
Abstract
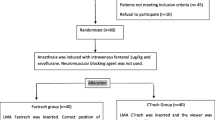
A prototype armoured laryngeal mask airway (LMA) was compared with tracheal intubation (ETT) for anaesthesia for adenotonsillectomy. Fifty-five children were randomised into the LMA group and 54 into the ETT group. During insertion of the LMA, peripheral oxyhaemoglobin desaturation (SpO2) < 94% occurred in ten patients (18.2%) and in seven patients (13%) during tracheal intubation (NS). After opening the Boyle-Davis gag, airway obstruction occurred in ten patients (18.2%) in the LMA group and in three patients (6%) in the ETT group (P = 0.07). In five patients (9%) the LMA was abandoned in favour of tracheal intubation. In all others (91%), when the need for adequate depth of anaesthesia was realized, a satisfactory airway was achieved more rapidly than with tracheal intubation (P < 0.001), and maintained throughout surgery. Manually assisted ventilation was required in all patients in the ETT group, mean duration 373 ± 385 sec, and in 26 patients (52%) in the LMA group, mean duration 134 ± 110 sec, P < 0.001. Mean end-tidal CO2 (PetCO2) was 45.5 ± 6.21 mmHg in the ETT group and 46.6 ± 6.09 in the LMA group (NS). The LMA did not limit surgical access. Heart rate, MAP and blood loss in the LMA group were 110 ± 21, 74 ± 9 mmHg and 1.92 ± 1.22 ml · kg−1 respectively, compared with 143 ± 13 (P < 0.001), 85 ± 12 mmHg (P < 0.001) and 2.62 ± 1.36 ml · kg−1 (P < 0.05) with tracheal intubation. Fibreoptic laryngoscopy at the end of surgery in 19 patients in the LMA group revealed no blood in the larynx. In the LMA group postintubation stridor and laryngospasm occurred in five and three patients respectively, compared with 14 (P < 0.05) and six patients respectively (NS) with tracheal intubation. SpO2 on admission to the PACU in the LMA group was 95.9 ± 2.21, and 93.5 ± 4.53 (P < 0.05) after tracheal intubation. Our study demonstrated that the LMA is a safe alternative to tracheal intubation for adenotonsillectomy. Control of airway reflexes by ensuring sufficient depth of anaesthesia is essential for successful use of the LMA in children.
Résumé
Un prototype de masque larngyé armé (ML) est comparé à l’intubation trachéale (TE) pendant l’anesthésie pour adéno-amygdalectomie. Cinquante-cinq enfants sont assignés au hasard au groupe ML et 54 au groupe TE. Pendant l’insertion du ML, une désaturation périphérique inférieure à 94% survient chez dix patients (18,2%) et pendant l’intubation trachéale chez sept patients (13%) (NS). Après la mise en place de l’ouvre-bouche de Boyle-Davis, l’obstruction des voies aériennes supérieures survient chez dix patients (18,2%) dans la groupe ML et trois patients dans le groupe TE (P = 0.07). Chez cinq patients (9%), on abandonne le ML en faveur de l’intubation trachéale. Chez tous les autres (91%), après l’atteinte d’un niveau d’anesthésie adéquat, un airway satisfaisant est réalisé plus rapidement qu’avec l’intubation trachéale (P < 0,001) et maintenu pendant la chirurgie. Une ventilation assistée manuellement devient nécessaire pour tous les patients du groupe TE, avec une durée moyenne de 373 ± 385 sec, et chez 26 patients (52%) du groupe ML, avec une durée moyenne de 134 ± 110 sec (P < 0,001). Le CO2 télé-expiratoire (PetCO2) est de 45,5 ± 6,21 mmHg dans le groupe TE et de 46,6 ± 6,09 mmHg dans le groupe MLA (NS). Le MLA ne limite pas l’accès chirurgical. La fréquence cardiaque, la PAM et la perte sanguine est de 110 ± 21, 74 ± 9 mmHg et 1,92 ± 1,22 ml · kg−1 respectivement pour le groupe ML, comparativement à 143 ± 13 (P < 0,001), 85 ± 12 mmHg (P < 0,001) et 2,62 ± 1,36 ml · kg−1 (P < 0,05) pour le groupe TE. Chez 19 patients du groupe ML, la fibroscopie à la fin de la chirurgie n’a pas révélé la présence de sang dans le larynx. Dans le groupe ML après l’intubation, un stridor et un laryngospasme sont apparus chez cinq et trois patients respectivement, comparativement à 14 (P < 0,05) et six patients respectivement (NS) dans le groupe TE. Notre étude montre que le ML est une alternative sécuritaire à l’intubation trachéale pour l’adéno-amygdalectomie. Pour utiliser avec succès la LM, il est essentiel de contrôler les réflexes des voies aériennes par une anesthésie suffisamment profonde.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Doughty A. Anaesthesia for adenotonsillectomy: a critical approach. Br J Anaesth 1957; 29: 407–14.
McAlpine DF, Bowering MW. Anaesthesia for tonsillectomy and adenoidectomy in children. Can Anaesth Soc J 1958; 5: 61–71.
Ribiero OV. Anesthesia for tonsillectomy and adenoidectomy in children: observations on 10,000 cases. Anesth Analg 1960; 39: 189–96.
Naunton RF. Tonsillectomy and adenoidectomy: current technique. Surg Clin North Am 1961; 41: 213–9.
Black AE, Mackersie AM. Accidental bronchial intubation with RAE tubes. Anaesthesia 1991; 46: 42–3.
Sen AK, Gupta B. Herniation of RAE tube through split Boyle Davis gag (Letter). Anaesth Intensive Care 1990; 18: 577–8.
Brain AIJ. The laryngeal mask airway — a new concept in airway management. Br J Anaesth 1983; 55: 801–5.
Brain AIJ, McGhee TD, McAteer EJ, Thomas A, Abu-Saad MAW, Bushman JA. The laryngeal mask airway: development and preliminary trials of a new type of airway. Anaesthesia 1985; 40: 356–61.
Brodrick PM, Webster NR, Nunn JF. The laryngeal mask airway: a study of 100 patients during spontaneous breathing. Anaesthesia 1989; 44: 238–41.
Maltby JR, Loken RG, Watson NC. The laryngeal mask airway: clinical appraisal in 250 patients. Can J Anaesth 1990; 37: 509–13.
Alexander CA. A modified Intavent laryngeal mask for ENT and dental anaesthesia (Letter). Anaesthesia 1990; 45: 892–3.
Williams PJ, Bailey PM. Comparison of the reinforced laryngeal mask airway and tracheal intubation for adenotonsillectomy. Br J Anaesth 1993; 70: 30–3.
Pounder DR, Blackstock D, Steward DJ. Tracheal extubation in children: halothane versus isoflurane, anaesthetized versus awake. Anesthesiology 1991; 74: 653–5.
Mason DG, Bingham RM. The laryngeal mask airway in children. Anaesthesia 1990; 45: 760–3.
Dain SL, Smith BD, Webster AC. A laptop computer based intra-operative physiological data acquisition system. Can J Anaesth 1992; 39: A31.
Motoyama EK, Cook CD. Respiratory physiology.In: Smith RM (Ed.). Anesthesia for Infants and Children. 4th ed. St. Louis: CV Mosby 1980; 38–86.
Koka BV, Jeon IS, Andre JM, MacKay I, Smith RM. Post-intubation croup in children. Anesth Analg 1977; 56: 501–5.
Olsson GI, Hallen B. Laryngospasm during anaesthesia: a computer-aided incidence study in 136,929 patients. Acta Anaesthesiol Scand 1984; 28: 567–75.
Patel RI, Hannallah RS, Norden J, Casey WF, Verghese ST. Emergence airway complications in children: a comparison of tracheal extubation in awake and deeply anesthetized patients. Anesth Analg 1991; 73: 266–70.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Webster, A.C., Morley-Forster, P.K., Dain, S. et al. Anaesthesia for adenotonsillectomy: A comparison between tracheal intubation and the armoured laryngeal mask airway. Can J Anaesth 40, 1171–1177 (1993). https://doi.org/10.1007/BF03009607
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03009607