
Abstract
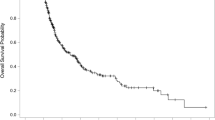
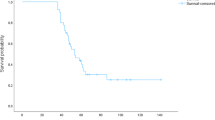
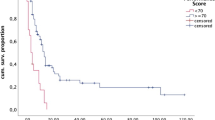
Metastatic cancer to the brain has a poor prognosis. The focus of this work was to determine the incidence of long-term (≥2 y) survival for patients with brain metastases from different primary cancers and to identify prognostic variables associated with prolonged survival. A retrospective review of 740 patients with brain metastases treated over a 20 y period identified 51 that survived 2 or more years from the time of diagnosis of the brain metastasis. Prognostic variables that were examined included age, sex, histology, tumor number and location, and treatment. In the 51 patients, 35 (69%) had single lesions and 16 (31%) had multiple tumors. For all tumor types (740 patients), the actuarial survival rate was 8.1% at 2 y, 4.8% at 3 y, and 2.4% at 5 y. At 2 y, patients with ovarian carcinoma had the highest survival rate (23.9%) and patients with small cell lung cancer (SCLC) had the lowest survival rate (1.7%). At 5 y, survival rates were 7.8% for ovarian carcinoma, 2.9% for non-SCLC, 2.3% for melanoma and renal cell carcinoma, 1.3% for breast carcinoma and there were no survivors with SCLC, gastrointestinal, bladder, unknown primary, or prostate cancer. Age, sex, histology, location for single tumors, systemic chemotherapy, and stereotactic radiosurgery did not significantly influence survival. The presence of a single lesion (P=0.001, chi-square test), surgical resection (P=0.001), and WBRT (P=0.009) were favorable prognostic variables for extended survival. Multiple bilateral metastases was a poor prognostic indicator (P=0.001). Multivariate analysis showed younger age (P<0.05), single metastasis (P<0.0001), surgical resection (P<0.0001), whole brain radiation therapy (P<0.0001), and chemotherapy (P=0.0288) were associated with prolonged survival. 29 patients (57%) died of systemic disease progression, 9 (18%) died of central nervous system progression, and the cause of death was unknown in 3 (6%). Patients with a single non-SCLC, breast, melanoma, renal cell, and ovarian carcinoma brain metastasis have the best chance for long-term survival if treated with surgical resection and WBRT.
Article PDF
Similar content being viewed by others
Avoid common mistakes on your manuscript.
References
Nussbaum ES, Djalilian HR, Cho KH, Hall WA. Brain metastases: histology, multiplicity, surgery and survival.Cancer 1996;78: 1781–1788.
Patchell RA. Metastatic brain tumors.Neurol Clin 1995;13: 915–925.
Markesbery WR, Brooks WH, Gupta GD, Young AB. Treatment for patients with cerebral metastases.Arch Neurol 1978;35: 754–756.
Patchell RAet al. A randomised trial of surgery in the treatment of single metastases to the brain.New Engl J Med 1990;322: 494–500.
Vecht CJet al. Treatment of single brain metastasis: radiotherapy alone or combined with neurosurgery?.Ann Neurol 1993;3: 583–590.
Bindal RK, Sawaya R, Leavens ME, Lee JJ. Surgical treatment of multiple brain metastases.J Neurosurg 1993;79: 210–216.
Hazuka MBet al. Multiple brain metastases are associated with poor survival in patients treated with surgery and radiotherapy.J Clin Oncol 1993;11: 369–373.
Ammirati M, Samii M, Skaf G, Sephernia A. Solitary brain metastasis 13y after removal of renal adenocarcinoma.J Neurooncol 1993;15: 87–90.
Radley MG, McDonald JV, Pilcher WH, Wilbur DC. Late solitary metastases from renal cell carcinoma: report of two cases.Surg Neurol 1993;39: 230–234.
Salvati Met al. Solitary cerebral metastasis from lung cancer with very long survival: report of two cases and review of the literature.Surg Neurol 1991;36: 458–461.
Sarma DP, Weilbaecher TG. Long-term survival after brain metastasis from lung cancer.Cancer 1986;58: 1366–1370.
Chang DBet al. Late survival of non-small cell lung cancer patients with brain metastases. Influence of treatment.Chest 1992;5: 1293–1297.
Kocher M, Müller R-I, Staar S, Degroot D. Long-term survival after brain metastases in breast cancer.Strahlenther Onkol 1995;171: 290–295.
Kaplan EW, Meier P. Nonparametric estimation from incomplete observations.J Am Stat Assoc 1958;53: 457–481.
Hall WA. Stereotactic radiosurgery for brain metastases.Crit Rev Neurosurg 1996;6: 257–262.
Joseph J, Adler JR, Cox RS, Hancock SL. Linear accelerator-based stereotaxic radiosurgery for brain metastases: the influence of number of lesions on survival.J Clin Oncol 1996;14: 1085–1092.
Macchiarini P, Buonaguidi R, Hardin M, Mussi A, Angeletti CA. Results and prognostic factors of surgery in the management of non-small cell lung cancer with solitary brain metastasis.Cancer 1991;68: 300–304.
Arbit E, Wronski M. Clinical decision making in brain metastases.Neurosurg Clin Nord Am 1996;7: 447–457.
Boogerd W, Vos VW, Hart AAM, Baris G. Brain metastases in breast cancer; natural history, prognostic factors and outcome.J Neurooncol 1993;15: 165–174.
Wronski M, Arbit E, Burt M, Galicich JH. Survival after surgical treatment of brain metastases from lung cancer: a follow-up study of 231 patients treated between 1976 and 1991.J Neurosurg 1995;83: 605–616.
Lang FF, Sawaya R. Surgical management of cerebral metastases.Neurosurg Clin Nord Am 1996;7: 459–484.
Armstrong JGet al. Postoperative radiation for lung cancer metastatic to the brain.J Clin Oncol 1994;12: 2340–2344.
Auchter RMet al. A multiinstitutional outcome and prognostic factor analysis of radiosurgery for resectable single brain metastasis.Int J Radiat Oncol Biol Phys 1996;35: 27–35.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hall, W., Djalilian, H., Nussbaum, E. et al. Long-term survival with metastatic cancer to the brain. Med Oncol 17, 279–286 (2000). https://doi.org/10.1007/BF02782192
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF02782192