
Abstract
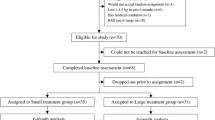
We found in an earlier study that participants in a short-term streatment program for obesity showed a good weight reduction (10.4 kg) 18 months after treatment terminated. The program included elements from cognitive therapy (CT) and psychoeducation. In the present study the efficacy of as light modification of the same treatment program (cognitive treatment group) was compared with a behavioral program that included moderate-intensity physical activity and behavioral techniques (the control treatment group) in a randomized controlled trial. The primary effect variable was weight change 18 months after the end of therapy. Both treatment programs lasted for 10 weeks (2 hr/week), and thereafter the participants were weighed periodically over an 18-month period. The participants were obese women employed outside the home. Twelve of the participants did not receive treatment after randomization. Eleven of these participants had been randomized to the cognitive program, whereas the remaining participant was randomized to the control program.The mean age for those that began the 2 programs was 48.5 years, and the mean body mass index (BMI) was 36.6. For those who completed the treatment programs and participated in the 18-month follow-up, the baseline BMI was 34.7. One participant in the cognitive treatment group (n = 16) and 6 in the control program (n = 26) dropped out during treatment. Both per-protocol and intention-to-treat analyses were performed on the data. Fifteen participants (94%) completed the cognitive program. Of these, 13 (87%) participated at the18-monthfollow-up.Their mean weight loss attreatment completion was 8.6kg(SD = 2.9) and 18 months later 5.9 kg (SD =5.4). Twenty participants (77%) completed the control program. Of these, 16 (80%) participated in the 18-month follow-up. Their mean weight lossatthe end of treatment was 0.7kg(SD=1.2), and 18 months later they showed an increase in weight of 0.3 kg (SD = 4.3) as compared with baseline weight. The weight differences between the 2 program groups were highly significant (p< .01-.001) at all posttreatment weighings. In the intention-to-treat analysis, all participants who started the cognitive treatment (n=16) or control program(n=26) were included. The last observation carried forward was used for those who dropped out from therapy or from follow-up. Eighteen months after the end of therapy, the mean weight loss was 5.5 kg (SD = 5.5) in the cognitive group, whereas the control group evidenced a weight loss of 0.6 kg (SD = 5.5). The weight change differences between the 2 groups were highly significant at all follow-up weighings (p < .001). The low drop-out rate during the treatment period demonstrates that the participants found the 2 programs acceptable. The long-term efficacy of the cognitive treatment program seems to be satisfactory. With its group format and short treatment duration, the cognitive program is attractive from a cost-effective standpoint.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Agras, W. S., Telch, C. F., Arnow, B., Eldredge, K., & Marnell, M. (1997). One-year follow-up of cognitive-behavioral therapy for obese individuals with binge eating disorder.Journal of Consulting and Clinical Psychology, 65, 343–347.
Foreyt, J. P., & Goodrick, G. K. (1993). Evidence for success of behavior modification in weight loss and control.Annals of International Medicine, 119, 698–701.
Foreyt, J. P., & Goodrick, G. K. (1994). Attributes of successful aproaches to weight loss and control.Applied and Preventive Psychology, 3, 209–215.
Foreyt, J. P., & Walker, S. C., Poston, W. S. (1998). What is the role of cognitive-behavior therapy in patient management?Obesity Research, 6, 18–22.
Goldstein, D. J. (1992). Beneficial health effects of modest weight loss.International Journal of Obesity and Related Metabolic Disorders, 16, 397–415.
Kanders, B. S., & Blackburn, G. L. (1992). Reducing primary risk factors by therapeutic weight loss. In T. A. Wadden, & T. B. VanItallie (Eds.),Treatment of seriously obese patients (pp. 213–230). New York: Guilford.
Kayman, S., Bruvold, W., & Stern, J. S. (1990). Maintenance and relapse after weight loss in women: Behavior aspects.American Journal of Clinical Nutrition, 52, 800–807.
Liao, K. L. (2000). Cognitive-behavioral approaches and weight management: An overview.Journal of the Royal Society for the Promotion of Health, 120, 27–30.
Melin, I., Karlström, B., Lappalainen, B., Mohsen, R., & Vessby, B. (2003). A programof behavior modification and nutrition counselling in the treatment of obesity: A randomised 2-y clinical trial.International Journal of Obesity, 27, 1127–1135.
Noppa, H., & Hällström, T. (1981). Weight gain in adulthood in relation to socioeconomic factors, mental illness, and personality traits: A prospective study of middle-aged women.Journal of Psychosomatic Research, 25, 83–89.
Paulsen, B. K., Lutz, R. N., McReynolds, W. T., & Kohrs, M. B. (1976). Behavior therapy for weight control: Long-term results of two programs with nutritionists and therapists.American Journal of Clinical Nutrition, 29, 880–888.
Perri, M. G., & Fuller, P. R. (1995). Success and failure in the treatment of obesity: Where do we go from here?Medicine, Exercise, Nutrition and Health, 4, 255–272.
Perri, M. G., Nezy, A. M., & Viegener, B. J. (1992).Improving the long-term management of obesity: Theory, research, and clinical guidelines. New York: Wiley.
Roberts, R. E., Delger, S., Strawbridge, W. J., & Kaplan, G. A. (2003). Prospective association between obesity and depression: Evidence from the Alameda county study.International Journal of Obesity, 27, 514–521.
Royal College of Physicians. (1998).Clinical management of overweight and obese patients (1998). London: Author.
Stahre, L. (2002).Kognitiv behandling vid övervikt och hetsätning [Cognitive treatment for obesity and binge eating]. Lund, Sweden: Studentlitteratur.
Stahre, L., & Hällström, T. (2005). A new short-term cognitive treatment program gives substantial weight reduction up to 18 months from the end of treatment: A randomized controlled trial.Journal of Eating and Weight Disorders: Studies in Anorexia Bulimia Obesity, 10, 51–58.
Stunkard, A. J., & Wadden, T. A. (1992). Psychological aspects of severe obesity.American Journal of Clinical Nutrition, 55(Suppl. 2), 524–532.
Tremblay, A., Doucet, E., Imbeault, P., Mauriege, P., Despres, J. P., & Richard, D. (1999). Metabolic fitness in active reduced-obese individals.Obesity Research, 7, 556–563.
Wadden, T. A., & Bell, S. T. (1990). Obesity. In A. S. Bellack, M. Hersen, & A. E. Kaxdin (Eds.),International handbook of behavior modification and therapy (2nd ed., p. 449). New York: Plenum.
Wadden, T. A., Berkowitz, R. I., Vogt, R. A., Steen, S. N., Stunkard, A. J., & Foster, G. D. (1997). Lifestyle modification in the pharmacologic treatment of obesity: A pilot investigation of a primary care approach.Obesity Research, 5, 218–226.
Wadden, T. A., & Stunkard, A. J. (1987). Psychopathology and obesity.Annals of the New York Academy of Sciences, 499, 55–65.
Waller, G. (1997). Drop-out and failure to engage in individual outpatient cognitive behavior therapy for bulimic disorders.International Journal of Eating Disorders, 22, 35–41.
WHO. (1997). Obesity. Preventing and managing the global epidemic. Report of WHO Consultation on Obesity, Geneva, 3–5 June 1997.
Williamson, D. A., & Perrin, L. A. (1996). Behavioral therapy for obesity.Endocrinology and Metabolism Clinics of North America, 25, 943–954.
Wing, R. R. (1992). Behavioral treatment of severe obesity.American Journal of Clinical Nutrition 55, 545–551.
Wing, R. R., & Jeffery, R. W. (1995). Effect of modest weight loss on changes in cardiovascular risk factors: Are there differences between men and women or between weight loss and maintenance?International Journal of Obesity, 19, 67–73.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Stahre, L., Tärnell, B., Håkanson, CE. et al. A randomized controlled trial of two weight-reducing short-term group treatment programs for obesity with an 18—month follow—up. Int. J. Behav. Med. 14, 48–55 (2007). https://doi.org/10.1007/BF02999227
Issue Date:
DOI: https://doi.org/10.1007/BF02999227