
Abstract
Breathing vitally serves body homeostasis. The prevalence of upper airway infections is often taken as an indicator of overall health status of a population living at a given time. In the present study we examined the unearthed remains of skulls from the XIII-XV century inhabitants searching for signs of maxillary sinusitis. Maxillary sinuses of the skulls of 92 individuals were inspected macroscopically and, if necessary, endoscopically. Osseous changes, including the pitting and abnormal spicule formation were present in 69 cases (75.0 %). It was found that, overall, dental infection was a major cause of maxillary sinusitis (18.8 %). Severe bone changes were observed in the adults’ skulls, but were also present in the sinus walls of children’s skulls. Post-inflammatory changes were manifest as remodeling and damage to the sinus walls. The results indicate that both children and adults of the Middle Ages suffered from chronic sinusitis. These observations confirm that the climate, environment, and lifestyle of the medieval populations contributed to the morbidity of the upper respiratory tract.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Breathing depends on clear sinuses, and the occurrence of sinusitis is particularly unpleasant. The paranasal sinusitis is a disease that afflicts a significant percentage of population and causes considerable long-term morbidity. A large part of the contemporary urban and rural populations suffer from mucositis of the nose and paranasal sinuses. It is estimated that this applies to about 12 % of population. Undoubtedly, environmental pollution and increasingly common allergization by natural and chemical environmental factors increase the occurrence of sinusitis. Both indoor and outdoor conditions were understandably different in the middle ages, with likely less outside environmental but more indoor pollution; the latter stemming from wood-burning, a source of emission of oxides of carbon and nitrogen, fine particulates, volatile organic compounds, and sulphur dioxide, combined with improper ventilation and biocontamination due often to living together with domestic animals (Engelhart et al. 1999). Contemporary studies demonstrate about 20 % incidence of chronic bronchitis which may have to do with poorly ventilated houses. The upper airway complaints particularly concern women due to their role in housekeeping and cooking (Roberts 2007; Shrestha and Shrestha 2005; Brauer et al. 1996). Respiratory diseases and their consequences were surely the cause of sickness in medieval human populations as well. The prevalence of such diseases is often taken as an indicator of health status (Benninger 2003), but their incidence in medieval times is largely unknown. In the present study, therefore, we set out to examine the skulls of people living in medieval times searching for signs of chronic inflammation in the maxillary sinus.
2 Methods
The study was approved by a local Ethics Committee. A total of 105 skulls unearthed from two XIII-XV century cemeteries belonging to the Order of the Knights Templar in the villages of Rurka and Chwarszczany (northwestern region of Poland) were examined in this study. The Order’s manor house in the village of Rurka was the center of the Knights’ commandery. The village chapel and a nearby cemetery served both the knights and their servants, which is reflected in the consecutively superimposed strata of the Order’s and secular burial layers at the cemetery. The Rurka commandery population was represented by 90 skulls (169 maxillary sinuses). The Rurka Order’s headquarters were situated in the flat, ellipsoidal area of a Rurzyca river bend, surrounded by marshes and wetlands and were situated in an area otherwise inconvenient for the purpose of a common settlement. The Order’s housing and offices were slightly better than those belonging to the commonalty, but they were largely typical for the time, with small or no windows – reducing the supply of ventilation and light and with household flock living together. A comparative sample from Chwarszczany consisted of 15 skulls (30 maxillary sinuses) of children, females, and males, and belonged to individuals aged 2–80. The inhabitants of this village apparently belonged to the Knights’ attendants and operating personnel and, judging from a very modest and simple burial outfit, belonged to a lower socio-economic class.
The assessment of sex and age was done according to criteria worked out by Ubelaker (1989). Briefly, gender was determined from the assessment of cranial morphology such as: the prominence of glabella, sharpness and thickness of the supra-orbital margins, the robustness of the nuchal crest, and the size of the mastoid processes. The age at death was estimated using the following criteria: dental eruption and occlusion, cranial suture closures, postcranial epiphyseal unions, and pubic symphyseal face morphology. The appearance of the anterior and posterior fontanelles and fusion of the suture lines was used to estimate age in the perinatal period and the general sequence of eruption of the deciduous and permanent teeth in older infants and children.
The maxillae were sorted by age and, whenever possible by gender of an individual. We studied the maxillary sinus macroscopically and with a rigid endoscope. In complete skulls, the endoscope was introduced in the sinus through the nasal cavity. Changes in the sinus walls caused by the inflammatory process were classified according to the ‘morphological type’: isolated spicules and clusters of interconnected spicules, pits, cysts, lobules, and the surface structure and thickness of the bony reaction (Roberts 2007; Merrett and Pfeiffer 2000; Ortner 2003). Eleven intact skulls were trephined through the posterior wall of the maxillary sinus to obtain access to the interior of sinuses. A 4 mm diameter, rigid endoscope was used to visualize the maxillary sinus lumen. The signal was recorded on computer and archived for off-line analysis. We investigated dental pathology such as: periapical abscesses, oroantral fistulae, evident periodontitis, and ante mortem tooth loss. Statistical analyses were done by using Microsoft Excel, version 2010. A p < 0.05 was considered significant for all comparisons.
3 Results
Ninety two skulls out of the 105 unearthed were suitable for further analysis. There were 13 female and 56 male skulls belonging to adult individuals; gender could not be conclusively defined in the children group (Table 20.1). In 69/92 (75 %) cases, the maxillae showed changes in bone morphology consistent with sinusitis. Overall, inflammation-related odontogenic changes were seen in 13/69 (18.8 %) of cases. Therefore, lack of inflammatory changes or ambiguous unsettled changes were found only in 25 % of cases. In the village of Rurka there was a high percentage of skulls belonging to children and young individuals with the signs of sinusitis (Figs. 20.1 and 20.2). Otherwise, however, there were little variations between the results obtained from the two locations.

Proportion of osseous lesions observed in maxillary sinuses in the XIII-XV century skulls unearthed in the villages of Rurka and Chwarszczany

Demographics concerning the XIII-XV century skulls unearthed in the villages of Rurka (R) and Chwarszczany (C), with the signs of remodeling, abscessing, and various osseous lesions
The correlation between age and the occurrence of sinusitis was significant (χ2 9.75, df. 2; p = 0.005). There also was a correlation between increasing age and dental pathology (χ2 11.33, df. 2; p < 0.001). In the infant and children’s maxillary sinuses examined, there were relatively abundant scarring marks seen in 17\23 (73.9 %); these marks were particularly evident in the skulls belonging to infants. In the sinus walls, there were a great deal of spicules, their combinations, or some form of remodeling of the wall as a result of the inflammatory process. These changes and their types were present in different proportions (Fig. 20.1). Spicules, lobules, the surface and thickness changes represent the bony reaction in the form of bone deposition, while pits and cysts reflect bone resorption (Figs. 20.3 and 20.4). The skulls of males from the village of Chwarszczany had significantly less signs of passed sinusitis. There were no statistical differences in the prevalence of remodeling and abscessing, or remodeling independent of abscessing, between the female and male samples examined, although the abscessing and dental pathologies tended to more frequently observed in male skulls (Fig. 20.2). Other differences were either less appreciable or obscured by demographic discrepancies.

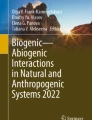
Clusters of interconnected spicules in a corner of the upper posterior wall of an adult left maxillary sinus (endoscope captured image)

Left maxillary sinus (adult male from the Rurka village, with sings of dental pathology); S-spicules and P-pits of the bony reaction in the maxillary floor
4 Discussion
The finding of the present study was that a substantial proportion of medieval inhabitants of villages in a northwestern region of Poland, despite being of a higher-than-average socio-economic status, suffered from maxillary sinusitis. Permanent traces of sinusitis in the form of sinus bone and dental remodeling were found in three thirds of the skulls examined. The corollary is that upper airway complaints must have been common in those times and the resistance of the body against airway infections was no higher than it is contemporarily.
Studying health status across ages is a unique way of understanding of how people adapted to changing socio-economic and political environments through the times, what their health condition was, and how that affected the ability to function in their communities (Merrett and Pfeiffer 2000). Upper airway diseases, most notably infections are often taken as a surrogate of respiratory health in both past and contemporary populations (Benninger 2003). The upper airways are special in this assessment of past generations’ health in that airways are the first line of defense against the environmental offenders and as such underlie body homeostasis. An inflammatory process often initiates in, and spreads from, the nasal cavities. The narrow sinus ostia are passages that easily get obstructed due to swelling and mucosal adenomatous hyperplasia developing around the ostiomeatal complex (Ramanathan and Lane 2007). These factors induce inflammation of the paranasal sinuses and mucous membrane lining them, but also affect the bonny walls in the course of time. The spongy skull structure contributes to the inflammatory complications (Perloff et al. 2000). Bones are subject to inflammatory remodeling, which also leads to sustained swelling of the adhering mucosa (Khalid et al. 2002). Thus, osteitis is a factor in the etiology of sinusitis. Some authors believe that the thickening of sinus walls and bone sclerosis underlie a chronic, years-long process of sinusitis (Perloff et al. 2000). The present study on the maxillary sinuses representing a sample of inhabitants of the medieval times confirms the theory that inflammatory changes in the mucosa of paranasal sinuses are reflected in bone inflammation.
Other studies on the status of maxillary sinuses in medieval populations suggest a possible relation between then-present living conditions, and air and climate quality and the incidence of sinusitis (Lewis et al. 1995; Roberts 2007). Those studies point to such potential factors facilitating sinusitis as pollution from the use of biomass fuels for cooking and heating, concentration of indoor pollutants caused by living together with domestic animals, or high humidity while living close to water resources. All those factors also were likely present in the environment of the inhabitants of the two villages whose skulls were examined in the present study for the remnant signs of passed sinusitis. A higher incidence of sinusitis in men could correspond to their being more exposed to the outside climatic conditions and weather changes. Also, a large number of changes in the sinuses of children suggest their low resistance to chronic pathologies of upper airways.
A small size of the sample, complex etiology of sinusitis, and difficulties in determining the presence of sinusitis make one interpret the results with caution. Despite all the inherent limitations of trying to get insight into the health status of the inhabitants of the time long bygone, we believe we may conclude that chronic upper airway pathologies were a frequent accompaniment in the medieval times as they continue to be so. Analysis of the whole sample also demonstrates that the prevalence of sinusitis increased with advancing age of the people of the time.
References
Benninger, M. S. (2003). Adult chronic rhinosinusitis: Definitions, diagnosis, epidemiology, and pathophysiology. Otolaryngology – Head and Neck Surgery, 129(3), 1–32.
Brauer, M., Bartlett, K., & Pineda, J. R. (1996). Assessment of particulate concentrations from domestic biomass combustion in rural Mexico. Environmental Science and Technology, 30, 104–109.
Engelhart, S., Burchardt, H., Neumann, R., Ewers, U., Exner, M., & Kramer, M. H. (1999). Sick building syndrome in an office building formerly used by a pharmaceutical company: A case study. Indoor Air, 9, 139–143.
Khalid, A. N., Hunt, J., Perloff, J. R., & Kennedy, D. W. (2002). The role of bone in chronic rhinosinusitis. Laryngoscope, 112, 1951–1957.
Lewis, M. E., Roberts, C. A., & Manchester, K. (1995). Comparative study of the prevalence of maxillary sinusitis in later medieval urban and rural populations in Northern England. American Journal of Physical Anthropology, 98, 497–506.
Merrett, D., & Pfeiffer, S. (2000). Maxillary sinusitis as an indicator of respiratory health in past populations. American Journal of Physical Anthropology, 111, 301–318.
Ortner, D. (2003). Identification of pathological conditions in human skeletal remains (2nd ed.). San Diego: Elsevier Science/Academic Press.
Perloff, J. R., Gannon, F. H., Bolger, W. E., Montone, K. T., Orlandi, R., & Kennedy, D. W. (2000). Bone involvement in sinusitis: An apparent pathway for the spread of disease. Laryngoscope, 110, 295–299.
Ramanathan, M., Jr., & Lane, A. P. (2007). Innate immunity of the sinonasal cavity and its role in chronic rhinosinusitis. Otolaryngology – Head and Neck Surgery, 136(3), 348–356.
Roberts, C. A. (2007). A bioarchaeological study of maxillary sinusitis. American Journal of Physical Anthropology, 133, 792–807.
Shrestha, I. L., & Shrestha, S. L. (2005). Indoor air pollution from biomass fuels and respiratory health of the exposed population in Nepalese households. International Journal of Occupational Environmental Health, 11, 150–160.
Ubelaker, D. H. (1989). Human skeletal remains: Excavation, analysis, interpretation. Washington, DC: Taraxacum.
Conflicts of Interest
The authors declare no conflicts of interest in relation to this article.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media Dordrecht
About this chapter
Cite this chapter
Teul, I., Lorkowski, J., Lorkiewicz, W., Nowakowski, D. (2013). Sinusitis in People Living in the Medieval Ages. In: Pokorski, M. (eds) Neurobiology of Respiration. Advances in Experimental Medicine and Biology, vol 788. Springer, Dordrecht. https://doi.org/10.1007/978-94-007-6627-3_20
Download citation
DOI: https://doi.org/10.1007/978-94-007-6627-3_20
Published:
Publisher Name: Springer, Dordrecht
Print ISBN: 978-94-007-6626-6
Online ISBN: 978-94-007-6627-3
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)