
Abstract
Objective: To assess whether vital sign measurements could identify internal medicine patients at risk for cardiopulmonary arrest.
Design: Retrospective case-control study comparing 72 hours of pre-arrest vital sign measurements with 72 hours of vital sign measurements for patients from the same units who did not experience cardiopulmonary arrest.
Setting: Twelve non — intensive care internal medicine units at a large midwestern academic medical center.
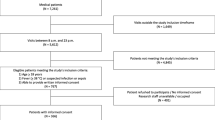
Patients: Cases included all 59 inpatients who had experienced cardiopulmonary arrest between May 1989 and December 1990; patients who were designated do-not-resuscitate (DNR) or had less than 72 hours of vital sign recordings were excluded. Controls included 91 inpatients without cardiopulmonary arrest who were matched for units and who had 72 hours of vital sign recordings.
Results: The occurrence of one or more respiratory rates >27 breaths per minute over a 72-hour period had a sensitivity of 0.5 4 and a specificity of 0.83 (odds ratio=5.56, 95% CL=2.67–11.49) in predicting cardiopulmonary arrest. Other respiratory rate thresholds were also predictive of arrest. The ability of respiratory rate to predict arrest was stronger in units with high incidences of arrest relative to units with low incidences, for example, in units for the management of gastrointestinal disease (sensitivity=1.00, specificity=0.86) and renal disease (sensitivity=0.69, specificity=0.87). Respiratory rate remained a significant predictor (p<0.001) after controlling for patient age and gender. Pulse rate and blood pressure were not predictive of cardiopulmonary arrest.
Conclusions: Using elevated respiratory rates as a signal for focused diagnostic studies and therapeutic interventions in internal medicine patients may be useful in reducing the incidence of subsequent cardiopulmonary arrest, and lowering associated morbidity and mortality.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Kory RC. Routine measurement of respiratory rate: an expensive tribute to tradition. JAMA. 1957;165:448–50.
Castagna J, Weil MH, Shubin H. Factors determining survival in patients with cardiac arrest. Chest. 1974;65:527–9.
Schein RMH, Hazday N, Pena M, Ruben BH, Sprung CL. Clinical antecedents to in-hospital cardiopulmonary arrest. Chest. 1990;98:1388–92.
Sax FL, Charlson ME. Medical patients at high risk for catastrophic deterioration. Crit Care Med. 1987;15:510–5.
Cohen CA, Zagelbaum G, Gross D, Rousses C, Macklem PT. Clinical manifestations of inspiratory fatigue. Am J Med. 1982;73:308–16.
Pardee NE, Winterbauer RH, Allen JD. Bedside evaluation of respiratory distress. Chest. 1984;85:203–6.
Tobin MJ, Perez W, Guenther SM, et al. The pattern of breathing during successful and unsuccessful trails of weaning from mechanical ventilation. Am Rev Respir Dis. 1986;134:1111–8.
Fallat RJ. Respiratory monitoring. Clin Chest Med. 1982;3:181–4.
Browning IB, D’Alonzo GE, Tobin MJ. Importance of respiratory rate as an indicator of respiratory dysfunction in patients with cystic fibrosis. Chest. 1980;97:1317–21.
Gravelyn TR, Weg JG. Respiratory rate as an indicator of acute respiratory dysfunction. JAMA. 1980;244:1123–5.
McFadden JP, Price RC, Eastwood HD, Briggs RS. Raised respiratory rate in elderly patients: a valuable physical sign. BMJ. 1982;284:626–7.
Bedell SE, Delbanco TL, Cook EF, Epstein FH. Survival after cardiopulmonary resuscitation in the hospital. N Engl J Med. 1983;309:569–76.
George AL, Folk BP, Crecelius PL, Campbell WB. Pre-arrest morbidity and other correlates of survival after in hospital cardiopulmonary arrest. Am J Med. 1989;87:28–34.
Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13:818–29.
SAS Institute. SAS Technical Report P-200 SAS/STAT Software: CALIS and LOGISTIC Procedures, Release 6.04. Cary, NC: SAS Institute, 1990.
Knaus WA, Wagner DP, Draper EA. Relationship between acute physiologic derangement and risk of death. J Chron Dis. 1985;38:295.
Krieger B, Feinerman D, Zaron A, Bizousky F. Continuous noninvasive monitoring of respiratory rate in critically ill patients. Chest. 1986;90:632–4.
Eberhart RC, Weigelt JA. Respiratory monitoring: current techniques and some new developments. Bull Eur Physiopathol Respir. 1985;21:295–300.
Arnson LA, Rau JL, Dixon RJ. Evaluation of two electronic respiratory rate monitoring systems. Respir Care. 1981;26:221–7.
Bedell SE, Deitz DC, Leeman D, Delbanco TL. Incidence and characteristics of preventable iatrogenic cardiac arrests. JAMA. 1991;265:2815–920.
Author information
Authors and Affiliations
Additional information
Supported in part by a grant from the Robert Wood Johnson Foundation, and by the Center for Health Services Research, University of Iowa.
Rights and permissions
About this article
Cite this article
Fieselmann, J.F., Hendryx, M.S., Helms, C.M. et al. Respiratory rate predicts cardiopulmonary arrest for internal medicine inpatients. J Gen Intern Med 8, 354–360 (1993). https://doi.org/10.1007/BF02600071
Issue Date:
DOI: https://doi.org/10.1007/BF02600071