
Abstract
Autologous fat grafting has been used extensively in the human body for various applications. These have included esthetic procedures for contour augmentation, particularly in the maxillofacial region, and ablative procedures, as in the treatment of various injuries of the frontal sinus and in the treatment of ankylosis of the temporomandibular joint. Autologous fat transfer has been used to prevent heterotopic bone formation after hip replacement surgery although, currently, the usual method for prevention of heterotopic bone in orthopedics is radiation treatment of the region. The senior author developed the philosophy and technique for placing fat grafts around TMJ total joint prostheses to prevent heterotopic bone formation, decrease fibrosis, improve pain levels as well as increase jaw function. The authors describe the technique and present case reports.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
The first report of an autologous fat transplantation appeared in the literature in 1893 (1). Since then, autologous fat grafting has been used extensively in the human body for various applications. These have included esthetic procedures for contour augmentation, particularly in the maxillofacial region, and ablative procedures, as in the treatment of various injuries of the frontal sinus. There have also been reports of its use in the treatment of ankylosis of the temporomandibular joint (TMJ) by Blair (2) in 1913 and by Murphy (3) in 1914. In 1992, Thomas (4) reported the use of autologous fat transplantation as a means of preventing the formation of the heterotopic bone after hip replacement surgery in six patients. Currently, the usual method for prevention of the heterotopic bone in orthopedics is radiation treatment of the region (5–7).
The problem of heterotopic calcification is frequently seen following alloplastic materials placed in the TMJ, particularly when alloplasts of Proplast/Teflon (PT) (Vitek Inc., Houston, TX) or Silastic (Dow-Corning, Midland, MO) had been previously implanted (8–11) (Fig. 48.1). Heterotopic bone can also result with TMJ involvement from trauma, reactive arthritis, osteoarthritis, sepsis, inflammation, failed previous surgeries, and connective tissue/autoimmune diseases such as rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, scleroderma, etc. (12–18). These calcifications can cause continued worsening pain, and a progressive decrease in a range of activities that may lead to bony ankylosis. A variable amount of fibrosis and possibly reactive tissues are commonly associated with the heterotopic bone, thereby worsening the effect. No pharmacologic agents have been identified to predictably prevent these unwanted tissues from developing in the TMJ. Durr et al. (19) have reported favorable outcomes in two-thirds of their patients with TMJ ankylosis, using postsurgical radiation. However, significant concerns exist relative to the effects of this treatment on nearby structures (i.e., the brain, orbital structures, and parotid gland). In addition to this, the increased vascularity of the TMJ region compared to the hip, and the frequent presence of particulated polymeric materials, may preclude a successful result with this modality. The experiences of other surgeons with the use of radiation therapy in patients with recurrent TMJ ankylosis have not been favorable.

A coronal tomogram of a prosthetically reconstructed TMJ joint, demonstrates heterotopic bone formation on the medial side between the mandibular ramus and base of skull. No fat graft was placed around the prosthesis at surgery
Wolford, in 1992, developed the philosophy and technique for placing fat grafts around TMJ total joint prostheses to prevent heterotopic bone formation, decrease fibrosis, improve pain levels, as well as increase jaw function. Wolford and Karras (20) published the first study evaluating fat grafts placed around TMJ total joint prostheses. Fifteen patients (2 males, 13 females) underwent TMJ reconstruction with Techmedica (Techmedica, Inc., Camarillo, CA), a custom-made total joint prostheses (this TMJ prosthesis system is currently manufactured by TMJ Concepts Inc, Ventura, CA). Seven patients had bilateral and eight had unilateral surgeries, for a total of 22 joints. All patients had autologous fat harvested from the abdomen grafted around the articulating portion of the joint prostheses after the fossa and mandibular components had been stabilized. Twenty patients (2 males, 18 females) who received Techmedica total joint prostheses without fat grafts served as controls with 17 bilateral and 3 unilateral cases for a total of 37 joints.
In the fat graft group, an average preoperative maximal incisal opening (MIO) was 26.9 mm and at long term follow-up was 38.7 mm; an improvement of 11.8 mm. Contralateral excursive movements averaged 2.3 mm preoperatively and 2.2 mm at long term follow-up. In the nonfat grafted group, the average preoperative MIO was 26.8 mm and at long term follow-up was 33.1 mm; an improvement of 6.3 mm. Contralateral excursive movements averaged 3.2 mm preoperatively and 1.7 mm at long term follow-up. The differences in the measured function between the two groups were found to be statistically significant (p < 0.01). Although both groups experienced significant decrease in pain, there was no significant difference noted in the patients’ perception of their level of pain at long term follow-up. There was no radiographic or clinical evidence of heterotopic calcifications or limitation of mobility secondary to fibrosis in any of the fat grafted group, while seven control patients (35%) developed heterotopic bone and required reoperation. This initial study proved that autologous fat transplantation was a useful adjunct to prosthetic TMJ reconstruction. Its use minimizes the occurrence of excessive joint fibrosis and heterotopic calcification, consequently providing an improved range of motion.
In another study, Wolford et al. (21) evaluated 115 patients (5 males, 110 females) who had TMJ reconstruction with total joint prostheses and simultaneous fat grafts (88 bilateral and 27 unilateral) for a total of 203 joints. All patients had autologous fat from the abdomen packed around the articulating portion of the joint prostheses after the fossa and mandibular components were stabilized. Patients were divided into two groups: Group 1 (n = 76 joints) received Christensen total joint prostheses (TMJ Implants Inc., Golden, CO) (Fig. 48.2) and Group 2 (n = 127 joints) received TMJ Concepts total joint prostheses (TMJ Concepts Inc, Ventura, CA) (Fig. 48.3).

The Christensen prosthesis is an off-the-shelf device with three selections for the mandibular component and over 40 selections for the fossa component. The best fitting components are selected to fit the anatomy. These devices have metal-on-metal articulations

The TMJ Concepts total joint prosthesis a custom-fitted device constructed on a stereolithographic three-dimensional model and designed for each patient’s specific anatomical requirements. The devices have metal-on-polyethylene articulations
The average patient follow-up was 31.2 months (range 12–65 months). In Group 1, MIO increased by 3.5 mm (23.6–27.1 mm), LE decreased by 0.2 mm (1.5–1.3 mm), and the jaw function improved by 1.9 levels (7.7–5.8), where 0 = normal jaw function and 10 = no jaw function. In Group 2, MIO increased by 6.8 mm (27.6–34.4 mm), LE decreased by 1.4 mm (3.4–2.0 mm), and the jaw function improved by 2.4 levels (7.6–5.2) (Table 48.1). There was a statistically significant improvement for MIO and patient perception of jaw function in both groups. There was no radiographic or clinical evidence of heterotopic calcifications or limitation of mobility secondary to fibrosis in either group. There were 25 Christensen prostheses (33%) removed because of elevated pain levels due to device failure and/or metal hypersensitivity due to metallosis; no fibrosis or heterotopic bone formation was seen at surgical removal. There were 4 TMJ Concepts prostheses (3%) removed because of metal hypersensitivity. Evaluation of the abdominal fat donor sites showed that 10 patients (8.7%) developed complications: 2 obese patients (1.8%) developed abdominal cysts superficial to the rectus abdominis muscle requiring surgical removal; 8 patients (6.9%) developed seroma formation requiring aspiration while 2 of these 8 patients required temporary drain insertion. This study showed that autologous fat transplantation is a useful adjunct to prosthetic TMJ reconstruction to minimize the occurrence of excessive joint fibrosis and heterotopic calcification, consequently providing an improved range of movement and jaw function. The removal of the 25 Christensen and 4 TMJ Concepts prostheses were the result of prosthesis failure (Christensen) and metal hypersensitivity (22–24), but not related to the autogenous fat grafting.
There are no other published studies in the literature in reference to fat grafts placed around TMJ total joint prostheses. There are a few reports in the literature in reference to fat grafts to the TMJ area, but without total joint prostheses. Rattan (25) reported a technique of transferring the buccal fat pad into the TMJ as a pedicle or random fat flap. He presented two cases of unilateral ankylosis treated by gap arthroplasty and a buccal fat pad graft with good results in one patient at 15 months and the other at 19 months postsurgery.
Dimitroulis (26) evaluated 11 patients with 13 ankylosed TMJs. He treated the patients with gap arthroplasty and the gap was filled with autogenous dermis-fat grafts harvested from the groin. Presurgical incisal opening was 15.6 mm and at the longest follow-up (average follow-up was 41.5 months) was 35.7 mm. Only one patient reankylosed. This study found the dermis-fat grafts to be successful in treating bony and fibrous ankylosis. Dimitroulis et al. (27) evaluated 15 patients (17 joints) with dermis-fat grafts within the TMJs by MRI. Between 6 months and 2 years postsurgery, fat tissue was identified within and surrounding all of the TMJs.
2 Surgical Technique
The senior author (LMW) has used two types of TMJ total joint prostheses: the Christensen prostheses and the TMJ Concepts prostheses (22–24). The Christensen TMJ total joint prostheses (Fig. 48.2) are off-the-shelf devices with a choice of three mandibular components and over 40 selections for a fossa component with try-in devices to get the best fit for each patient’s anatomy. The Christensen prostheses are metal-on-metal articulations (Fig. 48.2). The complication rate of these prostheses is significantly higher than with the TMJ Concepts prostheses (22–24).The TMJ Concepts total joint prostheses (10–18) (Fig. 48.3) are patient-fitted devices constructed on three-dimensional models of each patient’s maxillofacial region, including the skull base, maxilla, mandible, and TMJ, using computer-assisted design/computer assisted manufacture (CAD/CAM) principles, to conform to each patient’s specific anatomical requirements. These prostheses have metal-on-polyethylene articulations.
The prostheses are placed through endaural or preauricular and submandibular incisions (8, 17, 18), after a thorough debridement of the region. The fossa component is positioned through the endaural or preauricular incision and is stabilized at the lateral rim of the fossa and the posterior aspect of the zygomatic arch with four 2-mm diameter bone screws. The mandibular component is inserted through the submandibular incision and secured to the mandible usually with six to nine 2-mm diameter screws.
Following stabilization of all condylar and fossa components, fat is harvested for grafting around the prostheses. There are numerous areas from which fat can be harvested; abdomen (20, 21), buttock, buccal fat pad (25), breast, thigh, or anywhere else where a patient may have some excess fat. Most commonly we harvest fat grafts for TMJ use from the abdomen. There is usually abundant fat available there to provide adequate fat volume. Harvesting fat from the abdomen can be accomplished from several approaches: Suprapubic (Fig. 48.4), through the naval (Fig. 48.5), from the lateral aspect of the abdomen below the bikini line, or through a pre-existing scar. Enbloc fat harvesting does the best, relative to survival. Liposuction fat tends to do poorly because of significant damage to the fat cells and subsequent resorption problems.

(a) Fat grafts are harvested from the abdomen through a 4–5-cm length incision generally made in the supra-pubic area. (b) The outer dashed line is the extent of undermining of the skin and beneath the fat pad. The inner solid line denotes the fat graft to be harvested. (c) The abdominal fat graft has been harvested from the abdomen. (d) 3–0 polyglactin sutures are used to close the deep fat layers so no depression in the harvest area will be evident. The skin is closed with subcuticular suturing

Abdominal fat can be harvested from the umbilical area. (a) An incision site is outlined around the perimeter of the umbilicus. (b) An incision is made. (c) The skin is undermined maintaining 3–5 mm of fat tissue on the undersurface of the skin. (d) Dissection below the fat tissue, superficial to the rectus muscle fascia is completed, the fat excised, and delivered through the incision. (e) The fat is stored on ice until ready for insertion around the joint prostheses. (f) The incision is closed with subcuticular sutures
For the routine fat graft harvest, the abdomen is prepared and draped in the usual fashion from above the umbilicus to the pubic region. The superior portion of the pubic hair is shaved, if necessary, to place the incision as low as possible on the abdomen for optimal cosmetic result. If an existing scar is present in the lower abdomen, this can be used instead. A 4–5 cm transverse incision is made in the midline through the skin and subcutaneous tissues to expose the abdominal fat pad (Fig. 48.4). The skin is widely undermined superiorly and laterally, taking care to maintain a 3–5 mm layer of fat on the skin side. The initial incision is then deepened into the fat at a variable distance depending on the fat pad thickness and the amount of graft required (usual range per joint was 5–20 mL). The fat is then widely undermined superficial to the rectus abdominis muscle fascia to a similar extent as the overlying skin dissection. The desired amount of graft is then harvested in a single block from the midline region. Twenty to thirty percent more of fat than estimated to fill the dead space in the TMJ region is harvested to allow for shrinkage and errors in estimation. Meticulous hemostasis of the donor site is achieved with electrocautery, and the defect in the fat pad can be closed by advancing the lateral fat flaps toward the midline and suturing with 3–0 polyglactin (Fig. 48.6). The skin incision is closed with subcutaneous sutures of 4–0 polydiaxanone, and Steri-strips can be placed for re-enforcement.

Fat harvesting technique. (a) The skin is widely undermined, leaving a 3–5 mm layer of fat on the undersurface. The fat pad is then also undermined above the level of the rectus fascia to a similar extent and the graft is taken from the midline region. (b) The lateral fat flaps are then closed in the midline
In the initial cases, a suction drain (Fig. 48.7) was placed and removed 3–5 days postsurgery, but with careful attention to hemostasis before closure, the requirement for a drain has been significantly reduced, and in fact, rarely necessary. A pressure dressing of fluffed gauze and elastic tape is applied over the donor site and maintained for approximately 3 days before removal, to minimize the incidence of hematoma and seroma formation. The graft is immediately placed through the endaural or preauricular incision to fill the dead space around the articulating portion of the prosthetic components. In bilateral cases, the graft is divided into equal portions and one portion is stored in iced normal saline until placement in the second side. The fat is packed into the TMJ region quite firmly, without causing excessive damage to the tissue graft. Incision closure is accomplished in routine layered fashion, usually with 4–0 polydiaxanone for deep sutures and a 5–0 Prolene suture for a subcuticular skin closure.

A drain may be required to be placed in the fat donor area if adequate hemostasis cannot be achieved at surgery, or a persistent hematoma or seroma develops postsurgery. The drain is inserted and attached to the bulb so that a negative pressure can be applied
When harvesting fat from the umbilical area, a circular incision is made inside the navel area to gain access to the fat positioned higher on the abdomen (Fig. 48.5). The access is greatly limited making the harvesting more challenging. Also because of the limited access, establishing hemostasis is more difficult. With this approach, fat can be harvested from either or both the lateral sides and inferior to the incision. The incision is closed with 5–0 polydiaxanone suture in an unbroken fashion.
Inadequate packing of fat around the prosthesis can result in the development of fibrosis and heterotopic bone formation. In an extremely thin patient who needs a large graft, it may be a challenge procuring an adequate volume of fat from the abdomen. Harvesting from the buttock may provide an adequate source. However, harvesting fat from the buttock usually requires turning the patient toward one side and propping the buttock upward to improve access. The incision is made in the gluteal crease. There is usually more fat located superior to the incision line. Following fat harvest, the incision is closed with a continuous or interrupted subcuticular sutures with Steri-strips placed for reinforcement. The access may be somewhat difficult depending on how much body rotation can be accomplished. It is best to wait until it is time to harvest the fat before placing a supportive roll under the buttock to elevate it. Placing the roll under the hip at the beginning of surgery could result in nerve and soft tissue damage because of the prolonged pressure on the sciatic nerve and soft tissues.
When performing TMJ total joint prostheses surgery, antibiotics are routinely administered immediately before the surgery, then every 6 h while the IV is in place. The authors usually use a cephalosporin, but for those hypersensitive to cephalosporins Clindamycin or Levaquin is used. Following hospital discharge, patients are given oral antibiotics for 1–2 weeks postsurgery. This regiment minimizes the occurrence of postsurgical infection.
Rattan (25) reported the use of a buccal fat graft to the TMJ area. Although it is apparently possible to get the fat back to the joint area, there is a concern if enough fat would be available to pack adequately around the prostheses. Packing the fat tightly around the prostheses yields best results. In patients with a propensity to develop heterotopic bone, placing a fat graft that is not tightly packed to fill all of the voids, could still result in the development of heterotopic bone around the prostheses.
Case #1 (Figs. 48.8–48.11): This 45-year-old male was referred to the senior author after undergoing 14 previously failed right TMJ surgeries including procedures using devices that contained PT. He was 2 years post-TMJ reconstruction with an Osteomed total joint prosthesis (Osteomed Inc., Dallas, TX) without the placement of a fat graft around it for that surgery. He had severe TMJ and myofascial pain, headaches, and difficulty to eat. He presented with Class I occlusion on the left side and Class II occlusion on the right side. There was a massive heterotopic bone development and bony ankylosis surrounding the right TMJ, a foreign body giant cell reaction secondary to the previous PT materials, and severe limitation of incisal opening of 20 mm with no translation of the right condyle.

Case #1. (a) The TMJ Concepts total joint prosthesis was custom-made for this patient’s specific anatomical requirements. (b) The fossa component of the TMJ Concepts total joint prosthesis was placed through a preauricular incision. The mandibular component was placed through a submandibular incision. (c) The abdominal fat graft was packed into the joint space to prevent recurrence of heterotopic bone formation and fibrosis

Case #1. (a1, a2) A 45-year-old male who had 14 previous failed right TMJ surgeries; the last previous surgery involved right TMJ reconstruction with a total joint prosthesis (Osteomed system) without a fat graft. He had severe TMJ and myofascial pain, headaches and difficulty in eating. (b1, b2) Two years postreconstructive surgery with right TMJ debridement, removal of heterotopic bone and Osteomed prosthesis, TMJ reconstruction with TMJ Concepts custom-fitted total joint prosthesis, and fat graft.

Case #1. (a1–a3) Preoperative patient with a Class I occlusion on the left side and Class II occlusion on the right side. (b1–b3) The occlusion remained stable 2 years postsurgery

Case #1. (a) The presurgical panograph X-ray showed massive heterotopic bone formation (outlined by the black arrows) around the Osteomed prosthesis. (b) The heterotopic bone was removed in sections. (c) Ten-year postsurgical radiograph shows the effectiveness of the fat graft for prevention of heterotopic bone development
The TMJ reconstructive surgery was performed in one operation including: (a) Unilateral right TMJdebridement and removal of the heterotopic bone formation around the old prosthesis, (b) Removal of the Osteomed prosthesis, (c) Unilateral right TMJ reconstruction with patient-fitted TMJ Concepts total joint prosthesis, and (d) Unilateral right TMJ fat graft packed around the prosthesis harvested from the abdomen. The patient was evaluated 2 years postsurgery showing good stability, with elimination of the TMJ pain, headaches, myofascial pain, and improved jaw function. The occlusion remained stable. At 10 years postsurgery, his incisal opening was 42 mm with 2–3 mm of translation of the right prosthetic condyle and no radiographic evidence of heterotopic bone formation.
Case #2 (Figs. 48.12–48.14): This 12-year-old male developed right TMJ ankylosis at the age of 1 secondary to sepsis. He had two failed previous surgical attempts for correction by rib grafting. He had only 3 mm of incisal opening and was developing significant dental problems because of inability to receive dental care, had severe facial asymmetry, as well as sleep apnea symptoms. A three-dimensional radiograph demonstrates the magnitude of the ankylosis. A TMJ Concepts total joint prosthesis was manufactured to reconstruct the TMJ as well as advance and vertically lengthen the right mandibular ramus. He underwent the following procedures in one stage: (a) Right TMJ removal of a large mass of heterotopic bone; (b) Reconstruction of the right TMJ and mandibular advancement with TMJ Concepts custom-fitted total joint prostheses; and (c) Fat graft packed around the prostheses and area of previous heterotopic bone formation to prevent bone from redeveloping. The patient was evaluated 3 years postsurgery with improved facial balance and good jaw function (35 mm opening) without pain. At 3 years postsurgery, there was no radiographic evidence of heterotopic bone formation.

Case #2. (a) Twelve-year-old male developed right TMJ ankylosis at the age of 1 year secondary to TMJ sepsis. He had two failed attempts for correction by rib grafting without the use of fat grafts. He had only a 3-mm incisal opening and was developing significant dental problems as well as marked facial asymmetry and sleep apnea symptoms. (b1, b2) The patient was seen 3 year post right side TMJ reconstruction and mandibular advancement with a TMJ Concepts total joint prosthesis and fat graft. He had an improved facial balance and good jaw function (35 mm opening) without pain

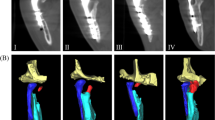
Case #2. (a) Three-dimensional CT scan demonstrates the magnitude of the heterotopic bone and joint ankylosis. (b) The heterotopic bone was removed in sections

Case #2. (a) TMJ Concepts total joint prosthesis was custom-made to reconstruct the TMJ as well as advance and vertically lengthen the right mandibular ramus. A fat graft was packed around the prosthesis to prevent heterotopic bone from redeveloping. (b) The lateral cephalogram shows the improved facial balance and normal oropharyngeal airway. (c) The tomogram shows the TMJ Concepts total joint prosthesis with no heterotopic bone formation around the prosthesis at 3 years postsurgery
3 Complications
Possible complications of abdominal fat graft harvesting include hematoma, seroma, infection, ileus, unaesthetic scar, subcutaneous soft tissue defect, abdominal esthetic concerns, pain and discomfort, and inadvertent peritoneal perforation. At the donor site, there were two extremely obese patients who developed abdominal cysts superficial to the abdominal muscle fascia that required excision for elimination. An unsightly scar can occur, but with careful incision closure, this should be of minimal concern. A few patients developed hematomas or seromas in the harvest area (Fig. 48.15). Obtaining good hemostasis at surgery is most important to avoid this problem. Immediately following procurement of the fat graft, the donor site can be packed with gauze for a few minutes. Electrocautery can be used to aide in achieving hemostasis. If hemostasis is not obtainable, then a drain can be inserted and attached to a suction bulb to create negative pressure to prevent hematoma and seroma formation, left in position for approximately 3 days and then pulled out. However, the authors rarely have to use a drain. Grossly obese patients present a greater risk of donor site morbidity. It may be more difficult to prevent postsurgical bleeding in these patients with a possible resultant hematoma, seroma, or cystic formation. The use of a negative pressure drain for several days immediate postsurgery in this patient type may help prevent this complication. Two additional patients required insertion of a drain on the first and second days postsurgery. Eight other patients did require postsurgical aspiration for the removal of a hematoma or a seroma at the donor site. Aspiration can be achieved by using a large gauge needle (16 gauge) on a large syringe or low pressure suction for removal. A pressure dressing is then applied. Repeat aspiration may be required. The occurrence of postsurgical hematoma/seroma can usually be avoided by achieving good hemostasis and placing a fluffed gauze dressing, secured with elastic tape or, alternatively, placing a Velcro-secured abdominal binder over the donor area.

(a) Left lateral abdominal hematoma is associated with fat harvest through the umbilical approach. (b1, b2) A large bore needle (16 gauge) and syringe can be used for aspiration
Additional potential complications include perforation through the abdominis rectus muscle into the abdominal cavity. The authors have never encountered this complication. Infection in the harvest area can occur and would be managed with incision and drainage, culture and sensitivity, irrigations, appropriate antibiotics, etc. Soft tissue defect from the harvest area can be an esthetic concern for some patients. However, careful harvesting, closure of lateral fat pad flaps should minimize this concern.
The authors have never encountered significant postsurgical ileus.
At the recipient site complications can also occur. Infections can occur which involve the prosthesis and fat graft (Fig. 48.16). The occurrence of an infection is very unusual, but with a greater risk in patients with immuno-dysfunctional problems. If an infection does occur, aggressive management will be required to salvage the prosthesis including: incision and drainage, removal of the fat graft if involved, and placement of irrigating catheters and drains. Multiple daily irrigations with antibiotic solutions work well and usually within 3–5 days, the drains and irrigating catheters can be advanced and removed. The authors have had about 10 patients who developed an infection involving the prosthesis and fat graft since 1989. The infections usually occur within the first month postsurgery. All but two of the prostheses have been salvaged with this regiment. Both patients who required prosthesis removal were informed early in the infectious process that immediate surgical intervention was recommended to salvage the prostheses. Both patients refused the recommendation for immediate surgical treatment, but both had draining fistulas so they had no significant pain. The first patient had a draining fistula from the right external auditory canal and did not return for treatment until 6 months postonset of infection. The prosthesis was removed and joint debrided. A new prosthesis was inserted 3 months later with a fat graft placed around the articulating portion of the prosthesis, and at 9 years postreplacement, the patient has had no further problems. The second patient had an immunodeficiency condition and developed a right submandibular draining fistula associated with the right total joint prosthesis at 1 month postsurgery. Although repeated recommendations for surgical intervention were made, she sought nonsurgical management for 5 years with numerous antibiotics that was unsuccessful before returning for surgical treatment. The prosthesis was removed and IV antibiotics were used for 2 months. The prosthesis was successfully replaced 3 months later with another fat graft placed around the prosthesis.

This 25-year-old female with juvenile rheumatoid arthritis and significant immunodysfunction had her TMJs reconstructed with TMJ Concepts total joint prosthesis and fat grafts. (a) One month postsurgery she developed a unilateral right side infection associated with the total joint prosthesis. (b) The patient was prepared for surgery and had spontaneous drainage from the original submandibular incision area. (c) The joint was debrided, but prosthesis maintained. An irrigating catheter was placed above the endaural incision into the articulating area of the joint and another placed along the ramus component. A drain was placed through the submandibular incision. Daily multiple irrigations were performed for 5 days, when the catheters and drain were removed. This prosthesis was salvaged
Case # 3 (Figs. 48.17–48.19): This 52-year-old female was 4 years post-trauma that involved multiple mandibular fractures including bilateral subcondylar fractures. She presented with bilateral TMJ severe arthritis, displaced condyles, and a class II skeletal and occlusal dentofacial deformity. She had severe TMJ pain, headaches, myofascial pain, difficulty in eating and chewing, as well as severe sleep apnea related to the retruded mandible and associated with severely reduced oropharyngeal airway. In addition, she had immunodysfunctional problems and chronic sinusitis. Following orthodontic preparation, surgery was performed in one operation including: (a) Bilateral TMJ reconstruction and mandibular counter-clockwise advancement (28 mm at pogonion) with custom made TMJ total joint prostheses (TMJ Concepts system®), (b) Bilateral coronoidectomies, (c) Bilateral TMJ fat grafts placement (harvest from the abdomen), (d) Left mandibular body osteotomy, and (e) Multiple maxillary osteotomies to down graft the posterior aspect and upright the incisors. At 6 weeks postsurgery, she developed bilateral infections around the prostheses with intraoral draining fistulas. She was taken back to surgery for joint and mandibular debridement, closure of the intraoral fistulas, and placement of bilateral extra-oral irrigating catheters and drains. She was placed on IV Clindamycin. At 3 days postsurgery, the drains and irrigating catheters were advanced and at day 5 removed. She was maintained on PO Clindamycin following hospital discharge for 1 month. The patient was evaluated 1 year postsurgery showing good stability, with elimination of TMJ pain, headaches, myofascial pain, improved jaw function and facial esthetics, and increased oropharyngeal airway, eliminating the sleep apnea. At 4 years postsurgery, no reccurrence of infection has been seen.

Case #3. (a1, a2) A 52-year-old female is seen 4 years post-trauma with bilateral temporomandibular joint severe arthritis and displaced condyles. The mandible is significantly retruded with a high occlusal plane angle and associated facial morphology. (b1, b2) One year postsurgery following bilateral TMJ reconstruction and mandibular advancement with custom-made TMJ total joint prostheses (TMJ Concepts system®), bilateral TMJ fat grafts, bilateral coronoidectomies, and simultaneous maxillary osteotomies

Case #3. (a1–a3) Presurgical occlusion demonstrates anterior open bite, Class II occlusal relationship, and posterior crossbite. (b1–b3) The occlusion remained stable 1-year postsurgery

Case #3. (a) Pretreatment cephalometric analysis shows a retruded mandible, anterior open bite, steep occlusal and mandibular plane angles, over-angulated lower incisors, severe decreased oropharyngeal airway and significant degenerative changes of the condyles. (b) The STO (prediction tracing) demonstrates the TMJ and orthognathic procedures required to achieve a good functional and esthetic result including bilateral TMJ reconstruction and mandibular advancement with custom made TMJ total joint prostheses (TMJ Concepts/Techmedica system®), bilateral coronoidectomies, and maxillary osteotomies for counter-clockwise rotation of the maxillo-mandibular complex and occlusal plane angle. (c) Cephalometric analysis at 1-year postsurgery demonstrates good facial balance. (d) Superimposition of the immediate postsurgery (red lines) and 1-year follow-up (black lines) cephalometric tracings demonstrate the treatment stability achieved for this patient
Case # 4 (Figs. 48.20–48.22): This 14-year-old female presented with juvenile rheumatoid arthritis, bilateral TMJ involvement with significant condylar resorption, class II skeletal and occlusal dentofacial deformity, an anterior open bite, and decreased oropharyngeal airway with sleep apnea symptoms, but no TMJ symptoms, pain, or headaches. Following orthodontic preparation, surgery was performed which consisted of: (a) bilateral TMJ reconstruction and mandibular counter-clockwise advancement with custom made TMJ total joint prostheses (TMJ Concepts system®), (b) bilateral TMJ fat grafts placement (harvest from abdomen), (c) bilateral coronoidectomies, (d) multiple maxillary osteotomies to down graft the posterior aspect and upright the incisors, and (e) chin augmentation with an HTR implant (Walter Lorenz CO. Jacksonville, FL). Pogonion advanced 25 mm. The patient was evaluated 1 year postsurgery showing good stability, free from TMJ pain, headaches and myofascial pain; as well as improved jaw function, facial esthetics, and increased oropharyngeal airway. Patients with inflammatory diseases such as rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, lupus, scleroderma, reactive arthritis, etc., have greater susceptibility to TMJ fibrosis and ankylosis. In patients with inflammatory disease processes, the fat grafts are essential to prevent fibrosis and reactive bone formation as well as to maximize the functional and comfort outcomes.

Case #4. (a1, a2) A 14-year-old girl had bilateral TMJ juvenile rheumatoid arthritis, significantly retruded mandible, high occlusal plane angle and associated facial morphology. (b1, b2) One year postsurgery following bilateral TMJ reconstruction and mandibular advancement with custom-made TMJ total joint prostheses (TMJ Concepts system®), bilateral TMJ fat grafts, bilateral coronoidectomies, simultaneous maxillary osteotomies and chin augmentation demonstrating a good stable, functional and esthetic outcome

Case #4. (a1–a3) Presurgical occlusion demonstrated an anterior open bite and Class II end-on cuspid relationship. (b1–b3) The occlusion remained stable 1-year postsurgery

Case #4. (a) Pretreatment cephalometric analysis shows a retruded maxilla and mandible, anterior open bite, steep occlusal and mandibular plane angles, over-angulated lower incisors, severe decreased oropharyngeal airway and significant degenerative changes of the condyles (juvenile rheumatoid arthritis). (b) The STO (prediction tracing) demonstrates the TMJ and orthognathic procedures required to achieve a good functional and esthetic result including bilateral TMJ reconstruction and mandibular advancement with custom-made TMJ total joint prostheses (TMJ Concepts system®), bilateral TMJ fat grafts (harvest fat from the abdomen) bilateral coronoidectomies, maxillary osteotomies for counter-clockwise rotation of the maxillo-mandibular complex, and chin augmentation. (c) Cephalometric analysis at 1-year postsurgery demonstrates good facial balance. (d) Superimposition of the immediate postsurgery (red lines) and 1-year follow-up (black lines) cephalometric tracings demonstrate the treatment stability achieved for this patient
4 Prevention of Fibrosis and Heterotopic Bone
The formation of extensive fibrosis and heterotopic bone has been problematic after total joint reconstruction of the TMJ, as well as from other types of TMJ arthrotomies. In the TMJ this is particularly true for multiple operated joints and joints with previously failed alloplastic implants, as well as following prosthetic and autologous joint reconstruction (20, 21, 28). Fibrosis is related to scar tissue deposition, especially in multiple operated joints or failed alloplastic reconstruction where a persistent inflammatory response may be present. Heterotopic bone may be deposited in a similar reaction in joints with inflammatory conditions and after alloplastic implant failure. Additionally, the presence of dead space after extensive joint debridement or total joint prosthesis placement leads to blood clot formation in the joint area, with subsequent organization. Pluripotential cells may then migrate into the area and be induced to differentiate into fibroblasts and osteoblasts, with deposition of collagen and bone respectively. In excessively fibrotic joints, there is a decrease in vascularity and thereby a decrease in oxygen tension in the surrounding tissues. This can lead to the transformation of fibrous tissue into cartilage and bone (29). In addition, heterotopic bone can also result with TMJ involvement from trauma, reactive arthritis, osteoarthritis, sepsis, inflammation, and connective tissue/ autoimmune diseases such as rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, scleroderma, and so on.
In the orthopedic experience, various pharmacologic agents, most notably indomethacin and etidronate, have been used with varying success (30, 31). Pharmacologic therapy has been suggested for use after prosthetic TMJ reconstruction, but no substantial data exist regarding its effectiveness (8). In the senior authors (LMW) experience with these medications, the results have been very disappointing.
Radiation treatment of the operated area within 4 days of prosthetic hip reconstruction is now a common practice and appears to offer an effective means of preventing heterotopic bone formation in orthopedics. However, local radiation of the TMJ raises concerns regarding potential adverse effects on adjacent vital structures, (i.e., eyes and associated structures, brain, middle ear, parotid gland), and it may be ineffective due to the substantially greater vascularity of the maxillofacial region. However, Durr et al. (19) reported on 10 patients (15 TMJs) with bony ankylosis surgically managed with either costochondral grafts, gap arthroplasty, or debridement of heterotopic bone and treated early postoperatively with radiation, 10 Gy in five fractions. With a mean of 19 months follow-up, 10 of 15 TMJs did not show heterotopic bone development while 5 patients (33%) had recurrence of heterotopic bone. An additional complication identified was parotitis in three patients (30%). The placement of fat grafts around the articulating area of the TMJ provides significantly better results than radiation in preventing fibrosis and heterotopic bone formation (20, 21, 26, 27).
The rationale for placing autologous fat grafts around the TMJ total joint prostheses is to obliterate the dead space present around the joint prosthesis, thus preventing the formation and subsequent organization of a blood clot. Creating this physical barrier, serves to minimize the presence of pluripotential cells, and prevents the formation of extensive fibrosis and heterotopic calcification. It may also isolate any residual reactive tissue from previous alloplastic failure to the periphery of the region, minimizing its formation around the joint components. The net result, as evidenced by the data collected, is a decrease and perhaps elimination of the incidence of heterotopic bone formation and improved jaw function (20, 21).
Fat grafts, however, should not be used as a disc replacement in loaded joints. In our procedure of fat grafting around the prostheses, the graft is not functioning as an articular disc, but only as a filling material to eliminate the dead space. Kohn et al. (32) presented an animal study where meniscectomies were performed and fat grafts placed as an articular disc replacement. Osteoarthritis was evident in all treated joints within 6 months. The authors state that fat is not suitable as a meniscal substitute.
Dimitroulis (26) evaluated 11 patients with 13 ankylosed TMJs that he treated with gap arthroplasty and the gap was filled with autogenous dermis-fat grafts harvested from the groin. Presurgical incisal opening was 15.6 mm and at longest follow-up (average follow-up was 41.5 months) was 35.7 mm. Only one patient reankylosed. These patients were not reconstructed with TMJ total joint prostheses, or any form of hard tissue TMJ reconstruction. The patients had improved jaw function, but there was no evaluation as to occlusal and skeletal outcomes. This study did find the dermis-fat grafts to be successful in treating bony and fibrous ankylosis. Dimitroulis et al. (27) evaluated 15 patients (17 joints) by MRI where dermis-fat grafts had been placed within the TMJs. At 6 months to 2 years postsurgery, fat tissue was identified within or surrounding all of the TMJs.
Merikanto et al. (33) studied the effects of creating cranial defects with placement of fat grafts into the defects. The control defects were not filled. The fat grafted cranial defects showed no bone regeneration while the control defects showed a complete bone fill with lamellar bone. Histologic evaluation of the fat grafted defects showed living fat cells filling the defect. Osteogenesis was inhibited in the fat grafted defects. Saunders et al. (34) demonstrated in mice that free fat grafts go through a period of initial breakdown of fat cells, followed by revascularization, resulting in normal appearing fat, although a smaller volume than originally grafted. In three human subjects who received fat grafts to the lumbar region at surgery, at up to 22 months later at reoperation, there was normal fat tissue although a reduced volume compared to the amount originally grafted, and no evidence of replacement by scar tissue.
Yamaguchi et al. (35) demonstrated the importance of early and adequate revascularization of autogenous fat grafts for maintenance of graft volume and for the production and interaction of adipocyte-derived angiogenic peptides such as vascular endothelial growth factor (VEGF) and leptin, important for graft survival and volume maintenance. Trevor et al. (36) showed there was no demonstrable difference in treatment outcomes following placement of a free fat graft vs. a pedicle fat graft in the surgical sites of dorsal laminectomy and duratomy. They concluded that there was no advantage of the use of a pedicle fat graft over a free graft. Qi et al. (37) demonstrated that at early stages following free fat grafting, the fat showed ischemia. The adipocytes released lipid and dedifferentiated to preadipocytes. After revascularization, the preadipocytes began to absorb lipid and became mature adipocytes. The fat grafts were almost normal at 6 months.
The ultimate fate of the transplanted fat around the TMJ is unknown. Studies of fat transplantation to other anatomic areas show a variable amount of resorption, with a decrease in volume ranging from 20 to 75% (38, 39). As an adjunct to prosthetic joint reconstruction, the ultimate resorption of a portion of the graft may not be detrimental to the result. If the formation of the initial hematoma, fibrosis, and reactive tissue can be prevented, there may be reduced incidence of complications. Clinically, the fat grafts appeared viable with some samples showing strands of collagen present in it, but no evidence of an inflammatory process. The consistency of the tissue around the prosthesis was significantly softer than seen in the nonfat grafted patients. Histologically, viable fat was observed (Fig. 48.23).

Histological examination of a fat graft biopsy taken 4 years after implantation around a TMJ Concepts total joint prosthesis shows viable fat still present without evidence of inflammation, heterotopic bone formation, or significant fibrosis
The technique of graft procurement is straight forward, with minimal potential for complications. The fat grafts are harvested just prior to graft placement, requiring only about 15 min of additional surgical time. However, some surgeons may prefer to have two surgical teams working concurrently so the operation is not prolonged. It is not recommended to harvest the fat grafts prior to beginning the TMJ reconstruction as this would require the grafts to be “on the table” for an extended time period, likely to result in significant loss of graft viability. It will usually take a minimum of 4 h to prepare the TMJs and place the prostheses in bilateral cases, before the fat grafts can be placed. Therefore, procuring the fat graft just prior to placement will maximize graft viability; an important factor for graft survival. If the fat graft placement is delayed (i.e., opposite side in bilateral cases) then the graft is stored on ice until ready for insertion. This improves graft viability.
The most common donor site for harvesting is the abdomen, where there is usually abundant fat for most cases. The most common approaches the authors use include: the supra-pubic incision, the umbilical or trans-naval incision, or approach through a pre-existing scar (C-section, hysterectomy, appendectomy, abdominoplasty) or other previous abdominal surgery scar. However, the fat can be harvested from almost any fat source including buttock, thigh, buccal fat pad, breast, etc.
Autologous fat grafting is a very useful adjunct to prosthetic reconstruction of the TMJ and may prove to be similarly beneficial in autologous reconstruction. Graft procurement is quick and easy, with minimal morbidity. The results of our studies (20, 21) demonstrate the efficacy of TMJ reconstruction with total joint prosthesis and simultaneous autologous fat grafts to the articulating area of the TMJ joints. A statistically significant improvement for fat grafted patients was found regarding MIO and the patient’s perception of the jaw function. The most common complication found in the donor area was seroma or hematoma, which was usually easily treated with aspiration and pressure dressing. TMJ reconstruction with TMJ Concepts total joint prostheses and autogenous fat grafts provides a highly predictable treatment method for patients with nonsalvageable TMJ pathology.
References
Neuber F. Fettransplantation. Chir Kongr Verhandl Deutsche Gesellsch Chir 1893;22:66.
Blair VP. Operative treatment of ankylosis of the mandible. Trans South Surg Assoc 1913;28:435.
Murphy JB. Arthroplasty for intra-articular bony and fibrous ankylosis of the temporomandibular articulation. J Am Med Assoc 1914;62:1783.
Thomas BJ. Heterotopic bone formation after total hip arthroplasty. Orth Clin North Am 1992;23(2):347–358.
Fingeroth RJ, Ahmed AQ. Single dose 6 Gy prophylaxis for heterotopic ossification after total hip arthroplasty. Clin Orthop Relat Res 1995;(317):131–140.
DeFlitch CJ, Stryker JA. Postoperative hip irradiation in prevention of heterotopic ossification: Causes of treatment failure. Radiology 1993;188(1):265–270.
Maloney WJ, Jasty M, Willett C, Mulroy RD, Jr., Harris WH. Prophylaxis for heterotopic bone formation after total hip arthroplasty using low-dose radiation in high-risk patients. Clin Orthop Relat Res 1992;(280):230–234.
Wolford LM, Cottrell DA, Henry CH. Temporomandibular joint reconstruction of the complex patient with the techmedica custom-made total joint prosthesis. J Oral Maxillofac Surg 1994;52(1):2–10.
Wolford LM, Henry CH, Nikaein A, Newman JT, Namey TC. The temporomandibular joint alloplastic implant problem. In: Sessle BJ, Bryant PS, Dionne RA (Eds), Temporomandibular Disorders and Related Pain Conditions, IASP Press, Seattle, WA 1995, pp. 443–447.
Henry CH, Wolford LM. Treatment outcomes for TMJ reconstruction after Proplast-Teflon implant failure. J Oral Maxillofac Surg 1993;51(4):352–358.
Wolford LM. Temporomandibular joint devices: Treatment factors and outcomes. Oral Surg Oral Med Oral Path Oral Radiol Endol 1997;83(1):143–149.
Mercuri LG, Wolford LM, Sanders B, White RD, Hurder A, Henderson W. Custom CAD/CAM total temporomandibular joint reconstruction system: Preliminary multicenter report. J Oral Maxillofac Surg 1995;53(2):106–115.
Mercuri LG, Wolford LM, Sanders B, White RD, Giobbie-Hurder A. Long-term follow-up of the CAD/CAM patient fitted total temporomandibular joint reconstruction system. J Oral Maxillofac Surg 2002;60(12):1440–1448.
Wolford LM. Concomitant temporomandibular joint and orthognathic surgery. J Oral Maxillofac Surg 2003;61: 1198–1204.
Wolford LM, Pinto LP, Cardenas LE, Molina OR. Outcomes of treatment with custom-made temporomandibular joint total joint prostheses and maxillomandibular counter-clockwise rotation. Baylor Univ Med Cent Proc 2008;21:18–24.
Wolford LM. Clinical indications for simultaneous TMJ and orthognathic surgery. Cranio 2007;25(4):273–282.
Wolford LM, Pitta MC, Reiche-Fischel O, Franco PF. TMJ Concepts/Techmedica custom made TMJ total joint prosthesis: 5-year follow-up study. Int J Oral Maxillofac Surg 2003;32(3):268–274.
Wolford LM, Mehra P. Custom-made total joint prostheses for temporomandibular joint reconstruction. Baylor Univ Med Cent Proc 2000;13:135–138.
Durr ED, Turlington EG, Foote RL. Radiation treatment of heterotopic bone formation in the temporomandibular joint articulation. Int J Radiat Oncol Biol Phys 1993;27(4): 863–869.
Wolford LM, Karras SC. Autologous fat transplantation around temporomandibular joint total joint prostheses: Preliminary treatment outcomes. J Oral Maxillofac Surg 1997;55(3):245–251.
Wolford LM, Morales-Ryan CA, Garcia-Morales P, Cassano DS. Autologous fat grafts placed around temporomandibular joint (TMJ) total joint prostheses to prevent heterotopic bone. Baylor Univ Med Center Proc 2008;21:248–254.
Wolford LM, Dingwerth DJ, Talwar RM, Pitta MC. Comparison of 2 temporomandibular joint total joint prosthesis systems. J Oral Maxillofac Surg 2003;61(6):685–690.
Wolford LM. Further comparison of temporomandibular joint prosthesis systems. J Oral Maxillofac Surg 2004;62: 264–269.
Wolford L. Factors to consider in joint prosthesis systems. Baylor Univ Med Cent Proc 2006;19:232–238.
Rattan V. A simple technique for use of buccal pad of fat in temporomandibular joint reconstruction. J Oral Maxillofac Surg 2006;64(9):1447–1451.
Dimitroulis G. The interpositional dermis-fat graft in the management of temporomandibular joint ankylosis. Int J Oral Maxillofac Surg 2004;33(8):755–760.
Dimitroulis G, Trost N, Morrison W. The radiological fate of dermis-fat grafts in the human temporomandibular joint using magnetic resonance imaging. Int J Oral Maxillofac Surg 2008;37(3):249–254.
MacIntosh RB. Costochondral and dermal grafts in temporomandibular joint reconstruction. Oral Maxillofac Clin North Am 1989;1:363.
Hall BK. Cartilage. Biomedical Aspects. New York, Academic Press 1988, pp. 322–323.
Francis MD, Russell RCG, Fleisch H. Diphosphonates inhibit formation of calcium phosphate crystals in vitro and pathologic calcification in vivo. Science 1969;165(899): 1264–1266.
Ritter MA, Gioe TJ. The effect of indomethacin on para-articular ectopic ossification following total hip arthroplasty. Clin Orthop 1982;(167):113–117.
Kohn D, Rudert M, Wirth CJ, Plitz W, Reiss G, Maschek H. Medial meniscus replacement by a fat pad autograft. An experimental study in sheep. Int Orthop 1997;21(4): 232–238.
Merikanto JE, Alhopuro S, Ritsila VA. Free fat transplant prevents osseous reunion of skull defects. A new approach in the treatment of craniosynostosis. Scan J Plast Reconstr Surg 1987;21(2):183–188.
Saunders MC, Keller JT, Dunsker SB, Mayfield FH. Survival of autogenous fat grafts in humans and in mice. Connect Tissue Res 1981;8(2):85–91.
Yamaguchi M, Matsumoto F, Bujo H, Skibasaki M, Takahashi K, Yashimoto S, Kchinose M, Saito Y. Revascularization determines volume retention and gene expression by fat grafts in mice. Exp Biol Med 2005;230(10): 742–748.
Trevor PB, Martin RA, Saunders GK, Trotter EJ. Healing characteristics of free and pedicle fat grafts after dorsal laminectomy and duratomy in dogs. Vet Surg 1991;20(5):282–290.
Qi Z, Li E, Wang H. Experimental study on free grafting of fat particles. Zhonghua Zheng Xing Shal Shang Wai Ke Za Zhi 1997;13(1):54–56.
Carpaneda CA, Ribeiro MT. Study of the histologic alterations and viability of the adipose graft in humans. Aesthetic Plast Surg 1993;17(1):43–47.
Horl HW, Feller AM, Biemer E. Technique for liposuction fat reimplantation and long-term volume evaluation by magnetic resonance imaging. Ann Plast Surg 1991;26(3): 248–258.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2010 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Wolford, L.M. (2010). Autologous Fat Grafts Placed Around Temporomandibular Joint (TMJ) Total Joint Prostheses to Prevent Heterotopic Bone. In: Shiffman, M. (eds) Autologous Fat Transfer. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-00473-5_48
Download citation
DOI: https://doi.org/10.1007/978-3-642-00473-5_48
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-00472-8
Online ISBN: 978-3-642-00473-5
eBook Packages: MedicineMedicine (R0)