
Abstract
World Health Organization (WHO) recommended standard ORS solution has sodium (90 mmol/L) and glucose (111 mmol/L) almost in the ratio of 1∶1 and a total osmolarity of 311 mmol/L. There are concerns that the sodium or glucose concentration and the overall osmolarity in the formulation is not appropriate. Therefore, the efficacy of standard and reduced-osmolarity ORS solutions in young children with acute diarrhea was evaluated in a recent WHO supervised multicentre trial conducted in India (New Delhi), Brazil, Mexico and Peru. The implications of trial results are discussed.
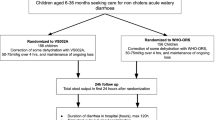
In non-cholera diarrhea, both the standard and reduced osmolarity ORS solutions were effective in achieving clinical rehydration. The stool output was 39% higher in the standard ORS solution group as compared to the reduced-osmolarity ORS solution group. The duration of diarrhea was 22% higher in the standard ORS solution group. The risk of requiring supplementary intravenous infusion was increased in children treated with standard ORS solution [relative risk 1.4 (0.9–2.4)]; this benefit was not observed in Indian patients due to high breast feading rate.
The mean sodium concentration at 24 hours after admission was lower in the reduced osmolarity ORS solution group [135 (134–136) vs 138 (136–139), p<0.01). The low osmolarity ORS deserves to be evaluated in adult cholera to determine its efficacy and any excess hyponatreamia. Meanwhile, it is reassuring that the WHO formulation was effective and its use was not associated with hypenatremia even in young children. Efforts must continue to be made to promote WHO-ORS while research to improve it further is welcome.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Schultz SG. Sodium coupled solute transport by small intestine; a status report.Am J Physiol 1977; 223: E249-E254.
Sandhu BK, Christoal FI, Brueton MJ. Optimizing oral rehydration solution composition in model systems: studies in normal mammalian small intestine.Acta Pediatr Scand 1989; Suppl 364: 17–22.
Farthing MJG. Disease-related animal models for optimizing oral rehydration solution composition.Acta Pediatr Scand 1989; Suppl 364: 23–30.
Elliot EJ. The role of human perfusion techniques in the assessment of oral rehydration solutions.Acta Pediatr Scand 1989; Suppl 364: 31–39.
Hunt JB, Thillainayagam AV, Salim AFMet al. Water and solute absorption from a new hypotonic oral rehydration solution; evaluation in human and animal perfusion models.Gut 1992; 33: 1652–1659.
El-Mougi M, El-Akkad N, Hendawi Aet al. Is low osmolarity ORS solution more efficacious than standard WHO ORS solution?J Pediatr Gastroenterol Nutr 1994; 19: 83–86.
International Study Group on Reduced-osmolarity ORS solutions. Multicentre evaluation of reduced-osmolarity oral rehydration salts solution.Lancet 1995; 345: 282–285.
Bhargava SK, Sachdev HPS, Das Gupta Bet al. Oral rehydration of neonates and young infants with dehydrating diarrhea: comparison of low and standard sodium content in oral rehydration solutions.J Pediatr Gastroenterol Nutr 1984; 3: 500–505.
World Health Organisation. Development of an improved formulation of oral rehydration salts (ORS) with anti-diarrheal and nutritional properties: a “Super ORS”. WHO document CDD/DDM/85. March 1985.
Report of a Consensus Meeting: Treatment of severe and malnutrition in refugee camps.Eur J Clin Nutr 1993; 47: 750–754.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Bahl, R., Bhandari, N. & Bhan, M.K. Reduced-Osmolarity oral rehydration salts solution multicentre trial: Implications for national policy. Indian J Pediatr 63, 473–476 (1996). https://doi.org/10.1007/BF02905721
Issue Date:
DOI: https://doi.org/10.1007/BF02905721