
Abstract
Objective: To determine patient characteristics associated with the desire for life-sustaining treatments in the event of terminal illness.
Design: In-person survey from October 1986 to June 1988.
Setting: 13 internal medicine and family practices in North Carolina.
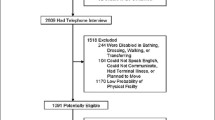
Patients: 2,536 patients (46% of those eligible) aged 65 years and older who were continuing care patients of participating practices, enrolled in Medicare. The patients were slightly older than the 65+ general population, 61% female, and 69% white, and most had one or more chronic illnesses.
Measurements and main results: The authors asked the patients whether they would want each of six different treatments (hospitalization, intensive care, cardiopulmonary resuscitation, surgery, artificial ventilation, or tube feeding) if they were to have a terminal illness. The authors combined responses into three categories ranging from the desire for more treatment to the desire for less treatment. After adjustment for other factors, 53% of women chose less treatment compared with 43% of men; 35%ofblacksvs 15% of whites and 23% of the less well educated vs 15% of the better educated expressed the desire for more treatment. High depression scores also were associated with the desire for more treatment (26% for depressed vs 18% for others).
Conclusion: Patients’ choices for care in the event of terminal illness relate to an intricate set of demographic, educational, and cultural factors. These results should not be used as a shortcut to determine patient preferences for care, but may provide new insights into the basis for patients’ preferences. In discussing choices for future life-sustaining care, physicians need to explore with each individual the basis for his or her choices.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Hastings Center. Guideline on the termination of life-sustaining treatment and the care of the dying. Bloomington, IN: University Press, 1987.
Wolf SM, Boyle T, Callahan D, et al. Sources of concern about the Patient Self-Determination Act. N Engl J Med. 1991;325:1666–71.
Emanuel IX, Barry MJ, Stoeckle JD, Ettelson LM, Emanuel EJ. Advance directives for medical care—a case for greater use. N Engl J Med. 1991;324:889–95.
Gamble ER, McDonald PJ, Lichstein PR. Knowledge, attitudes, and behavior of elderly persons regarding living wills. Arch Intern Med. 1991;515:277–80.
Lo B, McLeod GA, Saika G. Patient attitudes to discussing life-sustaining treatment. Arch Intern Med. 1986;146:1613–5.
Snow RM, Atwood K. Probable death: perspective of the elderly. South Med J. 1985;78:851–3.
Mossey J, Shapiro E. Self-rated health: a predictor of mortality among the elderly. Am J Public Health. 1982;72:800–8.
Kaplan RM, Anderson JP. The general health policy model: an integrated approach. In: Spilker B (ed). Quality of life assessments in clinical trials. New York: Raven Press, 1990;131–49.
Patrick DL, Bush J, Chen M. Toward an operational definition of health. J Health Soc Behav. 1973;14:6–23.
Kaplan RM, Bush JW, Berry CC. Health status: types of validity and the index of well-being. Health Serv Res. 1976;11:478–507.
Danis M, Patrick DL, Southerland LI, et al. Patients’ and families’ preferences for medical intensive care. JAMA. 1988;260:797–802.
Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Measurement. 1977;1:385–401.
Fries J. Personal communication, Sept 1991.
Frankl D, Oye RK, Bellamy PE. Attitude of hospitalized patients toward life support: survey of 200 medical inpatients. Am J Med. 1989;86:645–8.
Danis M, Mutran E, Fitzsimmons J. Attitudes associated with the desire for life-sustaining treatment in elderly patients. Clin Res. 1991;39(2):624A.
Wenger NS, Oye RK, Teno JM, et al. Patient age, race and perceived health status are associated with preferences for “comfort care.” Clin Res. 1992;40(2):620A.
Miles SH, August A. Courts, gender and “the right to die”. Law Med Health Care. 1990;19(1–2):85–95.
Strogatz DS. Use of medical care for chest pain: differences between blacks and whites. Am J Public Health. 1990;80:290–4.
Kessler RC, Neighbors HW. A new perspective on the relationships among race, social class, and psychological distress. J Health Soc Behav. 1986;27:107.
Kasiske BL, Neylan JF, Riggio RR, et al. The effects of race on access and outcome in transplantation. N Engl J Med. 1991;324:302–7.
Wenneker MB, Epstein AM. Racial inequalities in the use of procedures for patients with ischemic heart disease in Massachusetts. JAMA. 1989;261:253–7.
James SA, Wagner EH, Strogatz DS, et al. The Edgecombe County (NC) high blood pressure control program: II. Barriers to the use of medical care among hypertensives. Am J Public Health. 1985;74:468–72.
Gemson DH, Elinson J, Messeri P. Differences in physician prevention practice patterns for white and minority patients. Community Health. 1988;13(1):53–64.
Blendon RJ, Aiken LH, Freeman HE, Corey CR. Access to medical care for black and white Americans. JAMA. 1989;261:278–81.
Sehgal A, Galbraith A, Chesney M, Schoenfeld P, Charles G, Lo B. How strictly do dialysis patients want their advance directives followed: JAMA. 1992;267:59–63.
Meehan PJ, Saltzman LE, Sattin RW. Suicides among older United States residents: epidemiologic characteristics and trends. Am J Public Health. 1991;81:1198–200.
Lund J. Personal communication, Sept 1991.
National Center for Health Statistics. Health, United States, 1990. Hyattsville, MD: Public Health Service, 1991.
Kalish RA, Reynolds DK. Death and ethnicity: a psychocultural study. Los Angeles, CA: Ethyl Percy Andrus Gerontology Center, University of Southern California, 1976.
Blendon JR, Szalay VS, Knox RA. Should physicians aid their patients in dying? JAMA. 1992;267:2658–62.
President’s Commission for the Study of Ethical Problems in Medicine and Biomedical and Behavioral Research. Deciding to forego life-sustaining treatment. Washington, DC: U.S. Government Printing Office, 1983.
Wanzer SH, Federman DD, Adelstein SJ, et al. The physician’s responsibility toward hopelessly ill patients: a second look. N Engl J Med. 1989;320:844–9.
Author information
Authors and Affiliations
Additional information
Supported in part by a cooperative research agreement (95-C-98516/4) between the Health Care Financing Administration and the Department of Social Medicine, School of Medicine, in collaboration with the Cecil G. Sheps Center for Health Services Research, at the University of North Carolina at Chapel Hill (Joseph P. Morrissey, PhD, principal investigator).
The views expressed are those of the authors and do not necessarily reflect the opinions of HCFA.
Rights and permissions
About this article
Cite this article
Garrett, J.M., Harris, R.P., Norburn, J.K. et al. Life-sustaining treatments during terminal illness. J Gen Intern Med 8, 361–368 (1993). https://doi.org/10.1007/BF02600073
Issue Date:
DOI: https://doi.org/10.1007/BF02600073