
Abstract
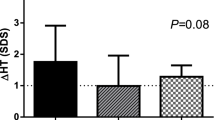
Auxological and endocrine data from 12 prepubertal children (3 males, 9 females) with Noonan syndrome (NS) were compared with those of 15 children with constitutional short stature (CSS), 20 children with partial GH deficiency (GHD), and 6 children with Turner syndrome (TS). Four children With NS were treated with human growth hormone (hGH) (n=4) (25 units/m2 week, divided on daily s.c. doses). In children with NS, the peak serum GH response to clonidine (5.4 ± 2.7 ug/L) and glucagon (7.4 ± 3.4 ug/L) were significantly lower than those for children with CSS (14.8 ±3.4 and 12.8 ± 2.8 ug/L respectively). Nine out of the 12 (75%) children with NS did not mount normal GH peak (10 ug/L or more) after provocation. The 12-h integrated GH secretion in the 3 children With NS who had normal GH response to provocation (2.7 ± 0.7 ug/L) was markedly lower compared to that for children with CSS (6.7 ±1.2 ug/L). The serum insulin-like growth factor-1 (IGF-l) concentrations were lower in children with NS (67 ± 32 ng/ml) vs CSS (165 ±35 ng/ml), but not different from those for GHD children (59 ± 33 ng/ml). In 4 children with NS, hGH therapy for a year increased height growth velocity from 4.1 ± 0.3 cm/yr to 7.4 ±0.6 cm/yr and height standard deviation score (Ht SDS) from -2.2 ± 0.6 to -1.45 ±0.3. This growth acceleration was accompanied by an increase in IGF-I concentration (from 52 ±21 ng/ml to 89 ± 25 ng/ml). In summary, these results prove a defect of the GH secretion in children with NS and suggest that GH therapy has an important role in the management of their short stature.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Mendez HM, Opitz. JM. Noonan syndrome: A review.Am J Med Genet 1985; 21:493–506.
Nora JJ, Nora AH, Sinha AK, Spangler RD, Lubs HA. The UllrichrNoonan syndrome (Turner phenotype).Am J Dis Child 1974; 127:48–55.
Sharland M, Burch M, McKenna WM, Paton MA. A clinical study of Noonan syndrome.Arch Dis Child 1992; 67: 178–183.
Witt DR, Keena BA, Hall JG, Allanson JE. Growth curves for height in Noonan syndrome.Clinical Genetics 1986; 30,: 150–153.
Ranke MB, Heindemann P, Kunpfer C, Enders H, Schmaltz AA, Bierich JR. Noonan syndrome: growth and clinical manifestations in 144 cases.Eur J Pediatr 1988; 148:22–27.
Char F, Rodriguez-Fernandez HL, Scott Cl, Borgaonkar DS, Bell BB, Rowe RD. The Noonan syndrome-a clinical study of forty five cases.Birth Defects: Original Articles Series 1972; 8 :110–118.
Collins E, Turner G. The Noonan syndrome: a review of the clinical and genetic features of 27 cases.J Pediatr 1973; 83:941–50.
Noonan JA. Association of congenital heart disease with syndromes or other defects.Pediatr Clin N Am 1978; 25: 797–816.
Pearl W. Cardiovascular anomalies in Noonan’s syndrome:Chest 1977; 71: 677–679.
Ross JL, Shenkman L. Case report: Noonans syndrome and hypopituitarism.Am J Med Sci 1980; 279: 47–52.
Sasagawa I, Nakada T, Kubota Y. Gonadal function and testicular histology in Noonan’s syndrome with bilateral cryptorchidism.Arch Androl 1994; 32: 135–140.
Theintz G, Savage MO. Growth and pubertal development in five boys with Noonan’s syndrome.Arch Dis Child 1982; 57:13–17.
Vestehus P, Aarskog D. Noonan’s syndrome and autoimmune thyroiditts.J Pediatr 1973; 83:237–240.
Ahmed ML, Foot AB, Edge JA, Lamkin VA, Savage VA, Dunger DB. Noonan’s syndrome: abnormalities of the growth hormone/IGF-1 axis and the response to treatment with human biosynthetic growth hormone.Acta Paediatr Scand 1991; 80 :446–450.
Tanaka K, Sato A, Naito T, Kuramochi K, Itabashi H, Takemura Y. Noonan syndrome presenting growth hormone neurosecretory dysfunction.Inter Med 1992; 31:908–911.
Thomas BC, Stanhope R. Long-term treatment with growth hormone in Noonan’s syndrome.Acta Paediatr 1993; 82: 853–855.
Batstone PJ, Faed MJ, Jung RT, Gsden J. 45,X/46, X dic (Y) mosaicism in a phenotypie male.Arch Dis Child 1991; 66: 252–253.
Assessment of endocrine function. In : Bertrand J, Rappaport R, Sizonenko PC (eds).Pediatric indocrinology, Physiology and Clinical Aspects. Williams and Wilkins, Baltimore, 1993; 658–683.
Tanner JM, Whitehouse RH. Clinical longitudinal standards for height, weight, height velocity, weight velocity and stages of puberty.Arch Dis Child 1976; 51: 170–179.
Preece MA, Greco L, Savage MO, Cameron N, Tanner JM. The auxology of growth delay (Abstract 14).Pediatr Res 1981; 15:76.
Goddard AD, Covello R, Luoh SM, Clackson T, Attie KM. Mutations of the growth hormone receptor in children with idiopathic short stature.N Engl J Med 1995; 333:1093.
Ranke MB, Blum WF, Haug F. Growth hormone somatomedin levels and growth regulation in Turner’s syndrome.Acta Endocrinol(Copenh) 1987; 116: 305–313.
Van Meter QL, Lee PA. Evaluation of puberty in male and female patients with Noonan syndrome.Pediatr Res 1980; 14: 485.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Soliman, A.T., Rajab, A., El Zalabany, M. et al. Defective Growth Hormone (GH) secretion and short-term treatment in Noonan syndrome. Indian J Pediatr 65, 741–749 (1998). https://doi.org/10.1007/BF02731057
Issue Date:
DOI: https://doi.org/10.1007/BF02731057