
Abstract
Objective
To evaluate the risk factors for postextubation laryngeal stridor and its prevention by hydrocortisone in adult patients.Design: Prospective, randomized, double-blind, placebo controlled study.
Setting
Medical and surgical ICU of a tertiary teaching hospital.
Patients
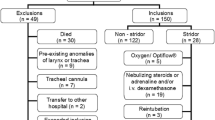
77 consecutive patients of both sexes, who had undergone tracheal intubation for more than 24 h and fulfilled the weaning criteria, were eligible for the study. Patients were excluded if they were less than 15 years of age, had a disease or the surgery of the throat, or had been extubated during the current hospitalization.
Intervention
The control group received placebo (normal saline 3 cc) and the experimental group received hydrocortisone 100 mg by intravenous infusion 60 min before extubation.
Main outcome measures
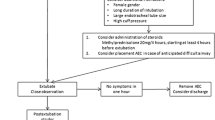
Patients were observed 24 h after extubation for symptoms or signs of laryngeal edema or stridor: prolonged inspiration with accessory usage of respiratory muscles or crowing sound with inspiration or reintubation.
Results
The overall incidence of postextubation stridor was 22% (17/77). Only one patient (1%), who belonged to the control group, needed reintubation. 39% of female patients and 17% of male patients developed stridor. The relative risk of females developing this complication was 2.29. 7/39 of the hydrocortisone group and 10/38 of patients in the control group developed postextubation stridor.Conclusions: Hydrocortisone did not significantly reduce the incidence of postextubation laryngeal edema or stridor. From the risk factors evaluated, we were unable to demonstrate a statistical correlation between postextubation stidor and the duration of the intubation, the patient's age, the internal diameter of the endotracheal tube, or the route of intubation. However, female patients were more likely to develop this complication.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Stauffer JL, Olson DE, Petty TL (1986) Complications and consequences of endotracheal intubation and tracheotomy. Am J Med 70:65–76
Bishop MJ, Weymuller EA, Fink BR (1984) Laryngeal effects of prolonged intubation. Anesth Analg 63:335–342
Kastanos N, Miro RE, Perez AM, Mir AX, Augusti-vidal A (1983) Laryngotracheal injury due to endotracheal intubation: incidence, evolution, and predisposing factors. A prospective longterm study. Crit Care Med 11:362–367
Burns HP, Dayal VS, Scott A, Peter Van Nostrand AW, Bryce DP (1979) Laryngotracheal trauma: observations on its pathogenesis and its prevention following prolonged orotracheal intubation in the adult. Laryngoscope 89:1316–1324
Donnelly WH (1969) Histopathology of endotracheal intubation. Arch Pathol Lab Med 88:511–520
Mackenzie CF, Shin B, McAslan TD, Blanchard CL, Cowley RA (1979) Severe stridor after prolonged endotracheal intubation using high-volume cuffs. Anesthesiology 50:235–239
Jordan WS, Grave CL, Elwyn RA (1970) New therapy for postintubation laryngeal edema and tracheitis in children. JAMA 212:585–588
Koka BV, Jeon JS, Andre JM, MacKay I, Smith RM (1977) Postintubation croup in children. Anesth Analg 56:501–505
Deming MV, Oech SR (1961) Steroid and antihistaminic therapy for postintubation subglottic edema. Anesthesiology 22:933–936
Haynes GR Jr, Murad F (1985) Andrenocorticotropic hormone: adrenocorticosteroids and their synthetic analogs: inhibitors of adrenocortical steroids biosynthesis. In: Gilman AG, Goodman LS, Rall TW, Murad F (eds) The pharmacological basis of therapeutics. McMillan, New York, pp 1459–1489
Biller HF, Bone RC, Harvey JE, Ogura JH (1970) Laryngeal edema: an experimental study. Ann Otol Rhinol 174:1084–1087
Woods CI, Postma DS, Prazma J, Sidman J (1987) Effects of dexamethasone and oxymetazoline on “postintubation croup”: a ferret model. Otolaryngol Head Neck Surg 96:554–558
Way WL, Sooy FA (1965) Histologic changes produced by endotracheal intubation. Ann Otol 744:799–813
Goddard JE, Phillipa OC, Marcy JH (1967) Betamethasone for prophylaxis of postintubation inflammation. Anesth Analg 46:348–353
Darmon JY, Rauss A, Dreyfuss D, Bleichner G, Elkharrat D, Schlemmer B, Tenaillon A, Brun-Buisson C, Huet Yann (1992) Evaluation of risk factors for laryngeal edema after tracheal extubation in adults and its prevention by dexamethasone. Anesthesiology 77: 245–251
Whited RE (1984) A prospective study of laryngeal sequelae in long-term intubation. Laryngoscope 94:367–377
Gaynor EV, Greenberg SB (1985) Untoward sequellae of prolonged intubation. Laryngoscope 95:1461–1467
Bishop MJ, Hibbard AJ, Fink BR, Vogel AM, Weymuller EA (1985) Laryngeal injury in a dog model of prolonged endotracheal intubation. Anesthesiology 62:770–773
Dixon TC, Sando MJW, Botton JM (1968) A report of 342 cases of prolonged endotracheal intubation. Med J Aust 2:529–533
Hedden M, Ersoz CJ, Donelly WH (1969) Laryngotracheal damage after prolonged use of orotracheal tubes in adults. JAMA 207:703–708
Harrison GA, Tonkin JP (1968) Prolonged (therapeutic) endotracheal intubation. Br J Anesth 40:241–248
Hawkins DB, Crockett DM, Shum TK (1983) Corticosteroids in airway management. Otolaryngol Head Neck Surg 91:593–596
Balestrieri F, Watson CB (1982) Intubation granuloma. Otolaryngol Clin North Am 15:567–579
Tellez DW, Galvis AG, Storgion SA, Amer HN, Hoseyni M, Deakers TW (1991) Dexamethasone in the prevention of postextubation stridor in children. J Pediatr 118:289–294
Author information
Authors and Affiliations
Additional information
Supported by grant from the National Science Council (NSC 85-2331-B-016-034)
Rights and permissions
About this article
Cite this article
Ho, L.I., Harn, H.J., Lien, T.C. et al. Postextubation laryngeal edema in adults risk factor evaluation and prevention by hydrocortisone. Intensive Care Med 22, 933–936 (1996). https://doi.org/10.1007/BF02044118
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF02044118