
Abstract
Supplemental melatonin is one of the most commonly recommended biomedical agents for difficulty falling asleep or maintaining sleep in children with neurodevelopmental disorders. This chapter provides an overview of melatonin, its synthesis, and its biological properties. Dosing of melatonin in sleep disorders, its pharmacokinetics, side effects, and potential drug interactions are discussed. Available data on the use of melatonin for sleep in specific neurodevelopmental populations including autism, attention-deficit/hyperactivity disorder, Angelman syndrome, Rett syndrome, fragile X syndrome, tuberous sclerosis, epilepsy, and traumatic brain injury is reviewed.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Melatonin
- Circadian rhythm
- Autism
- Attention-deficit/hyperactivity disorder
- Angelman syndrome
- Rett syndrome
- Fragile X syndrome
- Tuberous sclerosis
- Epilepsy
- Traumatic brain injury
- Insomnia
- Sleep problems
Introduction
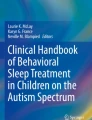
Melatonin is an endogenous neurohormone. It was first isolated from the pineal gland by Lerner et al. in 1958 [1]. While the majority of melatonin circulating in the blood is produced by the pineal gland, there is evidence that it is also made in other body sites including the skin, lymphocytes, bone marrow, thymus, platelets, retina, and gastrointestinal tract [2, 3]. Melatonin production is regulated by light-dark cycles which set the circadian rhythm of the suprachiasmatic nuclei (SCN) via the retinohypothalamic tract [4, 5]. Melatonin synthesis is activated during darkness and suppressed by light. In darkness, norepinephrine is secreted and acts on beta-adrenergic receptors in pinealocytes, resulting in an increase in cyclic adenosine monophosphate (cAMP), the transcription of arylalkylamine N-acetyltransferase (AANAT), the rate-limiting enzyme in melatonin synthesis, and thus melatonin production [6]. In a person with a normal circadian rhythm, the secretion of melatonin begins 2 h before routine sleep onset (the dim light melatonin onset or DLMO), is elevated during the night, and is minimal during the day. On the biochemical level, synthesis of melatonin occurs in a four-step reaction beginning with tryptophan, which is converted into 5-hydroxytryptophan, then serotonin, followed by N-acetylserotonin, and finally melatonin (N-acetyl-5-methoxytryptamine) [2] (Fig. 31.1).

Melatonin physiology. (a) Melatonin production is suppressed by light and stimulated by darkness. Nerve fibers travel from the retina through the retinohypothalamic tract to the suprachiasmatic nucleus (i.e., the “biologic clock”) in the hypothalamus. They continue through the paraventricular nuclei down to the superior cervical ganglion in the cervical spinal cord and back up to the pineal gland. (b) In the pineal gland, melatonin synthesis involves a four-step conversion process beginning with tryptophan. (c) An example of melatonin’s circadian pattern. Two hours before routine sleep onset, melatonin production increases in the pineal gland, marking the dim light melatonin onset (DLMO). Melatonin secretion peaks in the middle of the night and declines by morning
Melatonin has been found to have anxiolytic, antioxidant, free radical-scavenging, anti-inflammatory, antiproliferative, circadian entrainment, and hypnotic properties [2, 7, 8]. Its sedative effect comes from the binding of melatonin to the MT1 receptor, while circadian phase shifting effects come from binding of melatonin to the MT2 receptor [9]. The first report in the literature of melatonin being used for sleep in a child was in 1991 when Palm et al. entrained the circadian rhythm of a 9-year-old boy with intellectual disability who was blind and had a free-running circadian rhythm [10].
Pharmacokinetics of Melatonin
Melatonin is lipophilic [2]. It rapidly enters cells and crosses the blood-brain barrier [2]. Oral melatonin at doses of 2 and 4 mg has poor absolute bioavailability (only 15% of the dose makes it into the systemic circulation) thought to be due to poor oral absorption and/or large first-pass metabolism [8]. Normal physiologic levels of melatonin range from 60 to 300 pg/mL [11]. Administration of 0.3 mg of melatonin 2–4 h prior to habitual bedtime results in normal physiologic levels of melatonin [12]. Melatonin’s onset of action is fast with a Tmax of 30–60 min [13]. It has a short half-life of 30–60 min [2]. Immediate release oral melatonin maintains plasma melatonin levels above normal physiologic levels for 3–4 h while slow release oral melatonin maintains such levels for 5–7 h after ingestion [14]. Melatonin is metabolized in the liver by the cytochrome P450 enzyme CYP1A2 into 6-hydroxymelatonin [15]. It is then conjugated with sulfate into 6-sulphatoxymelatonin and excreted in the urine [15]. There is some evidence that prepubertal children metabolize melatonin faster than adults do and thus may require a higher dose of melatonin [4, 16].
Treating with Exogenous Melatonin
In the United States, supplemental melatonin is widely available over the counter (OTC) in multiple formulations (it is not available over the counter in many European countries such as the United Kingdom). These include immediate release tablets, slow release tablets, dual layer immediate and slow release tablets, dissolvable tablets, capsules, lozenges, liquids, sprays, dissolving strips, and gummies that may be taken orally. Some of the dissolvable tablets, liquids, and sprays are labeled to be taken sublingually for rapid absorption and to bypass first-pass metabolism for rapid onset. Crushed tablets dissolved in water and liquid melatonin may be administered per gastrostomy tube. If mixed into solution, melatonin will remain stable for up to 6 h at room temperature [17]. Body creams, lotions, and a transdermal patches are also available. Melatonin is typically sold in the following strengths: 0.3 mg (or 300 mcg), 0.5 mg, 1 mg, 1.5 mg, 2.5 mg, 3 mg, 5 mg, 10 mg, and 20 mg.
The burgeoning of melatonin formulations has likely been enabled by the categorization of melatonin as a dietary supplement in the United States as opposed to a medication. It is thus not subject to the rigorous Food and Drug Administration regulations to which prescription medications are held. This has opened up the market to melatonin products containing many other herbal supplements (e.g., valerian root, chamomile flower powder, magnesium, gamma-aminobutyric acid, vitamin B-6) that are also not tightly regulated. Consequently, there have been concerns for impurities and the accuracy of the melatonin strength on product labels. In June of 2007, the Food and Drug Administration issued a ruling requiring “current good manufacturing practices,” giving companies until June 2010 to put into place quality control procedures that eliminate contaminants and impurities and allow for accurate strength labeling. However, a 2017 study from Canada showed that melatonin content varied by −83% to +478% compared to the dose reported on the label [18]. This variability was not unique to specific formulations or brands, and in fact, lot to lot variability in a brand could be as high as 465% [18]. Of their 30 samples, 26% were found to contain serotonin, which at inappropriate doses can have harmful side effects [18]. To mitigate this issue, families may opt for “pharmaceutical grade” melatonin which can be acquired online [19]. Most melatonin available OTC in the United States is synthetic in order to avoid potential virus transmission from animal products [20]. Manufacturers are required to label their melatonin source if it is from a plant or animal [21]. It can otherwise be assumed that the melatonin is synthetically derived [21], but if there is any question or concern, it would be best to call the manufacturer for verification.
Dosing
There are no universal guidelines on dosing of melatonin. When melatonin is used to advance one’s circadian rhythm, it is most effective if given at the lower dose of 0.5 mg 5 h before the DLMO [22, 23]. Pediatric studies aiming to correct sleep onset and sleep maintenance issues have generally used doses of 2.5 mg up to 10 mg [2, 24]. In Jan et al.’s study, infants and toddlers were started on 2.5 mg of melatonin while older children were started on 5 mg [24]. An 11-month prospective, naturalistic, observational study of melatonin use in children with intellectual disability, ADHD, or autism who had not responded to behavioral interventions for sleep started subjects on a dose of 2.5 mg 30 min before bedtime [25]. If a subject showed no response to melatonin, then the dose was increased at 4-week intervals to a maximum dose of 10 mg. The researchers found that increasing the melatonin dose above 6 mg only benefitted a small percentage of children (9% of their study population). However, doses as high as 12 mg have been used in other studies [26, 27]. Even melatonin at very high doses does not result in uncontrollable sedation [6], but clinically, it is better to maintain a patient’s dose in the conventionally used ranges discussed above.
There is considerable interindividual variation in response to melatonin. The optimal dose of melatonin has not been found to be related to age or weight [28]. Thus there is not a standard mg per kg dosing recommendation for melatonin. Ways of predicting a clinically effective dose in a patient have not been identified. The therapeutic dose is essentially determined by clinical responsiveness; thus, follow-up with the prescribing provider is recommended [29]. Studies tend to show that melatonin is more useful for sleep induction as opposed to sleep maintenance [24]. For a sedating effect to help induce sleep, melatonin may be given 30–60 min before desired bedtime [15]. Typically, response to melatonin for sleep induction is experienced within days of starting it [4]. In an open-label, dose-escalation study of melatonin use in children with autism spectrum disorders, response to melatonin was typically seen within the first week of use [28].
Over time, some people find that melatonin’s sedating effect “no longer works” for them. It is natural to assume that one has developed a tolerance to melatonin and to respond by increasing the melatonin dose. However, Braam et al. found that an increased melatonin dose did not improve responsiveness, and thus did not believe that tolerance was the issue [15]. A prospective long-term study of children on melatonin (mean duration of use over 4.3 years) did not show loss of melatonin efficacy over time, suggesting that responders do not typically develop a tolerance to melatonin [29]. Additionally, in a study of 107 children with an autism spectrum disorder, 7 children had initial improvement in their sleep with melatonin, but the problem returned after 3–12 months of use even though they increased the melatonin dose [30]. Interestingly, Braam et al. found that melatonin clearance tests on subjects who stopped responding to melatonin suggested that these subjects were slow metabolizers of melatonin [15]. They theorized that being a slow melatonin metabolizer results in the accumulation of melatonin and that high levels of melatonin resulted in a loss of circadian rhythmicity, rendering the exogenous melatonin ineffective. Furthermore, those subjects who stopped responding to melatonin improved after their melatonin dose was lowered. A follow-up study showed that slow metabolizers of melatonin were likely due to certain single nucleotide polymorphisms in the CYP1A2 gene [31]. In the general population, about 12–14% of individuals have a slow melatonin metabolizer phenotype [31].
Once a good sleep schedule has been established for at least 6 weeks, providers can consider stopping the melatonin [32]. Chemical dependence, withdrawal, and abuse have not been observed for melatonin [33]; thus a slow tapering schedule is not necessary. However, providers may consider a taper to see what a patient’s ability to sleep without melatonin is. There are some children who have such poor neuromodulation of their sleep that they need to be on melatonin throughout their lifetime in order to sleep.
Safety of Melatonin
Melatonin use appears to be fairly benign [2, 34]. An acute toxicity study of melatonin in rats and mice showed that the median lethal oral dose (LD50 oral) was very high at 1250 mg/kg for the mouse and >3200 mg/kg for the rat (researchers essentially could not find the LD50 oral for the rat) [35]. This study also found that the sedative effect of melatonin occurred at doses far lower than doses necessary to cause neurotoxicity. In a randomized, double-blind study of adult men on 10 mg of melatonin versus placebo for 28 days, there were no significant changes in measures including complete blood count, comprehensive metabolic panel, cholesterol levels, urinalysis, T3, T4, thyroid-stimulating hormone (TSH), luteinizing hormone (LH), follicle-stimulating hormone (FSH), cortisol, and melatonin [36]. In girls with Rett syndrome, blood work including a complete blood count, chemistry, and liver function tests prior to melatonin (doses of 2.5 up to 10 mg were used) use and after a 4-week treatment period on melatonin did not show any adverse effects [11]. Miyamoto et al. followed complete blood counts, urinalyses, serum chemistries, LH, FSH, prolactin, and estradiol in two children with Rett syndrome on melatonin [37]. Over 2 years, no adverse effects were observed. In Malow et al.’s 14-week trial of melatonin in 24 children with an autism spectrum disorder, there were no changes in complete blood count, metabolic panels including liver and renal function, adrenocorticotropic hormone (ACTH), cortisol, estrogen, testosterone, FSH, LH, or prolactin [28].
There are a few long-term studies of chronic melatonin usage in children. The use of supplemental melatonin in children began fairly recently, starting in the early 1990s [10]. In 1996, Jan et al. reported no adverse consequences of taking melatonin over the course of 4 years in a group of 100 subjects [24]. They ranged in age from 3 months to 21 years and had taken melatonin in the dose range of 2.5–10 mg [24]. A prospective study on 41 subjects who had used melatonin over a mean duration of 4.3 years did not find any safety concerns [29]. Questionnaire-based follow-up of melatonin use in 94 children with ADHD over 3.7 years showed that only 1/5 of subjects had adverse events; however, most complaints were mild, and the study did not distinguish whether these adverse events were from melatonin use or other medications (such as stimulants) that subjects could have been taking [33].
Side Effects of Melatonin
Side effects of melatonin are relatively mild and, when compared to placebo in studies, tend to occur at similar rates [4, 38]. Symptoms that have been reported more commonly include headaches, dizziness, nausea, diarrhea, enuresis, rash, hypothermia, tiredness, fogginess, and daytime sleepiness [4, 21, 39]. These side effects may resolve after initial treatment and generally do not result in the patient discontinuing the melatonin [39]. In this author’s unpublished clinical experience, an increase in sleep terrors is sometimes seen with onset of melatonin use. Sleep terrors typically occur out of N3 sleep. It is possible that this initial increase in sleep terrors is because more N3 sleep has been seen in the context of higher melatonin levels [3].
Melatonin has been found to have some properties that have not been reported as significant side effects, but they are worth noting and being mindful of. For example, it has been observed to inhibit platelet aggregation [4]. Melatonin has also been found to lower blood pressure [40]. It can potentially have an adverse effect on mood [4, 11]. Whether or not melatonin exacerbates asthma in patients with nocturnal asthma is controversial [41]. Nocturnal asthma is believed to have a circadian pattern with increased airway inflammation at night [41]. It has been postulated that melatonin is pro-inflammatory, mediating this nocturnal airway inflammation [41]. A randomized, double-blind, placebo-controlled study of melatonin (dose of 3 mg) use in women with mild to moderate asthma for 4 weeks did not find any difference in asthma symptoms compared to placebo [42]. What this study did find was that melatonin improved sleep in subjects with asthma. In a randomized, double-blind, placebo-controlled study of 22 children with an autism spectrum disorder on a 3-month treatment period of melatonin, no asthma attacks were reported [38]. While further investigation is necessary, melatonin can still be considered as a sleep aid in patients with asthma [41] as long as the prescribing provider is aware of this potential side effect and thus knows to monitor and stop the melatonin if asthma exacerbations indeed increase on melatonin.
There has been a question of whether or not melatonin use affects pubertal development. Waldhauser and Steger looked at melatonin levels in 280 subjects and found that levels were low in early infancy, increased to their highest levels around 1–3 years of age, and dropped by about 75% until young adulthood at which time they remained stable [43]. This led to theories that in the prepubertal years, higher melatonin levels inhibit pubertal development and that a decline in melatonin results in the onset of puberty [4, 44]. Clinical data has not supported the theory that exogenous melatonin affects pubertal development (e.g., stopping exogenous melatonin has not resulted in precocious puberty, and long-term use of exogenous melatonin has not resulted in the delay of pubertal development). A Dutch study looked at long-term exogenous melatonin use in prepubertal children [45]. The mean duration of exogenous melatonin use was 3.1 years, and the mean dose of melatonin used was 2.7 mg (minimum dose of 0.3 mg and maximum dose of 10 mg). Of 59 children included in the study, Tanner stage information was available on 46 of the children. The authors concluded that long-term exogenous melatonin use did not affect the timing of pubertal development in their study population.
Drug Interaction
Drugs that affect norepinephrine levels or its action can affect melatonin secretion. For example, beta-blockers and alpha-2 agonists decrease melatonin production [6]. Tricyclic antidepressants that inhibit norepinephrine reuptake increase melatonin production [6]. Fluvoxamine and cimetidine can inhibit CYP1A2 and thus increase melatonin concentrations [21]. On the other hand, melatonin can inhibit CYP1A2 and CYP3A; thus medications metabolized by these enzymes can be increased in concentration if used with melatonin [21]. As discussed above, melatonin has the potential to decrease blood pressure. This should be taken into consideration when melatonin is used in conjunction with antihypertensives [21].
Case Vignette
Sarah was a 4-year-old girl with autism who was nonverbal and had been a “good sleeper” in infancy. When she was 2 years of age, she began to take longer to settle to sleep. Her parents had a firm bedtime routine that ended at 8 PM in her room with her being placed in her crib in the dark to sleep. On the baby monitor, they could see that she remained awake for hours playing in her crib or engaging in self-stimulatory behaviors, typically falling asleep at 12 AM. She woke at 6 AM for the day and did not take naps during the day. Melatonin was initiated at 1 mg given 30 min before bedtime. Her parents felt that it made her calmer, but did not help her fall asleep. The melatonin dose was thus increased and eventually titrated up to 3 mg given 30 min before bedtime, and she was able to fall asleep with this dosage by 9 PM. While she was only getting 9 h of sleep per night, her parents felt that this was a great improvement and continued her on this regimen. One month after achieving this improved sleep schedule, Sarah returned to clinic. Her parents reported that she was no longer responding to the melatonin. The melatonin dose was decreased to 0.5 mg 30 min before bedtime. On this dose, she was again able to fall asleep by 9 PM. On follow-up at 3 and 6 months, she continued to do well on the lowered melatonin dose.
Use of Melatonin in Special Populations
Available data on melatonin use for sleep problems in specific groups of neurodevelopmental disorders is reviewed in the remainder of this chapter. Due to the rarity of many of the diagnoses or challenges in study recruitment, many of the studies were small, including the gold standard randomized, double-blind, placebo-controlled studies.
Autism
The estimated prevalence of sleep problems in children with an autism spectrum disorder (ASD) is 44–83% with falling asleep and/or maintaining sleep being the most common issue [46]. The etiology of these difficulties sleeping is unclear. Multiple factors may affect sleep in children with autism including sleep fragmentation from seizures, side effects of medications taken for comorbid conditions, difficulty transitioning from one activity to another, anxiety, hyperarousal, and environmental conditions that affect the influence of zeitgebers or environmental cues that entrain the circadian rhythm (e.g., light exposure). Melatonin has drawn significant interest in the arena of autism research, originally for the biomedical model that melatonin hypersecretion could lead to autism [47]. However, the current focus is on melatonin and sleep and the potential that aberrations in melatonin could contribute to their sleep difficulties.
Compared to controls, children with ASD have been documented to have lower nocturnal melatonin levels [48,49,50,51]. The primary metabolite of melatonin, 6-sulphatoxymelatonin (6-SM), has also been found to have lower diurnal and nocturnal excretion rates in children with ASD compared to typically developing controls [52]. Additionally, polymorphisms in the acetylserotonin methyltransferase (ASMT) gene have been associated with decreased ASMT transcripts and activity (ASMT is the last enzyme in the melatonin synthesis pathway) [50]. However, studies documenting these low endogenous melatonin levels have not examined subjective or objective sleep measurements in these patients. In a study of 23 children (aged 4–10 years) with well-characterized ASD, 9 of whom had none or mild sleep concerns and 15 of whom had moderate to severe sleep issues, low nocturnal 6-SM levels were observed [3]. Interestingly, the low nocturnal 6-SM levels did not correlate with any subscales on the Children’s Sleep Habits Questionnaire that suggested difficulty sleeping (e.g., the Bedtime Resistance, Sleep Onset Delay, Sleep Duration or Sleep Anxiety subscales) [3]. Also, a pharmacokinetic study of endogenous and exogenous melatonin in nine children (aged 3–10 years) with confirmed diagnoses of ASD and a history of sleep onset insomnia showed that pretreatment endogenous melatonin levels were not abnormal [53]. Despite their normal endogenous melatonin profiles, these children still had improvement in their sleep on supplemental melatonin. It is possible that the discrepancy between melatonin levels occurred because one measured melatonin in platelets while another measured melatonin in serum and others measured urinary 6-SM levels. It is possible that a subset of children with ASD have low melatonin levels. It is also possible that the low melatonin and low nocturnal 6-SM levels have some other significance in ASD. A study found that specific single nucleotide polymorphisms (SNPs) in ASMT and CYP1A2 caused decreased ASMT expression (by virtue of which one would expect decreased melatonin) and decreased CYP1A2 enzyme activity, respectively, and that both were associated with sleep onset delay in children with ASD [54]. Perhaps the method by which melatonin helps children with ASD sleep is more convoluted than simple repletion of deficient melatonin levels. On the other hand, it could be as simple as melatonin exerting its hypnotic property.
Melatonin is commonly recommended by physicians for individuals with ASD. In an analysis of three survey studies, the overall prevalence of physicians making this recommendation was 32.4% [55]. Melatonin has largely been found to be helpful in managing difficulty with sleep onset for children with ASD. While starting melatonin can completely resolve insomnia in a child with ASD, it is also common for it to improve but not fully resolve. In Andersen et al.’s study of 107 children with ASD aged 2–18 years on a maximum dose of 6 mg of melatonin, only 25% reported full resolution of sleep issues while 60% reported that melatonin helped, but had not fully fixed the sleep problem [30].
Some studies have shown that night wakings in their study population improved [53, 56], but this is not typical for melatonin. Interestingly, in a study by Goldman et al., a child who routinely woke up at 2 AM stopped doing so on melatonin, even though pharmacokinetic profiles of her melatonin levels showed that on 1 mg of supplemental melatonin, her melatonin level had fallen to the same level as her endogenous melatonin level by 2 AM and that on 3 mg of supplemental melatonin, her melatonin level had fallen to her endogenous level by 5 AM [53].
A few randomized, double-blind, placebo-controlled crossover studies of melatonin for sleep problems in children with ASD have been done [27, 38, 56, 57]. While 3 of these studies were small, with sample sizes ranging from 11 to 22 [38, 56, 57], one multicenter trial had a sample size of 146 [27]. In these studies, children ranged in age from 2 to 16 years [27, 38, 56, 57]. Doses of melatonin used in these studies ranged from 0.5 to 12 mg [27, 38, 56, 57]. Treatment periods ranged from 2 weeks to 3 months [27, 38, 56, 57]. Sleep data was typically obtained from sleep diaries/charts and questionnaires with two of the studies including actigraphy as an objective sleep measure [27, 38, 56, 57]. These studies showed that the children tended to fall asleep earlier and faster and had longer total sleep times [27, 38, 56, 57]. With the exception of one of the studies, night wakings were not improved [27, 38, 56, 57]. Two of the studies specifically had study populations that had failed behavioral intervention for their severe difficulty sleeping [27, 38]. A further meta-analysis included three of the above-described randomized, double-blind, placebo-controlled crossover studies and two additional studies not described above, because they included children with other neurodevelopmental disabilities; however, the meta-analysis only included individuals with ASD [55]. This meta-analysis found that compared to baseline sleep, total sleep duration improved by 73 min; compared to placebo, total sleep duration in children taking melatonin improved by 44 min; compared to baseline, use of melatonin improved sleep onset latency by 66 min; and compared to placebo, sleep onset latency improved by 39 min [55]. In addition to the five studies used in the meta-analysis, Rossignol et al. also reviewed 13 additional uncontrolled trials of exogenous melatonin use [55]. Of the 18 total studies, 7 reported no side effects, and in the remaining studies, side effects were either transient or mild [55].
Although there are children with ASD and severe sleep problems that do not respond to behavioral management, physicians should always include behavioral interventions as part of their management. Cortesi et al. studied 160 children with ASD aged 4–10 years [58]. Their study was designed to have three treatment arms: (1) controlled release melatonin, (2) four sessions of cognitive behavioral therapy, and (3) a combination of controlled release melatonin and cognitive behavioral therapy. These treatment arms were compared to a placebo group. All treatment arms showed improvement in their sleep, but the combination of controlled release melatonin and cognitive behavioral therapy showed the most improvement with the most treatment responders and fewest dropouts.
ADHD
As many as 50% of children with attention-deficit/hyperactivity disorder (ADHD) have a sleep problem [59]. Sleep problems in children with ADHD include bedtime resistance, prolonged sleep onset, fragmented sleep, being tired in the morning, daytime sleepiness, restless legs syndrome, periodic limb movement disorder, and sleep disordered breathing [59, 60]. While issues with sleep onset are easy to blame on stimulant medication side effects, it is apparent that these issues can exist even in the absence of these medications. In children without ADHD who are medication-free, the prevalence of sleep onset insomnia is estimated to be 28% [33]. It is hard to know whether poor sleep begets ADHD or vice versa.
Melatonin has been shown to help with the sleep of children with ADHD and sleep onset insomnia. Van der Heijden et al. conducted a randomized, double-blind, placebo-controlled trial of 3 or 6 mg of melatonin (depending on weight) versus placebo in 105 medication-free children (aged 6–12 years) with ADHD [61]. DLMO advanced by a mean of 44 min on melatonin, and sleep onset advanced by about 27 min. Total sleep time increased by 20 min.
Being on a stimulant medication does not necessarily prevent melatonin from helping with a child’s sleep. Weiss et al. conducted a randomized, double-blind, placebo-controlled crossover trial of melatonin in 27 children with ADHD on stimulant medication aged 6–14 years whose sleep problems had not improved with sleep hygiene methods [62]. With 5 mg of melatonin given 20 min before bedtime, their sleep onset latency was found to decrease from a mean of 62 min down to 46 min. Further improvement in sleep onset latency was observed in those who continued melatonin in the 90 days post-trial.
Hoebert et al. found that melatonin was effective in improving sleep in children with ADHD and insomnia in 88% and that stopping the melatonin resulted in the return of sleep onset insomnia in 92% (subjects were to stop it for 1 week every year to see if it was still needed) [33]. Parents reported the additional benefit of improved mood and behavior [33].
Down Syndrome
The prevalence of sleep problems in children with Down syndrome is as high as 76% [63]. Research studying the use of melatonin specifically to treat their sleep problems has not been reported in the literature. A comparison of 24-h urinary 6-hydroxymelatonin sulfate levels in subjects with and without Down syndrome showed no significant differences between groups; thus they appear to exhibit normal diurnal and nocturnal melatonin secretion patterns [64]. Interestingly, research on long-term use of melatonin in Down syndrome has focused on its potential neuroprotective properties that could thus reduce cognitive decline [65].
Angelman Syndrome
Angelman syndrome results from loss of maternal genetic material in the 15q11–13 chromosomal region [66]. The most common maternal genetic deletion in this region that results in Angelman syndrome involves the UBE3A gene [67]. Sleep problems are common in this population with a prevalence rate of 50–90% [67]. Sleep problems in children with Angelman syndrome include difficulty settling at bedtime, night wakings, and circadian rhythm disorders [66, 67]. These sleep issues can become remarkably worse in the 2–6-year-old age range [67].
Two small studies have shown that melatonin can be helpful in sleep onset and maintenance problems in children with Angelman syndrome. Zhdanova et al. monitored 7 days of baseline sleep in 13 children with Angelman aged 2–10 years, then on 0.3 mg of melatonin 30–60 min before habitual bedtime for 5 days [68]. The total sleep time improved in these children as did their melatonin levels. During the baseline period, peak serum melatonin levels ranged from 19 to 177 pg/mL. The use of exogenous melatonin elevated peak serum melatonin levels to 128–2800 pg/mL. Braam et al. conducted a randomized placebo-controlled study on eight children with Angelman and chronic idiopathic insomnia [66]. Their baseline sleep pattern was observed for 1 week, and then the subjects received melatonin (2.5 mg at 6 PM in children <6 years and 5 mg at 7 PM in children ≥6 years of age) or placebo for 4 weeks [66]. Caregiver report of sleep parameters (recorded on sleep diaries) showed that sleep latency decreased by 32 min, sleep onset occurred 28 min earlier than usual, and total sleep time improved by an average of 56 min [66]. Number of nights with wakings decreased from 3.1 nights per week to 1.56 nights per week [66]. Salivary melatonin levels were higher after taking exogenous melatonin [66]. In this study, caregivers reported that they were satisfied with the improvement in their child’s sleep, that their child was easier to manage during the day, and that children were less sleepy and more attentive [66].
Melatonin may also benefit children with Angelman syndrome who have a circadian rhythm sleep disorder (CRSD). Takeasu et al. examined CSRD and serum melatonin patterns in 15 Angelman subjects [67]. Eight of them had a CRSD. Six of these subjects took 1 mg of melatonin between 6 PM and 7 PM for 3 months. This intervention improved sleep in the subjects who had a free-running circadian rhythm and irregular sleep/wake rhythm, increasing total nocturnal sleep time by more than 80%. Melatonin did not improve the sleep of the two subjects who had delayed sleep phase type. While the expected negative correlation between age and melatonin level was observed in controls, it was not observed in those with Angelman syndrome. Instead, serum melatonin levels were found to be lower in children with Angelman than controls throughout the night, suggesting that their melatonin levels are low well before puberty. Interestingly, the UBE3A gene involved in the etiology of Angelman syndrome is an ubiquitin ligase which affects control of proteins involved in circadian regulation [67]. Reduction in the expression of UBE3A may result in the circadian rhythm disorders seen in Angelman. In fact, a drosophila model of Angelman syndrome consisting of a UBE3A mutation exhibits a free-running circadian rhythm [69].
Rett Syndrome
More than 80% of children with Rett syndrome have problems with their sleep, and these issues tend to be lifelong [11]. These problems include irregular sleep/wake schedule, night wakings, and decreased total sleep time [11]. In a study by McArthur et al., 1 week of actigraphy data to look at baseline sleep/wake patterns showed a mean sleep onset latency of 42 min and about 15 awakenings per night [11]. The severity of sleep problems have not been found to correlate with the child’s age or stage of Rett syndrome [11]. Nor have conventionally used medications been found to consistently improve the sleep of children with Rett syndrome [11]. Melatonin has also been inconsistent in helping with the sleep of children with Rett syndrome.
Miyamoto et al. treated one child with Rett syndrome who had a free-running circadian rhythm and another who had fragmented sleep with screaming at night with 5 mg of melatonin [37]. Melatonin helped the child with the free-running circadian rhythm more so than the child who had night wakings. Additionally, the child with night wakings continued to have early morning awakenings which did not respond to increasing the melatonin dose. In both subjects, the progress that was made on the melatonin was lost when the melatonin was stopped. The subjects were reinitiated on 3 mg of melatonin each night, and their sleep problems improved again.
McArthur et al. conducted a double-blind placebo-controlled crossover trial of melatonin in nine girls with Rett syndrome with a mean age of 10.1 years [11]. Melatonin dosages were determined by weight (2.5 mg for 15–25 kg subjects, 5 mg for 25–30 kg subjects, 7.5 mg for 35–45 kg subjects, and 10 mg for >45 kg subjects). For the first 3 weeks of melatonin treatment, actigraphy data showed that subjects had improved sleep onset latencies compared to placebo (about 32 min on placebo vs. 19 min on melatonin). In the fourth week of melatonin treatment, this benefit was not observed. They postulated that this was because melatonin had worked by advancing the subjects’ circadian rhythms. Melatonin did not appear to improve sleep in all of the subjects; however, the total sleep time and sleep efficiencies improved in the subjects who had the worst sleep. While it may still be useful to trial a subject with Rett syndrome and sleep problems on melatonin, it is possible that the cause of sleep issues in Rett syndrome is unrelated to melatonin pathology.
Between the two studies described above, the only side effect reported was from one parent who reported that their child had “severe mood swings” during a 4-week trial of melatonin [11].
Tuberous Sclerosis
Severe sleep problems are common in tuberous sclerosis. In a survey study of caregivers, 60% reported that their child with tuberous sclerosis had difficulty settling to sleep, and 62% reported that their child had night wakings [34]. The etiology of the severe sleep problems is unknown. It is likely that it is multifactorial in nature with factors including challenging behavior, learning difficulties, sleep disruption from epilepsy, and side effects of anti-epileptic medications [34, 70, 71]. Sleep problems in children with tuberous sclerosis do not seem to respond to conventionally used behavior techniques or sedatives [34, 70]. On the contrary, these sedatives tend to increase their hyperactivity [70].
Trials of melatonin using 5–10 mg doses have shown mild benefit to children with tuberous sclerosis and problems sleeping. Melatonin was shown to improve total sleep time [34, 70, 71], but not number of night wakings [71]. In a comparison of 5 mg vs. 10 mg dosing of melatonin, children on 10 mg of melatonin fell asleep an average of 10 min faster than children on 5 mg of melatonin [71]. However, the higher dose of melatonin did not bring any added benefit to total sleep time or number of night wakings. No adverse side effects from the melatonin were reported.
Melatonin secretion patterns appear to be normal in children with tuberous sclerosis [70]. The sleep benefit that patients with tuberous sclerosis see after taking melatonin is suspected to be from melatonin’s sedating property [34, 70].
Epilepsy
The topic of melatonin and epilepsy is complex as there is the potential that melatonin has many different roles in this population. Melatonin has been studied in children with epilepsy as a hypnotic to improve sleep. It has been observed to have a possible pro-convulsant effect. There has also been much interest in melatonin for its possible anticonvulsant effect.
Poor sleep is common in children with epilepsy. Both seizures and anti-epileptics have the potential to cause sleep problems in children with epilepsy. Seizures can result in sleep fragmentation, increased wake time after sleep onset, and a change in their circadian rhythm [71, 72]. Anti-epileptic medications can affect melatonin levels and, thus, sleep. For example, valproic acid has been shown to decrease melatonin levels in healthy young adults [11]. Phenobarbital delays the rate-limiting step of melatonin synthesis and induces the enzyme that breaks melatonin down [11].
Small studies have investigated whether melatonin helps improve sleep in children with epilepsy. Uberos et al. looked at melatonin usage in ten children with severe epileptic disorders including West syndrome, Lennox syndrome, progressive myoclonic epilepsy, epileptic encephalopathy from hypoxic ischemic encephalopathy, and epilepsy from cytomegalovirus [72]. Their sleep diagnoses included irregular sleep/wake pattern, advanced sleep phase syndrome, and delayed sleep phase syndrome. Subjects were given placebo for 1 week and then 3 mg of melatonin 30 min before bedtime for 3 months. Actigraphy data showed that subjects receiving melatonin had an improved sleep latency, increased total sleep time, and improved sleep efficiency. Coppola et al. performed a randomized, double-blind, placebo-controlled, crossover trial to look at the efficacy of melatonin in improving sleep in 25 subjects with intellectual disability aged 3.6–26 years, some of whom had epilepsy [26]. Subjects were randomized to fast release oral melatonin or placebo. They were started on 3 mg of melatonin and titrated by 3 mg/week up to a maximum dose of 9 mg if needed. Melatonin was observed to improve sleep latency, but did not improve nocturnal awakenings or total duration of daytime sleep. In Elkhayat’s study of children with epilepsy, 1.5 mg of oral melatonin was given 30 min before bedtime for 3 months [73]. On melatonin, there was improvement in bedtime resistance, sleep duration, sleep latency, frequency of nocturnal awakenings, sleepwalking, and daytime sleepiness.
Sheldon conducted a study on six children aged 9 months to 18 years with multiple neurological deficits including a history of epilepsy, which was present in five of the six subjects, and severe sleep problems [74]. The intention was to see if 5 mg of melatonin given at bedtime improved sleep in these subjects. When treated with melatonin, five out of six subjects had improvement in sleep onset latency, sleep maintenance, and total sleep time. Although sleep improved, four of the subjects also had either an increase in their seizure activity or onset of a new type of seizure activity. After melatonin was discontinued, the seizure frequency or type of seizure reverted back to what it was prior to melatonin treatment. Three of the subjects were rechallenged with 1 mg of melatonin, and the change in seizure frequency or seizure type recurred, only to again stop with discontinuation of the melatonin.
On the other hand, there are other studies showing no effect of melatonin on seizures. In a study by Carr et al., 19 of 41 children had a seizure disorder, but chronic use of melatonin did not result in more seizures, and there were no subjects with new seizures [29]. In Hancock’s study, five subjects had seizures, and there was no change in seizure frequency compared with baseline before melatonin use [71].
While Sheldon’s study showed a potential pro-convulsant effect of melatonin, there is also data to suggest that melatonin can have an anticonvulsant effect. In Mongolian gerbils, pinealectomy resulted in onset of seizure activity [75]. However, treating pinealectomized Mongolian gerbils with melatonin resulted in a decline in seizure activity [76]. Additionally, when rats received intraventricular injection of anti-melatonin antibody, epileptiform activity was seen [77]. This data suggests that melatonin exerts an anticonvulsant effect. There are multiple potential ways in which melatonin could do this. It is possible that melatonin simply improves sleep quality and thus increases central motor seizure inhibition. Melatonin has been found to enhance GABAergic inhibitory neurotransmission [2], an important mechanism of action for many anti-epileptic drugs [78]. Interestingly, melatonin levels have been found to increase during seizures, suggesting that melatonin may be an endogenous anticonvulsant [78].
Studies have shown mixed results on how well melatonin helps to control seizures. Studies by Elkhayat et al. and Coppola et al. showed mixed effects of melatonin on seizures. Elkhayat et al. conducted a study on 23 children with intractable epilepsy, giving them 1.5 mg of melatonin 30 min before bedtime [73]. Over the 3-month treatment period, 87% had decreased frequency and/or severity of their seizures. However, in 13% of subjects, seizures worsened and melatonin was discontinued. Side effects reported in this study included headache, rash, and abdominal pain, but none of the side effects were significant enough for subjects to stop the melatonin. In Coppola et al.’s study, 11 of the subjects did not have seizures at study onset [26]. In two of them, seizures started after initiating melatonin treatment. Discontinuing melatonin resulted in the seizures stopping. Seven of the subjects had uncontrolled seizures at the start of the study. One of these became seizure-free, two had some improvement, two had worsening of seizures, and two were unchanged. Studies by Goldberg-Stern et al. and Uberos et al. showed general improvement in seizures while on melatonin. Goldberg-Stern et al. conducted a double-blind, randomized, placebo-controlled, crossover pilot trial including ten subjects [79]. The melatonin dose during the melatonin treatment period was 10 mg at bedtime. On placebo, the mean number of diurnal seizures was 7.75. On melatonin, the mean number of diurnal seizures was 4.6. Mean number of partial seizures was found to decrease from 8.31 on placebo down to 5.26 on melatonin. The researchers did not find significant changes in the frequency of generalized or nocturnal seizures, maximal number of seizures per day, or seizure duration. Their subjects did not experience worsening of their seizures and did not report any significant side effects. Uberos et al. showed decreased frequency of seizures [72]. Some studies have found no change in seizures while on melatonin. In a study of melatonin use in 107 children with autism, Andersen et al. did not find new onset seizure, nor did those children with a history of seizures have any increase in seizures [30]. Wright’s study of 22 children with ASD did not show seizures [38]. Gringras et al. found that the 16 children with a history of epilepsy who were enrolled in their study did not have worsening of seizure control or the emergence of a new type of seizure [27].
Fragile X Syndrome
Sleep problems are reported to occur in up to 77% of children with fragile X syndrome [57]. Compared to controls, boys with fragile X syndrome have greater variability in total sleep time, mean sleep onset latency, and sleep termination times [80]. Boys with fragile X syndrome have more frequent night wakings, and the night wakings are much longer than they are in control groups [80]. Their issues do not appear to be due to insufficient melatonin production. Instead, boys with fragile X syndrome have been found to have greater nocturnal melatonin production compared to controls [80]. Despite this, they have still been observed to have improved sleep when given supplemental melatonin. In a 4-week randomized, double-blind, placebo-controlled, crossover trial of 3 mg of melatonin that included children with ASD and fragile X syndrome, participants were found to have an increase in mean sleep duration, decrease in mean sleep onset latency, and earlier sleep onset time compared to placebo [57].
Concussion and Traumatic Brain Injury
Depending on the location of a person’s brain injury, a person can have resulting insomnia or hypersomnia [81]. Insomnia occurs in an estimated 40–65% of patients with minor traumatic brain injury (TBI) [82]. Polysomnography and actigraphy data in adolescents 3 years after minor head injury showed decreased sleep despite no other apparent clinical sequelae from the injury [83]. Multiple factors contribute to the insomnia including pain, emotional trauma, and damage to neural structures that regulate sleep/wake rhythms [81]. TBI patients have been found to have lower levels of melatonin production [84]. An evaluation of tentorial length and angle in TBI patients with sleep/wake disturbances showed that they had longer and flatter orientations of the tentorium compared to those without sleep problems [85]. The result is that the edge of the tentorium would be closer to the pineal gland and thus increase the likelihood that upon traumatic impact to the brain, the pineal gland could be injured [85].
In a study by Ayalon et al., 42 patients with insomnia complaints and a history of TBI underwent sleep evaluation [82]. The cause of their insomnia was diagnosed as a circadian rhythm disorder in 36% of subjects. Of them, eight had a delayed sleep phase pattern, and seven had an irregular sleep/wake pattern.
A randomized, double-blind, controlled, crossover trial comparing 5 mg of melatonin and 25 mg of amitriptyline to improve sleep in TBI patients showed no significant difference between the two when it came to sleep latency and total sleep time [86]. Once effect size was accounted for, patients on melatonin were found to have improved daytime alertness.
Other properties of melatonin, such as its anxiolytic, sedative, and anticonvulsant effects, can be useful after TBI since these patients can be agitated and have convulsions after head trauma [7]. While there are promising reasons to consider melatonin for treating sleep problems in TBI, there is an overall lack of evidence for this purpose and thus need for further studies [87].
Future Directions
While studies have shown that melatonin improves the sleep of children with neurodevelopmental disorders, further research examining appropriate dosing for age and or weight is essential. Controlled studies could also examine if there is optimal dosing specific to certain neurodevelopmental disorders. Most importantly, considering that melatonin is a neurohormone and that most doses available over the counter are supraphysiologic, further research into the effects of long-term use through childhood are needed. Research to answer how young is too young to start melatonin is necessary. Lastly, as more extended release formulations of melatonin become available, further controlled studies can clarify whether they confer any additional benefit or harm compared to instant release melatonin.
Conclusion
Melatonin seems to have positive effects on sleep in children with a variety of neurodevelopmental disorders. It typically shortens the length of time it takes for a child to fall asleep and increases total sleep time at night. Effect on night wakings is variable. While short-term use has been observed to have minimal side effects, long-term effects of initiating exogenous melatonin use in childhood are unknown.
References
Lerner AB, Case JD, Takahashi Y. Isolation of melatonin and 5-methoxyindole-3-acetic acid from bovine pineal glands. J Biol Chem. 1960;235:1992–7.
Chen YC, Tain YL, Sheen JM, Huang LT. Melatonin utility in neonates and children. J Formos Med Assoc. 2012;111(2):57–66.
Leu RM, Beyderman L, Botzolakis EJ, Surdyka K, Wang L, Malow BA. Relation of melatonin to sleep architecture in children with autism. J Autism Dev Disord. 2011;41(4):427–33.
Sajith SG, Clarke D. Melatonin and sleep disorders associated with intellectual disability: a clinical review. J Intellect Disabil Res. 2007;51(Pt 1):2–13.
Pandi-Perumal SR, Smits M, Spence W, Srinivasan V, Cardinali DP, Lowe AD, et al. Dim light melatonin onset (DLMO): a tool for the analysis of circadian phase in human sleep and chronobiological disorders. Prog Neuro-Psychopharmacol Biol Psychiatry. 2007;31(1):1–11.
Doyen C, Mighiu D, Kaye K, Colineaux C, Beaumanoir C, Mouraeff Y, et al. Melatonin in children with autistic spectrum disorders: recent and practical data. Eur Child Adolesc Psychiatry. 2011;20(5):231–9.
Maldonado MD, Murillo-Cabezas F, Terron MP, Flores LJ, Tan DX, Manchester LC, et al. The potential of melatonin in reducing morbidity-mortality after craniocerebral trauma. J Pineal Res. 2007;42(1):1–11.
DeMuro RL, Nafziger AN, Blask DE, Menhinick AM, Bertino JS Jr. The absolute bioavailability of oral melatonin. J Clin Pharmacol. 2000;40(7):781–4.
Dubocovich ML, Yun K, Al-Ghoul WM, Benloucif S, Masana MI. Selective MT2 melatonin receptor antagonists block melatonin-mediated phase advances of circadian rhythms. FASEB J. 1998;12(12):1211–20.
Palm L, Blennow G, Wetterberg L. Correction of non-24-hour sleep/wake cycle by melatonin in a blind retarded boy. Ann Neurol. 1991;29(3):336–9.
McArthur AJ, Budden SS. Sleep dysfunction in Rett syndrome: a trial of exogenous melatonin treatment. Dev Med Child Neurol. 1998;40(3):186–92.
Zhdanova IV, Wurtman RJ, Morabito C, Piotrovska VR, Lynch HJ. Effects of low oral doses of melatonin, given 2–4 hours before habitual bedtime, on sleep in normal young humans. Sleep. 1996;19(5):423–31.
Hollway JA, Aman MG. Pharmacological treatment of sleep disturbance in developmental disabilities: a review of the literature. Res Dev Disabil. 2011;32(3):939–62.
Aldhous M, Franey C, Wright J, Arendt J. Plasma concentrations of melatonin in man following oral absorption of different preparations. Br J Clin Pharmacol. 1985;19(4):517–21.
Braam W, van Geijlswijk I, Keijzer H, Smits MG, Didden R, Curfs LM. Loss of response to melatonin treatment is associated with slow melatonin metabolism. J Intellect Disabil Res. 2010;54(6):547–55.
Cavallo A, Ritschel WA. Pharmacokinetics of melatonin in human sexual maturation. J Clin Endocrinol Metab. 1996;81(5):1882–6.
Grigg-Damberger M, Ralls F. Treatment strategies for complex behavioral insomnia in children with neurodevelopmental disorders. Curr Opin Pulm Med. 2013;19(6):616–25.
Erland LA, Saxena PK. Melatonin natural health products and supplements: presence of serotonin and significant variability of melatonin content. J Clin Sleep Med. 2017;13(2):275–81.
Owens JA, Moturi S. Pharmacologic treatment of pediatric insomnia. Child Adolesc Psychiatr Clin N Am. 2009;18(4):1001–16.
Altun A, Ugur-Altun B. Melatonin: therapeutic and clinical utilization. Int J Clin Pract. 2007;61(5):835–45.
Damiani JM, Sweet BV, Sohoni P. Melatonin: an option for managing sleep disorders in children with autism spectrum disorder. Am J Health Syst Pharm. 2014;71(2):95–101.
Lewy AJ, Ahmed S, Jackson JM, Sack RL. Melatonin shifts human circadian rhythms according to a phase-response curve. Chronobiol Int. 1992;9(5):380–92.
Lewy AJ, Emens JS, Sack RL, Hasler BP, Bernert RA. Low, but not high, doses of melatonin entrained a free-running blind person with a long circadian period. Chronobiol Int. 2002;19(3):649–58.
Jan JE, O’Donnell ME. Use of melatonin in the treatment of paediatric sleep disorders. J Pineal Res. 1996;21(4):193–9.
Ayyash HF, Preece P, Morton R, Cortese S. Melatonin for sleep disturbance in children with neurodevelopmental disorders: prospective observational naturalistic study. Expert Rev Neurother. 2015;15(6):711–7.
Coppola G, Iervolino G, Mastrosimone M, La Torre G, Ruiu F, Pascotto A. Melatonin in wake-sleep disorders in children, adolescents and young adults with mental retardation with or without epilepsy: a double-blind, cross-over, placebo-controlled trial. Brain and Development. 2004;26(6):373–6.
Gringras P, Gamble C, Jones AP, Wiggs L, Williamson PR, Sutcliffe A, et al. Melatonin for sleep problems in children with neurodevelopmental disorders: randomised double masked placebo controlled trial. BMJ. 2012;345:e6664.
Malow B, Adkins KW, McGrew SG, Wang L, Goldman SE, Fawkes D, et al. Melatonin for sleep in children with autism: a controlled trial examining dose, tolerability, and outcomes. J Autism Dev Disord. 2012;42(8):1729–37; author reply 38.
Carr R, Wasdell MB, Hamilton D, Weiss MD, Freeman RD, Tai J, et al. Long-term effectiveness outcome of melatonin therapy in children with treatment-resistant circadian rhythm sleep disorders. J Pineal Res. 2007;43(4):351–9.
Andersen IM, Kaczmarska J, McGrew SG, Malow BA. Melatonin for insomnia in children with autism spectrum disorders. J Child Neurol. 2008;23(5):482–5.
Braam W, Keijzer H, Struijker Boudier H, Didden R, Smits M, Curfs L. CYP1A2 polymorphisms in slow melatonin metabolisers: a possible relationship with autism spectrum disorder? J Intellect Disabil Res. 2013;57(11):993–1000.
Johnson KP, Malow BA. Assessment and pharmacologic treatment of sleep disturbance in autism. Child Adolesc Psychiatr Clin N Am. 2008;17(4):773–85, viii.
Hoebert M, van der Heijden KB, van Geijlswijk IM, Smits MG. Long-term follow-up of melatonin treatment in children with ADHD and chronic sleep onset insomnia. J Pineal Res. 2009;47(1):1–7.
O’Callaghan FJ, Clarke AA, Hancock E, Hunt A, Osborne JP. Use of melatonin to treat sleep disorders in tuberous sclerosis. Dev Med Child Neurol. 1999;41(2):123–6.
Sugden D. Psychopharmacological effects of melatonin in mouse and rat. J Pharmacol Exp Ther. 1983;227(3):587–91.
Seabra ML, Bignotto M, Pinto LR Jr, Tufik S. Randomized, double-blind clinical trial, controlled with placebo, of the toxicology of chronic melatonin treatment. J Pineal Res. 2000;29(4):193–200.
Miyamoto A, Oki J, Takahashi S, Okuno A. Serum melatonin kinetics and long-term melatonin treatment for sleep disorders in Rett syndrome. Brain and Development. 1999;21(1):59–62.
Wright B, Sims D, Smart S, Alwazeer A, Alderson-Day B, Allgar V, et al. Melatonin versus placebo in children with autism spectrum conditions and severe sleep problems not amenable to behaviour management strategies: a randomised controlled crossover trial. J Autism Dev Disord. 2011;41(2):175–84.
Guenole F, Godbout R, Nicolas A, Franco P, Claustrat B, Baleyte JM. Melatonin for disordered sleep in individuals with autism spectrum disorders: systematic review and discussion. Sleep Med Rev. 2011;15(6):379–87.
Pechanova O, Paulis L, Simko F. Peripheral and central effects of melatonin on blood pressure regulation. Int J Mol Sci. 2014;15(10):17920–37.
Marseglia L, D'Angelo G, Manti S, Salpietro C, Arrigo T, Barberi I, et al. Melatonin and atopy: role in atopic dermatitis and asthma. Int J Mol Sci. 2014;15(8):13482–93.
Campos FL, da Silva-Junior FP, de Bruin VM, de Bruin PF. Melatonin improves sleep in asthma: a randomized, double-blind, placebo-controlled study. Am J Respir Crit Care Med. 2004;170(9):947–51.
Waldhauser F, Steger H. Changes in melatonin secretion with age and pubescence. J Neural Transm Suppl. 1986;21:183–97.
Crowley SJ, Acebo C, Carskadon MA. Human puberty: salivary melatonin profiles in constant conditions. Dev Psychobiol. 2012;54(4):468–73.
van Geijlswijk IM, Mol RH, Egberts TC, Smits MG. Evaluation of sleep, puberty and mental health in children with long-term melatonin treatment for chronic idiopathic childhood sleep onset insomnia. Psychopharmacology. 2011;216(1):111–20.
Richdale AL. Sleep problems in autism: prevalence, cause, and intervention. Dev Med Child Neurol. 1999;41(1):60–6.
Chamberlain RS, Herman BH. A novel biochemical model linking dysfunctions in brain melatonin, proopiomelanocortin peptides, and serotonin in autism. Biol Psychiatry. 1990;28(9):773–93.
Brzezinski A, Vangel MG, Wurtman RJ, Norrie G, Zhdanova I, Ben-Shushan A, et al. Effects of exogenous melatonin on sleep: a meta-analysis. Sleep Med Rev. 2005;9(1):41–50.
Kulman G, Lissoni P, Rovelli F, Roselli MG, Brivio F, Sequeri P. Evidence of pineal endocrine hypofunction in autistic children. Neuro Endocrinol Lett. 2000;21(1):31–4.
Melke J, Goubran Botros H, Chaste P, Betancur C, Nygren G, Anckarsater H, et al. Abnormal melatonin synthesis in autism spectrum disorders. Mol Psychiatry. 2008;13(1):90–8.
Nir I, Meir D, Zilber N, Knobler H, Hadjez J, Lerner Y. Brief report: circadian melatonin, thyroid-stimulating hormone, prolactin, and cortisol levels in serum of young adults with autism. J Autism Dev Disord. 1995;25(6):641–54.
Tordjman S, Anderson GM, Bellissant E, Botbol M, Charbuy H, Camus F, et al. Day and nighttime excretion of 6-sulphatoxymelatonin in adolescents and young adults with autistic disorder. Psychoneuroendocrinology. 2012;37(12):1990–7.
Goldman SE, Adkins KW, Calcutt MW, Carter MD, Goodpaster RL, Wang L, et al. Melatonin in children with autism spectrum disorders: endogenous and pharmacokinetic profiles in relation to sleep. J Autism Dev Disord. 2014;44(10):2525–35.
Veatch OJ, Pendergast JS, Allen MJ, Leu RM, Johnson CH, Elsea SH, et al. Genetic variation in melatonin pathway enzymes in children with autism spectrum disorder and comorbid sleep onset delay. J Autism Dev Disord. 2015;45(1):100–10.
Rossignol DA, Frye RE. Melatonin in autism spectrum disorders: a systematic review and meta-analysis. Dev Med Child Neurol. 2011;53(9):783–92.
Garstang J, Wallis M. Randomized controlled trial of melatonin for children with autistic spectrum disorders and sleep problems. Child Care Health Dev. 2006;32(5):585–9.
Wirojanan J, Jacquemont S, Diaz R, Bacalman S, Anders TF, Hagerman RJ, et al. The efficacy of melatonin for sleep problems in children with autism, fragile X syndrome, or autism and fragile X syndrome. J Clin Sleep Med. 2009;5(2):145–50.
Cortesi F, Giannotti F, Sebastiani T, Panunzi S, Valente D. Controlled-release melatonin, singly and combined with cognitive behavioural therapy, for persistent insomnia in children with autism spectrum disorders: a randomized placebo-controlled trial. J Sleep Res. 2012;21(6):700–9.
Weiss MD, Salpekar J. Sleep problems in the child with attention-deficit hyperactivity disorder: defining aetiology and appropriate treatments. CNS Drugs. 2010;24(10):811–28.
Barrett JR, Tracy DK, Giaroli G. To sleep or not to sleep: a systematic review of the literature of pharmacological treatments of insomnia in children and adolescents with attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol. 2013;23(10):640–7.
Van der Heijden KB, Smits MG, Van Someren EJ, Ridderinkhof KR, Gunning WB. Effect of melatonin on sleep, behavior, and cognition in ADHD and chronic sleep-onset insomnia. J Am Acad Child Adolesc Psychiatry. 2007;46(2):233–41.
Weiss MD, Wasdell MB, Bomben MM, Rea KJ, Freeman RD. Sleep hygiene and melatonin treatment for children and adolescents with ADHD and initial insomnia. J Am Acad Child Adolesc Psychiatry. 2006;45(5):512–9.
Bassell JL, Phan H, Leu R, Kronk R, Visootsak J. Sleep profiles in children with Down syndrome. Am J Med Genet A. 2015;167(8):1830–5.
Reiter RJ, Barlow-Walden L, Poeggeler B, Heiden SM, Clayton RJ. Twenty-four hour urinary excretion of 6-hydroxymelatonin sulfate in Down syndrome subjects. J Pineal Res. 1996;20(1):45–50.
Corrales A, Martinez P, Garcia S, Vidal V, Garcia E, Florez J, et al. Long-term oral administration of melatonin improves spatial learning and memory and protects against cholinergic degeneration in middle-aged Ts65Dn mice, a model of Down syndrome. J Pineal Res. 2013;54(3):346–58.
Braam W, Didden R, Smits MG, Curfs LM. Melatonin for chronic insomnia in Angelman syndrome: a randomized placebo-controlled trial. J Child Neurol. 2008;23(6):649–54.
Takaesu Y, Komada Y, Inoue Y. Melatonin profile and its relation to circadian rhythm sleep disorders in Angelman syndrome patients. Sleep Med. 2012;13(9):1164–70.
Zhdanova IV, Wurtman RJ, Wagstaff J. Effects of a low dose of melatonin on sleep in children with Angelman syndrome. J Pediatr Endocrinol Metab. 1999;12(1):57–67.
Wu Y, Bolduc FV, Bell K, Tully T, Fang Y, Sehgal A, et al. A Drosophila model for Angelman syndrome. Proc Natl Acad Sci U S A. 2008;105(34):12399–404.
Hancock E, O'Callaghan F, English J, Osborne JP. Melatonin excretion in normal children and in tuberous sclerosis complex with sleep disorder responsive to melatonin. J Child Neurol. 2005;20(1):21–5.
Hancock E, O'Callaghan F, Osborne JP. Effect of melatonin dosage on sleep disorder in tuberous sclerosis complex. J Child Neurol. 2005;20(1):78–80.
Uberos J, Augustin-Morales MC, Molina Carballo A, Florido J, Narbona E, Munoz-Hoyos A. Normalization of the sleep-wake pattern and melatonin and 6-sulphatoxy-melatonin levels after a therapeutic trial with melatonin in children with severe epilepsy. J Pineal Res. 2011;50(2):192–6.
Elkhayat HA, Hassanein SM, Tomoum HY, Abd-Elhamid IA, Asaad T, Elwakkad AS. Melatonin and sleep-related problems in children with intractable epilepsy. Pediatr Neurol. 2010;42(4):249–54.
Sheldon SH. Pro-convulsant effects of oral melatonin in neurologically disabled children. Lancet. 1998;351(9111):1254.
Philo R, Reiter RJ. Characterization of pinealectomy induced convulsions in the Mongolian gerbil (Meriones unguiculatus). Epilepsia. 1978;19(5):485–92.
Rudeen PK, Philo RC, Symmes SK. Antiepileptic effects of melatonin in the pinealectomized Mongolian gerbil. Epilepsia. 1980;21(2):149–54.
Fariello RG, Bubenik GA, Brown GM, Grota LJ. Epileptogenic action of intraventricularly injected antimelatonin antibody. Neurology. 1977;27(6):567–70.
Molina-Carballo A, Munoz-Hoyos A, Sanchez-Forte M, Uberos-Fernandez J, Moreno-Madrid F, Acuna-Castroviejo D. Melatonin increases following convulsive seizures may be related to its anticonvulsant properties at physiological concentrations. Neuropediatrics. 2007;38(3):122–5.
Goldberg-Stern H, Oren H, Peled N, Garty BZ. Effect of melatonin on seizure frequency in intractable epilepsy: a pilot study. J Child Neurol. 2012;27(12):1524–8.
Gould EL, Loesch DZ, Martin MJ, Hagerman RJ, Armstrong SM, Huggins RM. Melatonin profiles and sleep characteristics in boys with fragile X syndrome: a preliminary study. Am J Med Genet. 2000;95(4):307–15.
Galland BC, Elder DE, Taylor BJ. Interventions with a sleep outcome for children with cerebral palsy or a post-traumatic brain injury: a systematic review. Sleep Med Rev. 2012;16(6):561–73.
Ayalon L, Borodkin K, Dishon L, Kanety H, Dagan Y. Circadian rhythm sleep disorders following mild traumatic brain injury. Neurology. 2007;68(14):1136–40.
Kaufman Y, Tzischinsky O, Epstein R, Etzioni A, Lavie P, Pillar G. Long-term sleep disturbances in adolescents after minor head injury. Pediatr Neurol. 2001;24(2):129–34.
Ponsford JL, Ziino C, Parcell DL, Shekleton JA, Roper M, Redman JR, et al. Fatigue and sleep disturbance following traumatic brain injury – their nature, causes, and potential treatments. J Head Trauma Rehabil. 2012;27(3):224–33.
Yaeger K, Alhilali L, Fakhran S. Evaluation of tentorial length and angle in sleep-wake disturbances after mild traumatic brain injury. AJR Am J Roentgenol. 2013;202(3):614–8.
Kemp S, Biswas R, Neumann V, Coughlan A. The value of melatonin for sleep disorders occurring post-head injury: a pilot RCT. Brain Inj. 2004;18(9):911–9.
Keegan LJ, Reed-Berendt R, Neilly E, Morrall MC, Murdoch-Eaton D. Effectiveness of melatonin for sleep impairment post paediatric acquired brain injury: evidence from a systematic review. Dev Neurorehabil. 2014;17(5):355–62.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Leu, R.M. (2019). Melatonin. In: Accardo, J. (eds) Sleep in Children with Neurodevelopmental Disabilities. Springer, Cham. https://doi.org/10.1007/978-3-319-98414-8_31
Download citation
DOI: https://doi.org/10.1007/978-3-319-98414-8_31
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-98412-4
Online ISBN: 978-3-319-98414-8
eBook Packages: MedicineMedicine (R0)