
Summary
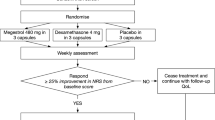
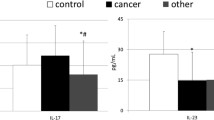
The aim of our study (clinical phase II open pilot study) was to evaluate the toxicity of megestrol acetate and its ability to increase appetite and body weigth in patients with advanced-stage (III–IV) primary head and neck squamous cell carcinoma treated with neoadjuvant (primary) chemotherapy. Serum levels of interleukin-1α and β, interleukin-2 and 6, tumor necrosis factor-α, and the soluble receptor for interleukin-2 were evaluated before and after megestrol acetate treatment. The same cytokines and soluble interleukin-2 receptor were also measured in culture medium of peripheral blood lymphocytes from the same patients after stimulation with phytohemagglutinin. From April 1993 to February 1994, 11 male patients were enrolled in our study: their mean age was 57.8 years (range 43–69 years). Megestrol acetate was administered at a dose of 320 mg/day in the interval between chemotherapeutic cycles for a total of three consecutive cycles; 9 of the 11 patients could be evaluated (81.8%). Except for the performance status according to Karnofsky, all parameters were increased after megestrol acetate treatment. The average weight increased by 6.3 kg (13.2%), appetite by a score of 2.4 (38.6%) and the Spitzer’s quality of life index by a score of 2.4 (36.2%). The performance status according to Karnofsky decreased in only 1 patient, remained the same in most patients, and in 2 patients was slightly improved. No significant side effects were observed during treatment. Serum levels of interleukin-1α and β, interleukin-2 and 6, tumor necrosis factor-α, and soluble interleukin-2 receptor were significantly higher than in normal subjects, prior to treatment with megestrol acetate. These levels dropped after megestrol acetate treatment with a statistically significant decrease for interleukin-1α and β and tumor necrosis factor-α. There were no significant differences in the production of cytokines by peripheral blood lymphocytes stimulated with phytohemagglutinin from patients before megestrol acetate treatment and normal subjects, with the exception of interleukin-6 (higher in patients) and of soluble interleukin-2 receptor (lower in patients). There was no significant difference in the cytokines and soluble interleukin-2 receptor produced in culture before and after megestrol acetate treatment, except for interleukin-6 which decreased after treatment.
Article PDF
Similar content being viewed by others
Avoid common mistakes on your manuscript.
References
Warren S. The immediate causes of death in cancer. Am J Med Sci 1932; 184:610.
Heber D, Byerley LO, Chi J. Pathophysiology of malnutrition in the adult cancer patient. Cancer Res 1986; 58:1867.
Bruera E. Clinical management of anorexia and cachexia in patients with advanced cancer. Oncology 1992; 49 [Suppl]:35.
Brennan MR. Uncomplicated starvation vs cancer cachexia. Cancer Res 1977; 37:2359.
McNamara MJ, Alexander HR, Norton JA. Cytokines and their role in the pathophysiology of cancer cachexia. J Parent Enter Nutr 1992; 16 [Suppl]:505.
Moldawer LL, Gelin J, Schersten T. Circulating interleukin 1 and tumor necrosis factor during inflammation. Am J Physiol 1987; 253:R922.
Moldawer LL, Andersson C, Gelin J. Regulation of food intake and hepatic protein synthesis by recombinant derived cytokines. Am J Physiol 1988; 254:6450.
Strassmann G, Fong M, Kenney JS, Jacob CO. Evidence for the involvement of interleukin-6 in experimental cancer cachexia. J Clin Invest 1992; 89:1681.
Busbridge J, Dascombe MJ, Hoopkins S. Acute central effects of interleukin-6 on body temperature, thermogenesis and food intake in the rat. Proc Nutr Soc 1989; 38:48A.
Gelin J, Moldawer LL, Lonnroth C. Role of endogenous tumor necrosis factor alfa and interleukin 1 for experimental tumor growth and the development of cancer cachexia. Cancer Res 1991; 51:415.
McLaughlin CL, Rogan GJ, Ton J. Food intake and body temperature responses of rat to recombinant interleukin 1 beta and a tripeptide interleukin 1 beta antagonist. Physiol Behav 1992; 52:1155.
Sherry BA, Gelin J, Fong Y. Anticachectin/tumor necrosis factor alfa antibodies attenuate development of cancer cachexia. Cancer Res 1991; 51:415.
Starnes HF Jr, Pearce MK, Tewan A. Anti-IL6 monoclonal antibodies protect against lethalEscherichia coli infection and lethal tumor necrosis factor-alpha challenge in mice. J Immunol 1990; 145:4185.
Nelson K, Walsh D. Management of the anorexia/cachexia syndrome. Cancer Bull 1991; 43:403.
Loprinzi CL, Ellison NM, Schaid DJ, et al. Controlled trial of megestrol acetate for the treatment of cancer anorexia and cachexia. J Natl Cancer Inst 1990; 82:1127.
Tchekmedyian NS, Tait N, Moody M, et al. Appetite stimulation with megestrol acetate in cachectic cancer patients. Semin Oncol 1986; 13 [Suppl 4]:37.
Bruera E, Macmillan K, Kuehn N, et al. A controlled trial of megestrol acetate on appetite, caloric intake, nutritional status, and other symptoms in patients with advanced cancer. Cancer 1990; 66:1279.
Tchekmedyian NS, Tait N, Moody M, Aisner J. High-dose megestrol acetate. A possible treatment for cachexia. JAMA 1987; 257:1195.
Aisner J, Tchekmedyian NS, Tait N, et al. Studies of high-dose megestrol acetate: potential applications in cachexia. Semin Oncol 1988; 15 [Suppl 1]:68.
Reitmeier M, Hartenstein RC. Megestrol acetate and determination of body composition by bioelectrical impedence analysis in cancer cachexia. Proc Annu Meet Am Soc Clin Oncol 1990; 9:A1256.
Tchekmedyian NS, Hickman M, Siau J, et al. Megestrol acetate in cancer anorexia and weight loss. Cancer 1992; 69:1268.
Von Roenn JH, Murphy RL, Wegener N. Megestrol acetate for treatment of anorexia and cachexia associated with human immunodeficiency virus infection. Semin Oncol 1990; 17 [Suppl 9]: 13.
Tchekmedyian NS, Hickman M, Heber D. Treatment of anorexia and weight loss with megestrol acetate in patients with cancer or acquired immunodeficiency syndrome. Semin Oncol 1991; 18 [Suppl 2]:35.
Rooney M, Kish J, Jacobs J, Kinzie J, Weaver A, Crissman J, Al-Sarraf M. Improved complete response rate and survival in advanced head and neck cancer after three-course induction therapy with 120-hour 5-FU infusion and cisplatin. Cancer 1985; 55:1123.
Spitzer OW, Dobson AJ, Hall J, et al. Measuring the quality of life of cancer patients. A concise QL-Index for use by physicians. J Chron Dis 1981; 34:585 (confirmed).
Aisner J, Tchekmedyian NS, Moody M, Tait N. High-dose megestrol acetate for the treatment of advanced breast cancer: dose and toxicities. Semin Hematol 1987; 24:48.
Muss HB, Case LD, Capizzi RL, et al. High-versus standard-dose megestrol acetate in women with advanced breast cancer: a phase III trial of the Piedmont Oncology Association. J Clin Oncol 1990; 8:1797.
Tchekmedyian NS, Tait N, Moody M, et al. Appetite stimulation with megestrol acetate in cachectic cancer patients. Semin Oncol 1986; 13:37.
Cruz JM, Muss HB, Brockschmidy JK, Evans JW. Weight changes in women with metastatic breast cancer treated with megestrol acetate: a comparison of standard- versus high-dose therapy. Semin Oncol 1990; 6 [Suppl 9]:63.
Tepmongkol P, Chonsiriwat K, Thansakul A. Megestrol acetate as the supportive treatment of Thai patients with advanced cancer. J Med Assoc Thai 1990; 73:487.
Tchekmedyian NS, Hariri L, Siau J, et al. Megestrol acetate in cancer anorexia and weight loss. Proc Annu Meet Am Soc Clin Oncol 1990; 9:336.
Nelson KA, Walsh D, Sheehan FA. The cancer anorexia-cachexia syndrome. J Clin Oncol 1994; 12:213.
Hamburger AW, Parnes H, Gordon GB, et al. Megestrol acetateinduced differentiation of 3T3-Li adipocytes in vitro. Semin Oncol 1988; 15:76.
Krauss RM, Grunfeld C, Doerrler WT, Feingold KR. TNF acutely increases plasma levels of very low density lipoproteins of normal size composition. Endocrinology 1990; 127:1016.
Torti F, Dieckmann B, Beumer B, et al. A macrophage factor inhibits adipose gene expression: an in vitro model of cachexia. Science 1985; 229:867.
Oliff A, Defeo-Jones D, Boyer M, et al. Tumors secreting human TNF/cachectin induce cachexia in mice. Cell 1987; 50:555.
Oliff A. The role of tumor necrosis factor (cachectin) in cachexia. Cell 1988; 54:141.
Saarinen UM, Koskelo EK, Teppo AM, et al. Tumor necrosis factor in children with malignancies. Cancer Res 1990; 50:592.
Sherry BA, Gelin J, Fong Y, et al. Anticachectin tumor necrosis factor-alpha antibodies attenuate development of cachexia in tumor models. FASEB J 1989; 3:1956.
Beck SA, Tisdale MJ. Effect of megestrol acetate on weight loss induced by tumor necrosis factor alpha and a cachexia-inducing tumor MAC 16 in NMRI mice. Br J Cancer 1990; 62:420.
Polan ML, Loukides J, Nelson P, et al. Progesterone and estradiol modulate interleukin-1 beta messenger ribonucleic acid levels in cultured human peripheral monocytes. J Clin Endocrinol Metab 1989; 69:1200.
Terada K, Parisa MD, Suthum A, et al. The effect of megestrol acetate on interleukin-1 activity. Gynecol Oncol 1991; 43:260.
Eisen HN. Tumor immunology. Philadelphia: Lippincott: 1990:231.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Mantovani, G., Macció, A., Bianchi, A. et al. Megestrol acetate in neoplastic anorexia/cachexia: clinical evaluation and comparison with cytokine levels in patients with head and neck carcinoma treated with neoadjuvant chemotherapy. Int J Clin Lab Res 25, 135–141 (1995). https://doi.org/10.1007/BF02592554
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF02592554