
Abstract
Patch testing is a complex procedure requiring considerable knowledge, experience, and infrastructure. As all comparable medical procedures, it is prone to pitfalls and errors. These relate to patient selection; selection and preparation of patch test allergens; their application, reading, and interpreting the patch test reaction; and judging patch test relevance. In this chapter, frequent pitfalls and errors encountered in patch testing are described. With an up-to-date quality assurance system in the patch test unit, they can be prevented with a high probability.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
3.1 Introduction
Patch testing is a biological test, and as all biological tests, it depends on many objective variables that may affect its validity. Furthermore, as all medical procedures, it is also subject to possible mistakes and errors. While medical error reporting has improved in recent years, the quality of error reporting that might be used for preventive purposes in the medical profession is still far below the standard found in aviation [1]. No statistical data are available for the kind of errors encountered in patch testing and their incidence. A recent report focussed on medical professional liability claims against dermatologists does not indicate if claims have been brought forward due to errors in patch testing [2]. Even anecdotal reports on pitfalls and errors in patch testing are rare. Standard textbooks on patch testing do not provide recommendations for quality assurance in a structured way. Thus, the present compilation of pitfalls and error sources in patch testing is mainly based on personal experience, either from own clinical practice or from expert opinions in occupational dermatology cases where patch test protocols are frequently reviewed.
3.2 Pitfalls in Patient Selection
Patch testing may reveal the cause of allergic contact dermatitis, but positive results may be irrelevant in patients with other skin diseases or in persons with no skin diseases at all (e.g., patients with psoriasis run the same risk of showing a positive patch test as the general population). One has to be aware that like any medical test, patch testing has limited sensitivity and specificity: Nethercott estimated a sensitivity of 70 % and a specificity of 70 % [3].
When this valuable diagnostic tool is used in asymptomatic persons without medical diagnostic indication, clinical epidemiology teaches us that the risk of false-positive tests is higher than in persons actually suffering from contact dermatitis. A recent study by the EDEN group in five European countries illustrates the problem: A representative general population sample of 3,119 persons was patch tested with three TRUE Test panels, and a prevalence of positive patch test reactions (+, ++, +++) in the normal population of 25.2 % was observed. For metals in the standard series, this value was 15.4 %. When only those were considered who had a lifetime history of metal avoidance, this number decreased to 9.5 %. When it was additionally taken into consideration whether the volunteers had ever experienced contact dermatitis in their lifetime, only 3.6 % of the general population remained. This means that in 75 % of persons with positive patch test reactions to metals from the general population, these reactions are without relevance. In contrast, the proportion of relevant metal allergy in a cohort of eczema patients will be much higher as reported in many studies.
It is therefore wise to critically review the indication for patch testing in every patient, especially in referrals. While a study from the United Kingdom indicated that referrals to patch testing from GPs were generally appropriate [4], a more recent study from Italy indicated that a high proportion of referrals from GPs, ENT specialists, and even allergists for patch testing was not appropriate, resulting in a reduced sensitization rate [5].
Uncritical performance of patch testing, especially with known sensitizers such as paraphenylenediamine or acrylates, although not indicated, may unnecessarily induce active sensitization, although this is considered to happen rarely [6]. When a delayed patch test reaction is observed after 10 or more days, active sensitization should be suspected and confirmed by a repeated patch test of the substance, which then will be positive at 2–4 days [7].
A cause for possibly multiple false-positive patch test reactions (“excited skin syndrome,” “angry back syndrome” [8]) may be the presence of active dermatitis. Thus, in patients with acute dermatitis, patch testing should be delayed until clearing of skin lesions.
False-negative reactions, on the contrary, may be due to any local or systemic immunosuppression. A frequent cause may be preceding intense exposure to natural or artificial UV irradiation. We therefore usually avoid patch testing in patients returning from a beach vacation or undergoing regular sunbathing or medical UV therapy. In this case, the patch test should be postponed by 4–6 weeks. Topical treatment with corticosteroids is well known to suppress patch test reactions, as is the systemic treatment with glucocorticosteroids, certainly if more than 20 mg of prednisone are taken daily [9]. A minimum of 7 days should be between discontinuation of topical corticosteroids and patch testing. No sufficient clinical data exist regarding the suppression of patch test reactions by topical immune modifiers and by oral immunosuppressants. We avoid patch testing in these situations unless an urgent indication exists. In mouse models, even more drugs were shown to suppress allergic contact dermatitis, such as calcium channel blockers, amiloride, pentoxifylline, pentamidine, clonidine, spiperone, N-acetylcysteine, and flavonoids [10]. The relevance of these findings to humans remains open. However, in our experience, there is no indication of a suppression of patch test reactions caused by the recently introduced systemic drug alitretinoin.
For legal purposes, we fully inform our patients about each diagnostic procedure including noninvasive ones such as patch testing and obtain informed consent. This should ideally be documented in writing. We therefore have developed a written informed consent form containing all information on the indication, benefits, and risks of patch testing to be signed before performance of the procedure.
3.3 Pitfalls in the Selection and Preparation of Allergens
Before patch testing can be performed, the appropriate patch test allergens have to be selected. While the standard series should always be tested, additional occupation or exposure-specific trays and allergens should be chosen based on history. The possible pitfalls can be to select too many irrelevant allergens, which may lead to an increase of false-positive reactions as described above on one side and the missing of important allergens with a high potential for relevance on the other side.
Patch test allergens should be of the highest possible quality. Therefore, if available, allergens from reliable commercial suppliers that are produced according to drug standards (good manufacturing practice) should be used. Indeed, in Germany, patch test allergens are regulated as drugs, which is not the case in many other countries. Allergen content in a patch test preparation may decay with time depending on environmental conditions. Therefore, the storage conditions and expiration dates prescribed by the manufacturer should be closely followed and monitored. A decay of allergen content due to improper storage conditions may occur, thus leading to false-negative reactions. Conversely, the oxidation of weak allergens may lead to highly sensitizing compounds [11].
Many allergens are not available as commercial test preparations and may have to be prepared by a pharmacy or the dermatologist’s own laboratory. This leads to increasing complexity, with a potential for dilution errors resulting in possibly false-positive, false-negative, or irritant reactions. The same is true for the patch testing of the patient’s own products that follow specific rules and cannot be treated here in detail. Recent reviews are available [12]. All dilution instructions should be documented in writing, and the documentation should be kept with patient data. It is often useful to test dilution series in patient’s own products, e.g., in order to estimate the degree of concentration-dependent reactions.
In addition to patch test allergens, the quality of application systems should be considered. Chamber systems should provide sufficient and constant occlusion. Both aluminum and plastic-type chambers seem to fulfill these requirements. When testing fluids, differences in spreading were observed between both chamber types, leading to differentiated recommendations [13].
3.4 Pitfalls in the Application of Patch Test Allergens
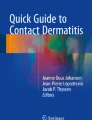
Correct dispensing of patch test allergens is essential to achieve repeatable dosing [14–16]; otherwise, false-negative results may occur (Fig. 3.1). The whole test area has to be covered with the allergen in question, and spreading should be avoided. For Finn Chambers, 20 mg of petrolatum preparation seems to fulfill this requirement best [14]. Technicians should be well trained in dosing techniques, and training should be repeated in intervals.

Doses of petrolatum allergen preparations in Finn Chambers. Dosing Finn Chambers with 10 mg (left), 20 mg (center), and 40 mg (right) of a petrolatum allergen preparation; 20 mg is the correct dose. Doses that are too low may lead to unreliable or false-negative readings and doses that are too high, to spreading of the allergen
Patch tests should be prepared shortly before application (maximum 2 h) to avoid oxidation or evaporation of allergens (especially fragrances) [17]. They should be placed on healthy, undamaged skin of the back in a well-documented and reproducible manner. In our department, we follow a standard application procedure and mark the tapes with a waterproof marker. In order to identify the patch test application sites, digital photos can be taken and stored; this is especially useful when late reactions are observed and no markings on the skin exist any longer.
The induction of an allergic delayed-type reaction depends on sufficient penetration of the allergen into the epidermis. Therefore, a complete occlusion during the application time should be achieved. Loosening of the patch test material and improper occlusion may lead to false-negative results. We therefore fixate the patches with a second layer of Fixomull (Beiersdorf, Germany). Profuse sweating in hot summer months, showering, and physical work or exercise may lead to loosening of the patches and impair patch test quality. Patients should be informed and abstain from exercise, physical work, and taking showers. Very hairy skin on the back is unsuitable for patch testing. It should be shaved first, but care has to be taken to avoid follicular irritant reactions. Usually, electric shaving is safer in this respect than wet shaving.
When a patch test to a substance that induced a strong reaction in the past is repeated, this patch should be placed a good distance from the next one to avoid spreading of the reaction and thus unreadability of the neighboring patches. If we deem such a repetition of a test to be warranted at all, we place the patch test usually on the upper arm a good distance from the other allergens. In case of intense and premature itching, patients may be instructed to return as early as 24 h after application in order to avert unnecessary intense reactions or even to pull off the patches themselves.
Testing in areas other than the back should be avoided, since patch test substances have been validated by testing on this skin. Other areas of the body may differ in penetration and irritation properties. If other patch test areas such as the upper legs have to be chosen, this should be well documented and taken into critical consideration.
Meteorological conditions at the time of patch testing may influence the results but only for weak reactions. A study of the German Contact Dermatitis Research Group indicated that with low temperature and humidity (i.e., winter conditions in Europe), both IR/? and + reactions were significantly increased with respect to the allergens fragrance mix, oil of turpentine, methyldibromo glutaronitrile + phenoxyethanol, and particularly formaldehyde, while ++/+++ reactions were hardly affected by weather conditions [18].
All nonstandardized patch test allergens, especially the patient’s own substances as well as drugs, should be removed shortly after 20 min of application, and the test area should be inspected to avoid unanticipated toxic or immediate-type reactions followed by potential contact urticaria syndrome. Otherwise, the patch test has to remain on the skin for 24 or 48 h. Differences in exposure times were not shown to influence patch test results for standard allergens in a large study of the IVDK [19].
On removal of the patches, the patch test sites should be marked with a water-resistant pen. However, these may stain the underwear of patients. We mark the sites with tapes and use templates to locate individual patches.
3.5 Pitfalls in Reading and Interpreting the Patch Test Reaction
The reading of the patch test is in the center of the procedure and thus prone to many pitfalls. The basics are clear: Reading should follow the ICDRG guidelines [20, 21]. Optimal lighting is necessary, and in positive reactions, palpation is mandatory. The difficulties lie less in the grading of strong (++ and +++) reactions than in discriminating between doubtful (positive) and irritant reactions. Even experienced dermatologists were shown to differ in their readings, but consistency improved after a repetition of their patch test reading training [22]. This points at the need of recurrent training, especially if results are to be compared between centers. Excellent patch test reading training material can be accessed on the Internet (http://dkg.ivdk.org/).
It is important to read reactions consistently according to the morphology. Allergic reactions show erythema and infiltration covering the whole test area, possibly papules, vesicles, and bullae, and may spread beyond the patch test application site [22]. Doubtful reactions are defined as erythema and/or infiltration not covering the whole test area and few papules, but without erythema/infiltration covering the whole test area [22]. Irritant reactions are bullae, erosion, and dry or shiny skin, with possible cigarette paper structure, scaling, pustules, and petechiae. Some allergens, mostly disinfectants, preservatives, and emulgators (e.g., cocamidopropyl betaine), are notorious problem allergens known for frequently eliciting doubtful, weak, and false-positive test reactions [23]. Simultaneous sodium lauryl sulfate testing may help in the differentiation between allergic and irritant reactions [24]. However, even in the hands of the experienced, a repeated open application test may be necessary to confirm or rule out allergic contact dermatitis.
Another potential for pitfalls lies in the reading of skin-staining allergens such as povidone iodine (leaving a brown stain) that may be misinterpreted as erythema. Many pitfalls exist with the reading of reactions to patient’s own substances. Mechanically irritating substances such as metal dust may cause follicular reactions, and false-positive patch tests may even be caused by microbial contamination of material [25].
Considering the skills and experiences needed for a correct reading of patch test reactions, this task should not be left to patients themselves. It has been shown that patients frequently misinterpret irritant patch test reactions as allergic (own unpublished data). If a patient is unable to return to the clinic for a reading due to any reason, we recommend at least to take a photo of the reaction(s) and to present it to us on the next appointment. Thereby, possibly necessary retesting can be confined to the number of allergens in questions.
Atypical, usually clearly irritant or even corrosive reactions should lead to reconsideration of the whole testing procedure, especially dilution steps in the testing of patient’s own substances. In rare cases, dermatitis artefacta has to be taken into consideration [26]. Retesting with nonirritant patch test preparations (e.g., physiological saline) may clarify the situation.
A minimum of two readings, one 30 min after removal of the patch test and one a minimum of 24 h later, are obligatory not to miss any reactions, since positive reactions may develop later with some allergens (paraphenylenediamine, neomycin, bacitracin, corticosteroids, and blue disperse dyes) [27]. Furthermore, a decrescendo phenomenon on the second reading may reveal an irritant reaction, although this is not true in all cases [23]. There is no general agreement that late readings (days 6 or 7) should be performed on a regular basis, though it has been reported that additional information can be generated in a significant proportion of patients. Allergens most involved in producing late-positive reactions mentioned in the literature are nickel sulfate, neomycin sulfate, tixocortol-21-pivalate, p.t. butylphenol formaldehyde resin, Cl + Me isothiazolinone, and gold sodium thiosulfate [28, 29].
3.6 Pitfalls in Judging Patch Test Relevance
Every positive patch test reaction read as allergic should be judged regarding its clinical relevance. Relevance is defined as the capability of an information retrieval system to select and retrieve data appropriate to a patient’s need [30]. In plain words, the information gained from patch testing should be useful for the patient to avoid sources of allergens leading to contact dermatitis in his private or occupational environment. Current relevance (CR) refers to the disease episode that leads the patient to the consultation and to subsequent patch testing. Past relevance (PR) refers to older clinical events that can be explained by the patch test data.
Judging of patch test relevance may be cumbersome. It involves a careful patient history, possibly additional testing procedures including patient’s own products, information from manufacturers on the chemical composition of products, and, ideally, but frequently unavailable, a chemical analysis of products. Pitfalls exist in all the mentioned steps. The patient’s memory may be unreliable, or he may have discarded products he used that lead to the clinical event. Product composition may have changed in the meantime without being communicated by manufacturers. Information from manufacturers regarding the composition of products may be unavailable or unreliable, especially if occupational substances are concerned. For cosmetics, the labeling of products is helpful, though not in all cases. In our experience, the best relevance judgments can be made in occupational cases when safety engineers of the occupational health insurance make actual workplace visits and take and analyze samples from the chemical environment.
For practical purposes, a simple relevance scoring system for positive patch test reactions has been proposed [30].
Practical Tips
-
Only patch test patients with a positive history of dermatitis; otherwise, you will perform an epidemiological study and may see many difficult-to-interpret false-positive reactions.
-
Be critical in patch testing with known sensitizers since you might actively sensitize a patient. There should be a history of contact to this substance.
-
Avoid patch testing in the presence of active dermatitis. You might end up with an “angry back.”
-
Avoid patch testing after intensive UV exposure or under immunosuppression. Reactions may be false-negative.
-
Test with high-quality allergens from reliable suppliers whenever possible.
-
Always test with the standard series and choose additional allergens based on the history of the patient.
-
If you test with a chamber system, make sure you use the correct allergen dose and that the patches remain well occluded.
-
Be careful when retesting allergens that caused intense reactions in the past. You might see a spreading reaction or even generalized dermatitis.
-
Reading of patch test reactions is an art. Follow the ICDRG guidelines and keep in good training.
-
Perform a minimum of two readings; you might need even more.
-
Do not forget to judge the relevance of a positive reaction and inform the patient about it.
References
Wilf-Miron R, Lewenhoff I, Benyamini Z, Aviram A. From aviation to medicine: applying concepts of aviation safety to risk management in ambulatory care. Qual Saf Health Care. 2003;12(1):35–9.
Moshell AN, Parikh PD, Oetgen WJ. Characteristics of medical professional liability claims against dermatologists: data from 2704 closed claims in a voluntary registry. J Am Acad Dermatol. 2012;66(1):78–85.
Nethercott JR. Practical problems in the use of patch testing in the evaluation of patients with contact dermatitis. Curr Probl Dermatol. 1990;2(4):97–123.
Lamb SR, Wilkinson SM. Audit of primary and secondary care as a source of patch test clinic referrals. Br J Dermatol. 2004;151(6):1258–60.
Corazza M, Borghi A, Mantovani L, Virgili A. Analysis of patch test referrals: influence of appropriateness of referrals on sensitization rate. Contact Dermatitis. 2012;66(2):95–100.
Devos SA, Van Der Valk PG. The risk of active sensitization to PPD. Contact Dermatitis. 2001;44(5):273–5.
Bruze M, Condé-Salazar L, Goossens A, Kanerva L, White IR. Thoughts on sensitizers in a standard patch test series. The European Society of Contact Dermatitis. Contact Dermatitis. 1999;41(5):241–50.
Mitchell J, Maibach HI. Managing the excited skin syndrome: patch testing hyperirritable skin. Contact Dermatitis. 1997;37(5):193–9.
Lindberg M, Matura M. Contact dermatitis. Heidelberg/New York: Springer; 2011.
Belsito DV. Patch testing with a standard allergen (“screening”) tray: rewards and risks. Dermatol Ther. 2004;17(3):231–9.
Sköld M, Hagvall L, Karlberg A-T. Autoxidation of linalyl acetate, the main component of lavender oil, creates potent contact allergens. Contact Dermatitis. 2008;58(1):9–14.
Frosch PJ, Geier J, Uter W, Goossens A. Patch testing with the patients’ own products. In: Contact dermatitis. Heidelberg/New York: Springer; 2011. p. 1107–19.
Isaksson M, Gruvberger B, Frick-Engfeldt M, Bruze M. Which test chambers should be used for acetone, ethanol, and water solutions when patch testing? Contact Dermatitis. 2007;57(2):134–6.
Bruze M, Isaksson M, Gruvberger B, Frick-Engfeldt M. Recommendation of appropriate amounts of petrolatum preparation to be applied at patch testing. Contact Dermatitis. 2007;56(5):281–5.
Bruze M, Frick-Engfeldt M, Gruvberger B, Isaksson M. Variation in the amount of petrolatum preparation applied at patch testing. Contact Dermatitis. 2007;56(1):38–42.
Frick-Engfeldt M, Gruvberger B, Isaksson M, Hauksson I, Pontén A, Bruze M. Comparison of three different techniques for application of water solutions to Finn Chambers®. Contact Dermatitis. 2010;63(5):284–8.
Gilpin SJ, Hui X, Maibach HI. Volatility of fragrance chemicals: patch testing implications. Dermatitis. 2009;20(4):200–7.
Uter W, Hegewald J, Kränke B, Schnuch A, Gefeller O, Pfahlberg A. The impact of meteorological conditions on patch test results with 12 standard series allergens (fragrances, biocides, topical ingredients). Br J Dermatol. 2008;158(4):734–9.
Brasch J, Geier J, Henseler T. Evaluation of patch test results by use of the reaction index. An analysis of data recorded by the Information Network of Departments of Dermatology (IVDK). Contact Dermatitis. 1995;33(6):375–80.
Maibach HI, Fregert S. Manual of contact dermatitis. Contact Dermatitis. 1980;6(7):430–4.
Fregert S. Manual of contact dermatitis: on behalf of the International Contact Dermatitis Research Group. Copenhagen: Munksgaard; 1974.
Svedman C, Isaksson M, Björk J, Mowitz M, Bruze M. ‘Calibration’ of our patch test reading technique is necessary. Contact Dermatitis. 2012;66(4):180–7.
Becker D. Allergic contact dermatitis. J Dtsch Dermatol Ges. 2013;11(7):607–21.
Löffler H, Becker D, Brasch J, Geier J, German Contact Dermatitis Research Group (DKG). Simultaneous sodium lauryl sulphate testing improves the diagnostic validity of allergic patch tests. Results from a prospective multicentre study of the German Contact Dermatitis Research Group (Deutsche Kontaktallergie-Gruppe, DKG). Br J Dermatol. 2005;152(4):709–19.
Schuster C, Mofarrah R, Aberer W, Kränke B. Pitfalls of patch testing with dental materials. Br J Dermatol. 2012;166(3):674–5.
Maurice PD, Rivers JK, Jones C, Cronin E. Dermatitis artefacta with artefact of patch tests. Clin Exp Dermatol. 1987;12(3):204–6.
Mowad CM. Patch testing: pitfalls and performance. Curr Opin Allergy Clin Immunol. 2006;6(5):340–4.
Davis MDP, Bhate K, Rohlinger AL, Farmer SA, Richardson DM, Weaver AL. Delayed patch test reading after 5 days: the Mayo Clinic experience. J Am Acad Dermatol. 2008;59(2):225–33.
Jonker MJ, Bruynzeel DP. The outcome of an additional patch-test reading on days 6 or 7. Contact Dermatitis. 2000;42(6):330–5.
Lachapelle JM. A proposed relevance scoring system for positive allergic patch test reactions: practical implications and limitations. Contact Dermatitis. 1997;36(1):39–43.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Elsner, P.U., Schliemann, S. (2014). Pitfalls and Errors in Patch Testing: Suggestions for Quality Assurance. In: Lachapelle, JM., Bruze, M., Elsner, P. (eds) Patch Testing Tips. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-45395-3_3
Download citation
DOI: https://doi.org/10.1007/978-3-642-45395-3_3
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-45394-6
Online ISBN: 978-3-642-45395-3
eBook Packages: MedicineMedicine (R0)