. Diaphragmatic and abdominal muscle activity after endoscopic cholecystectomy. Anesth Analg 1994; 78: 733–9.
Lew JKL, Gin T, Oh TE. Anaethetic problems during laparoscopic cholecystectomy. Anaesth Intensive Care 1992; 20: 91–2.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Iwasaka, H., Miyakawa, H., Yamamoto, H. et al. Respiratory mechanics and arterial blood gases during and after laparoscopic cholecystectomy. Can J Anaesth 43, 129–133 (1996). https://doi.org/10.1007/BF03011253
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03011253