
Abstract
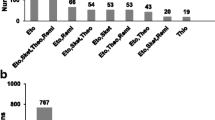
This study was designed to determine whether patients receiving chronic anticonvulsant therapy demonstrate an altered requirement for fentanyl during anaesthesia. Sixty-one patients undergoing craniotomy were studied; 20 controls (MED = 0) who had never received anticonvulsants and 41 epileptics in whom therapeutic plasma concentrations of either one (MED = 1), two (MED = 2), or three (MED = 3) different anticonvulsants were documented. During anaesthesia with 60–70 per cent N2O in O2 and 0.2 per cent isoflurane, a maintenance dose (MD) of fentanyl was administered using a continuous variable-rate IV fentanyl infusion, supplemented by intermittent 50 μg IV boluses. In order to define the minimal dosage of fentanyl required, the MD was titrated according to increases or decreases in the heart rate and/or mean arterial pressure exceeding 15 per cent of baseline ward values. A progressively higher fentanyl MD was required in the epileptic patients (MED = 1 − 4.3 ± 0.5 μg · kg− 1 · hr− 1;MED = 2 − 5.4 ± 0.6; MED = 3 − 7.6 ± 0.6) compared with the control MD (MED = 0 − 2.6 ± 0.5) (P < 0.001). These findings indicate that there appears to be a dose- effect relationship between the number of anticonvulsants received and the maintenance dose of fentanyl required during balanced anaesthesia.
Résumé
Le but de cette étude est d’observer les effets du traitement anticonvulsant de longue durée sur la dose de fentanyl requise pendant l’anesthésie. Soixante et un malades pour chirurgie intracranienne ont été etudiés de façon prospective: 20 patients controle (MED = 0) qui n’ont jamais recus d’anticonvulsant et 41 épileptiques avec des niveaux plasmatiques thérapeutiques pour un (MED = 1), deux (MED = 2) ou trois (MED = 3) anticonvulsants. La maintenance de l’anesthésie était assurée avec 70 pour cent N2O- O2, 0,2 pour cent isoflurane et une perfusion intraveineuse à niveau variable de fentanyl supplementée par des bolus intermittents de 50 μg. De manière a définir le dosage minimum de fentanyl requis (sans tenir compte du traitement anticonvulsant), la dose de maintenance de fentanyl (MD = perfusion + bolus) était augmentée ou diminuée selon les variations du rythme cardiaque et ou de la pression artérielle moyenne, pour les maintenir dans des limites n’éxcèdant pas ± 15 pour cent de leurs valeurs preop obtenues dans le service. Une augmentation progressive de la MD de fentanyl a été requise chez les patients épileptiques des differents groupes (MED = 1 − 4,3 ± 0,5 μg · kg− 1 · hr− 1; MED = 2 − 5,4 ± 0,6; MED = 3 − 7,6 ± 0,6) quand comparé au groupe contrôle (MED = 0− 2,6 ± 0,5) (P < 0.001). Aucune différence significative entre le groupe contrôle et les patients épileptiques, ne fut notée concernant les differents critères d’émergence de l’anesthésie. Ces resultats semble indiquer qu’il existe une relation dose- effet entre le nombre d’anticonvulsants recus par les malades et la dose de maintenance de fentanyl requise pendant l’anesthésie générate « balancée ».
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Ornstein E, Matteo RS, Young WL, Diaz J. Resistance to metocurine-induced neuromuscular blockade in patients receiving phenytoin. Anesthesiology 1985; 63: 294–8.
Roth S, Ebrahim ZY. Resistance to pancuronium in patients receiving carbamazepine. Anesthesiology 1987;66:691–3.
Ornstein E, Matteo RS, Schwartz AE, Silverberg PA, Young WL, Diaz J. The effect of phenytoin on the magnitude and duration of neuromuscular block following atracurium or vecuronium. Anesthesiology 1987; 67: 191–6.
Ebrahim Z, Bulkley R, Roth S. Carbamazepine therapy and neuromuscular blockade with atracurium or vecuronium. Anesth Analg 1988; 67: S55.
Modica P, Tempelhoff R. Effect of chronic anticonvulsant therapy on recovery from atracurium. Anesth Analg 1989; 68; S198.
Goldring S, Gregorie EM, Tempelhoff R. Neurosurgery.In: Rob and Smith’s Operative Surgery, 4th ed., London, Butterworths, 1989.
Stanley TH, de Lange S. The influence of patient habits on dosage requirements during high dose fentanyl anesthesia. Can Anaesth Soc J 1984; 31: 368–76.
Stanley TH, Philbin DM, Coggins CH. Fentanyl-oxygen anesthesia for coronary artery surgery: cardiovascular and antidiuretic hormone responses. Can Anaesth Soc J 1979; 26: 168–72.
Stanley TH, Webster LR. Anesthetic requirements and cardiovascular effects of fentanyl-oxygen and fentanyl-diazepam-oxygen anesthesia in man. Anesth Analg 1978; 57:411–6.
Mather LE. Clinical pharmacokinetics of fentanyl and its new derivatives. Clin Pharmacokinet 1983; 8: 422–46.
Stambaugh JE, Wainer IW, Schwartz I. The effect of phenobarbital on the metabolism of meperidine in normal volunteers. J Clin Pharmacol 1978; 18: 482–90.
Pond SM, Kretschzmer KM. Effect of phenytoin on meperidine clearance and normeperidine formation. Clin Pharmacol Ther 1981; 30: 680–6.
McClain GE, Sipes IG, Brown BR. An animal model of halothane hepatotoxicity: roles of enzyme induction and hypoxia. Anesthesiology 1979; 51: 321–6.
Luoma PV, Sotaniemi EA, Arranto AJ. Serum LDL cholesterol, the LDL/HDL cholesterol ratio and liver microsomal enzyme induction evaluated by antipyrine kinetics. Scand J Clin Lab Invest 1983; 43: 671–5.
Bird SJ, Kuhar MJ. Iontophorectic application of opiates to the locus coeruleus. Brain Res 1977; 122: 523–33.
Olpe HR, Jones RSG. The action of anticonvulsant drugs on the firing of locus coeruleus neurons: selective, activating effect of carbamazepine. Eur J Pharmacol 1983; 91: 107–10.
Aghajanian GK. Tolerance of locus coeruleus neurons to morphine and suppression of withdrawal response by clonidine. Nature 1978; 276: 86–8.
Ausems ME, Hug CC Jr,de Lange S. Variable rate infusion of alfentanil as a supplement to nitrous oxide anesthesia for general surgery. Anesth Analg 1983; 62: 982–6.
White PF. Use of continuous infusion versus intermittent bolus administration of fentanyl or ketamine during outpatient anesthesia. Anesthesiology 1983: 59: 294–300.
Ausems ME, Hug CC Jr,Stanski DR, Burm AGL. Plasma concentrations of alfentanil required to supplement nitrous oxide anesthesia for general surgery. Anesthesiology 1986; 65: 362–73.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Tempelhoff, R., Modica, P.A. & Spitznagel, E.L. Anticonvulsant therapy increases fentanyl requirements during anaesthesia for craniotomy. Can J Anaesth 37, 327–332 (1990). https://doi.org/10.1007/BF03005584
Issue Date:
DOI: https://doi.org/10.1007/BF03005584