
Abstract
Objective:To determine whether two different educational interventions would reduce polypharmacy in outpatients receiving ten (10) or more active medications at the Denver Veterans Affairs Center.
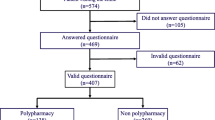
Design:292 patients were randomized into three (3) groups: Control (n=88); simple notification of primary care provider (n=102); intensive notification, provision of pharmacy profiles, compliance index, and chart review by senior clinician with recommendations (n=104).
Setting:Veterans Affairs Medical Center affiliated with the University of Colorado Health Sciences Center.
Patients/Participants:All patients receiving greater than ten (10) active medications who are followed by clinic staff at the Denver VAMC. The mean age was 62 years (range 26–88) and 96% were male.
Interventions:The simple notification group received only a single letter recommending that the patient’s number of medications be reduced. The intensive notification group received more sophisticated intervention with a chart review, two letters with calculation of patient compliance, and individualized suggestions for reduction in polypharmacy. The control group received no intervention.
Measurements and main results:Control patients had significantly less reduction in polypharmacy then either the simple or intensive intervention groups at four months (p=0.028). There was no significant difference between the intervention groups (p=0.189). By six months the difference was no longer significant.
Conclusions:A simple intervention can result in a significant reduction in the number of medications prescribed to patients with polypharmacy. The authors were unable to show that a more complex intervention resulted in a further reduction in polypharmacy.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Kroenke K. Polypharmacy: causes, consequences, and cure. Am J Med 1985;79:149–52.
Oboler SK, Blieden MA, Carter SA, et al. A mobile internal medicine clinic. Arch Intern Med 1983;143:97–9.
Kramer MS, Leventhal JM, Hutchinson TA, Feinstein AR. An algorithm for the operational assessment of adverse drug reactions: I. Background, description and instructions for use. JAMA 1979;242:623–32.
Steiner JF, Koepsell TD, Fihn SD, Inui TS. A general method of compliance assessment using centralized pharmacy records: description and validation. Med Care 1988;26:814–23.
Rodriguez LR, Halperin AK, Gordon B, Weber C. An ambulatory care pharmacy clinic to control polypharmacy. Va Practitioner (June 1987; 61–70.
Steele MA, Bess DT, Franse VL, Graber SE. Cost effectiveness of two interactions for reducing outpatient prescribing costs. DICP Ann Pharmacother 1989;23:497–500.
Martin AR, Wolf MA, Thibodeau LA, et al. A trial of two strategies to modify the test ordering behavior of medical residents. N Engl J Med 1980;303:1330–6.
Cummins RO, LoGerfo JP, Inui TS, Weiss NS. High yield referral criteria for post traumatic skull roentgenography. JAMA 1980;244:673–6.
Klein LE, German PS, Levine DM, et al. Medication problems among outpatients. Arch Intern Med 1984;144:1185–8.
Smith JW, Seidl LG, Cluff LE. Studies on the epidemiology of adverse drug reactions. V. Clinical factors influencing susceptibility. Ann Intern Med 1966;65:629–40.
Karch FE, Lasagna L. Adverse drug reaction — a critical review. JAMA 1975;231:1236–41.
Author information
Authors and Affiliations
Additional information
Received from the Department of Medicine, Denver VA Medical Center, and Division of General Medicine, University of Colorado Health Sciences Center, Denver, Colorado.
Supported by the Denver Veterans Affairs Medical Center and the Division of General Internal Medicine at the University of Colorado Health Sciences Center.
Rights and permissions
About this article
Cite this article
Meyer, T.J., Van Kooten, D., Marsh, S. et al. Reduction of polypharmacy by feedback to clinicians. J Gen Intern Med 6, 133–136 (1991). https://doi.org/10.1007/BF02598309
Issue Date:
DOI: https://doi.org/10.1007/BF02598309