
Abstract
Team-based primary care (TBPC) has diffused rapidly in concert with other reform initiatives. However, little is known about the contextual factors that best position practices to leverage team-based strategies for improved healthcare delivery. Sixty-two empirical articles were analysed in a scoping review to explore key factors in the domains of environment, task and technology that influence the success of establishing and maintaining TBPC practices. Key findings address the importance of internal performance management structures and external payment mechanisms that reinforce TBPC. Incremental task delegation, combined with consistent communication and integrated documentation practices, is critical for shared role understanding and sustained TBPC commitment. Finally, electronic health records can provide a collaboration and communication platform to enhance team functioning. This review provides insights to providers and policymakers regarding enabling contextual factors for successful TBPC implementation, and identifies promising areas for future research – specifically technology use and performance measurement as they relate to teams.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others

Keywords
Introduction
Comprehensive primary care is the cornerstone of a low cost, accessible and high-quality health system, and robust primary care infrastructure is a key to tackling unsustainable growth in health spending and significant gaps in patient care quality and outcomes (Donaldson et al. 1996; Starfield et al. 2005). Strengthened inter-professional teamwork amongst primary care physicians and practice staff —including nurses, medical assistants (MAs) and others—has emerged as a promising strategy to promote more effective care delivery, particularly as concurrent delivery reforms such as patient-centred medical home (PCMH) and pay-for-performance initiatives seek to expand the scope of primary care services. Team-based primary care (TBPC) can alleviate mounting time pressures on primary care physicians through improved delegation and empowerment of other staff members to work to the fullest extent of their training (Friedman et al. 2014; Mitchell et al. 2012; Saba et al. 2012; Shipman and Sinsky 2013). Furthermore, there is a reasonable body of empirical evidence supporting the link between the adoption of TBPC and improved efficiency (Page 2006; Thomas 2014), quality and comprehensiveness of services (Cutrona et al. 2010; McAllister et al. 2013; Mohr et al. 2013; Roblin et al. 2011), and physician, staff and patient satisfaction (Altschuler et al. 2012; Helfrich et al. 2014; Willard-Grace et al. 2014). Indeed, for many practices, adopting a team-based approach to care may be the critical element needed to realize the intended benefits of broader care reform efforts such as PCMH transformation (McAllister et al. 2013).
However, these relationships are not iron-clad. Estimates of the positive effects of TBPC on outcomes have been found to be unreliable, with calls for research to improve understanding of the mechanisms and facilitating factors which help practices achieve the intended benefits (Jesmin et al. 2012). Other scholars have echoed this call, trying to discern a more nuanced relationship of teamwork as a moderator, a ‘complex and adaptive’ process that needs to be deployed in the right situations and with the appropriate resources and support to implement these change practices effectively (Belanger and Rodríguez 2008; Bosch et al. 2008; Hann et al. 2007; Wise et al. 2011). There is a dearth of synthesized knowledge about the consideration of implementation factors and the context(s) in which TBPC is most likely to be successful. Thus, focusing on the domains of environment, task and technology —an approach rooted in prior theoretical and empirical work—I explore enabling contextual factors that support the use of TBPC to strengthen primary care delivery.
Approach
This review was informed and structured by adapting the holistic conceptual model developed by the Integrated Team Effectiveness Model (ITEM) (Lemieux-Charles and McGuire 2006). The goal of this review is to determine how a team approach best fits into the current context and dynamic nature of health systems and primary care delivery. Therefore, I explicitly focus on one nation’s healthcare system—the USA—and home in on three domains within ITEM that capture the most salient changes likely to be impacting a practice’s ability to successfully implement TBPC practices in that system:
-
1.
Environment Internal (organizational-level) as well as external (market, policy) characteristics or initiatives that may facilitate or impede TBPC changes;
-
2.
Task Specific changes in the scope and nature of health needs and primary care services that may shape the use of TBPC; and
-
3.
Technology Currently available technologies that impact practices’ ability to effectively implement improved care processes using TBPC.
Whilst these domains do not address the full scope of the ITEM, the implications of research findings in these areas are most likely to be actionable in a policy and practice setting. In addition, though the US-based perspective used in this analysis may limit generalizability, many of the findings summarized below—particularly related to internal organizational culture and teamwork-facilitating structures—may still translate to other nations with different healthcare organization, delivery and financing mechanisms.
Methods
This scoping review of published ‘primary care teams’ research in the US healthcare setting focuses on how findings in the domains of environment, task and technology better inform our understanding of the enabling contextual factors that promote TBPC. A scoping review was purposely selected because of the applied and dynamic nature of the motivating research question—the need to map available literature and research findings/evidence in a burgeoning area for policymakers and practitioners (Arksey and O’Malley 2005; Kastner et al. 2012).
Separate searches were conducted in Scopus and PubMed, dating from 2005 to 2015, limited to a more recent time period to capture only the more current environment and contextual factors most salient to providers and policymakers today. I used broad search terms, including ‘primary care team’ or ‘primary care’ AND (‘teamwork’ OR ‘team-based’). Articles were restricted to English only.
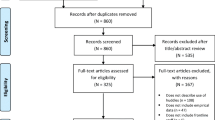
Figure 5.1 provides a flow diagram for the selection of included studies. Articles were searched and downloaded to an Excel database. I then removed duplicates and reviewed article titles for inclusion, followed by abstract review. Letters, editorials and position statement articles were excluded, as was research that didn’t meet the inclusion criteria outlined in Table 5.1. A total of sixty-two articles were included for the full review; these articles were ‘charted’ and summarized across the three domains of interest (Arksey and O’Malley 2005).

PRISM diagram
Results
Environment
Applying an ‘environmental’ lens helps to better understand what organizational and market factors make a setting conducive for deploying a TBPC approach, and where the different levers exist to reshape pressures that may facilitate or impede a ‘teams’ transition.
Internal Organizational Structures
Research on a ‘teams’-focused organizational culture frequently focuses on strong leadership and effective change management as staff deal with the uncertainties and vulnerability of significant role change and altered interpersonal dynamics (Goldman et al. 2010; Hilts et al. 2013). More concretely, practice characteristics that are associated with these enabling organizational strengths include first an organizational philosophy focused on TBPC that is explicitly tied to near-term practice goals and intended changes promoted under PCMH and other delivery reforms (Allan et al. 2014). Physicians’ consistent participation in frontline team huddles for daily care planning also sends an important message of physician buy-in and sets an open, collaborative tone for team functioning (Rodriguez et al. 2015a, b). Finally, identifying the personal characteristics in staff that facilitate strong interpersonal dynamics and incorporating them into hiring processes may be an increasingly important organizational strategy to foster high-functioning work relationships amid these changes (Bunniss and Kelly 2008).
Organizations trying to foster teamwork also require appropriate structures and aligned incentives that encourage the effective use of team-based care (TBC) approaches (Hung et al. 2006; Xyrichis and Lowton 2008). Understanding how effectively teams are working together, how the use of teams affects patient outcomes and how to strengthen team functioning all require changes in the traditional ways that practices measure and report performance (Hays 2007; O’Toole et al. 2011). In the context of TBPC, studies have revealed a significant lag between changes in how services are being delivered under new team-based care delivery models and how practice performance is assessed. In an interventional study with ‘Family Health Teams’ in Ontario , researchers found that existing performance indicators fail to reflect the role and contribution of different team members (Johnston et al. 2011). A qualitative evaluation of sixteen primary care practices in the nationalized healthcare system set up to treat US military veterans (i.e. the US Veterans Health Administration ) revealed that performance assessment failed to engage or activate non-physician team members and did little to further the stated organizational goals of emphasizing a team-based care approach (Hysong et al. 2014).
To facilitate enhanced performance initiatives that acknowledge and reinforce team-based care, all team members need access to performance reporting data, both to analyse personal performance and engender a stronger sense of shared responsibility for office functioning and patient care. Performance data should be actionable, with some level of role-specificity (particularly in process measures) to define and maintain individual roles and responsibilities. Having a designated data facilitator driving performance improvement is critical (Watts et al. 2014). Hysong et al. (2014) recommend that—when empowered to do so—a designated nurse or other team member is often better positioned to monitor and manage team processes and outcomes compared to a physician-managed model.
External Policy Environment
Team-based care approaches are typically seen as a facilitator and a mechanism to achieve success under broader delivery reform programmes in the USA, such as accountable care organizations, PCMHs and pay-for-value initiatives (Friedberg et al. 2013; Grace et al. 2014; Grover and Niecko-Najjum 2013). Key elements of a team transformation —(re)negotiating roles, establishing a shared sense of purpose that is patient-centric, fostering open communication etc.—are critical for meeting enhanced practice responsibilities under a PCMH model, particularly in areas such as improved care management and patient engagement/activation (Friedberg et al. 2013; Sanchez and Adorno 2013; True et al. 2014).
Though empirical work is limited, a number of studies have drawn attention to the fact that the financial and regulatory environment of healthcare can seriously impede the implementation of TBC approaches (Finlayson and Raymont 2012). The extent of organizational change possible, especially with respect to enhanced care roles for non-physician staff , is often limited by legal restrictions or ambiguity around role scope. The role of medical assistants in particular is an open question of policy and practical significance as their role continues to expand in the absence of clear regulations, guidelines or best practices (Freund et al. 2015; Ladden et al. 2013).
Existing payment methods in the USA also limit the expansion of TBPC approaches, given the physician-centric fee-for-service billing practices and the task-based nature of reimbursement (McInnes et al. 2015; Strumpf et al. 2012). In a study of salient organizational factors affecting primary care practice in New Zealand, researchers found that degree of inter-office collaboration is strongly influenced by the most prevalent funding mechanism , and that capitation or bulk-funding more strongly promoted the use of teamwork (Pullon et al. 2009). Similar findings from an evaluation of a global payment demonstration in the state of Massachusetts indicated that a transition to use of teams was a critically important component of practices’ response to these types of payment reforms (Mechanic et al. 2011).
Task
Primary care providers are faced with an unprecedented workload in today’s healthcare environment, coupled with a context of greatly increased documentation and reporting requirements. Whilst shifting to a team-based care approach seems like a natural and often suggested response to these pressures, the ways to best staff and structure these new care teams are less clear. Finlayson and Raymont (2012) emphasize that the ‘type, nature and strength of teamwork’ is critically shaped by the nature of work itself. Thus, this section explores types of care and service provision that best accommodate a teamwork structure, synthesizing specific findings about how and when teams can be used successfully to accelerate and/or extend care.
Staffing
The development of healthcare teams is often hampered by traditional role concepts (Chesluk and Holmboe 2010). However, increased requirements and resource demands under PCMH and other delivery reform models—particularly around patient-centric care management and coordination—have continued to erode traditional care models and accelerated the development and expansion of new supporting staff roles (Morrissey 2013). Staff in these roles (e.g. care managers, health coaches, navigators etc.) are often best positioned to improve patient activation, connect patients with social services and have the time necessary to manage service utilization and medications; empowered ancillary staff have a particularly well-documented role in the literature in the areas of preventive care and chronic disease management (Altschuler et al. 2012; Edwards et al. 2015; Ferrer et al. 2009; Graffy et al. 2010; Hudson et al. 2007; Margolius et al. 2012). Indeed, a number of recent studies have been able to detect improved patient outcomes as a result of introducing these new care roles (Anand et al. 2010; Chan et al. 2010; Collinsworth et al. 2014). Physicians are busy and have relatively less experience and training in these areas; incorporating new staff to carry out these tasks thus may be viewed as an extension of services rather than an acceleration of existing physician care, and fulfils patient needs complementary to their own role.
Role understanding is a key facilitator in the process of integrating these new staff into the primary care team. Indeed, it is integration rather than collaboration that signifies true embodiment of TBPC principles (Boon et al. 2009). The newness of these care roles , and ambiguity in their defined responsibility and scope, can pose a challenge to physicians and other staff as they incorporate this new team member. Qualitative studies on the role of health coaches emphasize positioning the new staff member as a liaison or as part of a ‘relational triad’ between the patient and physician. This arrangement cements the coach’s role as an advocate and extension of the patients’ best interests to improve patient care, and helps physicians and other team members better understand and appreciate this care role (Margolius et al. 2012; Ngo et al. 2010; Wholey et al. 2013). Clear delineation of scope of practice is also critical, as is an explicit understanding of interdependencies. The rest of the team—particularly the physician—needs to understand the functions being performed by the ancillary staff person and how it fits into achieving the broader vision of care that practice aims to provide (Donnelly et al. 2013; Wholey et al. 2013). Finally, securing adequate face-time between ‘traditional’ and new ancillary team members is critical for fostering an inclusive sense of teamness. Co-location facilitated more acceptance of and reliance on these new care roles, as did including ancillary staff in regular huddles and team meetings (Donnelly et al. 2013; O’Malley et al. 2014).
Structuring
Implementing TBPC requires a difficult navigation of trust, preferences and changed patterns of interaction as roles and responsibilities change, as do organization-level workflows and infrastructure (Mitchell et al. 2012). As new roles take shape, a natural tension and trade-off emerges between role clarity and flexibility. Some argue that a more mechanistic, highly structured team dynamic creates a consistency that builds trust and a feeling of competence (Drach‐Zahavy and Freund 2007; Elder et al. 2014). However, a certain degree of flexibility is critical; all team members need to share feelings of responsibility for total patient care that may require completing tasks or services outside his/her defined role description. Clear role guidelines tied to an explicit care mission statement, with guidance on staff cross-coverage expectations, reduce ambiguity to prevent feelings of territorialism or inconsistent TBPC implementation (Grace et al. 2014; Rodriguez et al. 2014).
Relatively discrete clinical tasks (e.g. administering screenings, vaccinations) or administrative tasks (referral tracking, well-visit documentation etc.) can be delegated, as can more nuanced but critical care roles such as patient engagement and education , connecting patients with social services and medication management. Promising strategies to help shape these new enhanced care roles amongst staff include the use of explicit protocols or care templates for routine services and screening (Cross et al. 2015; Goldman et al. 2010; Ladden et al. 2013; O’Malley et al. 2014). Medical assistants (i.e. individuals certified to complete various administrative and low-risk clinical tasks) or ancillary staff trained in case management can often be brought in and trained in panel management and the logistics of care coordination oversight ; guidelines and toolkits have been developed to help spread effective role guidelines and best practices for this emerging role (Ladden et al. 2013; Savarimuthu et al. 2013). Making these changes incrementally, with role support through inclusive team huddles and performance feedback, helps build and reinforce these new relationships (O’Malley et al. 2014; Rodriguez et al. 2015a, b).
Technology
Practitioners and researchers have long recognized that the design and functionality of clinical electronic health records (EHRs) shape not just how providers work but also how they can work together (Anand et al. 2010; Bates and Bitton 2010; Howard et al 2012). However, providers lack knowledge on how to use IT to support the holistic changes they are making in pursuit of patient-centric, team-based case (Roper 2014). This is largely due to the underdeveloped state of research exploring the interdependence and synergies of pursuing greater IT implementation in parallel with the use of a team-based approach. There is a dearth of understanding about how care teams learn to work collaboratively within the EHR system, what features facilitate or impede a team approach and how these systems can be designed with new functionality that not only accommodates but also enhances use of a care team.
As primary care teams grow to incorporate new team roles—including care managers, nutritionists, health coaches, etc.—documentation practices need to evolve to support and integrate these new services. Tasks performed and information collected by these ancillary clinical team members is often not incorporated into the central patient record; doctors and nurses often don’t see the availability of this information and don’t know to act, reiterate or follow-up on this critical resource (Cross et al. 2015; Donnelly et al. 2013; Kim et al. 2013; O’Malley et al. 2015). Available documentation features also tend to be ‘flat’, lacking some of the advanced features such as branching logic and decision support to act on collected information and provide enhanced management, education and support services to patients.
Developing EHRs that support a team-based workflow requires an intimate understanding of how team members work together and interface with technology support and documentation practices. Team members need to be able to complete tasks but also communicate about patient care and rely on EHR-facilitated reminders and workflow support to track and ensure the follow-up/reconciliation of pending responsibilities. In one of the few studies to explore the interaction of team behaviour and effective EHR use, authors identified the importance of team agreement on methods of communication and the consistency of EHR role and documentation practices (Denomme et al. 2011). For EHRs to function as a reliable coordination platform for patient care, all team members need to know where specific information should be recorded and can be retrieved; tracking and other automated decision support or registry functionality also requires consistent (and complete) documentation. Other studies have mentioned the availability of a limited set of internal communication and coordination tools within the EHR (Cross et al. 2015; Donnelly et al. 2013; Legault et al. 2012; O’Malley et al. 2015). However, this has yet to be the subject of rigorous exploration or optimization.
Technology can also be deployed to facilitate the expansion of team member responsibilities and autonomy beyond traditional roles. Existing studies mention team-based care approaches in concert with the use of care templates (Cross et al. 2015; Graffy et al. 2010; Kendall et al. 2013; O’Malley et al. 2015), panel management tools (Kaferle and Wimsatt 2012), registries (Graffy et al. 2010; Rodriguez et al. 2014) and the use of patient engagement tools/shared decision-making applications (Chunchu et al. 2012; Friedberg et al. 2013), yet stop short of identifying synergies in these concepts. More conceptual work and empirical analyses remain to be done to understand the full implications of integrating these technologies with a TBC practice design, including the specific challenges and potential legal or financial ramifications of using IT to support and extend patient care roles for non-physician team members.
Discussion
This review synthesizes available research exploring how three key contextual factors—environment, task and technology —shape primary care practices’ implementation of team-based approaches to primary care. Important environmental considerations that emerged from existing literature include strong and invested physician leadership, performance measurement practices that reflect and support a ‘teams’ approach and reimbursement structures that facilitate enhanced use of non-physician staff. The changing nature of tasks and workflow in primary care service delivery, including an elevated focus on preventive care, patient engagement and disease management, bring into focus a need for new staffing models and an efficient restructuring of roles to support new care practices. Technology applications (e.g. EHRs, registries etc.) can support and enhance team-based care practices by enhancing communication, coordination, role support and care quality assurance.
Practice-level efforts to implement TBPC practices may involve significant restructuring of physician and non-physician team roles to survive in a changing healthcare environment. Physicians and administrators need to spearhead changes in organizational culture to support this level of learning and change. This includes clear goal-setting and commitment to supporting new team-based models through changes in compensation, physical infrastructure and how practice performance is measured, evaluated and acted upon. Educational programmes and interventions to facilitate a ‘teams transformation’ may prove useful, distilling key principles and tools to help with the interpersonal, psychosocial processes of developing well-functioning teams (Chan et al. 2010; Kozlowski and Ilgen 2006).
A second key implementation factor to consider is that the adoption of team-based care practices doesn’t take place in a vacuum. TBPC efforts can both support but also be influenced by other concurrent practice changes promoted under PCMH, such as enhanced patient engagement and patient-centric care management services as well as the use of EHRs. Information technology can help to support structured efforts to enhance non-physician care team roles, improve coordination and workflow and facilitate communication amongst team members. However, a number of continued challenges hinder practices’ ability to effectively leverage these strategies. For example, practices need to develop procedures to deal with asynchronous communication within the team, and figure out how to integrate documentation practices across multiple care team providers in a systematic way that makes finding and sharing patient information easy and reliable.
At the state and national policy level, reimbursement practices need to continue to shift away from a physician-based fee-for-service model and acknowledge new care team practice models. This includes a focus on pay-for-value, but more broadly requires acknowledging the care roles of non-physician staff in task-based reimbursement. Without aligned financial incentives, practice physicians and administrators will find it much harder to sustain TBPC efforts. Any efforts to reform reimbursement structure will also require clearer guidelines on the education, role and scope of practice for non-physician care team members. This is particularly true in the case of medical assistants, whose numbers continue to grow exponentially and whose role varies widely across practices.
Conclusion
This study is the first to synthesize available research on the contextual factors that impact the implementation of team-based care practices in primary care settings. Focusing on three key domains of environment, task and technology, I explore the conditions under which practices can most effectively leverage TBPC strategies, and identify key ways to foster more effective TBPC in the future. These findings enhance our understanding of the tenuous link between the adoption of TBPC and the improvement of patient as well as practice-level outcomes. Further research should consider the findings of this review to improve the nuance of empirical analyses in this area, seeking to explain not just whether using teams works, but when. Studying the mechanisms through which the adoption of team-based care practices can lead to better outcomes—both mediating structures or processes such as the consistent use of huddles, as well as moderating organizational factors like presence of an EHR or participation in pay-for-value programmes—provide actionable findings to improve policy reforms, organizational change processes and ultimately patient care.
References
Allan, H. T., Brearley, S., Byng, R., Christian, S., Clayton, J., MacKintosh, M., & Ross, F. (2014). People and teams matter in organizational change: Professionals’ and managers’ experiences of changing governance and incentives in primary care. Health Services Research, 49(1), 93–112.
Altschuler, J., Margolius, D., Bodenheimer, T., & Grumbach, K. (2012). Estimating a reasonable patient panel size for primary care physicians with team-based task delegation. Annals of Family Medicine, 10(5), 396–400.
Anand, S. G., Adams, W. G., & Zuckerman, B. S. (2010). Specialized care of overweight children in community health centers. Health Affairs, 29(4), 712–717.
Arksey, H., & O’Malley, L. (2005). Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology, 8(1), 19–32.
Bates, D. W., & Bitton, A. (2010). The future of health information technology in the patient-centered medical home. Health Affairs, 29(4), 614–621.
Belanger, E., & Rodríguez, C. (2008). More than the sum of its parts? A qualitative research synthesis on multi-disciplinary primary care teams. Journal of Interprofessional Care, 22(6), 587–597.
Boon, H. S., Mior, S. A., Barnsley, J., Ashbury, F. D., & Haig, R. (2009). The difference between Integration and collaboration in patient care: Results from key informant interviews working in multiprofessional health care teams. Journal of Manipulative and Physiological Therapeutics, 32(9), 715–722.
Bosch, M., Dijkstra, R., Wensing, M., Van Der Weijden, T., & Grol, R. (2008). Organizational culture, team climate and diabetes care in small office-based practices. BMC Health Services Research, 8(1), 180.
Bunniss, S., & Kelly, D. R. (2008). ‘The unknown becomes the known’: Collective learning and change in primary care teams. Medical Education, 42(12), 1185–1194.
Chan, B. C., Perkins, D., Wan, Q., Zwar, N., Daniel, C., Crookes, P., & Harris, M. F. (2010). Finding common ground? Evaluating an intervention to improve teamwork among primary health-care professionals. International Journal for Quality in Health Care, 22(6), 519–524.
Chesluk, B. J., & Holmboe, E. S. (2010). How teams work––Or don’t––In primary care: A field study on internal medicine practices. Health Affairs, 29(5), 874–879.
Chunchu, K., Mauksch, L., Charles, C., Ross, V., & Pauwels, J. (2012). A patient centered care plan in the EHR: Improving collaboration and engagement. Families, Systems, & Health, 30(3), 199.
Collinsworth, A., Vulimiri, M., Snead, C., & Walton, J. (2014). Community health workers in primary care practice redesigning health care delivery systems to extend and improve diabetes care in underserved populations. Health Promotion Practice, 15(Suppl. 2), 51S–61S.
Cross, D. A., Cohen, G. R., Nong, P., Day, A.-V., Vibbert, D., Naraharisetti, R., & Adler-Milstein, J. (2015). Improving EHR capabilities to facilitate stage 3 meaningful use care coordination criteria. AMIA Annual Symposium Proceedings, 5, 448–455.
Cutrona, S. L., Choudhry, N. K., Fischer, M. A., Servi, A., Liberman, J. N., Brennan, T., & Shrank, W. H. (2010). Modes of delivery for interventions to improve cardiovascular medication adherence: Review. American Journal of Managed Care, 16(12), 929.
Denomme, L. B., Terry, A. L., Brown, J. B., Thind, A., & Stewart, M. (2011). Primary health care teams’ experience of electronic medical record use after adoption. Family Medicine, 43(9), 632–642.
Donaldson, M. S., Yordy, K. D., Lohr, K. N., & Vanselow, N. A. (1996). Primary care: America’s health in a new era. Washington, DC: National Academies Press.
Donnelly, C., Brenchley, C., Crawford, C., & Letts, L. (2013). The integration of occupational therapy into primary care: A multiple case study design. BMC Family Practice, 14(1), 60.
Drach-Zahavy, A., & Freund, A. (2007). Team effectiveness under stress: A structural contingency approach. Journal of Organizational Behavior, 28(4), 423–450.
Edwards, S. T., Rubenstein, L. V., Meredith, L. S., Hackbarth, N. S., Stockdale, S. E., Cordasco, K. M., & Yano, E. M. (2015). Who is responsible for what tasks within primary care: Perceived task allocation among primary care providers and interdisciplinary team members. Healthcare, 3(3), 142–149.
Elder, N. C., Jacobson, C. J., Bolon, S. K., Fixler, J., Pallerla, H., Busick, C., … Pugnale, M. (2014). Patterns of relating between physicians and medical assistants in small family medicine offices. The Annals of Family Medicine, 12(2), 150–157.
Ferrer, R. L., Mody-Bailey, P., Jaén, C. R., Gott, S., & Araujo, S. (2009). A medical assistant-based program to promote healthy behaviors in primary care. The Annals of Family Medicine, 7(6), 504–512.
Finlayson, M. P., & Raymont, A. (2012). Teamwork-general practitioners and practice nurses working together in New Zealand. Journal of Primary Health Care, 4(2), 150–155.
Freund, T., Everett, C., Griffiths, P., Hudon, C., Naccarella, L., & Laurant, M. (2015). Skill mix, roles and remuneration in the primary care workforce: Who are the healthcare professionals in the primary care teams across the world? International Journal of Nursing Studies, 52(3), 727–743.
Friedberg, M. W., Van Busum, K., Wexler, R., Bowen, M., & Schneider, E. C. (2013). A demonstration of shared decision making in primary care highlights barriers to adoption and potential remedies. Health Affairs, 32(2), 268–275.
Friedman, E. L., Chawla, N., Morris, P. T., Castro, K. M., Carrigan, A. C., Das, I. P., & Clauser, S. B. (2014). Assessing the development of multidisciplinary care: Experience of the National Cancer Institute Community Cancer Centers Program. Journal of Oncology Practice, 11(1), 36–43.
Goldman, J., Meuser, J., Lawrie, L., Rogers, J., & Reeves, S. (2010). Interprofessional primary care protocols: A strategy to promote an evidence-based approach to teamwork and the delivery of care. Journal of Interprofessional Care, 24(6), 653–665.
Grace, S. M., Rich, J., Chin, W., & Rodriguez, H. P. (2014). Flexible implementation and integration of new team members to support patient-centered care. Healthcare, 2(2), 145–151.
Graffy, J., Grant, J., Williams, K., Cohn, S., Macbay, S., Griffin, S., & Kinmonth, A. L. (2010). More than measurement: Practice team experiences of screening for type 2 diabetes. Family Practice, 27(4), 386–394.
Grover, A., & Niecko-Najjum, L. M. (2013). Primary care teams: Are we there yet? Implications for workforce planning. Academic Medicine, 88(12), 1827–1829.
Hann, M., Bower, P., Campbell, S., Marshall, M., & Reeves, D. (2007). The association between culture, climate and quality of care in primary health care teams. Family Practice, 24(4), 323–329.
Hays, R. (2007). Measuring quality in the new era of team-based primary care. Quality in Primary Care, 15(3), 133–135.
Helfrich, C. D., Dolan, E. D., Simonetti, J., Reid, R. J., Joos, S., Wakefield, B. J. and Nelson, K. (2014). Elements of team-based care in a patient-centered medical home are associated with lower burnout among VA primary care employees. Journal of General Internal Medicine, 29(Suppl. 2), S659–S666.
Hilts, L., Howard, M., Price, D., Risdon, C., Agarwal, G., & Childs, A. (2013). Helping primary care teams emerge through a quality improvement program. Family Practice, 30(2), 204–211.
Howard, J., Shaw, E. K., Felsen, C. B., & Crabtree, B. F. (2012). Physicians as inclusive leaders: Insights from a participatory quality improvement intervention. Quality Management in Health Care, 21(3), 135–145.
Hudson, S. V., Ohman-Strickland, P., Cunningham, R., Ferrante, J. M., Hahn, K., & Crabtree, B. F. (2007). The effects of teamwork and system support on colorectal cancer screening in primary care practices. Cancer Detection and Prevention, 31(5), 417–423.
Hung, D. Y., Rundall, T. G., Crabtree, B. F., Tallia, A. F., Cohen, D. J., & Halpin, H. A. (2006). Influence of primary care practice and provider attributes on preventive service delivery. American Journal of Preventive Medicine, 30(5), 413–422.
Hysong, S. J., Knox, M. K., & Haidet, P. (2014). Examining clinical performance feedback in patient-aligned care teams. Journal of General Internal Medicine, 29(Suppl. 2), S667–S674.
Jesmin, S., Thind, A., & Sarma, S. (2012). Does team-based primary health care improve patients’ perception of outcomes? Evidence from the 2007–2008 Canadian survey of experiences with primary health. Health Policy, 105(1), 71–83.
Johnston, S., Green, M., Thille, P., Savage, C., Roberts, L., Russell, G., & Hogg, W. (2011). Performance feedback: An exploratory study to examine the acceptability and impact for interdisciplinary primary care teams. BMC Family Practice, 12(1), 14.
Kaferle, J. E., & Wimsatt, L. A. (2012). A team-based approach to providing asthma action plans. Journal of the American Board of Family Medicine, 25(2), 247–249.
Kastner, M., Tricco, A. C., Soobiah, C., Lillie, E., Perrier, L., Horsley, T., … Straus, S. E. (2012). What is the most appropriate knowledge synthesis method to conduct a review? Protocol for a scoping review. BMC Medical Research Methodology, 12(1), 114.
Kendall, M., Mason, B., Momen, N., Barclay, S., Munday, D., Lovick, R., … Cormie, P. (2013). Proactive cancer care in primary care: A mixed-methods study. Family Practice, 30(3), 302–312.
Kim, T. W., Saitz, R., Kretsch, N., Cruz, A., Winter, M. R., Shanahan, C. W., & Alford, D. P. (2013). Screening for unhealthy alcohol and other drug use by health educators: Do primary care clinicians document screening results? Journal of Addiction Medicine, 7(3), 204–209.
Kozlowski, S. W., & Ilgen, D. R. (2006). Enhancing the effectiveness of work groups and teams. Psychological Science in the Public Interest, 7(3), 77–124.
Ladden, M. D., Bodenheimer, T., Fishman, N. W., Flinter, M., Hsu, C., Parchman, M., & Wagner, E. H. (2013). The emerging primary care workforce: Preliminary observations from the primary care team: Learning from effective ambulatory practices project. Academic Medicine, 88(12), 1830–1834.
Legault, F., Humbert, J., Amos, S., Hogg, W., Ward, N., Dahrouge, S., & Ziebell, L. (2012). Difficulties encountered in collaborative care: Logistics trumps desire. Journal of the American Board of Family Medicine, 25(2), 168–176.
Lemieux-Charles, L., & McGuire, W. L. (2006). What do we know about health care team effectiveness? A review of the literature. Medical Care Research and Review, 63(3), 263–300.
Margolius, D., Wong, J., Goldman, M. L., Rouse-Iniguez, J., & Bodenheimer, T. (2012). Delegating responsibility from clinicians to nonprofessional personnel: The example of hypertension control. Journal of the American Board of Family Medicine, 25(2), 209–215.
McAllister, J. W., Carl Cooley, W., Van Cleave, J., Boudreau, A. A., & Kuhlthau, K. (2013). Medical home transformation in pediatric primary care-what drives change? Annals of Family Medicine, 11(SUPPL. 1), S90–S98.
McInnes, S., Peters, K., Bonney, A., & Halcomb, E. (2015). An integrative review of facilitators and barriers influencing collaboration and teamwork between general practitioners and nurses working in general practice. Journal of Advanced Nursing, 71(9), 1973–1985.
Mechanic, R. E., Santos, P., Landon, B. E., & Chernew, M. E. (2011). Medical group responses to global payment: Early lessons from the ‘alternative quality contract’ in Massachusetts. Health Affairs, 30(9), 1734–1742.
Mitchell, P., Wynia, M., Golden, R., McNellis, B., Okun, S., Webb, C. E., Von Kohorn, I. (2012). Core principles & values of effective team-based health care. Washington, DC: Institute of Medicine.
Mohr, D. C., Benzer, J. K., & Young, G. J. (2013). Provider workload and quality of care in primary care settings: Moderating role of relational climate. Medical Care, 51(1), 108–114.
Morrissey, J. (2013). Filling the gaps in primary care: New roles strengthen relationships with patients. Trustee: The Journal for Hospital Governing Boards, 66(4), 8–10.
Ngo, V., Hammer, H., & Bodenheimer, T. (2010). Health coaching in the teamlet model: A case study. Journal of General Internal Medicine, 25(12), 1375–1378.
O’Malley, A. S., Gourevitch, R., Draper, K., Bond, A., & Tirodkar, M. A. (2014). Overcoming challenges to teamwork in patient-centered medical homes: A qualitative study. Journal of General Internal Medicine, 30(2), 183–192.
O’Malley, A. S., Draper, K., Gourevitch, R., Cross, D. A., & Scholle, S. H. (2015). Electronic health records and support for primary care teamwork. Journal of the American Medical Informatics Association, 22(2), 426–434.
O’Toole, T. P., Cabral, R., Blumen, J. M., & Blake, D. A. (2011). Building high functioning clinical teams through quality improvement initiatives. Quality in Primary Care, 19(1), 13–22.
Page, N. (2006). Task overlap among primary care team members: An opportunity for system redesign? Journal of Healthcare Management, 51(5), 295.
Pullon, S., McKinlay, E., & Dew, K. (2009). Primary health care in New Zealand: The impact of organisational factors on teamwork. British Journal of General Practice, 59(560), 191–197.
Roblin, D. W., Howard, D. H., Junling, R., & Becker, E. R. (2011). An evaluation of the influence of primary care team functioning on the health of Medicare beneficiaries. Medical Care Research & Review, 68(2), 177–201.
Rodriguez, H. P., Chen, X., Martinez, A. E., & Friedberg, M. W. (2015a). Availability of primary care team members can improve teamwork and readiness for change. Health Care Management Review, 41(4), 286–295.
Rodriguez, H. P., Ivey, S. L., Raffetto, B. J., Vaughn, J., Knox, M., Hanley, H. R., … Shortell, S. M. (2014). As good as it gets? Managing risks of cardiovascular disease in California’s top-performing physician organizations. Joint Commission Journal on Quality and Patient Safety, 40(4), 148–158.
Rodriguez, H. P., Meredith, L. S., Hamilton, A. B., Yano, E. M., & Rubenstein, L. V. (2015b). Huddle up! The adoption and use of structured team communication for VA medical home implementation. Health Care Management Review, 40(4), 286–299.
Roper, R. (2014). Insights on innovative strategies for harnessing health information technology to help individuals, teams. Journal of Ambulatory Care Management, 37(2), 96–99.
Saba, G. W., Villela, T. J., Chen, E., Hammer, H., & Bodenheimer, T. (2012). The myth of the lone physician: Toward a collaborative alternative. The Annals of Family Medicine, 10(2), 169–173.
Sanchez, K., & Adorno, G. (2013). “It’s like being a well-loved child”: Reflections from a collaborative care team. The Primary Care Companion for CNS Disorders, 15(6), PCC.13m01541. http://doi.org/10.4088/PCC.13m01541.
Savarimuthu, S. M., Jensen, A. E., Schoenthaler, A., Dembitzer, A., Tenner, C., Gillespie, C., … Sherman, S. E. (2013). Developing a toolkit for panel management: Improving hypertension and smoking cessation outcomes in primary care at the VA. BMC Family Practice, 14(1), 176.
Shipman, S. A., & Sinsky, C. A. (2013). Expanding primary care capacity by reducing waste and improving the efficiency of care. Health Affairs, 32(11), 1990–1997.
Starfield, B., Shi, L., & Macinko, J. (2005). Contribution of primary care to health systems and health. Milbank Quarterly, 83(3), 457–502.
Strumpf, E., Levesque, J.-F., Coyle, N., Hutchison, B., Barnes, M., & Wedel, R. J. (2012). Innovative and diverse strategies toward primary health care reform: lessons learned from the Canadian experience. Journal of the American Board of Family Medicine, 25(Suppl 1), S27–S33.
Thomas, M. H. (2014). Development and implementation of a pharmacist-delivered Medicare annual wellness visit at a family practice office. Journal of the American Pharmacists Association, 54(4), 427–434.
True, G., Stewart, G. L., Lampman, M., Pelak, M., & Solimeo, S. L. (2014). Teamwork and delegation in medical homes: Primary care staff perspectives in the Veterans Health Administration. Journal of General Internal Medicine, 29(Suppl. 2), S632–S639.
Watts, B., Lawrence, R. H., Singh, S., Wagner, C., Augustine, S., & Singh, M. K. (2014). Implementation of quality improvement skills by primary care teams: Case study of a large academic practice. Journal of Primary Care and Community Health, 5(2), 101–106.
Wholey, D. R., White, K. M., Adair, R., Christianson, J. B., Lee, S., & Elumba, D. (2013). Care guides: An examination of occupational conflict and role relationships in primary care. Health Care Management Review, 38(4), 272–283.
Willard-Grace, R., Hessler, D., Rogers, E., Dubé, K., Bodenheimer, T., & Grumbach, K. (2014). Team structure and culture are associated with lower burnout in primary care. Journal of the American Board of Family Medicine, 27(2), 229–238.
Wise, C. G., Alexander, J. A., Green, L. A., Cohen, G. R., & Koster, C. R. (2011). Journey toward a patient-centered medical home: Readiness for change in primary care practices. Milbank Quarterly, 89(3), 399–424.
Xyrichis, A., & Lowton, K. (2008). What fosters or prevents interprofessional teamworking in primary and community care? A literature review. International Journal of Nursing Studies, 45(1), 140–153.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 The Author(s)
About this chapter
Cite this chapter
Cross, D.A. (2018). Contextual Factors Affecting the Implementation of Team-Based Primary Care: A Scoping Review. In: McDermott, A., Kitchener, M., Exworthy, M. (eds) Managing Improvement in Healthcare. Organizational Behaviour in Health Care. Palgrave Macmillan, Cham. https://doi.org/10.1007/978-3-319-62235-4_5
Download citation
DOI: https://doi.org/10.1007/978-3-319-62235-4_5
Published:
Publisher Name: Palgrave Macmillan, Cham
Print ISBN: 978-3-319-62234-7
Online ISBN: 978-3-319-62235-4
eBook Packages: Business and ManagementBusiness and Management (R0)