
Abstract
Objective:To determine whether transferring the care of patients to another senior resident the day after admission to the bospital adversely affects the efficiency and quality of care.
Design:Retrospective analysis of a natural experiment.
Setting:The general medical service of the Minneapolis Veterans Affairs Medical Center, a major tertiary teaching hospital of the University of Minnesota internal medicine residency program.
Patients/participants:Subjects were all the patients admitted to the medicine service from 5:00 PM to 6:00 AM over an eight-month period.
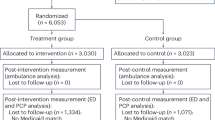
Intervention:After 5:00 PM, half of the patients were admitted to the hospital by a cross-covering senior resident (CC group of patients), and their care was transferred to a different senior resident the following day. The other patients were initially evaluated by the primary senior resident (PE group of patients). Assignment to the different services was a random, sequential process.
Measurements and main results:The CC group had significantly more laboratory tests performed during their hospital stay than did the PE group of patients (44 vs. 32, p=0.01), even when adjusted for length of stay. Using multiple linear regression to adjust for other clinical parameters including length of stay, DRG weight, and number of consults, the authors found that being a CC subject was a significant predictor of the number of laboratory tests obtained (p=0.01). Furthermore, the median length of stay in the CC group (n=74) was longer than that in the PE group (n=72) (eight days vs. six days); this was of borderline statistical significance, using a two-sample median test (p=0.06).
Conclusion:Patients transferred to a different resident the day after admission had more laboratory tests performed and longer inpatient stays.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Wasson JH, Sauvigne AE, Mogielnicki RP, et al. Continuity of outpatient medical care in elderly men: a randomized trial. JAMA. 1984;252:2413–7.
Cohen DI, Breslau D, Porter DK, et al. The cost implications of academic group practice: a randomized controlled trial. N Engl J Med. 1986;314:1553.
Rudd PA, Siegler M, Byyny RL. Perioperative diabetic consultation: a plea for improved training. J Med Educ. 1978;53:590–6.
Lazare A, Eisenthal S. A negotiated approach to the clinical encounter. In: Lazare A. Outpatient psychiatry: diagnosis and treatment. Baltimore: Williams & Wilkins, 1979:141–56.
Quill TE. Partnerships in patient care: a contractual approach. Ann Intern Med. 1983;98:228–34.
Starfield B, Wray C, Hess K, Gross R, Birk P, D’Lugoff B. The influence of patient-practitioner agreement on outcome of care. Am J Public Health. 1981;71:127–31.
Balint M. The doctor, his patient, and the illness. New York: International University Press, 1972.
Novack DH. Therapeutic aspects of the clinical encounter. J Gen Intern Med. 1987;2:346–55.
Cohen-Cole SA, Bird J. Interviewing the cardiac patient. II: A practical guide for helping patients cope with their emotions. Quality of Life and Cardiovasc Care. 1986;Jan/Feb.
Rich EC, Crowson TW, Harris IB. The diagnostic value of the medical history. Arch Intern Med. 1987;147:1957–60.
Sandler G. Costs of unnecessary tests. Br Med J. 1979;2:21–4.
Young MJ, Poses RM. Medical student perceptions of the value of the history and physical examination. J Med Educ. 1983;58:738–9.
Kroenke K, Hanley JF, Copley JB, et al. Improving house staff ordering of three common laboratory tests: reductions in test ordering need not result in underutilization. Med Care. 1987;25:928–35.
Tierney WM, Miller ME, McDonald CJ. The effect of test ordering on informing physicians of the charges for outpatient diagnostic tests. N Engl J Med. 1990;322:1499–504.
Cohen DI, Breslau D, Porter DK, et al. Group practice in an academic setting: a controlled trial. Report to the National Center for Health Services Research, 1985.
Cohen DI, Breslau D, Porter D, et al. Academic group practice: the patient’s perspective. Med Care. 1986;24:990.
Fineberg HV. Clinical chemistries: the high cost of low-cost diagnostic tests. In: Altman SH, Blendon R, eds. Medical technology: the culprit behind health care costs? Hyattsville, MD: Public Health Service, 1979; DHEW publication no. (PHS) 79-3216.
Glickman RM. House-staff training: the need for careful reform. N Engl J Med. 1988;318:780–2.
Resident supervision and hours: recommendations of the Association of American Medical Colleges. Reprinted in: J Med Educ. 1988;63:421–6.
American College of Physicians. Working conditions and supervision for residents in internal medicine programs: recommendations. Ann Intern Med. 1989;110:657–63.
Lubell A. NY moves to restrict resident, intern work hours. Am Med News. 1988;(July 1):18–22.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Lofgren, R.P., Gottlieb, D., Williams, R.A. et al. Post-call transfer of resident responsibility. J Gen Intern Med 5, 501–505 (1990). https://doi.org/10.1007/BF02600880
Issue Date:
DOI: https://doi.org/10.1007/BF02600880