
Abstract
Background
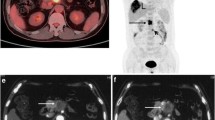
This study examined the effect that 18-fluorodeoxyglucose positron emission tomography (18FDG-PET) imaging had on the clinical management of patients with suspected periampullary malignancy.
Methods
Fifty-four patients with suspected pancreatic neoplasms underwent both whole-body18FDG-PET and abdominal computed tomography (CT). Malignant or benign disease was confirmed pathologically in 47 patients.
Results
Of the 41 patients with malignancy,18FDG-PET failed to identify the primary tumor in 5 patients.18FDG-PET demonstrated increased uptake suggesting primary malignancy in 37 patients. Malignant pathology was confirmed in 36 cases.18FDG-PET identified malignant locoregional lymph node metastases in six of ten patients. All nodes identified before surgery by18FDG-PET were also seen on preoperative CT. Six patients who were thought to have resectable disease by CT were found to have distant metastasis at laparotomy.18FDG-PET did not detect metastasis in any of these cases. Before surgery,18FDG-PET identified distant metastases that were not detected by CT in one patient.
Conclusions
Despite high sensitivity and specificity in diagnosing periampullary malignancy,18FDG-PET did not change clinical management in the vast majority of patients previously evaluated by CT. In addition,18FDG-PET missed>10% of periampullary malignancies and did not provide the anatomical detail necessary to define unresectability.
Article PDF
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
References
Yeo CJ, Cameron JL. The pancreas. In: Sabiston DC, ed.Textbook of Surgery: The Biological Basis of Modern Surgical Practice. Philadelphia: WB Saunders, 1997:1152–86.
Greenlee R, Murray T, Bolden S, Wingo P. Cancer statistics, 2000.CA Cancer J Clin 2000;50:7–33.
National Cancer Institute.SEER Cancer Statistics Review 1973–1990. Bethesda, MD: National Institutes of Health, 1993.
Sohn TA, Yeo CJ, Cameron JL, et al. Resected adenocarcinoma of the pancreas—616 patients: results, outcomes, and prognostic indicators.J Gastrointest Surg 2000;4:567–79.
Yeo CJ, Cameron JL, Sohn TA, et al. Six hundred fifty consecutive pancreaticoduodenectomies in the 1990s: pathology, complications, and outcomes.Ann Surg 1997;226:248–57; discussion, 257–60.
Reddy KR, Levi J, Livingstone A, et al. Experience with staging laparoscopy in pancreatic malignancy.Gastrointest Endosc 1999; 49:498–503.
Warshaw AL, Gu ZY, Wittenberg J, Waltman AC. Preoperative staging and assessment of resectability of pancreatic cancer.Arch Surg 1990;125:230–3.
Berberat P, Friess H, Kashiwagi M, Beger HG, Buchler MW. Diagnosis and staging of pancreatic cancer by positron emission tomography.World J Surg 1999;23:882–7.
van Heertum RL, Fawwaz RA. The role of nuclear medicine in the evaluation of pancreatic disease.Surg Clin North Am 2001;81:345–58.
Frohlich A, Diederichs CG, Staib L, Vogel J, Beger HG, Reske SN. Detection of liver metastases from pancreatic cancer using FDG PET.J Nucl Med 1999;40:250–5.
Higashi T, Tamaki N, Honda T, et al. Expression of glucose transporters in human pancreatic tumors compared with increased FDG accumulation in PET study.J Nucl Med 1997;38:1337–44.
Reske SN, Grillenberger KG, Glatting G, et al. Overexpression of glucose transporter 1 and increased FDG uptake in pancreatic carcinoma.J Nucl Med 1997;38:1344–8.
Jadvar H, Fischman AJ. Evaluation of pancreatic carcinoma with FDG PET.Abdom Imaging 2001;26:254–9.
Mertz HR, Sechopoulos P, Delbeke D, Leach SD. EUS, PET, and CT scanning for evaluation of pancreatic adenocarcinoma.Gastrointest Endosc 2000;52:367–71.
Rose DM, Delbeke D, Beauchamp RD, et al.18Fluorodeoxyglucose-positron emission tomography in the management of patients with suspected pancreatic cancer.Ann Surg 1999;229:729–37.
Keogan MT, Tyler D, Clark L, et al. Diagnosis of pancreatic carcinoma: role of FDG PET.AJR Am J Roentgenol 1998;171:1565–70.
Imdahl A, Nitzsche E, Krautmann F, et al. Evaluation of positron emission tomography with 2-[18F]fluoro-2-deoxy-D-glucose for the differentiation of chronic pancreatitis and pancreatic cancer.Br J Surg 1999;86:194–9.
Zinny M, Buell U.18FDG-positron emission tomography in pancreatic cancer.Ann Oncol 1999;10:28–32.
Inokuma T, Tamaki N, Torizuka T, et al. Evaluation of pancreatic tumors with positron emission tomography and F-18 fluorodeoxy-glucose: comparison with CT and US.Radiology 1995;195:345–52.
Friess H, Langhans J, Ebert M, et al. Diagnosis of pancreatic cancer by 2[18F]-fluoro-2-deoxy-D-glucose positron emission tomography.Gut 1995;36:771–7.
Kasperk RK, Riesener KP, Wilms K, Schumpelick V. Limited value of positron emission tomography in treatment of pancreatic cancer: surgeon's view.World J Surg 2001;25:1134–9.
Delbeke D, Rose DM, Chapman WC, et al. Optimal interpretation of FDG PET in the diagnosis, staging and management of pancreatic carcinoma.J Nucl Med 1999;40:1784–91.
Diederichs CG, Staib L, Glatting G, Beger HG, Reske SN. FDG PET: elevated plasma glucose reduces both uptake and detection rate of pancreatic malignancies.J Nucl Med 1998;39:1030–3.
Lindholm P, Minn H, Leskin-Kallio S. Influence of blood glucose concentration on FDG uptake in cancer: a PET study.J Nucl Med 1993;34:1–6.
Nakamoto Y, Higashi T, Sakahara H, et al. Evaluation of pancreatic islet cell tumors by fluorine-18 fluorodeoxyglucose positron emission tomography: comparison with other modalities.Clin Nucl Med 2000;25:115–9.
Adams S, Baum R, Rink T, Schumm-Drager PM, Usadel KH, Hor G. Limited value of fluorine-18 fluorodeoxyglucose positron emission tomography for the imaging of neuroendocrine tumours.Eur J Nucl Med 1998;25:79–83.
Diederichs CG, Staib L, Vogel J, et al. Values and limitations of18F-fluorodeoxyglucose-positron-emission tomography with preoperative evaluation of patients with pancreatic masses.Pancreas 2000;20:109–16.
Kubato R, Yamada Y, Torizuka T. Intratumoral distribution of fluorine-18-fluorodeoxyglucose in vivo: high accumulation in macrophages and granulation tissues studied by microradiography.J Nucl Med 1992;33:1972–80.
Shreve P. Focal fluorine-18 fluorodeoxyglucose accumulation in inflammatory pancreatic disease.Eur J Nucl Med 1998;25:259–64.
Sendler A, Avril N, Helmberger H, et al. Preoperative evaluation of pancreatic masses with positron emission tomography using18F-fluorodeoxyglucose: diagnostic limitations.World J Surg 2000;24:1121–9.
Schwarz M, Pauls S, Sokiranski R, et al. Is a preoperative multidiagnostic approach to predict surgical resectability of periampullary tumors still effective?Am J Surg 2001;182:243–9.
Hommeyer SC, Freeny PC, Crabo LG. Carcinoma of the head of the pancreas: evaluation of the pancreaticoduodenal veins with dynamic CT-potential of improved accuracy in staging.Radiology 1995;196:233–8.
Ruers T, Langenhoof B, Neeleman N, et al. Value of positron emission tomography with [F-18] fluorodeoxyglucose in patients with colorectal liver metastases: a prospective study.J Clin Oncol 2002;20:388–95.
White R, Hurwitz H, Lee C, et al. Neoadjuvant chemoradiation for localized adenocarcinoma of the pancreas.Ann Surg Oncol 2001; 8:758–65.
Sperti C, Pasquali C, Chierichetti F, Liessi G, Ferlin G, Pedrazzoli S. Value of 18-fluorodeoxyglucose positron emission tomography in the management of patients with cystic tumors of the pancreas.Ann Surg 2001;234:675–80.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kalady, M.F., Clary, B.M., Clark, L.A. et al. Clinical utility of positron emission tomography in the diagnosis and management of periampullary neoplasms. Annals of Surgical Oncology 9, 799–806 (2002). https://doi.org/10.1007/BF02574503
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF02574503