
Abstract
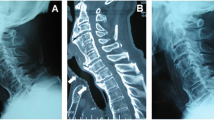
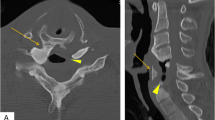
A case is reported in which anterior osteophytes on the cervical vertebra, in combination with a subglottic stenosis, resulted in distortion of the airway and led to unexpected difficulties during intubation. The osteophytes, associated with the syndrome of diffuse idiopathic skeletal hyperostosis (DISH) were centred at the midcervical level and resulted in anterior displacement of the larynx with an acute angulation of the trachea just below the larynx. This acute angulation, immediately above an unrecognized subglottic stenosis, rendered it impossible to pass all but the smallest endotracheal tube. Diffuse idiopathic skeletal hyperostosis is an ossifying diathesis leading to bone formation in spinal and extraspinal sites, paravertebral osteophyte formation and ligamentous calcification and ossification. Ossification of the anterior longitudinal ligament is common, may be discontinuous, and is often more marked in the thoracolumbar spine than elsewhere. However, isolated and predominant cervical spinal involvement may occur. Diffuse idiopathic skeletal hyperostosis occurs primarily in the elderly population and is often associated with the syndromes of osteoarthritis and ossification of the posterior longitudinal ligament (OPLL). Difficult intubation resulting from anatomical abnormalities of the cervical spine is rare. Although radiological evaluation may be useful in assessing the airway in patients deemed to be at risk for difficult intubation, it cannot be recommended for screening patient populations on a routine basis because of the cost and anticipated extremely low yield. Careful clinical evaluation of the airway before operation and having an approach to the unexpected difficult intubation are emphasized.
Résumé
Cette observation décrit une difformité des voies respiratoires causée par la présence d’ostéophytes situés en avant des vertèbres cervicales. Accompagnée d’un oedème sous-glottique, elle fut la cause de difficultés inattendues lors de l’intubation. Les ostéophytes, centraux et médiocervicaux associés au syndrome d’hyperostose squelettique diffuse idiopathique provoquèrent un déplacement antérieur du larynx à angle aigu avec la trachée,juste sous le larynx. Cette formation d’un angle, localisé en haut d’un oedème sousglottique méconnu, a rendu impossible le passage d’une canule endotrachéale du plus petit calibre. L’hyperotose squelettique idiopathique diffuse constitue une diathèse ossifiante entraînant la formation de sites osseux spinaux et extraspinaux, d’ostéophytes paravertébraux, à la calcification et à l’ossification ligamentaires. L’ossification du ligament longitudinal antérieur est fréquente, peut être interrompue et est souvent plus importante au rachis thoracolombaire. Cependant, une atteinte isolée à prédominance cervicorachidienne peut survenir. L’hyperostose idiopathique squelettique diffuse survient dans la population âgée et s’associe souvent aux syndromes ostéoarthritiques et à l’ossification du ligament longitudinal postérieur. Les difficultés d’intubation résultant d’anomalies anatomiques de la colonne cervicale sont rares. Bien que l’evaluation radiologique puisse être utile dans l’évaluation des voies respiratoires du patient comportant un risque d’intubation difficile, elle ne peut être recommandée pour le dépistage de populations de façon régulière à cause du coût et du rendement anticipé extrèmement faible. La nécessité d’une évaluation préopératoire méticuleuse des voies aériennes et une approche systématique de l’intubation difficile imprévue s’imposent.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Mallampati SR, Gatt SP, Gugino LD, et al. A clinical sign to predict difficult tracheal intubation: a prospective study. Can Anaesth Soc J 1985; 32: 429–34.
Wilson ME, Spiegelhalter D, Robertson JA, Lesser P. Predicting difficult intubation. Br J Anaesth 1988; 61: 211–6.
Gronert GA, Theye RA. Pathophysiology of hyperkalemia induced by succinylcholine. Anesthesiology 1975; 43: 89–99.
Horton WA, Fahy L, Charters P. Disposition of cervical vertebral, atlanto-axial joint, hyoid and mandible duringx- ray laryngoscopy. Br J Anaesth 1989; 63: 435–8.
Keenan MA, Stiles CM, Kaufman RL. Acquired laryngeal deviation associated with cervical spine disease in erosive polyarticular arthritis. Use of the fibreoptic bronchoscope in rheumatoid arthritis. Anesthesiology 1983; 58: 441–9.
Hayashi H, Okada K, Hamada M, Tada K, Ueno R. Etiologic factors of myelopathy. A radiographic evaluation of the aging changes in the cervical spine. Clin Orthop 1987; 214: 200–9.
Lee HC, Andree RA. Cervical spondylosis and difficult intubation. Anesth Analg 1979; 58: 434–5.
Brechner VL. Unusual problems in the management of airways. 1. flexion-extension mobility of the cervical vertebrae. Anesth Analg 1979; 47: 362–73.
Resnick D. Hyperostosis and ossification in the cervical spine. Arthritis Rheum 1984; 27: 564–9.
Forestier J, Lagier R. Ankylosing hyperostosis of the spine. Clin Orthop 1971; 74: 65–83.
Houk RW, Hendrix RW, Lee C, Lal S, Schmid FR. Cervical fracture and paraplegia complicating diffuse idiopathic skeletal hyperostosis. Arthritis Rheum 1984; 27: 472–5.
Oates JDL, MacLeod AD, Oates PD, Pearsall FJ, Howie JC, Murray GD. Comparison of two methods for predicting difficult intubation. Br J Anaesth 1991; 66: 305–9.
Frerk CM. Predicting difficult intubation. Anaesthesia 1991; 46: 1005–8.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Crosby, E.T., Grahovac, S. Diffuse idiopathic skeletal hyperostosis: an unusual cause of difficult intubation. Can J Anaesth 40, 54–58 (1993). https://doi.org/10.1007/BF03009319
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03009319