
Summary
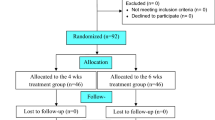
In a prospective randomized multicenter trial for the therapy of erythema migrans, 40 patients received ceftriaxone 1 g daily for 5 days and 33 patients obtained phenoxymethylpenicillin, 1 million units 3 times daily, for 12 days. Follow-up was for a mean of 10±5 months. Eight oral penicillin recipients (24%) and six ceftriaxone recipients (15%) developed minor consecutive manifestations. Two ceftriaxone and one penicillin recipient(s) still had elevated IgG antibody titers 10 to 20 months after therapy.Borrelia burgdorferi could be isolated from the erythema migrans in 29 out of 56 patients (52%) before therapy and in one oral penicillin recipient but none of 24 other patients after therapy. Ceftriaxone was superior to oral penicillin in a subgroup of patients with more than one symptom prior to therapy (p<0.01), but not in the overall evaluation of clinical, serological and bacteriological outcome data. Ceftriaxone ought to be preferred to oral penicillin in patients with more severe early Lyme borreliosis.
Zusammenfassung
In einer prospektiven, randomisierten Multizenter-Studie zur Therapie des Erythema migrans wurden 40 Patienten mit täglich 1 g Ceftriaxon intramuskulär über fünf Tage und 33 Patienten mit täglich 3 × 1 Mill. I. E. Phenoxymethylpenicillin über 12 Tage behandelt. Die Nachbeobachtung betrug durchschnittlich 10±5 Monate. Acht mit Penicillin (24%) und sechs mit Ceftriaxon behandelte Patienten (15%) entwickelten leichtere spätere Manifestationen. Zwei mit Ceftriaxon und ein mit Penicillin Behandelter wiesen erhöhte IgG Antikörper-Titer 10 bis 20 Monate nach Therapie auf.Borrelia burgdorferi konnte bei 29 von 56 Patienten (52%) vor und bei einem Patienten der Penicillingruppe, aber bei keinem Patienten der Ceftriaxongruppe nach Behandlung aus dem Erythema migrans isoliert werden. Ceftriaxon war dem Oral-Penicillin bei einer Untergruppe von Patienten mit mehr als einem Symptom vor Therapie überlegen (p<0,01), aber nicht bei der Gesamtauswertung klinischer, serologischer und bakteriologischer Erfolgsdaten. Ceftriaxon sollte dem oralen Penicillin bei Patienten mit schwererer früher Lyme-Borreliose vorgezogen werden.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Steere, A. C., Hutchinson, G. J., Rahn, D. W., Sigal, L. H., Craft, J. E., DeSanna, E. T., Malawista, E. E. Treatment of the early manifestations of Lyme disease. Ann. Intern. Med. 1983 (99) 22–26.
Steere, A. C., Malawista, S. E., Newman, J. H., Spieler, P. N., Bartenhagen, H. N. Antibiotic therapy in Lyme disease. Ann. Intern. Med. 93 (1980) 1–8.
Weber, K., Neubert, U. Thurmayr, R. Antibiotic therapy in early erythema migrans disease and related disorders. Zbl. Bakt. Hyg. A 263 (1986) 377–388.
Weber, K., Preac-Mursic, V., Neubert, U., Thurmayr, R., Herzer, P., Wilske, B., Schierz, G., Marget, W. Antibiotic therapy of early European Lyme borreliosis and acrodermatitis chronica atrophicans. Ann. NY Acad. Sci. 539 (1988) 324–345.
Berger, B. W. Treatment of erythema chronicum migrans of Lyme disease. Ann. NY Acad. Sci. 539 (1988) 346–351.
Weber, K. Erythema-chronicum-migrans-Meningitis — eine bakterielle Infektionskrankheit? Münch. Med. Wochenschr. 116 (1974) 1993–1998.
Steere, A. C., Batsford, W. P., Weinberg, M., Alexander, J., Berger, H. J., Wolfson, S., Malawista, S. E. Lyme carditis: cardiac abnormalities of Lyme disease. Ann. Intern. Med. 93 (1980) 8–16.
Weber, K., Bratzke, H. J., Neubert, U., Wilske, B., Duray, P. H. Borrelia burgdorferi in a newborn despite oral penicillin for Lyme borreliosis during pregnancy. Ped. Infect. Dis. 7 (1988) 286–289.
Dattwyler, R. J., Halperin, J. J. Failure of tetracycline therapy in early Lyme disease. Arthritis Rheum. 30 (1987) 448–450.
Johnson, R. C., Kodner, C., Russell, M. In vitro andin vivo susceptibility of the Lyme disease spirochete,Borrelia burgdorferi, to four antimicrobial agents. Antimicrob. Agents. Chemother. 31 (1987) 164–167.
Preac-Mursic, V., Wilske, B., Schierz, G., Holmburger, M., Süss, E. In vitro andin vivo susceptibility ofBorrelia burgdorferi.Eur. J. Clin. Microbiol. 6 (1987)424–426
Luft, B. J., Volkman, D. J., Halperin, J. J., Dattwyler, R. J. New chemotherapeutic approaches in the treatment of Lyme borreliosis. Ann. NY Acad. Sci. 539 (1988) 352–361.
Dattwyler, R. J., Halperin, J. J., Volkman, D. J., Luft, B. J. Treatment of late Lyme borreliosis — randomised comparison of ceftriaxone and penicillin. Lancet i (1988) 1191–1194.
Weber, K., Neubert, U. Clinical features of early erythema migrans disease and related disorders. Zbl. Bakt. Hyg. A 263 (1986) 209–228.
Wilske, B., Schierz, G., Preac-Mursic, V., Weber, K., Pfister, H. W., Einhäupl, K. Serological diagnosis of erythema migrans disease and related disorders. Infection 12 (1984) 331–337.
Wilske, B., Schierz, G., Preac-Mursic, V., Pfister, H. W., Weber, K., v. Busch, K., Baruschke, A.: IgM and IgG immune response toBorrelia burgdorferi in erythema migrans and neuroborreliosis. Zbl. Bakt. Hyg. A. (in press).
Wilske, B., Schierz, G., Preac-Mursic, V., von Busch, K., Kühbeck, R., Pfister, H. W., Einhäupl, K. Intrathecal production of specific antibodies againstBorrelia burgdorferi in patients with lymphocytic meningoradiculitis (Bannwarth's syndrome). J. Infect. Dis. 153 (1986) 304–314.
Preac-Mursic, V., Wilske, B., Schierz, G. EuropeanBorrelia burgdorferi isolated from humans and ticks: Culture conditions and antibiotic susceptibility. Zbl. Bakt. Hyg. A 263 (1986) 112–118.
Weber, K.: Clinical differences between European and North-American Lyme borreliosis — a review. Zbl. Bakt. Hyg. A (in press).
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Weber, K., Preac-Mursic, V., Wilske, B. et al. A randomized trial of ceftriaxone versus oral penicillin for the treatment of early european lyme borreliosis. Infection 18, 91–96 (1990). https://doi.org/10.1007/BF01641422
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF01641422