
Abstract
Influenza and influenza-like illnesses are recorded in all latitudes and in every age group. In Poland, the number of cases varies between several thousand and several million depending on the epidemic season. These figures are probably underestimated since a great deal of patients avoids consulting the doctor. To some extent, this situation is caused by the fear of financial loss resulting from being on sick leave. Influenza virus is classified into three types A, B, and C according to antigenic differences in their nuclear and matrix proteins. Influenza viruses are characterized by their high changeability in terms of hemagglutinin (HA) and neuraminidase (NA). The changes may be referred to as antigenic drift that consists of point mutations in the genes encoding the HA and NA or sudden changes, referred to as antigenic shift that results from an exchange of gene segments encoding hemagglutinin and neuraminidase. Since there is an animal reservoir of influenza type A virus, reassortment of different subtypes of this virus may occur with type A virus strains which occur solely in the human. This can result in the creation of an entirely new strain with hemagglutinin and/or neuraminidase subtypes which have not been encountered in humans previously, to which a large part of the population will not be resistant and which therefore has a pandemic potential. Poland participates in the Global Influenza Surveillance System for influenza and influenza-like infection throughout the year and also during the epidemic season. The main objective of supervision is a continuous monitoring of the influenza situation in the country and the most rapid detection of the emergence of a new strain of influenza virus with pandemic potential.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Antigenic drift
- Antigenic shift
- Influenza-like virus
- Influenza virus
- Epidemiological surveillance
- Mutations
1 Introduction
Since 2001, Poland has been a member of the European Influenza Surveillance Network of the European Center for Disease Prevention and Control (website EISN 2012; Machala et al. 2006b). The country is represented by the Department of Influenza Research, National Influenza Center (DIR-NIC) which is an integral part of the National Institute of Public Health – National Institute of Hygiene (NIPH-NIH), based in Warsaw. The Sentinel influenza surveillance system has operated in Poland since the epidemic season 2004–2005 and is an organization operating independently of the WHO Global Influenza Surveillance and Response System (GISRS) in which Poland has participated for many years. It is believed that the Sentinel system is of key importance in view of the increasingly realistic probability of another influenza pandemic. This paper presents data on cases of influenza and influenza-like illness in the 2011–2012 season.
The paper describes the operation of the Sentinel system using the example of the 2011–2012 epidemic season. This system is used to monitor the incidence of influenza and influenza-like illness in Poland. It also includes the contribution of the Department of Influenza Research, National Influenza Center in this regard. This facility constantly monitors and surveys data on the current activity of the influenza virus at the country level, forwarded from the Voivodeship Sanitary-Epidemiological Station (VSESs), WHO and EISN websites. In addition the present paper, demonstrates the virological situation concerning influenza and influenza-like infection in Poland for the 2011/2012 epidemic season with analysis of data for the period 29.08.2011–24.06.2012 (Table 12.1).
2 Sentinel Influenza Surveillance System in Poland
The Sentinel influenza surveillance system became operational in Poland from the 2004–2005 epidemic season. Its main objective was to integrate epidemiological and virological surveillance in such a way that information on the number of cases of influenza would be associated with laboratory confirmation of infection caused by influenza virus and influenza-like virus. This action was necessary for Poland to join, to the greatest possible extent, the system that already operated in other European countries. That also has made it possible to provide the information required which in terms of its quality and quantity became an integral part of European data on the influenza activity in Poland in comparison with other European countries. Efforts to standardize the influenza surveillance system were supported from 2003 by the National Influenza Center, Influenza Laboratory based at the National Institute of Health, now the National Institute of Public Health-National Institute of Health. It was there that the procedures were developed due to which the Sentinal influenza surveillance system operates today with good results. Specific forms are used for the collection of epidemiological and virological data and for the data on patients with suspected influenza virus infection, from whom samples were taken for virological tests.
The National Influenza Centre, Influenza Laboratory, currently the DIR-NIC conducts hands-on laboratory training for laboratory scientists from the Voivodeship Sanitary – Epidemiological Station (VSESs), whose strong commitment is necessary for the proper functioning of the Sentinel system. These courses are primarily a compendium of knowledge on the methods of laboratory detection of influenza virus genetic material and of methods of culture and isolation of influenza viruses from clinical samples.
Surveillance of influenza is conducted throughout the year. It requires special support during the epidemic season, i.e., from about early September to early June. Participants include selected family physicians, the above mentioned VSES which receive the transmitted data from the District Sanitary – Epidemiological Stations, the DIR-NIC which has the role of coordinator and the Department of Epidemiology, based at the NIPH-NIH (Machala and Brydak 2006; Brydak et al. 2005; Machala et al. 2006b).
3 Principles of Operation of Integrated Sentinel Epidemiological and Virological System
A comprehensive system of epidemiological and virological surveillance is focused on a constant, unchanging population which is representative of the whole of the country. Approximately 1–5 % of all physicians in the country and all 16 VSES are involved in this type of analysis. Surveillance figures include recorded new cases of influenza and influenza-like illness for the 0–4, 5–14, 15–64, and ≥ 65 years age groups for each of the 52 weeks of the year (according to the numbering of calendar weeks) starting from Monday to Sunday each week, reported by the physicians participating in the program. The data are sent to the appropriate territorial VSES with data on the number of patients assigned to a physician participating in the program (Romanowska and Brydak 2007; Brydak and Machala 2006). Based on the data obtained from family physicians, each of the 16 VSES prepare a summary report for the given week of the year and forward this within the deadline to the DIR-NIC, where the weekly report is prepared for the whole country. This information is then transmitted to the European Influenza Surveillance Network (EISN 2012).
Virological surveillance involves, as also does epidemiological surveillance, the same physicians who are also required to collect samples from patients with influenza and influenza-like symptoms. Samples are sent to the appropriate territorial VSES and to the DIR-NIC. A scheme of the Sentinel integrated viral epidemiological surveillance in Poland is shown in Fig. 12.1.

Sentinal viral epidemiological surveillance in Poland
This monitoring includes:
-
Isolation of influenza virus strains and diagnostics using molecular biology techniques and serological analysis of samples taken from patients with symptoms of influenza or other influenza-like infections.
-
Transmission of information concerning the results of virological and serological investigations within the deadline set by the VSES to the DIR-NIC in weekly reports.
-
Transfer to the DIR-NIC of influenza virus strains isolated by the VSES or from other institutions. Further analysis of the antigenic and/or genetic strains acquired is conducted by the Department in order to identify the type and subtype.
-
The isolated influenza virus strains, including those for which the type/subtype cannot be determined are sent by the DIR-NIC to the WHO Collaborating Center for Reference and Research on Influenza, National Institute for Medical Research (NIMR) in London.
-
A report for the whole country is prepared by the DIR-NIC based on own data and those obtained from the reports received each week from the VSES. The report is transmitted to the EISN.
4 Participation in Sentinel Program: Benefits for Doctor and Patient
As in most other countries, participation by family medicine specialists in the Sentinel program is voluntary and is conducted on an honorary basis. Participation in the program has specific benefits for both doctors and patients. For the patient, these include free of charge laboratory testing for influenza and often for other respiratory infections caused by viruses which cause influenza-like symptoms (reimbursement by the National Health Fund). In addition, thanks to the fast availability of results it is possible to administer appropriate and effective treatment to the patient with antiviral and anti-influenza medication. This helps significantly to reduce the duration of the illness with implications for absenteeism from work due to reduced costs for patients and employers, which otherwise would be incurred due to inefficiency of a potentially non-specific treatment of patients (Madej-Pilarczyk et al. 2006; Machala et al. 2006a; Brydak and Machala 2006).
5 Participation in Sentinel Program: Benefits for Country and World
The integrated epidemiological and virological surveillance system for influenza provides data on the activity of influenza and other respiratory viruses not only at the local level, but also for the whole country. Collecting this type of data is important for early warning in cases of epidemic and pandemic influenza in Poland, neighboring countries, and for the world. Incorporating the influenza surveillance system with other countries makes it possible to analyze the epidemiological and virological situation of influenza in Poland in comparison with Europe and the world. These data are supplied to the EISN by the countries participating in the project and provide the basis for the Euro surveillance weekly newsletter, available in an electronic format. The newsletter contains data on the epidemiological and virological situation of influenza in Europe with comments by representatives of selected countries and by the newsletter’s editorial team and is available on the website http://ecdc.europa.eu.
6 Incidence of Influenza and Influenza-Like Illness in Poland in 2011–2012
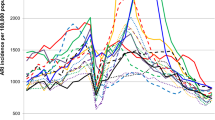
The annual cost of a large outbreak of influenza in Poland can be as high as five billion PLN, and in the capital city of Warsaw alone this cost may reach 600 million PLN, at the minimum, every season due to influenza. It is estimated that 286 million PLN loss results from the illness-related absenteeism, of which 2/3 is caused by influenza itself, and 1/3 results from its complications. Approximately 145 million PLN is expended annually on care of young children. However, 187 million PLN is loss associated with death or long-term absence from work as a result of complications of influenza. Data in Tables 12.1 and 12.2 and in Fig. 12.2 indicate that taking into account solely the ever improving operation of the Sentinel influenza surveillance system it is possible to conclude that in the 2011–2012 season nearly 2,000 samples were collected of which over 20 % tested positive for detection of influenza virus or other respiratory virus. Furthermore, the work carried out over the years to improve the Sentinel system can be observed in an increased number of samples taken from patients in the 2011–2012 season compared with the same period in 2004–2005. Data on this issue are presented in Table 12.2.

Laboratory confirmation of infections caused by influenza and influenza-like virus causing respiratory disease in Poland for the 2011/2012 epidemic season from Week 35 of 2011 to Week 25 of 2012 (29.08.2011–24.06.2012)
7 Conclusions
Conducting effective influenza surveillance is not an easy task, and certainly will not be easy during an epidemic or pandemic. However, when comparing the data from the initial period when Poland entered the Sentinel program in the 2004–2005 season with data from 2011 to 2012, it is evident that the awareness of physicians, patients, and the sanitary and epidemiological monitoring services have all considerably increased. The necessity for wide-ranging efforts in terms of monitoring of influenza and influenza-like virus infections has become a reality, without which the modern virologist and epidemiologist would be deprived of tools for the analysis of the current epidemiological and virological situation in Poland in comparison with the situation in Europe and the rest of the world.
References
Brydak, L. B., & Machala, M. (2006). Role of family physician in the European integrated influenza surveillance SENTINEL. Family Medicine & Primary Care Review, 8, 848–853 (in Polish).
Brydak, L. B., Lietzau, G., & Machala, M. (2005). Diagnostics of viral respiratory infections in hospitalized patients and ambulatory patients from SENTINEL program during 2004/05 season in Poland. Archives of Internal Medicine, CXIV(4), 958–966 (in Polish).
European Centre for Disease Prevention and Control. European Influenza Surveillance Network (EISN). (2012).http://ecdc.europa.eu/en/activities/surveillance/EISN/Pages/index.aspx.http://ecdcwhosurveillance.org. Accessed 31 Oct 2012.
Machala, M., & Brydak, L. B. (2006). The surveillance program of influenza Sentinel in Poland. Essentia Medica, 5–6, 14–18 (in Polish).
Machala, M., Lasota, P., Zycinska, K., & Brydak, L. B. (2006a). Use of molecular biology techniques in virological surveillance of influenza in the epidemic season 2005/2006. Family Medicine & Primary Care Review, 8, 682–684 (in Polish).
Machala, M., Zycinska, K., & Brydak, L. B. (2006b). Virological and epidemiological surveillance of influenza SENTINEL in Poland function in the first two influenza epidemic season 2004/2005 and 2005/2006. Family Medicine & Primary Care Review, 8, 685–688 (in Polish).
Madej-Pilarczyk, A., Machala, M., Lasota, P., Zycinska, K., & Brydak, L. B. (2006). Significance of laboratory diagnostics of infections caused by influenza virus in pediatrics. Family Medicine & Primary Care Review, 8, 183–1185 (in Polish).
Romanowska, M., & Brydak, L. B. (2007). Role of the surveillance in the fight against influenza, including pandemic situation. Family Medicine & Primary Care Review, 9, 823–829 (in Polish).
Conflicts of Interest
The authors declare no conflict of interests in relation to this article.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media Dordrecht
About this chapter
Cite this chapter
Wozniak-Kosek, A., Brydak, L.B. (2013). Virological Monitoring of Influenza Activity and Influenza-Like Illness in the Epidemic Season 2011–2012 in Poland. In: Pokorski, M. (eds) Neurobiology of Respiration. Advances in Experimental Medicine and Biology, vol 788. Springer, Dordrecht. https://doi.org/10.1007/978-94-007-6627-3_12
Download citation
DOI: https://doi.org/10.1007/978-94-007-6627-3_12
Published:
Publisher Name: Springer, Dordrecht
Print ISBN: 978-94-007-6626-6
Online ISBN: 978-94-007-6627-3
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)