
Abstract
Peripheral nerve injuries vary widely in extent and severity. In the peripheral trigeminal nerve, these injuries may result from extraction of teeth, placement of dental implants, benign and malignant tumor removal, maxillofacial trauma, endodontic procedures, orthognathic procedures, and even local anesthetic injections. Each form of insult results in various extent and type of nerve fiber injury with differing abilities for the nerve to regenerate spontaneously.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
9.1 Introduction
Peripheral nerve injuries vary widely in extent and severity. In the peripheral trigeminal nerve, these injuries may result from extraction of teeth, placement of dental implants, benign and malignant tumor removal, maxillofacial trauma, endodontic procedures, orthognathic procedures, and even local anesthetic injections. Each form of insult results in various extent and type of nerve fiber injury with differing abilities for the nerve to regenerate spontaneously.
The consequences of peripheral trigeminal nerve injury to the patient are almost always detrimental and can influence the patient’s ability to speak clearly, eat comfortably, taste foods, handle oral secretions, and perform everyday activities such as shaving or applying makeup. Many types of lingual and inferior alveolar nerve injuries require no surgical intervention, and the patient’s sensation returns to normal over time. Other injuries show incomplete or no improvement with time. In order to compare these two types of clinical scenarios, the surgeon must first understand the response of the peripheral nerve to injury. The fate of the axons and the surrounding architecture of the nerve components after injury are critical for forecasting possible neural regeneration and recovery.
The ability of the peripheral nerve to regenerate and reinnervate target organs has been recognized for more than a century. In reality, peripheral axonal regrowth is often delayed and seldom complete. Complete functional recovery from severe injuries is rarely achieved despite advances in microsurgical techniques and improved understanding of nerve regeneration at the cellular level. Functional recovery is particularly poor for injuries that sever the nerve far from the target and those that incur a considerable delay prior to target reinnervation [14]. In nerve transection (axotomy) cases where the distal stumps are denervated for a prolonged period of time, they become nonconducive to regeneration as a result of loss of supportive cell assistance.
After a peripheral nerve is injured, a complex and finely regulated sequence of events is initiated to remove the damaged tissue and begin the regenerative process. The healing of peripheral nerve injuries is unique within the body as the process is one of cellular repair rather than cell division or mitosis. The nerve cells at the site are not increasing in number after an injury but are attempting to restore the volume and continuity of the original neurons.
9.2 Anatomy
An in-depth knowledge of peripheral nerve anatomy is beneficial to understand the series of events that take place after an injury. Peripheral nerves are made up of a stroma (the scaffold made of connective tissue elements) and a parenchyma (the nerve axons and Schwann cells). The components of the peripheral nerve therefore include a large amount of connective tissue, blood vessels, and the basic unit of the peripheral nerve – an axon and its associated Schwann cells. The nerve trunk represents a composite tissue constructed for the purpose of maintaining continuity, nutrition, and protection of these basic units, which require a continuous energy supply to allow for impulse conductivity and axonal transport.
9.2.1 Connective Tissue
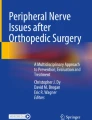
The connective tissue subdivisions provide the framework around and within the nerve. The resulting architecture consists of an external and internal epineurium and a perineurium surrounding each fascicle, in which are contained multiple axons surrounded by endoneurium (Fig. 9.1). A fourth subdivision includes a mesoneurium that consists of loose areolar tissue continuous with the epineurium and the surrounding tissue bed. The mesoneurium allows the nerve to move a certain distance longitudinally within the surrounding tissue.

Diagrammatic depiction of a cross-sectional view of the peripheral trigeminal nerve internal anatomy (From Steed [34]; with permission)
The outer connective tissue layer of the nerve is the external epineurium, which is a supporting and protective connective tissue made up primarily of collagen and elastic fibers (Fig. 9.2). The internal epineurium is the structure that invests the fascicles, which contain the nerve fibers themselves. Usually several fascicles are grouped together in bundles, constituting well-defined subunits of the nerve trunk. Fascicles vary in their size and quantity depending primarily on whether the region in question is at the proximal or distal site of the nerve. Both the lingual and inferior alveolar nerves are polyfascicular. The lingual nerve contains 15–18 fascicles at the region adjacent the mandibular third molar, while the inferior alveolar nerve contains 18–21 fascicles within the angle of the mandible. There may be fewer fascicles contained in the lingual nerve in the third molar region.

Light micrograph of a peripheral nerve in transverse section. Several fascicles that make up this nerve are enveloped by the connective tissue of the epineurium (Ep) that merges imperceptibly with the surrounding loose connective tissue – the mesoneurium. A more deeply stained perineurium (Pe) encloses the fascicles. Each fascicle consists of a large number of nerve fibers that are embedded in a more delicate endoneurium (not well defined at this level of magnification), 200×, Masson trichrome (From Steed [34]; with permission)
Each fascicle is surrounded by a perineurium, a lamellated sheath with considerable tensile mechanical strength and elasticity (Fig. 9.3). The perineurium is made up of collagen fibers dispersed among perineural cells and acts as a diffusion barrier as a result of its selective permeability, maintaining the endoneurial space within it from the surrounding tissues. This preserves the ionic environment within the fascicle. The nerve fibers themselves are closely packed together within endoneurial connective tissue (endoneurium) inside of each fascicle (Figs. 9.4 and 9.5). The endoneurium is composed of a loose gelatinous collagen matrix.

Light micrograph of a nerve fascicle at higher magnification. Here, the perineurium (Pe) is dark blue and the endoneurium (EN) light blue. Nerve fibers (NF) are densely stained structures surrounded by a myelin sheath (MS), which is red. A capillary (Cap) is shown. 465×. Masson trichrome (From Steed [34]; with permission)

Light micrograph of a peripheral nerve fascicle in transverse section. (a) Osmium fixation shows well-preserved myelin sheathes of nerve fibers. Nerve fibers vary in diameter and perineurium (Pe) surrounds the fascicle (toluidine blue, magnification ×600; semithin plastic section). (b) Electron micrograph of a myelinated nerve fiber and its associated Schwann cell in transverse section. The myelinated nerve fiber axoplasm (Ax) contains cytoskeletal elements and mitochondria that parallel its long axis. The Schwann cell, sectioned at the level of its nucleus, is enveloped by a basal lamina. Flattened perineurial cells (Pe) and collagen fibers of the endoneurium (En) are also seen (magnification ×16,800) (From Steed [34]; with permission)

Light micrograph of peripheral nerve in longitudinal section. Nerve fibers (NFs) – the slender deeply stained threads – pursue a wavy course. Myelin sheaths (MSs) appear vacuolated because of high lipid content and the effects of paraffin embedding on the tissue sample. Schwann cells (SCs) have elongated nuclei. They are indistinguishable from nuclei of fibroblasts of the delicate endoneurium (En) that invests the individual nerve fibers. A deeply stained perineurium (Pe) surrounds the nerve fascicle externally. 700×. H&E (From Steed [34]; with permission)
9.2.2 Blood Supply
Each neuron’s axon requires a continuous energy supply for impulse transmission and axonal transport. This is provided by an extrinsic vascular system and an intrinsic vascular system, which are interconnected. The extrinsic vessels enter the mesoneurium and communicate with the epineurial space via the vasa nervorum. A plexus develops at this level and runs longitudinally (Fig. 9.6). If the fascicles are examined closely, a large number of epineurial vascular branching is seen, supplying each fascicle in a segmental manner, so that each fascicle is vascularly analogous to a complete axon in a miniature model.

Clinical photo of a lingual nerve under microscopic magnification demonstrating the vasa nervorum (VN). Large longitudinally oriented intrinsic epineurial arteriolar and venular vessels can be seen deep to this plexus (From Steed [34]; with permission)
The vascular plexus enters the endoneurium through the perineurium at an oblique angle to anastomose with the intrinsic circulation that surrounds each fascicle. The oblique passage of vessels through the inner perineurial membrane is a site of potential circulatory compromise within the intrafascicular tissue.
9.2.3 Nerve Fibers
A neuron consists of a nerve cell body and its processes. There are a number of dendrites associated with the cell body and one long extension – an axon, which travels to an end organ with branches terminating in peripheral synaptic terminals. Nerve fibers can be either myelinated or unmyelinated. Sensory and motor nerves contain both types of fibers in a ratio of 4 unmyelinated axons to 1 myelinated axon.
Unmyelinated fibers are made up of several axons enclosed by a single Schwann cell (Fig. 9.7). Unmyelinated axons are small in diameter, usually averaging 0.15–2.0 μm. The axons of a myelinated fiber are individually wrapped by a single Schwann cell that has laid down a laminar myelin sheath (Fig. 9.8). The center of a myelinated fiber is made up of cytoplasm (axoplasm) with associated cytoskeletal elements surrounded by a membrane (axolemma). A concentric sheath of myelin and a Schwann cell surround this membrane (Fig. 9.9). A thin basal lamina invests the interdigitating processes of Schwann cells. At the junction between two Schwann cells, the axolemma becomes exposed at a gap called a node of Ranvier (Fig. 9.10). The propagation of an action potential along the axon “jumps” from node to node over the insulated areas covered with myelin in the process of saltatory conduction. This provides for more rapid propagation along the axon. As a result, myelinated fibers are able to conduct an impulse at a speed up to 150 m/s, while unmyelinated fibers propagate impulses at speeds of 2–2.5 m/s.

Electron micrograph of a Schwann cell associated with several unmyelinated nerve fibers in transverse section. Nerve fibers (Ax) occupy channel-like invaginations of Schwann cell cytoplasm (SC). Most nerve fibers contain neurofibrils and microtubules; synaptic vesicles (SV); collagen fibrils (CF); basal lamina (BL) (From Steed [34]; with permission)

Electron micrograph of a myelinated peripheral nerve fiber in transverse section. The axon is surrounded by a myelin sheath (MS) composed of multiple lamellae formed by the plasma membrane of a Schwann cell. A thin rim of Schwann cell cytoplasm (SC) envelops the myelin and is invested externally by a thin basal lamina (BL). Collagen fibers (CFs) of the endoneurium and flattened perineurial cells (Pe) are in the surrounding area. The nerve axoplasm contains mitochondria (Mi), neurofilaments, and a few microtubules. 30,000× (From Steed [34]; with permission)

High-resolution scanning electron micrograph of a myelinated peripheral nerve fiber fractured in the transverse plane. The axon, fractured open, reveals mitochondria (Mi) and cytoskeletal elements in the axoplasm (Ax). A peripheral rim of Schwann cell cytoplasm (SC) is outside the myelin sheath (MS). Collagen fibrils (CFs) of the surrounding endoneurium are shown well. A flattened perineurial cell (Pe) is also fractured open. 15,000× (From Steed [34]; with permission)

Light micrograph of teased myelinated nerve fibers demonstrating a node of Ranvier. The axon (Ax) is the central pale region in each fiber. Myelin sheaths (MSs), visible when fixed and stained with osmium, appear as dark linear densities. A node of Ranvier (arrows) is indicated. 500×. Osmium (From Steed [34]; with permission)
The cell bodies of the peripheral trigeminal nerve, including the lingual and inferior alveolar nerve, are contained within the trigeminal ganglion (also called the semilunar ganglion). The trigeminal ganglion is analogous to the dorsal root ganglia of the spinal cord, which contain the cell bodies of incoming sensory fibers from the rest of the body. These nerve cells may have axons that extend over a distance corresponding to thousands of cell body diameters. This imposes special requirements on the communication systems between the proximal and distal regions of the cell. To meet these requirements the neuron has unique systems of anterograde as well as retrograde intracellular transport. These transport mechanisms are involved in the response to an injury.
9.3 Basic Injury Types
Clinically useful injury grading systems have been developed that allow reflection of patient symptomatology after nerve injury and with the histological changes occurring to the nerve. Histological parameters are the far most used predictors of peripheral nerve damage and regeneration. In 1941, Cohen introduced a classification scheme to describe the injury to peripheral nerves: neuropraxia, axonotmesis, and neurotmesis [30]. In the early 1940s, Seddon [33] examined 650 patients with peripheral injuries and popularized Cohen’s time and degree of recovery-based classification system. In 1951, Sunderland [36] expanded upon this classification system by defining five distinct degrees of nerve injury based on histological changes within the nerve [30] (Figs. 9.11 and 9.12). Within this classification scheme, first-degree injuries are representative of a neuropraxia, while axonotmesis is divided into second-, third-, and fourth-degree injuries. Fifth-degree injuries represent a neurotmesis. In 1989, Mackinnon coined the term “Sixth-degree injury” which was defined as a mixed injury involving different combinations of the above [29].

Diagrammatic representation of Sunderland classification of distal segment nerve injury in transverse plane. A normal, uninjured fascicle with myelinated axons is represented at the top left. Proceeding clockwise, fascicle number I represents a first-degree injury with demyelination of some axons. Fascicle number II depicts a second-degree injury with more extensive demyelination without injury to the endoneurium. Fascicle number III is involved in a third-degree injury, now with disruption of the endoneurium around each axon. Fascicle number IV shows a fourth-degree injury with damage extending through the perineurium. Transection injury to all of the nerve components and supporting elements is reflected by the number V representing a fifth degree injury (Courtesy of Don Johnson, Atlanta VA Medical Center)

Schematic representation of Sunderland classification of nerve injury in longitudinal plane. Sunderland classification scheme is shown in longitudinal section demonstrating the “inside–out” histological progression of injury with a fifth-degree injury representing a neurotmesis defined as complete nerve transection
9.3.1 First-Degree Injury, Neuropraxia
A first-degree peripheral nerve injury (neuropraxia) clinically shows recovery within the first 3 months. It represents a conduction block with good chances for complete recovery from within days to 3 months. Pathologic changes are mild (demyelination) or absent in first-degree injuries [4]. An example would be a mild nerve stretch injury to the lingual nerve from retraction of a lingual flap during a surgical extraction of a third molar tooth.
9.3.2 Second-Degree Injury, Axonotmesis
In second-degree injury the endoneurium and perineurium remain intact. In second-degree injuries there is little histological change at the injury site or proximal to it; however, distal to the site of injury, a calcium-mediated process known as Wallerian degeneration occurs [2]. The general arrangement of the axonal sheaths and the remaining structures comprising the nerve are preserved [30]. The prospect of recovery is possible in such injuries because of the remaining uninjured mesenchymal latticework that provides a path for subsequent sprouting axons to reinnervate their target organ. Nerve recovery should be complete but progresses slowly at approximately 1 cm/day or 1 in./month.
9.3.3 Third-Degree Injury, Axonotmesis
The third-degree injury pattern involves endoneurium scarring and disorganization with the fascicles. Damage extends to the perineurium. The endoneurial tube (or sheath) is disrupted, resulting in misalignment of any regenerating axonal fibers. Regeneration from the proximal nerve takes place through scar tissue in the endoneurium, thereby limiting the regenerating axons ability to make contact with distal sites [30]. The rate of recovery progresses as expected for an axonotmesis (1 in./month), but the degree of return will not be complete.
9.3.4 Fourth-Degree Injury, Axonotmesis
A fourth-degree injury is in which the nerve is physically in continuity, but only the epineurium remains intact. Damage extends through the perineurium and regeneration attempts are blocked by scar tissue. After Wallerian degeneration takes place, the axonal continuity may eventually be interrupted, resulting in degeneration of the distal axonal segment and complete denervation. If recovery is to occur, then surgical intervention is necessary. These injuries are typically the result of severe stretch, traction, crush, or cautery injuries, or nerve injection injuries [30].
9.3.5 Fifth-Degree Injury, Neurotmesis
A fifth-degree injury results from the complete transection of a nerve trunk and loss of all supporting elements. Although these injuries can result from severe stretch that leads to avulsion, they are more often associated with sharp or penetrating trauma. Recovery is not possible without a surgical repair, although inferior alveolar nerve transection during third molar removal with replacement of the proximal and distal nerve stumps into the inferior alveolar canal may have a reasonable prognosis for spontaneous recovery without subsequent nerve repair. However, in most fifth-degree injuries, functional loss is complete and spontaneous recovery is unlikely.
9.3.6 Sixth-Degree Injury, Neuroma in Continuity
Mackinnon used the term “Sixth-degree injury, neuroma in continuity” in 1989, to describe a mixed nerve injury [29]. She illustrated how the pattern of recovery of the whole nerve is mixed to a varying degree by fascicle (I, II, III, IV, and V) [30]. Complete recovery takes place in fascicles that have sustained a first- or second-degree injury. Partial recovery is seen in fascicles that have a third-degree injury, while no recovery is seen in fourth- or fifth-degree injury patterns.
9.4 Overview of Response to Injury
The healing of peripheral nerve injuries is quite unique within the body as it is a process of cellular repair rather than tissue repair. In other words, the nerve cells themselves do not undergo mitoses. The number of nerve cells (neurons) does not increase, but the amputated nerve cell regains its original axoplasmic volume by sending out new processes to the end organ target. Peripheral nerves do have this capacity to regrow, but functional recovery in humans is often incomplete [15]. This is because the neuron and surrounding cells cannot maintain an effective growth promoting response for long periods of time. Peripheral nerves are some of the longest and most spatially complex cells in the body. A normal, uninjured nerve is represented in Fig. 9.13. Their length makes them unable to function without the structural and metabolic support provided by approximately ten times as many glial support cells [20]. A nerve injury that takes place centimeters from a neuronal cell body induces a response that involves the entire cell and its associated glial support cells. Although the number of neurons does not increase in number, the repair of each cell takes place in an environment of intense cellular proliferation. The cells that do show evidence of proliferation include Schwann cells, endothelial cells, and fibroblasts.

A normal myelinated axon. A schematic representation of a normal myelinated axon associated with a longitudinal chain of Schwann cells and enclosed within a continuous basal lamina (From Steed [34]; with permission)
Peripheral nerve response to injury has been shown to be a complex yet finely regulated sequence of events. These are aimed at removing the damaged tissue and beginning the reparative process. First, the neuron itself must survive the injury and mount an effective metabolic response to initiate regeneration [14]. Second, the growth environment in the nerve stump distal to the injury must provide sufficient support for regenerating axons. Third, the successfully regenerated axon must reinnervate the proper target and the target must retain the ability to accept reinnervation and recover from denervation atrophy. These response events take place at the cell body of the neuron, distal and proximal portions of the axon, and at the site of injury.
9.4.1 Proximal Nerve Segment Response
The first prerequisite for axonal regeneration is survival of the neuron following the injury. Survival depends upon several factors, including neuron type, age, and the degree of proximity of the injury to the cell body [14]. Certain types of neurons appear to be more susceptible to injury, such as cutaneous afferent neurons [22], and spinal motoneurons are less susceptible to injury-induced cell death than cranial sensory neurons such as the peripheral trigeminal nerve. Perhaps counterintuitively, mature neurons in the adult are less susceptible than immature neurons in the young animal. Proximal injuries produce more marked neuronal loss than distal injuries [42], and neurons subjected to injury far from their cell bodies are less susceptible than those that occur close to cell bodies. Numbers quoted in the literature vary according to the experimental animal model used, but can be substantial as 30–40 % of the small-diameter sensory neurons which contribute to a dorsal root ganglion die after nerve transection.
The mechanisms of injury-induced neuronal death are not yet fully understood, but it is clear that axotomized neurons die by apoptosis [26]. The neuron displays characteristic morphological changes associated with apoptosis and undergoes DNA fragmentation. This is primarily as a result of loss of target-derived neurotrophic support (neurotrophic factors) [14]. Neurotrophic factors are released by target tissues and by glial cells, fibroblasts, and macrophages in the local environment of both the neurons cell body and axon.
Changes in the neuronal cell body and in nerve fibers proximal to the site of injury depend both upon the severity of the injury and the proximity of the injury to the cell body. The nerve cell body itself reacts to axonal injury in a relatively predictable fashion. The series of morphologic changes that ensue in the cell body after injury are known as chromatolysis and they entail cell body and nucleolar swelling as well as nuclear eccentricity [17]. Within 6 h of injury, the nucleus migrates to the periphery of the cell body, and Nissl granules (rough endoplasmic reticulum) break up and disperse, reflecting an increased mRNA synthesis and enhanced protein synthesis.
These changes involve a switch in the cell “machinery” from being primarily concerned with transmitting nerve impulses to fabricating structural components for regeneration and reflect an altered gene expression associated with preparedness for axonal outgrowth and regeneration. The neurons convert from “transmitting mode” to “growth mode.” More important than the morphological changes are the series of alterations involving a downregulation of molecules such as neurofilaments and neuropeptides with upregulation of regeneration-associated genes (RAGs) [41].
The protein synthesis switches from producing neurotransmitter related substances to those required for axonal reconstruction [31, 38]. Examples of these substances include actin and tubulin. Evidence of upregulation of tubulin and actin mRNA and downregulation of neurofilament proteins after axotomy [39] strongly suggests that regenerating axons recapitulate developing axons in transporting increased supplies of actin and tubulin to the injury site for axonal growth [17, 21]. Downregulation of neurofilament proteins has been suggested to increase the fluidity of the axoplasm and thereby facilitate axonal transport of the tubulin and actin [23, 39]. Simultaneously there is a significant proliferative response of perineurial glial (support) cells, most likely signaled by the process of chromatolysis.
9.4.2 Injury Site Response
Within hours of physical interruption, the ends of the axon are sealed. Anterograde axoplasmic transport continues within the proximal stump, and retrograde axonal transport continues for several days. As a consequence the ends of the sealed axons swell as they fill with organelles that are unable to progress beyond the site of the discontinuity forming end bulbs [20]. There is evidence that accumulation and release of molecules from axonal end bulbs influence several aspects of the local environment [43]. End bulbs accumulate potent vasoactive peptides such as calcitonin gene-related peptide (CGRP) and the enzyme nitric oxide synthase (NOS) that generates gradients of nitric oxide (NO). Both CGRP and NO mediate the striking rises in local blood flow that develop early at the sites of injury, perhaps synergistically [44]. End bulbs accumulate sodium channels thought to contribute to ectopic discharges that generate neuropathic pain [11].
A subsequent series of proliferative events involving the proximal nerve trunk at the site of injury takes place at day 3 following the injury with combined endothelial cell, Schwann cell, mast cell, and connective tissue proliferation [9, 45, 46]. This coincides with axon sprouting and macrophage infiltration [27]. After transection, a single axon produces multiple axonal sprouts. New axonal sprouts can emerge directly from the end bulbs, but more often arise from their proximal junction with the axon or at nodes of Ranvier. At the tip of these sprouts, a growth cone exists that has an affinity for the fibronectin and laminin of the Schwann cell basal lamina. The growth cone explores the distal environment for an appropriate physical substrate.
9.4.3 Axonal Degeneration
In the distal nerve stump, a parallel series of changes develop after injury. Distal to the injury, a series of molecular and cellular events (some simultaneous while others are consecutive) that are collectively termed Wallerian degeneration (Fig. 9.14) are triggered throughout the distal nerve stump and within a small reactive zone at the tip of the proximal stump. In Wallerian (or anterograde) degeneration the primary histological change involves physical fragmentation of both axons and myelin. Ultrastructurally, both neurotubules and neurofilaments become disarrayed. Until recently, it was assumed that axons degenerated because they were no longer supported by their cell bodies. More recent studies have revealed that disconnected axons destroy themselves through a local caspase-independent process [12, 32] that leads to cytoskeletal disintegration.

Transection injury such as could occur with a scalpel or straight fissure bur and accompanying axonal degeneration – resulting in dissolution of distal myelin sheaths, degeneration of axoplasm distally, and sealing of the tip of the proximal stump of the axon (From Steed [34]; with permission)
The intrinsic degeneration of detached distal axons has been identified as the key event in Wallerian degeneration, triggering a cascade of nonneuronal cellular responses that leads to clearing of the inhibitory debris and production of an environment that supports axon regrowth in the months after the injury [15]. An initial and transient calcium signal within the axon is likely the sentinel development [43].
Axon degeneration does not occur immediately. Detached axon segments remain intact for days after peripheral nerve injury and can still transmit action potentials when stimulated [15, 28, 40]. The lag between injury and axonal degeneration is 24–48 h in murine models and several days for humans [8, 15, 18]. Eventually axons bead and swell before catastrophic granular disintegration of the cytoskeleton into fine debris is completed [16].
9.4.4 The Inflammatory Response in Wallerian Degeneration
Macrophages, T cells, and neutrophils infiltrate the site of an injury within 2 days. There are two populations of macrophages in an injured peripheral nerve, resident and recruited. Resident endoneurial macrophages constitute approximately 4 % of the endoneurial cell population and respond extremely rapidly to injury. They are joined by recruited macrophages from the vascular supply attracted by locally produced chemokines. These macrophages penetrate the tubes of the Schwann cell, degrade the myelin sheaths, and phagocytose the axonal debris that has occurred (Fig. 9.15). Schwann cells themselves may participate in the breakdown of myelin if the numbers of macrophages are depleted. Although the endoneurium and basal lamina remain essentially intact, the neural tube eventually collapses as the myelin and axonal contents are digested. The process continues until the axons neural components are completely resorbed, at which time the neural tube becomes replaced by Schwann cells and macrophages.

The inflammatory response. The Schwann cell tube is invaded by macrophages, which breach the basal lamina. Schwann cells distal to the injury site proliferate and axon sprouts begin to emerge from the proximal stump (From Steed [34]; with permission)
9.4.5 Schwann Cells
Schwann cells, the ensheathing glial cells of the peripheral nervous system, are crucial for normal nerve function and for nerve repair (Gaudet et al. 2011). Schwann cells constitute 90 % of nucleated cells within peripheral nerves [3]. They provide nutritional support for developing, mature, and regenerating axons. Basal lamina produced by Schwann cells surrounds the cell and its associated axon(s), isolating units from their neighbors and from extracellular matrix. The functional relationship between Schwann cells and their axons is normally tightly regulated by reciprocal signaling [20]. The manner in which Schwann cells respond to the loss of that relationship, whether as a result of demyelination or of axonal degeneration after crush or transection, is a critical component of the response to injury [20].
9.4.5.1 Proliferation and Support
Schwann cells in the distal stump undergo proliferation and phenotypical changes to prepare the local environment for favorable axonal regeneration. Schwann cells in the distal nerve begin to dedifferentiate soon after peripheral nerve injury, a process that is dependent on the ubiquitin–proteasome system [24]. Myelinating Schwann cells associated with detached axons respond by altering their gene expression. Within 48 h these cells stop producing myelin proteins, upregulate the synthesis of neurotrophic factors and their receptors, and begin to proliferate [20]. Proliferating Schwann cells organize themselves into columns (referred to as bands of Bungner or Schwann tubes), and the regenerating axons associate with them by growing distally between their basal membranes (Fig. 9.17). Schwann cells that are contacted by regenerating axons uncouple [6, 7], differentiate, and start to secrete myelin once again.
Schwann cells that have not been reinnervated may apoptose and disappear [37]. Cells that have been denervated for more than 6 months are morphologically and functionally different from their acutely denervated counterparts [20]. They show evidence of downregulating expression of receptors used in Schwann cell – axon signaling. Loss of these receptors may be the reason why denervated Schwann cells become progressively less able to support axonal regeneration. Interestingly, chronically denervated Schwann cells can be reactivated by treatment with TGF-B, a cytokine that is released by proliferating Schwann cells and macrophages. These reactivated Schwann cells can support axonal regeneration [35]. The weight of experimental evidence strongly suggests that there is a relatively narrow window of opportunity when transected neurons are in survival mode and denervated Schwann cells are axon responsive thus reinforcing the view that nerve repair should not be delayed when there is unequivocal evidence of the separation of nerve stumps [20].
The environment of the distal nerve directs nerve growth by means of contact attraction (contact guidance) and chemo-attraction (neurotropism) or supports nerve cell survival (neurotrophism) (Fig. 9.16). Each of these mechanisms involves Schwann cells. Schwann cells produce a large number of molecules that can potentially regulate axonal regeneration either directly or indirectly. The molecules can be roughly divided into three groups: cell adhesion molecules (CAMs), extracellular matrix proteins, and neurotrophic factors [14].

Mechanisms of regenerative nerve guidance. With operative alignment, the axons are physically aligned with the target. In neurotropism, the growth cone follows a chemotactic gradient of neurotransmitters secreted by the distal segment. In contact guidance, the axons follow physical guideposts such as cell adhesion molecules (CAMs) or ECM neurite outgrowth promoting factors to reach their target. In neurotrophism, growth cones will reach a target and receive chemical support (preventing cell death) if it is the correct one
9.4.5.2 Cell Adhesion Molecules (CAMs) and Extracellular Matrix Proteins
Schwann cells play an indispensable role in promoting regeneration by increasing their synthesis of surface cell adhesion molecules (CAMs), such as N-CAM, L1, and N-cadherin. They also show enhanced expression of extracellular matrix proteins such as laminin, collagen, fibronectin, and tenascin-C [14]. These molecules mediate adhesion between axon and axon, axon and Schwann cells, and axon and basal lamina and thereby regulate contact attraction axonal growth into the distal nerve stump (Fig. 9.17a). Adhesions between axons and between axons and Schwann cells are primarily mediated by homophilic binding of L1, N-CAM, and N-cadherin, although heterophilic binding of N-CAM to L1 and N-CAM or L1 to integrins (receptors) also occurs [14]. Adhesion between axons and the basal lamina is primarily accomplished by binding of extracellular matrix molecules, such as laminin and tenascin, to integrin receptors [10].

Axon growth cone orientation, adhesiveness, and survival. (a) Axonal growth requires the presence of extracellular matrix proteins (present within the basement membrane produced by Schwann cells) and surface cell adhesion molecules (CAMs) (present on the Schwann cell surface). The presence of receptors (integrins) for these molecules or homophilic binding to the same molecules allows advancement of the axonal growth cone. (b) If these receptors or same molecules are not present, the advancement of the axonal growth cone will not occur. (c) Growth can only occur if neurotrophic factors are available in the growth terrain. The trophic factors are incorporated into the axon and transported to the cell body to support its survival. (d) If local neurotrophic factors are not present, growth will not occur and the axotomized neuron may not survive
9.4.5.3 Neurotrophic Factors
Neurotrophic factors are a family of polypeptides required for survival of discrete neuronal populations [13]. The neurotrophin family includes NGF (nerve growth factor), BDNF (brain derived neurotrophic factor), NT-3 (neurotrophin 3), NT-4/5 (neurotrophin 4/5), FGFa (acidic fibroblast growth factor), PDGF (platelet derived growth factor), and GGF (glial growth factor), all of which may have autocrine and paracrine effects on neurons in addition to their effects on nonneuronal cells in the growth pathway [14]. The upregulation of neurotrophic factors in the distal nerve stumps of injured nerves and their subsequent return to normal levels after regeneration and target reinnervation have led to the natural association between these factors and regeneration [14]. Although a direct effect of these molecules on regeneration has been extensively looked for, there is increasing evidence that the neurotrophic molecules act directly to promote neuron survival and indirectly on regenerating axons via nonneuronal cells such as Schwann cells.
Different populations of neurons express receptors for different neurotrophins, indicating that each distinct neuronal population will respond differently to the mix of neurotrophins supplied by the Schwann cells and the target tissue [5].
9.4.6 Axonal Regeneration
The Schwann cell is therefore an intimate and essential partner to axons during early regenerative outgrowth. Three to four days after injury, Schwann cells throughout the distal stump and at the tip of the proximal stump start to divide. Schwann cells migrate into injury sites. The proliferating Schwann cells then organize into columns and form the “bands of Bungner” which are arrays of Schwann cells within a space circumscribed by the basal lamina (“Schwann tube”) (Fig. 9.18). The spouts from the proximal stump of the axon grow towards the lesion site within the basal lamina tubes that enveloped their parent axons and enter the “bands of Bungner.” The advancement of regenerating axons into the distal segment is promoted by neurite outgrowth promoting factors such as laminin and fibronectin [1, 19, 25]. Although sprouting usually starts within several hours of injury, it may be several days before a cellular outgrowth emerges from the proximal stump, and at least 4 weeks before all regrowing axons have negotiated the interface between proximal and distal stumps, a process which has been termed “regeneration stagger” [20]. Since an excess number of sprouts invade the distal Schwann columns, the initial number of axons present in the distal nerve segment may considerably exceed the number in the same nerve proximal to the site of injury [17]. With successful elongation and in the case of minimal separation of the two ends of the damaged axon, there may be no axonal misrouting, and remyelination of the axon from the daughter Schwann cells will take place (Fig. 9.19). Regrettably, the presence of a nearby or attached distal stump does not ensure directionality of peripheral axons [43].

Axonal regeneration. The proliferating Schwann cells form a tube (also known as the band of Bungner). Axon sprouts from the proximal end of the axon (From Steed [34]; with permission)

Daughter Schwann cells and complete regeneration over a less than critical nerve gap. “Daughter” Schwann cells re-myelinate the regenerating axon. The new myelin sheaths are thinner and the intermodal distances are shorter than the axon’s more proximal counterparts (From Steed [34]; with permission)
9.4.7 Pathway Selection
If axons degenerate without rupture of the basal lamina that surrounds each Schwann tube (e.g., in an ischemic or compressive injury), the axon sprouts are less likely to be misrouted. This is not always the case; however, the prime example of failed directional growth or inability for the axons themselves to cross a gap is the “neuroma in continuity,” a partial nerve trunk injury in which the distal and proximal stumps remain connected, but fail to utilize this relationship [43]. The connective tissue bridge of the neuroma in continuity contains small numbers of axons or none at all. In traumatic injuries to the peripheral nerve resulting in complete disruption, the nerve ends become a swollen mass of disorganized Schwann cells, capillaries, fibroblasts, macrophages, and collagen fibers. Regenerating axons that reach the swollen bulb of the proximal stump encounter significant barriers to further regeneration. Most sprouts will remain in the endoneurium, but others may traverse into the epineurium through breaches in the damaged perineurium or may grow ectopically between the layers of the perineurium. In both situations their behavior may produce a painful neuroma (Fig. 9.20).

Neuroma of the peripheral trigeminal nerve at its exit from the right mental foramen (From Steed [34]; with permission)
9.4.8 Roadblocks to Regenerative Outgrowth
The growth potential of regenerating axons has been suggested to be maximal 3 weeks after injury, based on temporal changes of the metabolic status of axotomized neurons [14]. Growth support provided by the distal nerve stump and the capacity of the axotomized neurons to regenerate axons may not be sustained indefinitely. Even if the neurons survive the injury, their capacity to regenerate may deteriorate with prolonged neurotrophic factor deprivation. As a result, axotomized axons that attempt to regenerate their axons after delayed nerve repair may fail. Even when regenerating axons gain access to the distal nerve stump after early microsurgical repair, they must regenerate over long distances to reach their denervated targets at a rate of 1–3 mm/day.
In peripheral nerve repair, scar formation is a major clinical problem. Many axons fail to regenerate past the injury site because they become trapped in scar tissue after the repair even with primary neurorrhaphy. In the injured human nerve, while the Schwann cell environment within the bands of Bungner is supportive of axonal growth, the fibrotic scar that forms at the site of repair represents a barrier to successful regeneration.
Examples of poor axon regeneration beyond that of a neuroma suggest a highly constrained regenerative capacity of peripheral neurons [43]. In the central nervous system (CNS), constrained regrowth is essential to the refinement of topographical circuitry. Molecular pathways to limit exuberant and inappropriate growth are needed in the CNS [43]. Similar persistent expression of growth restraining mechanisms within the peripheral system may limit regeneration when it is needed.
9.5 Summary
Surgeons caring for patients who have sustained a nerve injury to a branch of the peripheral trigeminal nerve must possess an understanding of the peripheral nerve’s response to trauma. The series of events that subsequently take place are largely dependent upon the injury type and severity, but are consistent with the response of all other peripheral nerves throughout the body. Regeneration of the peripheral nerve is possible in many instances and future manipulation of the regenerative microenvironment will lead to advances in the management of these difficult injuries.
References
Baron-Van Evercooren A, Kleinman HK et al (1982) Nerve growth factor, laminin, and fibronectin promote neurite growth in human fetal sensory ganglia cultures. J Neurosci Res 8:179–183
Burnett MG, Zager EL (2004) Pathophysiology of peripheral nerve injury: a brief review. Neurosurg Focus 16:E1
Campana WM (2007) Schwann cells: activated peripheral glia and their role in neuropathic pain. Brain Behav Immun 21:522–527
Campbell WW (2008) Evaluation and management of peripheral nerve injury. Clinical neurophysiology 119:1951–1965.
Carlstedt T (2011) An overture to basic science aspects of nerve injuries. J Hand Surg 36E:726–729
Chandross KJ (1998) Nerve injury and inflammatory cytokines modulate gap junctions in the peripheral nervous system. Glia 24:21–31
Chandross KJ, Kessler JA, Cohen RI et al (1996) Altered connexin expression after peripheral nerve injury. Mol Cell Neurosci 7:501–518
Chaudhry V, Cornblath DR (1992) Wallerian degeneration in human nerves: serial electrophysiological studies. Muscle Nerve 15:687–693
Cheng C, Zochodne DW (2002) In vivo proliferation, migration, and phenotypic changes of Schwann cells in the presence of myelinated fibers. Neuroscience 115:321–329
Daniloff JK, Levi G, Grumet M et al (1986) Altered expression of neuronal cell adhesion molecules induced by nerve injury and repair. J Cell Biol 103:929–945
Devor M (1991) Neuropathic pain and the injured nerve: peripheral mechanisms. Br Med Bull 47:619–630
Finn JT, Weil M et al (2000) Evidence that Wallerian degeneration and localized axon degeneration induced by local neurotrophin deprivation do not involve caspases. J Neurosci 20:1333–1341
Frostick SP, Kemp GJ (1998) Schwann cells, neurotrophic factors, and peripheral nerve regeneration. Microsurgery 18:397–405
Fu SY, Gordon T (1997) The cellular and molecular basis of peripheral nerve regeneration. Mol Neurobiol 14:67–116
Gaudet AD, Popovich PG, Ramer MS (2011) Wallerian degeneration: Gaining perspective in inflammatory events after peripheral nerve injury. J Neuroinflam 8:110–123
George EB, Glass JD et al (1995) Axotomy-induced axonal degeneration is mediated by calcium influx through ion specific channels. J Neurosci 15:6445–6452
Geuna S, Raimondo S, Ronchi G et al (2009) Histology of the peripheral nerve and changes occurring during nerve regeneration. In: Geuna S (ed) International review of neurobiology-essays on peripheral nerve repair and regeneration. Elsevier, New York
Gilliat RW, Hjorth RJ (1972) Nerve conduction during Wallerian degeneration in the baboon. J Neurol Neurosurg Psychiatry 35:335–341
Hall S (1997) Axonal regeneration through acellular muscle grafts. J Anat 190:57–71
Hall S (2005) The response to injury in the peripheral nervous system. J Bone Joint Surg 87 B:1309–1319
Hoffman PN, Cleveland DW (1988) Neurofilament and tubulin recapitulates the developmental program during axonal regeneration: induction of a specific beta tubulin isotype. Proc Natl Acad Sci USA 85:4530–4533
Hu P, McLachlan EM (2003) Selective reactions of cutaneous and muscle afferent neurons to peripheral nerve transection in rats. J Neurosci 23:10559–10567
Kreutzberg GW (1995) Reaction of the neuronal cell body to axonal damage. In: Waxman SG (ed) The axon: structure, function and pathophysiology. Oxford University Press, New York/Oxford
Lee HK, Shin YK, Jung J et al (2007) Schwann cells: activated peripheral glia and their role in neuropathic pain. Brain Behav Immun 21:522–527
Liu HM (1996) Growth factors and extracellular matrix in peripheral nerve regeneration, studied with a nerve chamber. J Peripher Nerv Syst 1:97–110
Lo AC, Houenou LJ et al (1995) Apoptosis in the nervous system: morphological features, methods, pathology, and prevention. Arch Histol Cytol 58:139–149
Lu X, Richardson PM (1993) Responses of macrophages in rat dorsal root ganglia following peripheral nerve injury. J Neurocytol 22:334–341
Luttges MW, Kelly PT et al (1976) Degenerative changes in mouse sciatic nerves: electrophoretic and electrophysiologic characterizations. Exp Neurol 50:706–733
Mackinnon SE (1989) New directions in peripheral nerve surgery. Ann Plast Surg 22:257–273
Maggi SP, Lowe JB et al (2003) Pathophysiology of nerve injury. Clin Plast Surg 30:109–126
Muller HW, Stoll G (1998) Nerve injury and regeneration: basic insights and therapeutic interventions. Curr Opin Neurol 11:557–562
Raff MC, Whitmore AV et al (2002) Axonal self-destruction and neurodegeneration. Science 296:868–871
Seddon JJ (1943) Three types of nerve injury. Brain 66:237
Steed M (2011) Peripheral Trigeminal Nerve Injury, Repair, and Regeneration. In: Steed M (ed) Atlas Oral Maxillofac Surg Clin North Am 19:1–13. Elsevier/Saunders, Philadelphia
Sulaiman OA, Gordon T (2002) Transforming growth factor beta and forskolin attenuate the adverse effects of long term Schwann cell denervation on peripheral nerve regeneration in vivo. Glia 37:206–218
Sunderland S (1951) A classification of peripheral nerve injuries produced by loss of function. Brain 74:491
Syroid DE, Maycox PR, Burrola PG et al (1996) Cell death in the Schwann cell lineage and its regulation by neuregulin. Proc Natl Acad Sci USA 93:9229–9234
Terzis J, Smith K (1990) The peripheral nerve. Structure, function, and reconstruction. Raven Press, New York
Tetzlaff W, Bisby MA, Kreutzberg GW (1988) Changes in cytoskeletal protein in the rat facial nucleus following axotomy. J Neurosci 8:3181–3189
Tsao JW, George EB et al (1999) Temperature modulation reveals three distinct stages of Wallerian degeneration. J Neurosci 19:4718–4726
Verge VM, Gratto KA, Karchewski LA et al (1996) Neurotrophins and nerve injury in the adult. Philos Trans R Soc Lond B Biol Sci 351:423–430
Ygge J (1989) Neuronal loss in lumbar dorsal root ganglia after proximal compared to distal sciatic nerve resection: a quantitative study in the rat. Brain Res 478:193–195
Zochodne DW (2012) The challenges and beauty of peripheral nerve regrowth. J Peripher Nerv Syst 17:1–18
Zochodne DW, Levy D et al (1999) Evidence for nitric oxide and nitric oxide synthase activity in proximal stumps of transected nerves. Neuroscience 91:1515–1527
Zochodne DW, Nguyen C (1997) Angiogenesis at the site of neuroma formation in transected peripheral nerve. J Anat 191:23–30
Zochodne DW, Nguyen C et al (1994) Accumulation and degranulation of mast cells in experimental neuromas. Neurosci Lett 182:3–6
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Steed, M.B. (2013). Nerve Injury and Regeneration. In: Miloro, M. (eds) Trigeminal Nerve Injuries. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-35539-4_9
Download citation
DOI: https://doi.org/10.1007/978-3-642-35539-4_9
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-35538-7
Online ISBN: 978-3-642-35539-4
eBook Packages: MedicineMedicine (R0)