
Abstract
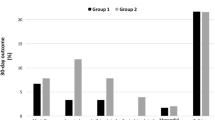
Between 1986 and 1994 we identified 57 patients who underwent carotid endarterectomy (CEA) and coronary artery bypass grafting (CABG) during the same hospitalization. Simultaneous CABG and CEA was performed in 28 patients (mean age 70.5 years, 58% male). Indications for CABG in these patients were myocardial infarction in two, crescendo angina in 19, congestive heart failure in two and left main or triple-vessel coronary artery disease noted during carotid preoperative evaluation in five. Indications for CEA were transient ischemic attack (TIA) in 12, crescendo TIA in six, cerebrovascular accident (CVA) in five, and asymptomatic stenosis in five. There were no postoperative myocardial infarctions or perioperative deaths. Two patients developed atrial fibrillation, and four patients had CVAs (two were ipsilateral to the side of CEA). Twenty-nine patients underwent staged procedures (i.e., not performed concomitantly but during the same hospitalization). Indications for CABG and CEA were comparable to those in the group undergoing simultaneous procedures. In 17 patients CEA was performed before CABG. There was a single CVA, the result of an intracerebral hemorrhage. Five of the 17 patients had a myocardial infarction and two died; one patient had first-degree heart block requiring a pacemaker. Four additional patients developed atrial fibrillation, one of whom required cardioversion. The remaining 12 patients had CABG followed by CEA. There were no CVAs, myocardial infarctions, arrhythmias, or deaths in this subgroup. These data demonstrate that the performance of simultaneous CABG and CEA procedures is associated with increased neurologic morbidity (14.3%), both ipsilateral and contralateral to the side of carotid surgery in contrast to staged CABG and CEA (3.4%). In addition, when staged carotid surgery preceded coronary revascularization in those with severe coronary artery disease, the combined cardiac complication and mortality rate was significantly higher than when coronary revascularization preceded CEA. This evidence suggests that when CABG and CEA must be performed during the same hospitalization, the procedures should be staged with CABG preceding CEA.
Similar content being viewed by others

References
Ennix CL, Lawrie GM, Morris GC, et al. Improved results of carotid endarterectomy in patients with symptomatic coronary artery disease: An analysis of 1546 consecutive carotid operations. Stroke 1979;10:122–125.
Brener BJ, Brief DK, Alpert J, et al. The risk of stroke in patients with asymptomatic carotid stenosis undergoing cardiac surgery: A follow-up study. J Vasc Surg 1987;5:269–279.
Bass A, Krupski WC, Dilley RB, et al. Combined carotid endarterectomy and coronary revascularization: A sobering review. Isr J Med Sci 1992;28:27–32.
Hertzer NR, Loop FD, Taylor PC, et al. Combined myocardial revascularization and carotid endarterectomy. J Thorac Cardiovasc Surg 1983;85:577–589.
Hertzer NR, Loop FD, Beven EG, et al. Surgical staging for simultaneous coronary and carotid disease: A study including prospective randomization. J Vasc Surg 1989;9:455–463.
Bernhard JM, Johnson WD, Peterson JJ. Carotid artery stenosis. Association with surgery for coronary artery disease. Arch Surg 1972;105:837–840.
Jones EL, Craver JM, Michalik RA, et al: Combined carotid and coronary operations: When are they necessary? J Thorac Cardiovasc Surg 1984;87:7–16.
Hertzer NR, Beven EG, Young JR, et al. Coronary artery disease in peripheral vascular patients. Ann Surg 1984;199:223–233.
Imparato AM, Ramirez A, Riles TS, et al. Cerebral protection in carotid surgery. Arch Surg 1982;117:1073–1076.
Rizzo RJ, Whittemore AD, Couper GS, et al. Combined carotid and coronary revascularization: The preferred approach to the severe vasculopathy. Ann Thorac Surg 1992;54:1099–1109.
McCrory DC, Goldstein LB, Samsa GP, et al. Predicting complications of carotid endarterectomy. Stroke 1993;24:1285–1291.
Sundt TM, Sandok BA, Whisnant JP. Carotid endarterectomy. Complications and preoperative assessment of risk. Mayo Clin Proc 1975;50:301–306.
Barnes RW, Marszalek PB. Asymptomatic carotid disease in the cardiovascular surgical patient: Is prophylactic endarterectomy necessary? Stroke 1981;12:497–500.
Furlan AJ, Craciun R. Risk of stroke during coronary artery bypass graft surgery in patients with internal carotid artery disease documented by angiography. Stroke 1985;16:797–799.
Lord RSA, Graham AR, Shanahan MX, et al. Rationale for simultaneous carotid endarterectomy and aortocoronary bypass. Ann Vasc Surg 1986;1:201–207.
Rosenthal D, Caudill DR, Lamis PA, et al. Carotid and coronary arterial disease: A rational approach. Am Surg 1984;50:233–235.
Chang BB, Darling RC, Shah DM, et al. Carotid endarterectomy can be safely performed with acceptable mortality and morbidity in patients requiring coronary artery bypass grafts. Am J Surg 1994;168:94–96.
Mehigan JT, Buch WS, Pipkin RD, et al. A planned approach to coexistent cerebrovascular disease in coronary artery bypass candidates. Arch Surg 1977;112:1403–1409.
Minami K, Sagoo KS, Breyman T, et al. Operative strategy in combined coronary and carotid artery disease. J Thorac Cardiovasc Surg 1988;95:303–309.
Pome G, Passini L, Colucci V, et al. Combined surgical approach to coexistent carotid and coronary artery disease. J Cardiovasc Surg 1991;32:787–793.
Perler BA, Burdick JF, Minken SL, et al. Should we perform carotid endarterectomy synchronously with cardiac surgical procedures? J Vasc Surg 1988;8:402–409.
Demopoulos LA, Tunick PA, Bernstein NE, et al. Protruding atheromas of the aortic arch in symptomatic patients with-carotid artery disease. Am Heart J 1995;129:40–44.
Brener BJ, Brief DK, Alpert J, et al. A four-year experience with preoperative noninvasive carotid evaluation of two thousand twenty-six patients undergoing cardiac surgery. J Vasc Surg 1984;1:326–338.
Author information
Authors and Affiliations
About this article
Cite this article
Giangola, G., Migaly, J., Riles, T.S. et al. Perioperative morbidity and mortality in combined vs. staged approaches to carotid and coronary revascularization. Annals of Vascular Surgery 10, 138–142 (1996). https://doi.org/10.1007/BF02000757
Issue Date:
DOI: https://doi.org/10.1007/BF02000757