
Abstract
The vast knowledge of the physiologic functions of zinc in at least 3000 proteins and the recent recognition of fundamental regulatory functions of zinc(II) ions released from cells or within cells links this nutritionally essential metal ion to numerous diseases. However, this knowledge so far has had remarkably limited impact on diagnosing, preventing, and treating human diseases. One major roadblock is a lack of suitable biomarkers that would detect changes in cellular zinc metabolism and relate them to specific disease outcomes. It is not only the right amount of zinc in the diet that maintains health. At least as important is the proper functioning of the dozens of proteins that control cellular zinc homeostasis, regulate intracellular traffic of zinc between the cytosol and vesicles/organelles, and determine the fluctuations of signaling zinc(II) ions. Cellular zinc deficiencies or overloads, a term referring to zinc concentrations exceeding the cellular zinc buffering capacity, compromise the redox balance. Zinc supplementation may not readily remedy zinc deficiency if other factors limit the capability of a cell to control zinc. The role of zinc in human diseases requires a general understanding of the wide spectrum of functions of zinc, how zinc is controlled, how it interacts with the metabolism of other metal ions, in particular copper and iron, and how perturbation of specific zinc-dependent molecular processes causes disease and influences the progression of disease.
Please cite as: Met. Ions Life Sci. 13 (2013) 389–414
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
The biochemistry of zinc deserves much more attention than it generally receives in textbooks in the biomedical sciences and in some parts of the scientific literature. There are historic reasons for this lack of coverage. Unlike iron, which was easily detected and analyzed in blood and tissues due to the color of its complexes, zinc compounds are colorless. Therefore the field of zinc biology developed much later and only with the advent of new methods to analyze zinc in biological material. Also, unlike iron, where a large amount is found in heme, zinc is not predominantly part of a single substance but instead serves as a cofactor of at least 3000 human proteins. This distribution among so many proteins dilutes zinc and requires sensitive methods for the speciation and characterization of proteins. Zinc is involved in a much wider variety of processes and molecular mechanisms than vitamins and other cofactors with more specific chemical functions. The notion of zinc being a trace metal also somewhat confuscates the issues at hand. While the total amount of zinc in a human (70 kg) is 2–3 g and about as much as that of iron, cellular zinc ion concentrations are rather high, almost as high as those of major metabolites such as ATP.
A multi-authored text summarizes the knowledge accumulated since the field was last reviewed two decades ago in terms of the biochemical basis of zinc physiology as it relates to the numerous functions of zinc in metalloenzymes and transcription factors [1,2]. What has changed in the time between these accounts is the increase of the number of zinc proteins by one order of magnitude, demonstrating a much more general role of zinc in protein structure and in protein-protein interactions, an understanding of the biological and chemical aspects of how cellular zinc is controlled (zinc homeostasis), and the discovery that zinc(II) ions function in cellular regulation and information transfer. All these advances demonstrate that the present knowledge has by far surpassed the already impressive zinc biochemistry, which in 1993 was deemed to be, based on functions of zinc, “too numerous to cite” [2].
The implications of zinc biology for human health are enormous as about half of the world’s population is believed to be at risk for zinc deficiency [3]. The World Health Organization (WHO) has identified zinc deficiency as the fifth most important risk factor for morbidity and mortality in developing countries (11th worldwide) [4]. The figure translates into 3.2% of all lost disability-adjusted life years (DALYs). These estimates are derived primarily from the incidence of infectious and parasitic diseases due to compromised immune functions in zinc deficiency. Clearly, this measured outcome is far from inclusive. It does not take into account the functions of zinc in human memory acquisition and storage, behavior, growth retardation and development, delayed wound healing, the effects of environmental exposures to substances interfering with zinc metabolism, or the role of zinc in aging and in chronic diseases, such as cancer, diabetes, and neurodegeneration.
Rather than trying to summarize all the functions of zinc in physiology, which would be an immense task well beyond the scope of this chapter, the subject matter is approached by discussing the general significance of zinc in biochemistry for health and the specific involvement of zinc in pathophysiology and diseases at the molecular level. This approach will necessitate a certain degree of selectivity when referencing from the immense literature.
2 Zinc Biochemistry
Almost all our knowledge about the molecular roles of zinc is based on the interaction of zinc with proteins. Whether any interactions with other biomolecules are important is not known. Zinc has a role in enzymatic catalysis and in the structure and regulation of proteins. The coordination chemistry of zinc in proteins has been discussed in detail [5]. A major aspect of the cellular biology of zinc includes the storage of zinc(II) ions in cellular vesicles/organelles, in which relatively high concentrations can be reached and from which zinc(II) ions are released in a controlled way. In this regard, zinc resembles calcium and is quite different from iron, which uses redox chemistry of the central atom and a protein (ferritin) for storage and release.
2.1 Zinc in Enzymes and Proteins
Discoveries of zinc in numerous proteins demonstrated the key role of zinc for life. They occurred in the order of (i) zinc as a catalytic ion in enzymes, (ii) zinc in the structure of proteins, and (iii) zinc in the regulation of proteins [6]. By analyzing sequences of proteins from databases and detecting signatures for metal-binding sites with characteristically spaced amino acids providing the ligands, it became possible to estimate the number of zinc proteins in genomes, the so-called zinc proteome [7]. The estimate is about 3000 human zinc proteins [8].
2.1.1 Catalytic Zinc
The field of zinc metalloproteins began with the discovery of carbonic anhydrase as a zinc enzyme in 1939 [9]. Gradually, it became known that every enzyme class contains zinc enzymes. By far the largest number of zinc enzymes is in the class of hydrolases in the form of hundreds of zinc proteinases. Many proteinases are called metalloproteinases, e.g., matrix metalloproteinases (MMP), when in fact “metallo” stands for zinc only. For the most part, zinc enzymes seem to be absent in the major biochemical pathways of intermediary metabolism. This absence does not mean, however, that zinc has no roles in metabolism. It appears that rather than being a permanent constituent of metalloenzymes in these pathways, zinc has a role in controlling some of them.
2.1.2 Structural Zinc
Only a few structural zinc sites in enzymes were known before zinc finger proteins were discovered in 1986 [10]. The discovery revealed a new principle, namely the widespread use of zinc in proteins – which for the most part are not enzymes – to form domains for interacting with and recognizing DNA (transcription factors)/RNA, other proteins, or lipids. Many additional “zinc finger motifs” were found, thus establishing zinc as an important metal ion in the tertiary structure of proteins and for the interaction of proteins, the interactome. Also, zinc participates in the interaction between peptide chains and determines the quaternary structure of some proteins. How many of these zinc-binding sites at the interface between subunits exist is presently unknown, leaving a final count open with regard to the already remarkably high number of zinc-requiring proteins.
2.1.3 Regulatory Zinc
A regulatory role of zinc in protein structure – as opposed to a role of zinc as a permanent cofactor in regulatory proteins – is not as firmly defined as the literature indicates. In contrast to catalytic and structural zinc in proteins, where sites are thought to be always fully occupied with zinc, regulation requires zinc association and dissociation. With the exception of metallothionein, variable zinc contents of proteins as a function of physiological changes have not been established unequivocally.
Since there is now evidence for zinc(II) ions being signaling ions in the cell, this issue is receiving renewed scrutiny. Some zinc-binding sites satisfy criteria for serving in regulation, which occurs at remarkably low zinc(II) ion concentrations and with controlled release of zinc(II) ions. The proteins targeted and their coordination sites are the subject of recent investigations and include many proteins that were not known to be zinc proteins but bind zinc in their active sites very tightly and need to be activated by removal of the inhibitory zinc [11,12].
2.2 Zinc in Vesicles: Intracellular and Intercellular Signaling with Zinc(II) Ions
Mainly by employing histological staining techniques, it was recognized that many cells contain zinc(II) ions that apparently are not protein-bound [13]. These zinc(II) ions are found predominantly in intracellular compartments. From vesicular/organellar stores, tightly controlled processes release zinc(II) ions into the cytosol or into the extracellular space. Examples of zinc secretion from cells are the exocytosis of vesicles loaded with zinc in specialized neurons in the hippocampus, in pancreatic β-cells of the islets of Langerhans, and in epithelial cells of mammary glands [14]. Other cells secreting zinc(II) ions include somatotrophic cells in the pituitary gland, pancreatic acinar cells, Paneth cells in the crypts of Lieberkühn, cells of the tubuloacinar glands of the prostate, epithelial cells of the epididymal ducts, and osteoblasts [13]. Zinc(II) ions are also released intracellularly from the endoplasmatic reticulum [15]. Together, these and additional findings led to the concept that zinc(II) ions are messengers in cellular control and in intra- and intercellular communication [16,17]. The targets of these regulatory zinc(II) ions seem to be primarily proteins, again linking zinc to the functions of proteins. The types of functions of zinc(II) ions secreted from cells are the subject of present investigations. They include the modulation of postsynaptic receptors (neurons), supplying the milk with zinc (mammary gland epithelial cells), and, more speculative, keeping secreted enzymes inhibited (pancreatic acinar cells and prostate epithelial cells), preventing proteins from forming amyloids (pancreatic β-cells) or simply being bactericidal. Within cells, the released zinc(II) ions affect many signaling pathways [18]. Altered signal transduction activity associated with changed phosphorylations of proteins and the very tight inhibition of several protein tyrosine phosphatases indicate a role of zinc in phosphorylation signaling and suggests even more abundant interactions of zinc with proteins than based on the estimate of 3000 human proteins [19–24]. The regulatory functions of zinc depend on how cellular zinc homeostasis is controlled and at which amplitudes and frequencies zinc(II) ion transients occur [25].
2.3 Cellular Zinc Homeostasis
Proper control of cellular zinc is critical for the balance between health and disease. How this control is achieved at the molecular level has been the subject of the latest phase of biological zinc research. Very tight control of cellular zinc is necessary to make the right amount of zinc available for protein structure and function, folding, and aggregation and to prevent zinc from interfering with the metabolism of other metal ions. The number of proteins involved in controlling cellular zinc and the fact that proteins control zinc subcellularly is remarkable and attests to the importance of this transition metal in biology. In humans, ten proteins of the ZnT family (SLC30A) export zinc from the cytosol, either out of the cell or into vesicles/organelles, fourteen proteins of the Zip family (SLC38A) import zinc into the cytsol from the extracellular space or from vesicles/organelles, and at least a dozen metallothioneins (MTs) buffer and translocate zinc [26–28]. Another major factor in the control of cellular zinc is the role of metal response element-binding transcription factor-1 (MTF-1) [29], which is a sensor of elevated zinc(II) ion concentrations and regulates zinc-dependent gene expression. In addition to this direct role of zinc in gene expression, there are multiple effects on signal transduction pathways. Accordingly, many investigations using transcriptomics demonstrated that variation of zinc concentrations affects a myriad of gene products.
The zinc homeostatic proteins have dynamic coordination environments with specific mechanisms for handling transition metal ions [30,31]. MTs, for instance, have different binding constants for the seven zinc(II) ions and carry, release, and accept zinc ions dependent on cellular conditions [32,33]. In addition, they are redox-active zinc proteins. Zinc itself, on the contrary, is redox-inert. In MTs, the oxidation of the sulfur donors in the cysteine ligands of zinc causes zinc dissociation while the reduction of the oxidized cysteines generates zinc-binding capacity [34]. This property establishes redox cycles that link redox changes and the availability of cellular zinc [35,36].
The zinc homeostatic proteins are integrated into metabolism and exquisitely controlled by major signal transduction pathways. Thus, they do not work in isolation and are not only involved in housekeeping of zinc but control zinc(II) ion fluxes for specific cellular functions. Aside from compiling the “parts list” of proteins involved in cellular zinc homeostasis, significant advances have been made in understanding the concentrations at which cellular zinc is controlled. In contrast to other metal ions such as magnesium and calcium, most of the zinc is protein-bound with high affinity. The consequence is that only picomolar concentrations are in the form of non-protein-bound “free” zinc(II) ions [37]. But this pool of zinc is not negligible and undergoes controlled fluctuations [38]. Minute increases of cytosolic free zinc(II) ion concentrations have potent biological effects, which led to the concept of free zinc(II) ions being cellular signaling ions at much lower concentrations than signaling calcium(II) ions. In fact, the two ions complement each other in signaling and their different coordination chemistries allow signaling with metal ions over a wide range of concentrations [39]. Zinc buffering determines the amplitudes of the zinc(II) ion transients, and ultimately cellular zinc deficiencies and overloads [37].
Owing to the fact that many proteins bind zinc, the overall cellular zinc buffering capacity is high but only the cellular zinc buffering capacity in the range of physiological zinc(II) ion concentrations is important. This buffering capacity is rather limited. Compromising it, e.g., by decreasing the concentrations of critical sulfhydryls involved in binding zinc, results in higher free zinc(II) ion concentrations with functional consequences. About a third of the cellular zinc buffering capacity relies on sulfhydryl donors (thiols) as zinc-binding ligands [21]. Some environmental agents and therapeutic drugs react with thiols and make fewer thiols available for zinc buffering. Such reactions change the zinc buffering capacity and increase the availability of free zinc(II) ions, which then bind to and change the functions of proteins that are not targeted under physiological conditions. This issue can hardly be over-emphasized because it demonstrates that factors other than zinc itself affect zinc-dependent functions. The concept of metal buffering in biology includes dynamic changes in buffering capacity. A unique feature in the cellular control of zinc and calcium is muffling, which refers to the transport of zinc(II) ions into vesicles/organelles and out of the cell. Muffling also contributes to buffering because the activity of transporters increases or decreases the cellular metal ion concentrations [28]. Thus, the capacities of the transport systems and the vesicular stores also contribute to zinc buffering.
A central regulatory hormone of zinc metabolism akin to hepcidin in iron metabolism is not known. Knowledge about systemic control of zinc is lacking except for the acute phase response where adrenocorticotropic hormone (corticotropin, ACTH) decreases zinc in the blood [40].
2.4 Zinc and Oxidoreduction (Redox)
Zinc occurs as the redox-inert zinc(II) ion in biology. Because of this, the often quoted antioxidant properties of zinc can be indirect only, i.e., pro-antioxidant [41]. Zinc has this property only in a certain range of concentrations. Outside this range, it is a pro-oxidant, also by indirect mechanisms [41]. Cellular zinc deficiency and zinc overload cause oxidative stress. These opposing effects demonstrate a major function of zinc in redox metabolism and how important it is to control cellular zinc(II) ion concentrations in the correct range. The pro-antioxidant effects of zinc are due to (i) binding to and protecting free sulfhydryls against oxidation, (ii) competing with redox-active transition metal ions and suppressing the production of damaging free radicals, and (iii) inducing the synthesis of antioxidants, such as the expression of genes coding for antioxidant enzymes through MTF-1 and Nrf-2 (NF-E2-related factor) dependent gene transcription. Zinc deficiency compromises these three functions and therefore constitutes a pro-oxidant condition that can trigger a cascading effect: oxidative stress releases zinc from zinc/thiolate coordination environments in proteins, such as metallothioneins and increases the oxidative stress through the actions of the released zinc if the buffering capacity is too weak. Pro-oxidant effects of zinc(II) ions at higher than normal concentrations have been linked to zinc inhibition of antioxidant enzymes, the mitochondrial respiratory chain with concomitant increased formation of reactive species, and other proteins, for example the cellular iron exporter ferriportin [42].
Biomarkers of oxidative stress or inflammation decreased when normal healthy, middle aged or elderly humans were supplemented with zinc [43,44]. Sufficient zinc may need to be present in cells before an oxidative insult occurs in order to support an antioxidant effect, e.g., liver protection against alcohol, cardiac protection (infarct size), vascular protection (postischemic injury), and protection of tissues against the oxidative stress of diabetic complications. In isolated cells and in mice, zinc deficiency exacerbates endothelial cell dysfunction through pro-inflammatory pathways that involve NF-κB and peroxisome proliferator-activated receptor (PPAR) signaling, while prior zinc supplementation reduces fatty acid or tumor necrosis factor α-induced oxidative stress [45,46].
2.5 Global Functions of Zinc
Globally, the pro-oxidant effects express themselves as cytotoxic, pro-inflammatory, and pro-apoptotic functions while the pro-antioxidant effects translate into cytoprotective, anti-inflammatory, and anti-apoptotic functions [41]. With molecular functions in so many proteins in metabolism and signal transduction, it is understandable that zinc is involved in proliferation, differentiation, and apoptosis of all cells with profound implications for healthy growth, renewal, and repair of cells. Zinc deficiency retards growth, compromises the immune and nervous systems, and affects virtually any other organ system. The most cited clinical manifestations in humans are skin lesions, depressed mental functions, impaired night vision, anorexia, hypogonadism, depressed wound healing, and changed immune functions. In animals, reduced growth, decreased food intake, alopecia, skin lesions (parakeratosis and hyperkeratinization), impaired skeletal development and abnormal gait and stance are observed. Zinc is involved in normal development through many specific zinc finger transcription factors, in genetics and epigenetics through zinc enzymes that control methylation of DNA and methylation and acetylation of histones, and in maintaining the integrity of DNA through its role in DNA repair enzymes.
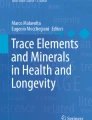
The involvement of zinc in the NF-κB pathway of inflammation serves to illustrate the widespread role of zinc in many signaling pathways. In this pathway, no less than 24 zinc(II) ions are involved in various aspects of protein structure (Figure 1). Human IKKβ has a zinc-binding site in its kinase domain, thus increasing the number of zinc(II) ions in this pathway to 25 [47]. This complexity and the pleiotropic functions of zinc demonstrate the inherent difficulties that investigators face in defining single modes of action for zinc or finding suitable biomarkers for either the cellular zinc status or specific zinc-dependent events.

Zinc proteins involved in turning off the NF-κB pathway of inflammation. A balance sheet of the number of zinc-containing proteins is given. The figures were kindly provided by Barbara Amann, Department of Chemistry, Goucher College, Towson, MD, USA.
One of the major issues in overcoming this difficulty is the lack of knowledge about the hierarchy of cellular zinc distribution under zinc-limiting conditions. Do some proteins hold on to their zinc whereas others yield their zinc to support more crucial functions? Or are all zinc-dependent proteins affected to the same extent? Are vesicular pools of stored zinc(II) ions and signaling functions affected first before the functions of zinc metalloproteins are compromised? Of course, such questions need to be asked for systemic zinc homeostasis as well: Which organs/tissues yield their zinc first and are therefore primarily affected by zinc deficiency? Compartmental models have described re-distribution of zinc from the bone/skeleton to the liver, but answers lie in the affinities of zinc for cellular proteins and the kinetics of cellular proteins that re-distribute zinc.
With this knowledge, it is clear that the subject of zinc in organ pathophysiology and disease remains largely phenomenological as it has rarely been possible to relate pathology to single or specific zinc-dependent molecular events. It would be, however, a severe mistake to conclude that the zinc status is not a major determinant in the etiology and the progression of diseases. Unfortunately, such a conclusion seems to be the prevailing assessment of a large part of the medical community due to the absence of any suitable clinical marker of cellular zinc status.
3 Zinc in Organ Pathophysiology
The following short summaries are merely snapshots of examples where the field has matured to indicate specific roles of zinc in organ pathophysiology and diseases. In most instances, pathways common to all cells are discussed in the literature of specific disciplines, but the knowledge applies across disciplines and will become the focus of zinc biology in the years to come. Challenges remain to tease apart the specific roles of zinc in zinc-dependent molecular pathways from the myriad of cellular functions of zinc. The involvement of zinc in the NF-κB pathway serves to illustrate this point (see Figure 1). The following summaries remain limited in scope as they focus on recently emerging general principles involving zinc(II) ion fluxes rather than focusing on zinc metalloproteins or the many interactions of zinc with membrane ion channels and other membrane proteins. Some topics will be treated only cursorily in order to keep a focus on molecular events and to avoid too much phenomenology. Comprehensive reviews on most of the topics will be cited.
3.1 Liver and Gastrointestinal System
The liver is a central organ in zinc distribution. Therefore, liver disease can affect zinc-dependent functions of many other organs and can lead to zinc deficiency [48]. In zinc deficiency caused by factors other than liver disease, the liver is less protected against various insults. Early observations indicated marked abnormalities of zinc metabolism in post-alcoholic (Laennec’s) cirrhosis with low serum and liver zinc and zincuria that correlated with the severity of the disease. A considerable improvement of liver function was noted when patients were supplemented with zinc and it was suggested that alcoholic liver disease is a conditioned zinc deficiency [49,50]. These observations have been confirmed repeatedly and demonstrate the therapeutic potential of zinc [51]. Alcohol consumption is also a risk factor for the severity of hepatitis C. The hepatitis C virus increases hepatic mitochondrial oxidative stress, thereby sensitizing hepatocytes to further oxidative insults from excessive alcohol consumption [52]. Nutritional and conditioned zinc deficiencies, which are pro-oxidative conditions, are therefore cumulative risk factors for liver disease. Zinc is effective in treating alcoholic and viral liver disease. In liver regeneration, the zinc transporter Zip14, which also transports non-transferrin bound iron, is upregulated. The additional cellular influx of zinc affects the phosphorylation of the hepatocyte growth factor receptor c-Met via inhibiting its dephosphorylation by protein tyrosine phosphatase-1B (PTP-1B) [53].
The gastrointestinal tract is equally important in the systemic control of zinc because it is the main organ for zinc uptake, which increases under zinc deficiency, as well as zinc excretion. Body zinc is a rather closed system where only a few milligrams (one thousandth of the total of 2–3 g) need to be replenished every day. Additional conservation of body zinc is afforded through re-uptake of the zinc secreted from the salivary glands, stomach, bile, and pancreas. Paneth cells located in the crypts of Lieberkühn in the small intestine secrete zinc(II) ions that are thought to be adjuvants to the microbicidal properties of secreted defensin peptides (cryptidins) [54].
3.2 Cardiovascular and Pulmonary System
The cellular role of zinc in protecting the vasculature and the extracellular role of zinc in hemostasis have implications for atherosclerosis and thrombosis. Zinc deficiency is associated with bleeding and clotting abnormalities through the involvement of zinc in platelet aggregation, coagulation, anticoagulation and fibrinolysis [55]. Beyond these roles with significance for cardiovascular disease, zinc has been implicated in congestive heart failure, myocardial infarction, arrhythmias, and in diabetic cardiomyopathy through its involvement in diabetes [56]. Numerous investigations support a role of zinc in the pathways leading to heart disease. Some human zinc supplementation trials have shown positive effects on clinical parameters related to heart disease although the lack of suitable biomarkers of zinc status remains a serious issue in interpreting the findings [57]. Experiments with rats demonstrated that suboptimal dietary intake of zinc promotes vascular inflammation and atherogenesis by affecting lipoprotein levels and by enhancing proliferation of vascular smooth muscle cells [58,59]. A proteomics analysis of the rats has already provided significant insights into the pathways involved [60].
The lung epithelium and endothelium have been the subject of extensive investigations with regard to zinc [61,62]. As is the case in many other tissues, zinc chelation and zinc deficiency render the lung endothelium susceptible to injury, whereas zinc(II) ions released in the cell have a protective effect, though this effect is clearly a matter of the amount of zinc released because amounts that exceed the cellular zinc buffering capacity cause injury. The investigations have demonstrated that the zinc/thiolate clusters of metallothionein are oxidized in vivo and serve as a source of zinc(II) ions by converting redox signals into zinc signals [63,64]. Hormones and agents that stimulate the cellular production of nitric oxide (NO), hydrogen peroxide, or other reactive species release cellular zinc(II) ions. The pathway with oxidative mobilization of zinc from metallothionein and subsequent zinc inhibition of enzymes operates in many tissues [11].
Hormone → NO (reactive species) → Zn/S (metallothionein) → Zn2+ → inhibition of enzymes
The central role of metallothionein in this pathway draws attention to the many factors involved when it serves as a source of zinc released in cells. The differential gene expression of the about twelve human metallothioneins in tissues, their amounts, metal loads, and genetics, and their different reactivites towards thiol-reactive agents all determine the balance between cytoprotective and cytotoxic functions of zinc [65,66]. The roles of metallothioneins in diseases cover most of the areas where zinc is involved and are not discussed here as they have been the subject of a recent monograph [67].
3.3 Immune System
Zinc has extensive roles in both the adaptive (specific) and the innate (non-specific) immune response at multiple levels, including the development of immune cells and gene expression in these cells that either affects the cells themselves or other cells through secreted cytokines [68]. Investigations with rodents demonstrated that immune responses decline significantly (>50%) in zinc deficiency [69]. Human zinc deficiency leads to atrophy of the thymus with apoptotic cell death of precursor lymphocytes as well as to deficits in erythropoiesis resulting in anemia [70]. T- and B-cells are the basis of the adaptive immune system. Zinc deficiency affects T-cell function more readily than B-cell function, but there are fewer B-cells formed because of the pro-apoptotic effect of zinc deficiency in lymphopoiesis. In human zinc deficiency, there is a shift in T-cell populations (Th1/Th2 balance) with the result of less interferon γ, interleukin-2, and TNFα being produced [71]. T-cell receptor-mediated T-cell activation also causes influx of extracellular zinc via the zinc transporter Zip6. The zinc inhibits subsynaptically the recruitment of the protein tyrosine phosphatase SHP-1 to the T-cell receptor [72]. Zinc is also needed to link the T-cell receptor CD4/CD8 and the tyrosine kinase Lck at protein interface sites between the two proteins and to induce the subsequent dimerization of this protein complex [73,74].
The innate immune response and inflammation constitutes the first line of defense of the host. It includes granulocytes, monocytes/macrophages, dendritic cells, and natural killer cells. Zinc is involved in the development, maturation, and function of all these cells. Zip6 is downregulated and cellular zinc decreases when toll-like receptor-4 of dendritic cells is stimulated [75]. Zip6 is needed to initiate zinc-dependent expression of major histocompatibility class II molecules. Zinc signaling in the immune system recently gained additional attention when a role of a protein kinase C-induced zinc(II) ion signal in the formation of neutrophil extracellular traps (NET) was discovered [76]. NETosis is a process, in which components such as DNA, chromatin, and proteins are released from cells to capture bacteria.
At the molecular level, a re-distribution of zinc is important for the immune response. The acute phase response to injury or infection decreases plasma zinc and increases cellular zinc [40]. In the liver, the pro-inflammatory cytokine interleukin-6 induces the expression of Zip14 and metallothionein, resulting in zinc influx and binding of zinc [77]. Subsequent to restriction of zinc in the blood, induced cellular zinc(II) ion fluxes are critical for functions of immune cells. FcεR1 receptor stimulation of mast cells increases cellular zinc(II) ions and so does stimulation of Jurkat T cells and monocytes [78,79]. The increase in mast cell zinc is important for allergic and autoimmune reactions (anaphylaxis, asthma, atopic dermatitis). Under conditions of zinc deficiency, the cellular re-distribution of zinc cannot take place, compromising the function of immune cells and increasing morbidity and mortality, especially in the critically ill with sepsis.
Another important observation is that the zinc transporter Zip8 is a transcriptional target of NF-κB [47]. Zinc transport through Zip8 suppresses pro-inflammatory conditions by zinc-dependent down-regulation of IκB (IKK) kinase activity. Zinc deficiency, in contrast, results in increased inflammation. Zip8 transports iron in addition to zinc [80].
Control of zinc homeostasis must be intact for proper immune functions. Zinc supplementation must be chosen carefully. Too much zinc causes copper deficiency, leukopenia, inhibits immune functions, and counteracts the acute phase response, which removes zinc from the circulation so that an invading pathogen does not have access to the zinc it needs. Zinc deficiency, on the other hand, increases bacterial invasion, in particular through an inflammatory response and the damaging effects on mucosal functions in the gastrointestinal and respiratory tracts [81]. These effects of zinc on the immune system are important for autoimmune diseases and neoplastic growth, and the efficacy of vaccinations in zinc-deficient individuals. Since zinc affects B-cells indirectly through its effect on T-cells, T-cell function should be optimal prior to vaccination.
3.4 Central and Peripheral Nervous System
In addition to the functions of zinc in every nerve cell, specialized neurons in the cerebral cortex store zinc in synaptic vesicles. Upon neuronal stimulation, zinc(II) ions are released from these vesicles and have multiple effects on the postsynaptic neurons. Therefore, control of synaptic zinc homeostasis is critical [82]. ZnT3 and MT3 (growth inhibitory factor) participate in the loading of the synaptic vesicles with zinc. The role of zinc(II) ions in synaptic neurotransmission and in excitotoxicity has been investigated extensively [83,84]. In a provocative article entitled “Do we need zinc to think?” the role of synaptic zinc was discussed [85]. It is becoming clear that synaptic zinc is involved in cortical plasticity affecting learning and memory and thus critical to the function of the hippocampus [86–88].
Stroke leads to ischemic neuronal injury and neurodegeneration [89]. Release of vesicular zinc associated with a stroke either affects the receptors at the postsynaptic neuron, such as NMDA channels, acid-sensing channels or GABAA receptors, or enters the postsynaptic neuron through the AMPA receptor and other calcium channels and acts intracellularly. In the neuron, zinc is also released from proteins by oxidative/nitrosative stress and acidosis, both of which are consequences of ischemia. The zinc(II) ions then enter mitochondria and inhibit the respiratory chain and antioxidant enzymes in the matrix with the result of mitochondria churning out more reactive oxygen species. Reperfusion following ischemia may augment the injury. The fine balance between zinc being released for protective functions and zinc being neurotoxic and the timing of the events make it very difficult to intervene therapeutically with either chelating agents or with zinc supplementation. The protective functions of zinc are evident in preconditioning that lowers the damage of an ensuing ischemic insult.
Zinc(II) ions released from vesicles through exocytosis and from cellular proteins by oxidative and nitrosative stress also contribute to neurotoxicity in traumatic brain injury and seizures [90–92].
For human brain health and for public health in general, it is important to realize that subclinical zinc deficiency impairs brain function [93].
3.5 Reproductive System
The observation of hypogonadism in zinc deficiency underscores the role of zinc in the reproductive system. The prostate, seminal fluid, and sperm are all very rich in zinc. Testicular zinc is required for spermatogenesis. The high amount of zinc in the prostate has been linked to the inhibition of mitochondrial aconitase for the production of high concentrations of citrate, which together with secrected zinc(II) ions is important for the physiology of the seminal fluid [94]. The high concentrations of zinc in prostate epithelial cells has been suggested to have antiproliferative and antitumor effects [94].
Significant advances have been made recently in elucidating the role of zinc in oocytes. At the end of maturation, mouse oocytes accumulate zinc and arrest at metaphase II after the first meiotic division. The fertilized oocytes then secrete zinc(II) ions with characteristic “zinc sparks” into the environment in order to lower intracellular zinc as a requirement for resuming the meiotic cell cycle [95]. Zinc is also involved in prophase I arrest through its effect on the MOS-MAPK pathway [96]. The authors comment on these remarkable findings in the following way: “These results establish zinc as a crucial regulator of meiosis throughout the entirety of oocyte maturation, including the maintenance of and release from the first and second meiotic arrest points.” Oocytes interact with cumulus cells and their cellular zinc content is intricately linked to the control of zinc homeostasis in cumulus cells [97].
These recent discoveries will impact significantly our knowledge about fertility, reproductive health, and embryonic development.
3.6 Sensory Systems
Among the sensory systems, most work has focused on the eye, where the retina and the retinal pigment epithelium/choroid complex are particularly rich in zinc [98,99]. Drusen, deposits in the retina, accumulate metal ions, suggesting a pathology similar to that of perturbation of metal homeostasis in the deposits of Alzheimer’s disease (see below). Dietary supplementation with zinc has become a method of treatment for age-related macular degeneration.
Loss of taste acuity is a clinical sign of zinc deficiency; hearing and smelling may also be affected. The olfactory bulb has very high zinc concentrations. Zinc is stored in vesicles of olfactory sensory neurons and can be released by electrical stimulation [100].
3.7 Other Systems
Other organ pathologies are also linked to zinc. There is a relative extensive literature on the role of zinc in skin diseases, wound healing, and bone health.
One additional general subject is the role of zinc in growth. Stunting is a consequence of zinc deficiency. Hypopituitarism was observed when human zinc deficiency was first described [101]. Therefore, research has addressed the role of zinc in the growth hormone (somatostatin) – insulin-like growth factor-1 (IGF-1) axis. Neuroendocrine cells store secreted proteins in dense cores of secretory granules. Zinc has a role in the secretory pathway of growth hormone [102]. It binds to growth hormone in a stoichiometry close to 1:1 in the secretory granules of the pituitary glands and induces the dimerization of the hormone [103,104]. And anterior pituitary cells, which release growth hormone, secrete zinc(II) ions [13]. Growth hormone then stimulates the synthesis of IGF-1 in the liver. The function of IGF-1 in tissues (muscle, bone) is zinc-dependent in pathways that also involve Zip7, Zip13, and Zip14 [19,105–107].
4 Zinc in Disease
4.1 Genetic Disease
In addition to the many changes in mRNA levels of zinc transporters observed in diseases, a number of mutations in zinc transporters are associated with human diseases (Table 1). A polymorphism of MT1A, an Asn27Thr substitution, changes the zinc-binding properties of the protein and is associated with type 2 diabetes and coronary heart disease [108]. Therefore, not only the availability of zinc in the diet but also the proteins that control cellular zinc homeostasis are important for health. Very little is known, however, about genetically determined differences in requirements for zinc or sensitivities towards an excess of zinc, nor have the genetics of the about 3000 human zinc proteins been much explored with regard to disease-causing mutations. In addition to the metabolic effects of mutations in zinc homeostatic proteins, the effect of such mutations on mental health are quite remarkable (Table 1). There are individuals with hyperzincemia [109]. Their high zinc in the blood is associated with calprotectinemia. Calprotectin is a protein of the S100 family that binds zinc. It is released from leukocytes in the acute phase response, and is involved in the innate immune response by binding manganese to deprive invading bacteria of this metal ion [110]. Hyperzincemic individuals present with the same symptoms as those with zinc deficiency.
4.2 Metabolic and Chronic Disease
4.2.1 Diabetes
A role of zinc in diabetes was considered for a long time but did not receive much attention because insights into molecular mechanisms were lacking, the many key functions of zinc in proteins and in the control of metabolism were not yet known, and cause versus effect could not be addressed [125–127]. Already in the 1930s, it was reported that the pancreas of cadavers from diabetics has only about half the amount of zinc compared to a healthy pancreas. Also, diabetics have significant hyperzincuria. However, a zinc deficiency is not readily established as reliable clinical markers of cellular zinc status are not available. Molecular studies in three areas have now significantly strengthened the link between zinc and diabetes. Zinc enhances the insulin action in peripheral tissues; it has a role in insulin storage and secretion in pancreatic β-cells; and it has pro-antioxidant functions in protecting the endocrine pancreas and peripheral tissues. The following summaries are based on recent reviews that cite the original work [112,128,129].
4.2.1.1 Zinc in Pancreatic β-Cell Physiology
In the granules of human pancreatic β-cells, human insulin is stored as a crystalline hexamer with two bound zinc ions. The zinc(II) ions that are co-secreted with insulin may affect glucagon secretion from α-cells, channel proteins, and/or prevent amyloidogenesis of co-secreted proteins. For instance, zinc inhibits the fibrillation of monomeric insulin and the formation of the dimer of the human islet amyloid polypeptide (IAPP, amylin).
The zinc transporter, ZnT8 provides zinc to the insulin-storing granules. A strong association between a polymorphism in the SLC30A8 gene (coding for ZnT8) and type 2 diabetes exists in different populations. ZnT8 with an Arg instead of a Trp at position 325 in its cytoplasmic domain increases the risk for diabetes by 53%. The risk allele is the most prevalent in populations, 55% in Asians, 75% in Europeans, and 95% in Africans. There is another variant with Gln at position 325. ZnT8 is also a significant autoantigen in type 1 diabetes and the single nucleotide polymorphism modulates the ZnT8 autoantibody specificities, indicating that the amino acid substitution has probably a critical role. Mice with a β-cell specific knock-out of ZnT8 have decreased zinc in the granules, altered insulin secretion, and mild glucose intolerance. Other zinc transporters participate in zinc metabolism of β-cells and some of them are associated with diabetes type 2.
4.2.1.2 Zinc in the Physiology of Cells Targeted by Insulin
Already in the 1960s it was shown that zinc has an insulin-sparing effect and that zinc-deficient rats are less sensitive to insulin. Zinc stimulates lipogenesis in isolated adipose tissue and affects glucose uptake in target tissues. Remarkably, for the culture of some mammalian cells, zinc can replace insulin in serum-free media. These insulin-mimetic effects of zinc are intracellular. Zinc increases the phosphorylation of the insulin/IGF-1 receptor and hence protein phosphorylations downstream in insulin signal transduction. One molecular target of zinc is the protein tyrosine phosphatase PTP-1B, a major regulator of the phosphorylation state of the insulin receptor. Zinc inhibits this enzyme with an apparent zinc binding constant of 15 nM [19,130].
4.2.1.3 Zinc and Oxidative and Carbonyl Stress
Diabetic hyperglycemia causes the glycation of proteins. The resulting advanced glycation end products (AGEs) increase reactive carbonyls, resulting in so-called carbonyl stress, which modifies, among other targets, sulfhydryl groups, lowers the zinc buffering/binding capacity, and mobilizes zinc from proteins [131]. Oxidative stress is a cause of insulin resistance [132]. The role of zinc in mediating oxidative stress thus establishes a causal link between zinc and insulin resistance.
4.2.2 Cancer
The roles of zinc in the immune system and thus immune surveillance and in maintaining genome stability are all relevant to cancer [133]. In addition, metastasis and angiogenesis require zinc. Matrix metalloproteinases are involved in metastasis. Cancer is often associated with low serum zinc, and with increased or decreased zinc in the malignant tissue. Zinc deficiency is a major risk factor for esophageal and oral small cell carcinoma and is involved in the development of chemically induced esophageal cancer [134,135]. It causes a pro-inflammatory environment through the expression of onco-micro RNAs [136]. The diminished cytoprotection in zinc deficiency constitutes a risk factor for reactions of biomolecules with environmental carcinogens and therefore has general implications for carcinogenesis.
Zinc chelation arrests cell growth. Zinc is required for cells to pass through the G1 and G2 restriction points of the cell cycle and for differentiation. In addition, mRNAs of specific cyclins decrease under zinc deficiency [137]. Fluctuations of free cellular zinc(II) ions have been observed at the two restriction points [38].
Changes in zinc and in zinc homeostatic proteins (zinc transporters and metallothioneins) have also been observed in many cancers. Zinc transporters have a role in cancer signaling through the apparent activation of protein tyrosine kinases [138]. Very tight zinc inhibition of protein tyrosine phosphatases supports such activation [22].
Zip6 (LIV-1) is an estrogen-induced protein in breast cancer cells [139]. Zip6 is regulated by the transcription factor STAT3 and has a role in the EMT (epithelial to mesenchymal transition) in metastasis [140]. The increase of cellular zinc(II) ions caused by Zip6 induction inhibits downstream events, in particular the expression of E-cadherin, which is involved directly in cell detachment and hence metastasis [141].
4.2.3 Neurodegeneration
Among the neurodegenerative diseases, Alzheimer’s disease (AD) received the most attention with regard to zinc’s involvement in both the Aβ and tau protein pathologies. The reason is that zinc and other metals (Fe, Cu) were found in the amyloid plaques of AD at relatively high concentrations [142]. This finding led to the hypothesis that Aβ disrupts the control of neuronal zinc homeostasis by sequestering metals and that inappropriately localized zinc leads to a loss of zinc’s function in neurotransmission. Zinc induces the aggregation of Aβ into an insoluble form, the processing of amyloid precursor protein (APP), the metabolism of iron and copper, and interferes with microtubule-associated tau, the protein forming neurofibrillary tangles, the second hallmark of AD pathology [143]. Elevated levels of zinc inhibit the iron exporter ferroportin, possibly leading to iron overload and associated oxidative stress in neurons [42].
A quite remarkable observation is the shared phylogenetic origin of some Zip proteins and the prion proteins [144]. A role of the prion protein in uptake of zinc into neuronal cells indicates functional significance for neurodegeneration [145].
4.3 Infectious Disease
With compromised immunity of the host in zinc deficiency, infection with parasites is a major health concern, in particular for those at risk: children, pregnant women, and the elderly. Treating and preventing diarrhea in children under the age of five with zinc is robust and saves a high number of lives in the developing world. There is correlative evidence between zinc deficiency and malaria, measles, HIV, tuberculosis, and respiratory tract infections such as pneumonia. However, evidence for efficacy of the treatment and prevention of these diseases with zinc is less clear [146].
5 General Conclusions
The importance of proper control of cellular zinc is being recognized in several specialized disciplines of academic medicine. Zinc is involved in pathways common to all cells and in virtually all aspects of molecular and cellular biology. While changed levels of zinc in diseases were mostly considered consequences of the diseases, causation is now indicated strongly in many cases. Zinc biology, therefore, will have a major impact on the practice of medicine in many disciplines, including those where the roles of zinc are not considered at present.
Translation of the knowledge into practice has been, and continues to be, hampered by the lack of suitable clinical markers, especially markers for milder forms of zinc deficiency [147]. Biomarker discovery can be better pursued now because many additional and wider functions of zinc are known. In particular the knowledge about proteins involved in zinc homeostasis raise expectations that biomarkers reflecting the zinc status akin to transferrin and ferritin in iron metabolism will be discovered. The majority of clinical cases of zinc deficiency present themselves with overt signs. Mild zinc deficiency, though known to affect the nervous and immune system, is generally not addressed in the clinical setting.
Blood zinc represents only about 0.1% of total body zinc and corresponds to about the amount of zinc replenished every day, but the requirements are different for children, pregnant and lactating women, the elderly, healthy and sick humans, and populations that are at risk for zinc deficiency. As a systemic marker, blood zinc it is not a sensitive marker for the cellular zinc status, in particular since acute infections can lower serum zinc and increase cellular zinc, cells differ in their zinc requirements and kinetics, and major functions of zinc are within cells. Zinc therapy is already proven to be effective in diseases, such as intestinal diseases, acrodermatitis enteropathica, transient neonatal zinc deficiency, and Wilson’s disease.
Although many deficits have been linked unequivocally to zinc deficiency and zinc appears to be a panaceum for a large number of ailments, zinc supplementation is often ineffective in reversing deficits [148]. This failure has perplexed some and is sometimes used to refute the hypothesis that zinc deficiency is the cause of a condition. However, there are multiple reasons for the occasional failure of reversing symptoms with zinc supplementation. The control of zinc metabolism is remarkably complex and encompasses competition with and interactions among other metal ions; zinc supplementation depends on the dose as too much zinc may have the opposite effects; and last but not least, restoration of function may require additional factors because other micronutrient deficiencies often accompany zinc deficiency.
Supplementing only zinc may not restore the control of cellular zinc homeostasis. Additional zinc may be a pro-oxidant and harmful under conditions of sustained oxidative stress when free zinc(II) ion concentrations are already higher than normal and the zinc buffering capacity is reduced. Under conditions such as oxidative stress, the binding capacity of cellular thiols is reduced and supplemental zinc may not be retained in the cells or bind to non-physiological targets with adverse side effects. Restoring control of cellular, not necessarily systemic, zinc homeostasis, restoring the cellular redox state, and addressing the factors that condition zinc deficiency (Table 2) seem to be a prerequisites to successful zinc therapy in the many conditions that may require zinc.
With the discovery of the many proteins controlling cellular zinc homeostasis and the genetics of these proteins, the focus of attention shifted from the presence or absence of zinc to the functions of the proteins that determine the cellular allocation of zinc to zinc proteins, re-distribute zinc under changing conditions, and, importantly, regulate the functions of zinc in intra- and intercellular communication. Specific roles of zinc in cellular signaling pathways are being identified and examined. Changed functions of zinc homeostatic proteins affect the redox state, inflammation, genetic stability, and cellular signaling and metabolism through altered cellular zinc metabolism.
- ACTH:
-
adrenocorticotrophic hormone, corticotropin
- AD:
-
Alzheimer’s disease
- AGE:
-
advanced glycation end product
- AMPA:
-
α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid
- APP:
-
amyloid precursor protein
- DALY:
-
disability-adjusted life years
- EMT:
-
epithelial-to-mesenchymal transition
- GABAA:
-
γ-aminobutyric acid A
- HIV:
-
human immunodeficiency virus
- IAPP:
-
islet amyloid polypeptide, amylin
- IGF-1:
-
insulin-like growth factor 1
- IKKβ:
-
IκB kinase β
- MMP:
-
matrix metalloproteinase
- MOS-MAPK:
-
mos (a protein serine/threonine kinase)-mitogen-activated protein kinase
- MRE:
-
metal response element
- MT:
-
metallothionein
- MTF-1:
-
metal response element (MRE)-binding transcription factor-1
- NET:
-
neutrophil extracellular trap
- NF-κB:
-
nuclear factor κ light-chain-enhancer of activated B cells
- NMDA:
-
N-methyl D-aspartate
- PPAR:
-
peroxisome proliferator-activated acceptor
- PTB-1B:
-
protein tyrosine phosphatase-1B
- TNFα:
-
tumor necrosis factor α
- WHO:
-
World Health Organization
- Zip:
-
Zrt-, Irt-like proteins
- ZnT:
-
zinc transporter
References
Zinc in Human Health, Ed L. Rink, IOS Press, Amsterdam, 2011, pp. 1–577.
B. L. Vallee, K. H. Falchuk, Physiol. Rev. 1993, 73, 79–118.
K. H. Brown, S. E. Wuehler, Zinc and Human Health: The Results of Recent Trials and Implications for Program Interventions and Research, Ottawa: Micronutrient Initiative, 2000, pp.1–69.
World Health Report 2002 – Reducing Risks, Promoting Healthy Life. Geneva: WHO, 2002, pp. 1–250.
D. S. Auld, BioMetals 2001, 14, 271–313.
W. Maret, Adv. Nutr. 2013, 4, 82–91.
W. Maret, J. Anal. At. Spectrom. 2004, 19, 15–19.
C. Andreini, L. Banci, I. Bertini, A. Rosato, J. Proteome Res. 2006, 5, 196–201.
D. Keilin, T. Mann, Nature 1939, 144, 442–443.
J. Miller, A. D. McLachlan, A. Klug, EMBO J. 1985, 4, 1609–1614.
W. Maret, C. Jacob, B. L. Vallee, E. H. Fischer, Proc. Natl. Acad. Sci. USA 1999, 96, 1936–1940.
W. Maret, BioMetals 2013, 26, 197–204.
G. Danscher, M. Stoltenberg, J. Cytochem. Histochem. 2005, 53, 141–153.
S. L. Kelleher, N. H. McCormick, V. Velasquez, V. Lopez, Adv. Nutr. 2011, 2, 101–111.
K. M. Taylor, S. Hiscox, R. I. Nicholson, C. Hogstrand, P. Kille, Sci. Signal. 2012, 5:ra11.
H. Haase, W. Maret, in Cellular and Molecular Biology of Metals, Eds R. Zalups, J. Koropatnick, Taylor and Francis, Boca Raton, 2010, pp. 179–210.
T. Fukada, S. Yamasaki, K. Nishida, M. Murakami, T. Hirano, J. Biol. Inorg. Chem. 2011, 16, 1123–1134.
D. Beyersmann, H. Haase, BioMetals 2001, 14, 331–341.
H. Haase, W. Maret, Exp. Cell Res. 2003, 291, 289–298.
H. Haase, W. Maret, J. Trace Elem. Med. Biol. 2005, 19, 37–42.
A. Krezel, Q. Hao, W. Maret, Arch. Biochem. Biophys. 2007, 463,188–200.
M. Wilson, C. Hogstrand, W. Maret, J. Biol. Chem. 2012 , 287, 9322–9326.
W. Maret, Pure Appl. Chem. 2008, 80, 2679–2687.
W. Maret, Metallomics 2010, 2, 117–125.
W. Maret, BioMetals 2009, 22, 149–157.
L. A. Lichten, R. J. Cousins, Annu. Rev. Nutr. 2009, 29, 153–176.
T. Fukada, T. Kambe, Metallomics 2011, 3, 662–674.
R. A. Colvin, W. R. Holmes, C. P. Fontaine, W. Maret, Metallomics 2010, 2, 306–317.
V. Günther, U. Lindert, W. Schaffner, Biochim. Biophys. Acta 2012, 1823, 1416–1425.
W. Maret, Y. Li, Chem. Rev. 2009, 109, 4682–4707.
W. Maret, J. Inorg. Biochem. 2012, 111, 110–116.
A. Krężel, W. Maret, J. Am. Chem. Soc. 2007, 129, 10911–10921.
W. Maret, J. Biol. Inorg. Chem. 2011, 16, 1079–1086.
W. Maret, B. L. Vallee, Proc. Natl. Acad. Sci. USA 1998, 95, 3478–3482.
W. Maret, Biochemistry 2004, 43, 3301–3309.
W. Maret, Antioxid. Redox Signal. 2006, 8, 1419–1441.
A. Krezel, W. Maret, J. Biol. Inorg. Chem. 2006, 11, 1049–1062.
Y. Li, W. Maret, Exp. Cell Res. 2009, 315, 2463–2470.
W. Maret, Proc. Natl. Acad. Sci. USA 2001 , 98, 12325–12327.
K. H. Falchuk, New Engl. J. Med. 1977, 269, 1129–1134.
W. Maret, Exp. Gerontol. 2008, 43, 363–369.
J. A. Duce, A. Tsatsanis, M. A. Cater, S. A. James, E. Robb, K. Wikhe, S. L. Leong, K. Perez, T. Johanssen, M. A. Greenough, H.-H. Cho, D. Galatis, R. D. Moir, C. L. Masters, C. McLean, R. E. Tanzi, R. Cappai, K. J. Barnham, G. D. Ciccotosto, J. T. Rogers, A. I. Bush, Cell 2010, 142, 857–867.
A. S. Prasad, B. Bao, F. W. J. Beck, P. Kucuk, F. H. Sarkar, Free Radic. Biol. Med. 2004, 37, 1182–1190.
A. S. Prasad, F. W. J. Beck, B. Bao, J. T. Fitzgerald, D. C. Snell, J. D. Steinberg, L. J. Cardozo, Am. J. Clin. Nutr. 2007, 85, 837–844.
B. Hennig, P. Meerarani, M. Toborek, C. J. McClain, Am J. Coll. Nutr. 1999, 18, 152–158.
H. Shen, E. Oesterling, A. Stromberg, M. Toborek, R. MacDonald, B. Hennig, J. Am. Coll. Nutr. 2008, 27, 577–587.
M.-J. Liu, S. Bao, M. Galvez-Peralta, C. J. Pyle, A. C. Rudawsky, R. E. Pavlovicz, D. W. Killilea, C. Li, D. W. Nebert, M. E. Wewers, D. L. Knoell, Cell Reports 2013, 3, 386–400.
K. Grüngreiff, D. Reinhold, in Zinc in Human Health, Ed L. Rink, IOS Press, Amsterdam, 2011, pp. 473–492.
B. L. Vallee, W. E. C. Wacker, A. F. Bartholomay, E. D. Robin, New Engl. J. Med. 1956, 255, 403–408.
B. L. Vallee, W. E. C. Wacker, A. F. Bartholomay, F. L. Hoch, New Engl. J. Med. 1956, 257, 1056–1065.
M. K. Mohammad, Z. Zhou, M. Cave, A. Barve, M. J. McClain, Nutr. Clin. Pract. 2012, 27, 8–20.
M. Korenaga, M. Okuda, K. Otani, T. Wang, Y. Li, S. A. Weinman, J. Clin. Gastroenterol. 2005, 39, S162–166.
T. B. Aydemir, H. S. Sitren, R. J. Cousins, Gastroenterology 2012 , 142, 1536–1546.
L. J. Giblin, C. J. Chang, A. F. Bentley, C. Frederickson, S. J. Lippard, C. J. Frederickson, J. Histochem. Cytochem. 2006, 54, 311–316.
T. T. Vu, J. C. Fredenburgh, J. I. Weitz, Thrombosis Haemost. 2013, 109, 421–430.
P. J. Little, R. Bhattacharya, A. E. Moreyra, I. L. Korichneva, Nutrition 2010, 26, 1050–1057.
M. Foster, P. Petocz, S. Samman, Atherosclerosis 2010, 210, 344–352.
J. H. Beattie, M.-J. Gordon, S. J. Duthie, C. J. McNeil, G. W. Horgan, G. F. Nixon, J. Feldmann, I.-S. Kwun, Mol. Nutr. Food Res. 2012, 56, 1097–1105.
E. H. Alcantara, M. Y. Shin, J. Feldmann, G. F. Nixon, J. H. Beattie, I. S. Kwun, Atherosclerosis 2013, 228, 46–52.
J. H. Beattie, M.-J. Gordon, G. J. Rucklidge, M. D. Reid, G. J. Duncan, G. W. Horgan, Y.-E. Cho, I.-S. Kwun, Proteomics 2008, 8, 2126–2135.
A. Q. Truong-Tran, J. Carter, R. Ruffin, P. D. Zalewski, Immunol. Cell Biol. 2001, 79, 170–177.
K. Thambiayya, A. M. Kaynar, C. M. St.Croix, B. R. Pitt, Pulm. Circ. 2012, 2, 443–451.
W. Maret, J. Nutr. 2000, 130, 1455S–1458S.
W. Maret, J. Nutr. 2003, 133, 1460S–1462S.
Y. Chen, Y. Irie, W. M. Keung, W. Maret, Biochemistry 2002, 41, 8360–8367.
Y. Li, W. Maret, J. Anal. At. Spectrom. 2008, 23, 1055–1062.
Metallothioneins in Biochemistry and Pathology, Ed P. Zatta, World Scientific Publishing Co., Singapore, 2008, pp. 1–320.
L. Rink, H. Haase, Trends Immunol. 2007, 28, 1–4.
P. J. Fraker, S. M. Haas, R. W. Luecke, J. Nutr. 1977, 107, 1889–1895.
P. J. Fraker, L. E. King, Annu. Rev. Nutr. 2004, 24, 277–298.
F. W. Beck, A. S. Prasad, J. Kaplan, J. T. Fitzgerald, G. J. Brewer, Am. J. Physiol. 1997, 272, E1002–1007.
M. Yu, W.-W. Lee, D. Tomare, S. Pryshchep, M. Czyzesnikiewicz-Guzik, D. L. Lamar, G. Li, K. Singh, L. Tian, C. M. Weyand, J. J. Goronzy, J. Exp. Med. 2011, 208, 775–785.
P. W. Kim, Z.-Y. J. Sun, S. C. Blacklow, G. Wagner, M. J. Eck, Science 2003, 301, 1725–1728.
J. Romir, H. Lilie, C. Egerer-Sieber, F. Bauer, H. Sticht, Y. A. Muller, J. Mol. Biol. 2007, 365, 1417–1428.
H. Kitamura, H. Morikawa, H. Kamon, M. Iguchi, S. Hojyo, T. Fukada, S. Yamashita, T. Kaisho, S. Akira, M. Murakami, T. Hirano, Nat. Immunol. 2006, 7, 971–977.
R. Hasan, L. Rink, H. Haase, Innate Immun. 2012, 19, 253–264.
J. P. Liuzzi, L. A. Lichten, S. Rivera, R. K. Blanchard, T. B. Aydemir, M. D. Knutson, T. Ganz, R. J. Cousins, Proc. Natl. Acad. Sci. USA 2005, 102, 6843–6848.
S. Yamasaki, K. Sakata-Sogawa, A. Hasegawa, T. Suzuki, K. Kabu, E. Sato, S. Kurasaki, M. Yamashita, K. Tokunaga, K. Nishida, T. Hirano, J. Cell Biol. 2007, 177, 637–645.
H. Haase, J. L. Ober-Blöbaum, G. Engelhardt, S. Hebel, A. Heit, H. Heine, L. Rink, J. Immunol. 2008, 181, 6491–6502.
C.-Y. Wang, S. Jenkitkasemwong, S. Duarte, B. K. Sparkman, A. Shawki, B. Mackenzie, M. D. Knutson, J. Biol. Chem. 2012, 287, 34032–34043.
D. L. Knoell, B. Y. Besecker, in Zinc in Human Health, Ed L. Rink, IOS Press, Amsterdam, 2011, pp. 254–267.
A. Takeda, M. Nakamura, H. Fujii, H. Tamano, Metallomics 2013, 5, 417–423, DOI 10.1039.c3mt20269k
S. L. Sensi, P. Paoletti, A. I. Bush, I. Sekler, Nat. Rev. Neurosci. 2009, 10, 780–791.
C. J. Frederickson, J.-Y. Koh, A. I. Bush, Nat. Rev. Neurosci. 2005, 6, 449–462.
Y. V. Li, C. J. Hough, J. M. Sarvey, SciSTKE 2003 (182), pe19.
A. S. Nakashima, H.-P. Wu, R. Dyck, in Zinc in Human Health, Ed L. Rink, IOS Press, Amsterdam, 2011, pp. 389–402.
E. Pan, X. Zhang, Z. Huang, A. Krezel, M. Zhao, C. E. Tinberg, S. J. Lippard, J. O. McNamara, Neuron 2011, 71, 1116–1126.
K. Toth, Annu. Rev. Nutr. 2011, 31, 139–153.
C. W. Shuttleworth, J. H. Weiss, Trends Pharmacol. Sci. 2011, 32, 480–486.
C. J. Frederickson, W. Maret, M. P. Cuajungco, The Neuroscientist 2004, 10, 18–25.
Y. Li, B. E. Hawkins, D. S. Prough, D. S. DeWitt, W. Maret, Brain Res. 2010, 1330, 131–141.
D. R. Morris, C. W. Levenson, Hindawi Publishing Corporation, J. Toxicology 2012, Article ID 785647.
H. Sandstead, J. Trace Elem. Biol. Med. 2012, 26, 70–73.
R. B. Franklin, L. C. Costello, Arch. Biochem. Biophys. 2007, 463, 211–217.
A. M. Kim, M. L. Bernhardt, B. Y. Kong, R. W. Ahn, S. Vogt, T. K. Woodruff, T. V. O’Halloran, ACS Chem. Biol. 2011, 6, 716–723.
B. Y. Kong, M. L. Bernhardt, A. M. Kim, T. V. O’Halloran, T. K. Woodruff, Biol. Reprod. 2012, 87, 11, 1–12.
R. S. Lisle, K. Anthony, M. A. Randall, F. J. Diaz, Reproduction 2013, 145, 381–390.
M. Ugarte, N. N. Osborne, Prog. Neurobiol. 2001, 64, 219–249.
N. Barzegar-Befroei, S. Cahyadi, A. Gango, T. Peto, I. Lengyel, in Zinc in Human Health, Ed L. Rink, IOS Press, Amsterdam, 2011, pp 530–553.
L. J. Blakemore, E. Tomat, S. J. Lippard, P. Q. Trombley, Metallomics 2013, 5, 208–213.
H. H. Sandstead, Adv. Nutr. 2013, 4, 76–81.
V. Petkovic, M. C. Miletta, P.-E. Mullis, in Developmental Biology of GH Secretion, Growth and Treatment, Vol. 23 of Endocr. Dev., Ed P.-E. Mullis, Karger, Basel, 2012, pp. 96–108.
P. C. Cunningham, M. G. Mulkerrin, J. A. Wells, Science 1991, 253, 545–548.
O. Thorlacius-Ussing, Neuroendocrinology 1987, 45, 233–242.
R. S. McDonald, J. Nutr. 2000, 130, 1500S–1508S.
K. M. Taylor, P. Kille, C. Hogstrand, Cell Cycle 2012, 11, 1–2.
T. Fukada, S. Hojyo, T. Furuichi, J. Bone Miner. Metab. 2013, 31, 129–135.
R. Giacconi, A. R. Bonfigli, R. Testa, C. Sirolla, C. Cipriano, M. Marra, E. Muti, M. Malavolta, L. Costarelli, F. Piacenza, S. Tesei, E. Mocchegiani, Mol. Genet. Metab. 2008, 94, 98–104.
B. Sampson, M. K. Fagerhol, C. Sunderkötter, B. E. Golden, P. Richmond, N. Klein, I. Z. Kovar, J. H. Beattie, B. Wolska-Kusnierz, Y. Saito, J. Roth, Lancet 2002, 360, 1742–1745.
S. M. Damo, T. E. Kehl-Fie, N. Sugitani, M. E. Holt, S. Rathi, W. J. Murphy, Y. Zhang, C. Betz, L. Hench, G. Fritz, E. P. Skaar, W. J. Chazin, Proc. Natl. Acad. Sci. USA 2013, 110, 3841–3846.
W. Chowanadisai, B. Lönnerdal, S. Kelleher, J. Biol. Chem. 2006, 281, 39699–39707.
F. Chimienti, J. Diabetes Invest. 2013, 3, 202–2011.
M. Quadri, A. Federico, T. Zhao, G. J. Breedveld, C. Battisti, C. Delnooz, L. A. Severijnen, L. Di Toro Mammarella, A. Mignarri, L. Monti, A. Sanna, P. Lu, F. Punzo, G. Cossu, R. Willemsen, F. Rasi, B. A. Oostra, B. P. van de Warrenburg, V. Bonifati, Am. J. Hum. Genet. 2012, 90, 467–477.
K. S. Burgdorf, A. P. Gjesing, N. Grarup, J. M. Justesen, C. H. Sandholt, D. R. Witte, T. Jorgensen, S. Madsbad, T. Hansen, O. Pedersen, Diabetologia 2012, 55, 105–113.
R. Giacconi, E. Muti, M. Malavolta, M. Cardelli, S. Pierpaoli, C. Cipriano, L. Costarelli, S. Tesei, V. Saba, E. Mocchegiani, Rejuvenation Res. 2008, 11, 297–300.
H. M. Ollila, P. Soronen, K. Silander, O. M. Palo, T. Kieseppä, M. A. Kaunisto, J. Lönnqvist, L Peltonen, T. Partonen, T. Paunio, Mol. Psychiatry 2009, 14, 351–353.
K. Wang, B. Zhou, Y. M. Kuo, J. Zemansky, J. Gitschier, Am. J. Hum. Genet. 2002, 71, 66–73.
S. Kury, B. Dreno, S. Bezieau, S. Giraudet, M. Kharfi, R. Kamoun, J. Moisan, Nature Genet. 2002, 31, 239–240.
D. M. Waterworth, S. L. Ricketts, K. Song, L. Chen, J. H. Zhao, S. Ripatti, Y. S. Aulchenko, W. Zhang, X. Yuan, N. Lim, J. Luan, S. Ashford, E. Wheeler, E. H. Young, D. Hadley, J. R. Thompson, P. S. Braund, T. Johnson, M. Struchalin, I. Surakka, R. Luben, K. T. Khaw, S. A. Rodwell, R. J. Loos, S. M. Boekholdt, M. Inouye, P. Deloukas, P. Elliott, D. Schlessinger, S. Sanna, A. Scuteri, A. Jackson, K. L. Mohlke, J. Tuomilehto, R. Roberts, A. Stewart, Y. A. Kesäniemi, R. W. Mahley, S. M. Grundy; Wellcome Trust Case Control Consortium, W. McArdle, L. Cardon, G. Waeber, P. Vollenweider, J. C. Chambers, M. Boehnke, G. R. Abecasis, V. Salomaa, M. R. Järvelin, A. Ruokonen, I. Barroso, S. E. Epstein, H. H. Hakonarson, D. J. Rader, M. P. Reilly, J. C. Witteman, A. S. Hall, M. J. Samani, D. P. Strachan, P. Barter, C. M. van Duijn, J. S. Kooner, I. Peltonen, N. J. Wareham, R. McPherson, V. Mooser, M. S. Sandhu, Artherioscler. Thromb. Vasc. Biol. 2010, 30, 2264–2276.
N. Carrera, M. Arrojo, J. Sanjuán , R. Ramos-Ríos, E. Paz, J. J. Suárez-Rama, M. Páramo, S. Agra, J. Brenlla, S. Martínez, O. Rivero, D. A. Collier, A. Palotie, S. Cichon, M. M. Nöthen, M. Rietschel, D. Rujescu, H. Stefansson, S. Steinberg, E. Sigurdsson, D. St Clair, S. Tosato, T. Werge, K. Stefansson, J. C. González, J. Valero, A. Gutiérrez-Zotes, A. Labad, L. Martorell, E. Vilella, A. Carracedo, J. Costas, Biol. Psychiatry 2012, 71, 169–177.
P. Muglia, F. Tozzi, N. W. Galwey, C. Francks, R. Upmanyu, X. Q. Kong, A. Antoniades, E. Domenici, J. Perry, S. Rothen, C. L. Vandeleur, V. Mooser, G. Waeber, P. Vollenweider, M. Preisig, S. Lucae, B. Müller-Myhsok, F. Holsboer, L. T. Middleton, A. D. Roses, Mol. Psychiatry 2010, 15, 589–601.
M. Bly, Schizophr. Res. 2006, 81, 321–322.
T. Fukada, Y. Asada, K. Mishima, S. Shimoda, I. Saito, J. Oral Biosci. 2011, 53, 1–12.
J. Jeong, J. M. Walker, F. Wang, J. G. Park, A. E. Palmer, C. Giunta, M. Rohrbach, B. Steinmann, D. J. Eide, Proc. Natl. Acad. Sci. USA 2012, 78, E3530–3538.
A. B. Chausmer, J. Am. Coll. Nutr. 1998, 17, 109–115.
C. G. Taylor, Biometals 2005, 18, 305–312.
W. Maret, Biometals 2005, 18, 293–294.
G. A. Rutter, Islets 2010, 2, 1–2.
W. Maret, “Zinc and Diabetes”, Encyclopedia of Metalloproteins, Eds V. N. Uversky, R. H. Kretsinger, E. A. Permyakov, Springer Science + Business Media LLC, Dordrecht, 2013, 2371–2375.
A. Krezel, W. Maret, J. Biol. Inorg. Chem. 2008, 13, 401–409.
Q. Hao, W. Maret, FEBS J. 2006, 273, 4300–4310.
N. Houstis, E. D. Rosen, E. S. Lander, Nature 2006, 440, 944–948.
R. Sharif, P. Thomas, P. Zalewski, M. Fenech, Mutation Res. 2012, 733, 111–121.
P. M. Newberne, S. Broitman, T. F. Schrager, Pathobiology 1997, 65, 253–263.
L. Y. Y. Fong, L. Zhang , Y. Jiang, J. L. Farber, J. Natl. Cancer Inst. 2005, 97, 40–50.
H. Alder, C. Taccioli, H. Chen, Y. Jiang, K. J. Smalley, P. Fadda, H. G. Ozer, K. Huebner, J. L. Farber, C. M. Croce, L. Y. Y. Fong, Carcinogenesis 2012, 33, 1736–1744.
J. K. Chesters, L. Petrie, J. Nutr. Biochem. 1999, 10, 279–290.
C. H. Hogstrand, P. Kille, R. I. Nicholson, K. M. Taylor, Trends Mol. Med. 2009, 15, 101–111.
K. M. Taylor, S. Hiscox, R. I. Nicholson, Trends Endocrinol. Metabol. 2004, 15, 461–463.
S. Yamashita, C. Miyagi, T. Fukuda, N. Kagara, Y. S. Che, T. Hirano, Nature 2004, 429, 298–302.
K. Taylor, J. Gee, P. Kille, in Zinc in Human Health, Ed L. Rink, IOS Press, Amsterdam, 2011, pp. 283–304.
S. Ayton, P. Lei, A. I. Bush, Free Radic. Biol. Med. 2013, 62, 76–89.
T. J. A. Craddock, J. A. Tuszynski, D. Chopra, N. Casey, L. E. Goldstein, S. A. Hameroff, R. E. Tanzi, PloSOne 2012, 7(3)e33552.
S. Ehsani, H. Huo, A. Salehzadeh, C. L. Pocanschi, J. C. Watts, H. Wille, D. Westaway, E. Rogaeva, P. H. St. George-Hyslop, G. Schmitt-Ulms, Prog. Neurobiol. 2011, 93, 405–420.
N. T. Watt, D. R. Taylor, T. L. Kerrigan, H. H. Griffiths, J. V. Rushworth, I. J. Whitehouse, N. M. Hooper, Nat. Commun. 2012, 3:1134.
C. L. Fischer Walker, L. Lamberti, D. Roth, R. E. Black, in Zinc in Human Health, Ed L. Rink, IOS Press, Amsterdam, 2011, pp. 234–253.
N. M. Lowe, K. Fekete, T. Decsi, Am. J. Clin. Nutr. 2009, 89, 1S–12S.
W. Maret, H. H. Sandstead, J. Trace Elem. Med. Biol. 2006, 20, 3–18.
K. Grüngreiff, Zink und Leber, Dr. Falk Pharma GmbH, Freiburg, Germany, 2012, pp. 1–84.
Acknowledgment
I thank Dr. Barbara Amann, Department of Chemistry, Goucher College, Towson, MD, for providing the figures.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media Dordrecht
About this chapter
Cite this chapter
Maret, W. (2013). Zinc and Human Disease. In: Sigel, A., Sigel, H., Sigel, R. (eds) Interrelations between Essential Metal Ions and Human Diseases. Metal Ions in Life Sciences, vol 13. Springer, Dordrecht. https://doi.org/10.1007/978-94-007-7500-8_12
Download citation
DOI: https://doi.org/10.1007/978-94-007-7500-8_12
Published:
Publisher Name: Springer, Dordrecht
Print ISBN: 978-94-007-7499-5
Online ISBN: 978-94-007-7500-8
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)