
Abstract
Solar radiation represents an important environmental stress for human skin. The biological reactions resulting from this interaction leads to physiological and pathological reactions such as an increased photosensitivity. The present chapter focuses on the mechanisms underlying photosensitivity, especially phototoxic and photoallergic reactions caused by exogenous and endogenous chemicals, especially drugs.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Solar radiation represents the most important environmental stress to which human beings are exposed. Within the spectrum of solar radiation reaching the Earth’s surface, the ultraviolet (UV) and visible portions of the electromagnetic radiation are of particular importance to human skin. According to different photochemical and photobiological reactions, the UV portion of the electromagnetic spectrum is divided into different regions: UVC (wavelength 200–290 nm), UVB (290–320 nm), UVA (320–400 nm), and visible light (400–800 nm) [1–3]. UV radiation is able to penetrate the skin and blood. Its photon energy is sufficient to cause unimolecular and bimolecular chemical reactions within the skin.
The biological reactions resulting from the interaction of UV or visible radiation with human skin include physiological responses such as enhanced melanogenesis or thickening of the epidermal layers, and pathological reactions include photocarcinogenesis, photoaging, and the triggering of skin diseases characterized by an increased photosensitivity. In general, increased photosensitization is an abnormal reactivity of a biological substrate to, in principle, ineffective doses of UVA, UVB, and visible radiations. This can manifest as photodermatoses such as polymorphic light eruption or solar urticaria, as well as photoallergic and phototoxic reactions [4, 5].
For photosensitivity responses to occur, the relevant radiation must penetrate the tissue, be absorbed by biomolecules, and initiate chemical reactions in the tissue. The light-absorbing molecules are called chromophores or photosensitizers. In skin cells, the major UV-radiation-absorbing chromophores are nucleic acids, lipids, and proteins. Additionally, other molecules such as porphyrins, vitamins, or drugs are also able to absorb UV and visible radiation. In general, photosensitivity reactions result from the interaction of solar radiation with chromophores that are present constitutively in human skin or that have been topically or systemically applied [6]. Examples of endogenous molecules causing a photosensitivity reaction are porphyrins, whereas phytophotodermatitis is a prime example of an exogenous photosensitivity reaction. The combination of drugs and UV can produce both desired and undesired effects. Thus, PUVA therapy (psoralen plus UVA radiation) has long been employed for the treatment of psoriasis, and porphyrins can be used therapeutically, i.e., in photodynamic therapy [7–9].
The present chapter focuses on the mechanisms underlying phototoxic and photoallergic reactions caused by exogenous chromophores, especially drugs.
2 Clinical Aspects of Photoallergic and Phototoxic Reactions
Phototoxicity is the result of direct cellular damage caused by an inflammatory nonimmunological mechanism, which is initiated by a phototoxic agent and subsequent irradiation. In contrast, photoallergic reactions represent delayed or cell-mediated or type IV hypersensitivity responses, which require the specific sensitization of a given human individual to a photoactivated drug. Differentiation of phototoxic from photoallergic reactions is often difficult. This is due to the fact that most drugs are capable of causing both photoallergic and phototoxic reactions, and that the two types of photosensitivity reactions are very similar in their clinical and histological features. The following criteria can be used to differentiate between these two types of photosensitivity (Table 8.1).
Phototoxic reactions develop in most individuals if they are exposed to sufficient amounts of light and the drug. They represent an unwanted pharmacological effect. Typically, reactions appear as an exaggerated sunburn response (Figs. 8.1a, b and 8.2). Photoallergic reactions develop in only a minority of individuals exposed to the compound and light; its incidence is less than that of phototoxic skin reactions. The amount of drug required to elicit photoallergic reactions is considerably smaller than that required for phototoxic reactions. Moreover, photoallergic reactions are a delayed-type hypersensitivity; their onset is often delayed for as long as 24–72 h after exposure to the drug and light. Although the clinical appearances of phototoxic and photoallergic reactions are similar, they result from photobiologic mechanisms that can be clearly differentiated [2–4, 10].

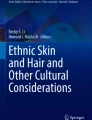
(a) Acute phototoxic dermatitis after contact to Cow parsnip (Heracleum sphondylium). (b) Hyperpigmentation 4 weeks later

Photoallergic dermatitis due to quinidine sulfate
Core Message
-
Phototoxicity is the result of direct cellular damage caused by a nonimmunological inflammatory mechanism that results from the chemical or pharmacological structure of the used substances. In contrast, photoallergic reactions represent a cell-mediated hypersensitivity response, which requires the specific sensitization to a photoactivated drug.
3 Phototoxicity: General Mechanisms
In order for phototoxic reactions to occur, they require photons to be absorbed by a molecule that is the chromophore or photosensitizer. The structural requirement of this molecule to induce photosensitization is its ability to absorb radiation. Typically, these are wavelengths that penetrate the skin deeply (above 310 nm). This characteristic absorption spectrum is determined by the chemical structure of the molecule, in particular, by the presence of single or double bonds or halogenated aromatic rings.
The absorbed photon promotes electrons within the molecule from a stable ground to an excited state, the so-called singlet or triplet state of the photosensitizer. Singlet and triplet states are higher-energy states that are defined by the spin state of the two electrons with the highest energies. When these two electrons have opposite spins, the electronic state is a singlet state; when they have the same spin, it is a triplet state. This excited singlet or triplet state is an unstable state and exists for only a very short time after photophysical formation. Typically, excited singlet states are stable for less than 10−10 s. Triplet states exist for a longer period, and in tissues, their lifetime is limited due to deactivation by oxygen (less than 10−6 s).
The excited states return to the ground state and the absorbed energy discharges by the emission of radiation (fluorescence), heat, or a chemical reaction producing a photoproduct. Complex processes are initiated by this photoproduct, which may then result in phototoxic reactions. It is important to keep in mind that not all drugs with the chemical features of a chromophore produce a photochemical reaction, because this also depends on variables such as drug absorption, metabolism, stability, and solubility. In general, phototoxicity can be produced in all individuals given a high enough dose of a photosensitizer and light irradiation. The most common skin manifestation of a phototoxic reaction is an exaggerated sunburn reaction with or without edema, blisters, and subsequent hyperpigmentation and desquamation in the exposed area. In other words, phototoxicity represents an inflammatory reaction, which results from direct cellular damage produced by the photochemical reaction between a photosensitizer and the appropriate wavelength of radiation in the UV or visible range. In contrast to photoallergic reactions, phototoxic reactions can occur during the first exposure of a given individual to this chemical in combination with irradiation and do not require a previous sensitization phase [4, 10, 11] (Fig. 8.3).

Pathomechanism of phototoxic reactions (modified after [6])
From a photochemical point of view, four pathways may be involved to exert phototoxic effects on a biological substrate. In general, these reactions can be further subdivided into oxygen-dependent photodynamic reactions and oxygen-independent nonphotodynamic reactions.
Photosensitizer + photon photosensitizer*
-
1.
An energy transfer from the excited photosensitizer to the oxygen produces excited singlet oxygen, which can participate in lipid and/or protein oxidation or induce DNA damage.
Photosensitizer* + O2 ® Photosensitizer + 1O2 ® 1O2 + target
-
2.
An electron or hydrogen transfer can lead to the formation of free radicals that directly attack biomolecules. In another pathway, interaction of these free radicals with ground state oxygen can result in the generation of reactive oxygen species. These include superoxide anion, singlet oxygen, hydroxyl radicals, and hydrogen peroxide.
(I) Photosensitizer* ® Photosensitizer • ® Photosensitizer • + target
(II) Photosensitizer • + O2 ® Photosensitizer O2 • ® Photosensitizer O2 • + target
(II) Photosensitizer • + O2 ® Photosensitizer + + O2 −• ® H2O2 ® OH• ® OH• + target
Reactive oxygen intermediates generated through this process are then capable of damaging subcellular organelles, which in turn can lead to tissue injury and inflammation. Many photosensitization reactions may be explained on the basis of these reactions.
-
3.
In contrast, the nonphotodynamic reaction is a direct reaction and leads to the generation of stable photoproducts independent of oxygen. A prime example of a nonphotodynamic type III reaction is a photosensitivity reaction induced by psoralens [11] (Fig. 8.3).
Photosensitizer* + target ®|
Photosensitizer − target
-
4.
Finally, the photosensitizer can undergo decomposition so that the resulting photoproduct can act as either a toxin or a new photosensitizer (adapted by [12]).
Photosensitizer* ® Photosensitizer • ® Photoproduct ® Photoproduct + target ¯ + hv
Photoproduct* ® Photoproduct* + target
Core Message
-
There are direct and indirect photochemical mechanisms involved in phototoxicity.
The precise cellular target of phototoxic reactions depends on the physiochemical characteristics of the phototoxic agent. Topically applied agents are more likely to damage keratinocytes due to their higher concentration in the epidermis. Systemically applied drugs cause the greatest phototoxicity to the components of the dermis, specifically mast cells and endothelial cells. At the cellular level several organelles may be damaged by the phototoxic reaction. A hydrophilic photosensitizer mainly damages the cell membranes, whereas lipophilic substances diffuse into the cell and have been shown to destroy the components within the cell including lysosomes, mitochondria, and the nucleus [13, 14]. It should be noted that although the effects on one organelle may predominate, most photosensitizers affect more than one structure. Damage to the cells results in the release of soluble mediators that cause the inflammatory response. Among these mediators, eicosanoids, histamine, and complement have all been implicated in the generation of inflammatory responses induced by photosensitizers. Cytokines such as interleukin-1, interleukin-6, and tumor necrosis factor-α (TNF-alpha) which have been detected in UVB-induced erythema responses (sunburn reaction), may be involved in phototoxicity caused by drugs and chemicals; however, experimental evidence supporting this concept is lacking for most agents [15].
The specific wavelengths of light absorbed by a given phototoxic chemical depend on the physicochemical characteristics of the phototoxic agent. As a general rule, in most instances, the wavelengths are within the UVA range. It is important to keep in mind, however, that a few agents such as sulfonamides, vinblastine, and fibric acid derivatives absorb in the UVB range, whereas porphyrins absorb energy from the long-wave UV and visible spectrum.
In general, phototoxic drugs pertain to different therapeutic classes, i.e., antibiotics, antidiabetic drugs, antihistamines, cardiovascular drugs, diuretics, nonsteroidal anti-inflammatory drugs (NSAIDs), psychiatric drugs, and others. These drugs appear in the literature as phototoxic either in vivo or in vitro. It is problematic that it is not possible to predict phototoxic potency [16, 17].
4 Some Examples of Specific Agents Capable of Causing Phototoxic Reactions
The following examples are given to illustrate the different mechanisms and factors that cause and influence phototoxic reactions.
4.1 Psoralens
Psoralens are heterocyclic, aromatic compounds derived from the condensation of a furan ring with a coumarin ring. Phototoxic reactions induced by psoralens constitute the major therapeutic principle of PUVA (psoralen plus UVA-radiation) therapy. For PUVA therapy, linear psoralens such as 8-methoxypsoralen, 5-methoxypsoralen, and trimethylpsoralen are mostly used in combination with UVA radiation (Fig. 8.4). PUVA therapy is a mainstay in the treatment of patients with psoriasis vulgaris, cutaneous T-cell lymphoma, and several other inflammatory skin diseases. Psoralens are able to produce photomodifications of various biomolecules. Unlike most other photosensitizing compounds, psoralens mediate their phototoxic effect for the most part through a nonoxygen-dependent photoreaction, although photodynamic reactions may additionally contribute. As opposed to other phototoxic agents, psoralens primarily target DNA. The interaction between psoralens and DNA occurs in two separate steps. In the first step, the nonirradiated ground state of psoralen intercalates inside the nucleic acid duplex. In combination with UVA radiation, the excited psoralen molecules then form monofunctional and bifunctional psoralen–DNA photoadducts (cross-links) with pyrimidine bases – mainly thymine, but also cytosine and uracil. This mechanism may explain the antiproliferative effects of psoralens. Psoralen-induced DNA damage is responsible for adverse effects such as increased mutagenicity and skin cancer [18].

Structure of 8-methoxypsoralen (8-MOP), 5-methoxypsoralen (5-MOP) and 4,5,8-trimethylpsoralen (TMP)
Other important targets of psoralens are specific receptors, in particular the epidermal growth factor (EGF) receptor and this interaction could provide another basis to explain the antiproliferative effect of PUVA therapy in psoriasis [19]. However, there are, also effects on other cell membrane components [20]. For example, it has been shown that psoralen–fatty acid adducts can activate a signaling transduction cascade leading to melanosynthesis in melanocytes. This effect may explain the beneficial effects of PUVA therapy in vitiligo patients [21] or the strong tanning following the treatment. More recently, it has been noticed that PUVA therapy can induce programmed cell death (apoptosis) in skin-infiltrating T-helper lymphocytes. The resulting depletion of skin-infiltrating T-cells from psoriatic skin is thought to be one of the major mechanisms by which PUVA therapy clears psoriasis. The precise mechanism by which PUVA induces T-helper-cell apoptosis remains to be elucidated [22].
In addition to PUVA therapy, psoralen-induced photosensitivity reactions may also cause unwanted reactions, as they are observed in phytophotodermatitis and berloque dermatitis such as hyperpigmentation of a bizarre configuration, blister formation, and erythema [23, 24].
4.2 Porphyrins
The phototoxicity of porphyrins and their derivatives is important for the pathogenesis of cutaneous symptoms of porphyrias and the therapeutic use of porphyrins in photodynamic therapy. The photoactivation of porphyrins results in the formation of singlet oxygen and thus represents a prime example of a type II reaction. The formation of singlet oxygen and other free radicals then results in the production of peroxides, which can cause cell damage and cell death. It should be noted that the action spectrum of porphyrins does not lie within the UV range, but rather in the range of visible light (405 nm Soret band) [7, 8].
4.3 Fluoroquinolones
Quinolone antibiotics bearing fluorine substituent are commonly called fluoroquinolones (FQ). Chemically the parent compound is nalidixic acid. Some derivatives maintain the naphthyridinecarboxylic nucleus (enoxacin, trovafloxacin), but in others, it is replaced by the quinolinecarboxylic acid (norfloxacin, lomefloxacin, sparfloxacin, clinafloxacin, ciprofloxacin). In both the cases, the nucleus is substituted with halogens in one or two positions. Phototoxicity induced by FQ appears to be related to structural features. 8-Halogenated FQ (i.e., lomefloxacin, clinafloxacin) provokes severe reactions in the skin in comparison with the low phototoxicity exhibited by 8-methoxy derivatives. Moreover, fluorine substituent on the 8-position of the quinoline ring of FQ also induces photoallergic responses. In general, the presence of an electron-donating substituent has been suggested to confer photostability to the halogenated substituent at the 8-position, reducing the phototoxicity. Although the exact mechanism of FQ photosensitization remains unclear, basically the following processes have been indicated to justify the FQ photoreactivity:
-
An oxygen singlet is produced by the zwitterionic form resulting from the dissociation of carboxylic acid and the simultaneous protonation of the piperazinyl group.
-
The formation of reactive oxygen species including singlet oxygen, superoxide radical, hydroxyl radical, and hydrogen peroxide, although a mechanism based on these toxic agents does not appear to be correlated with the FQ photoreactivity.
-
The photochemically induced dehalogenation generates a highly reactive carbene C-8, which reacts with some cell component.
-
A combined process wherein the hemolytic defluorination leads to the formation of aryl radical which triggers the attack of the cellular substrate, whereas the oxygen reactive species could operate in a secondary or a parallel process [12, 13, 25–28].
4.4 Nonsteroidal Anti-Inflammatory Drugs
NSAIDs frequently cause phototoxic reactions. The capacity of NSAIDs to cause an inflammatory skin reaction contrasts with their pharmacological capacity to inhibit inflammatory responses. NSAIDs are a chemically heterogeneous group of drugs. Basically, three subclasses may be considered: the carboxylic acids (salicylates, arylalkanoic acids, and fenamates), pyrazoles, and oxicams. In any of these subclasses phototoxic and nonphototoxic molecules can be found.
It has been pointed out that their common use in clinical practice has led to multiple reports of photo-induced effects. The result is the existence of a number of mechanistic studies on this subject. There are numerous reports of phototoxic reactions resulting from the use of carprofen, ketoprofen, suprofen, tiaprofenic acid, and naproxen. Benoxaprofen was removed from the European market in 1982 because of a high frequency of phototoxic reactions. Photochemical studies have shown that NSAID phototoxicity is mainly mediated by reactive oxygen species and free radicals. This has been worked out mainly for naproxen. For example, Diclofenac is lesser phototoxic than naproxen. Nevertheless, this drug has received attention because of its wide use. The major photoproducts of diclofenac are carbazole derivates (compounds: 8ClCb and cb). In vitro assays performed with diclofenac and its photoproducts have shown phototoxicity only for 8ClCb, which has structural similarities to the phototoxic drug carprofen [1, 12, 29–31].
4.5 Amiodarone
Amiodarone – an antiarrhythmic drug – often induces phototoxicity. As a clinical consequence a gray hyperpigmentation develops in the UV-exposed areas. Amiodarone and its metabolite desethylamiodarone are highly phototoxic and cause cell damage by injuring the cell membrane in an oxygen-dependent process. Because of the long half-time of amiodarone, this phototoxic reaction may persist for several months. The action spectrum of amiodarone-induced phototoxicity lies within the UVA range. This is surprising because in vitro studies have shown that the UVB range mediates the phototoxicity induced by amiodarone more efficiently than the UVA range. A possible explanation might be that the highest concentration of amiodarone in vivo was found in the dermis, which is reached preferentially by UVA, whereas the UVB portion of solar radiation is almost completely absorbed within the epidermis [32].
5 Photoallergic Reactions: General Mechanisms
Both phototoxic and photoallergic reactions require the presence of a chemical and radiation in the UV or visible range. Nevertheless, the mechanisms of action are completely different in both the reactions. Photoallergic reactions are classic T-cell-mediated immune mechanisms (Gell and Coombs type IV reactions) and, as a consequence, patients do not have clinical manifestations upon first exposure, because sensitization to the photoallergic agent is an indispensable prerequisite. The photoallergic reaction can be produced by substances that are applied topically or systemically and, in contrast to phototoxic reactions, it does not depend on the concentration of the photosensitizer. The clinical features of photoallergic reactions closely resemble those of an eczematous reaction, as they are observed in contact dermatitis and usually occur 24–72 h after irradiation.
Agents that can cause photoallergic reactions include topical antimicrobials, fragrances, sunscreen ingredients, NSAIDs, psychiatric medications, and others. It is important to know that some of these substances might also have the potency to induce a common allergic contact dermatitis [6, 10, 32–35].
The steps involved in this photochemical reaction, which results in the formation of a complete antigen, are only poorly understood. From the mechanistic point of view, photoallergy involves covalent drug – protein photobinding (haptenization) leading to the formation of a complete photoantigen. This photoantigen may trigger a hypersensitivity reaction due to a cell-mediated immune response. In addition, the photosensitized modifications of proteins may also produce extensive structural changes associated with the loss of biological function [6, 10].
For quinidine sulfate photoallergic reactions, the presence of serum components has been implicated in the pathogenesis of the photosensitivity reaction. Accordingly, an eczematous reaction could be provoked after an intradermal injection of the drug together with patient serum into the previously UVA-irradiated skin, whereas injection of the drug alone in the absence of serum did not induce eczema. It has therefore been proposed that binding of the hapten quinidine sulfate to a potential carrier protein that is present in the serum may be of crucial importance in the pathogenesis of this particular type of photoallergic reaction [36].
In the past, most photoallergic reactions resulted from the topical use of soaps and deodorants containing halogenated salicylanilides and related compounds, whereas recently, sunscreen ingredients have been found to be among the most frequent photoallergens. Systemic photoallergens include phenothiazines, chlorpromazine as well as NSAIDs. It should been noted that the same agents can also cause phototoxic reactions. For the majority of photoallergens the action spectrum lies within the UVA range. Exceptions are sulfonamides, benzodiazepines, diphenhydramine, isotretinoin, and thiazide diuretics, which produce photoallergic reactions upon exposure to UVB radiation [34] (Fig. 8.5).

Mechanism of a photoallergic reaction (modified after [6])
References
Ferguson J (1999) Drug and chemical photosensitivity. In: Hawk JLM (ed) Photodermatology. Arnold, London, pp 155–169
Krutmann J, Hönigsmann H, Elmets CA, Bergstresser PR (eds) (2000) Dermatological phototherapy and photodiagnostic methods. Springer, Berlin
Epstein JH (1989) Photomedicine. In: Smith KC (ed) The science of photobiology, 2nd edn. Plenum, New York, pp 155–192
Epstein JH (1983) Phototoxicity and photoallergy in man. J Am Acad Dermatol 8:141–147
Hölzle E, Plewig G, Lehmann P (1987) Photodermatoses – diagnostic procedures and their interpretation. Photodermatology 4:109–114
Gould JW, Mercurio MG, Elmets CA (1995) Cutaneous photosensitivity diseases induced by exogenous agents. J Am Acad Dermatol 33:551–573
Fritsch C, Goerz G, Ruzicka T (1998) Photodynamic therapy in dermatology. Arch Dermatol 134:207–214
Lim HW (1989) Mechanisms of phototoxicity in porphyria cutanea tarda and erythropoietic protoporphyria. Immunol Ser 46:671–685
Strauss GH, Bridges BA, Greaves M, Vella-Briffa D, Hall-Smith P, Price M (1980) Methoxypsoralen photochemotherapy. Lancet 122:1134–1135
Gonzalez E, Gonzalez S (1996) Drug photosensitivity, idiopathic photodermatoses, and sunscreens. J Am Acad Dermatol 35:871–885
Ljunggren B, Bjellerup M (1986) Systemic drug photosensitivity. Photodermatology 3:26–35
Quintero B, Miranda MA (2000) Mechanisms of photosensitization induced by drugs: a general survey. Ars Pharmadeutica 1:27–46
Quedraogo G, Morliere P, Santus R, Miranda CJV (2000) Damage to mitochondria of cultured human skin fibroblasts photosensitized by fluoroquinolones. J Photochem Photobiol 58:20–25
Kochevar KE (1991) Phototoxicity mechanisms: chlorpromazine photosensitized damage to DNA and cell membranes. J Invest Dermatol 77:59–64
Terencio MC, Guillen I, Gomez-Lechon MJ, Miranda MA, Castell JV (1998) Release of inflammatory mediators (PGE2, IL-6) by fenofibric acid-photosensitized human keratinocytes and fibroblasts. Photochem Photobiol 68:331–336
Diffey BL, Farr PM, Adams SJ (1988) The action spectrum in quinine photosensitivity. Br J Dermatol 118:679–685
Diffey BL, Farr PM (1988) The action spectrum in drug induced photosensitivity. Photochem Photobiol 47:49–53
Dall’Acqua F, Vedaldi D, Bordin F, Rodighiero G (1979) New studies on the interaction between 8-methoxypsoralen and DNA in vitro. J Invest Dermatol 73:191–197
Laskin JD, Lee E, Laskin DL, Gallo MA (1986) Psoralens potentiate ultraviolet light-induced inhibition of epidermal growth factor binding. Proc Natl Acad Sci USA 83:8211–8215
Zarebska Z (1994) Cell membrane, a target for PUVA therapy. J Photochem Photobiol B 23:101–109
Anthony FA, Laboda HM, Costlow ME (1997) Psoralen-fatty acid adducts activate melanocyte protein kinase C: a proposed mechanism for melanogenesis induced by 8-methoxypsoralen and ultraviolet A light. Photodermatol Photoimmunol Photomed 13:9–16
Coven TR, Walters IB, Cardinale I, Krueger JG (1999) PUVA-induced lymphocyte apoptosis: mechanism of action in psoriasis. Photodermatol Photoimmunol Photomed 15:22–27
Pathak MA, Daniels F, Fitzpatrick TB (1962) The presently known distribution of furocomarins (psoralens) in plants. J Invest Dermatol 32:225–239
Kavli G, Volden G (1984) Phytophotodermatitis. Photodermatology 1:65–75
Dawe RS, Ibbotson SH, Sanderson JB, Thomson EM, Ferguson J (2003) A randomized controlled trial (volunteer study) of sitafloxacin, enoxacin, levofloxacin and sparfloxacin phototoxicity. Br J Dermatol 149:1232–1241
Kawada A, Hatanaka K, Gomi H, Matsuo I (1999) In vitro phototoxicity of new quinolones: production of active oxygen species and photosensitized lipid peroxidation. Photodermatol Photoimmunol Photomed 15:226–230
Neumann NJ, Holzle E, Lehmann P, Rosenbruch M, Klaucic A, Plewig G (1997) Photo hen’s egg test: a model for phototoxicity. Br J Dermatol 136:326–330
Ferguson J, Johnson BE (1993) Clinical and laboratory studies of the photosensitizing potential of norfloxacin, a 4-quinolone broad-spectrum antibiotic. Br J Dermatol 128:285–295
Diffey BL, Daymond TJ, Fairgreaves H (1983) Phototoxic reactions to piroxicam, naproxen and tiaprofenic acid. Br J Rheumatol 22:239–242
Ljunggren B (1985) Propionic acid-derived nonsteroidal anti-inflammatory drugs and phototoxicity in vitro. Photodermatology 2:3–9
Stern RS (1983) Phototoxic-reactions to piroxicam and other non-steroidal anti-inflammatory agents. N Engl J Med 309:186–187
Ferguson J, Addo HA, Jones S, Johnson BE, Frain-Bell W (1985) A study of cutaneous photosensitivity induced by amiodarone. Br J Dermatol 113:537–549
Elmets CA (1986) Drug-induced photoallergy. Dermatol Clin 4:231–241
Emmett EA (1978) Drug photoallergy. Int J Dermatol 17:370–379
Horio T (1984) Photoallergic reaction. Classification and pathogenesis. Int J Dermatol 23:376–382
Schurer NY, Holzle E, Plewig G, Lehmann P (1992) Photosensitivity induced by quinidine sulfate: experimental reproduction of skin lesions. Photodermatol Photoimmunol Photomed 9:78–82
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2011 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Mang, R., Stege, H., Krutmann, J. (2011). Mechanisms of Phototoxic and Photoallergic Reactions. In: Johansen, J., Frosch, P., Lepoittevin, JP. (eds) Contact Dermatitis. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-03827-3_8
Download citation
DOI: https://doi.org/10.1007/978-3-642-03827-3_8
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-03826-6
Online ISBN: 978-3-642-03827-3
eBook Packages: MedicineMedicine (R0)