
Abstract
This study proposed a quantitative estimation method for interpersonal distance by using a prototype measurement system. With the aid of motion capture technology and marker caps, we estimated the body position and orientation of children with autism spectrum disorders (ASD) and their therapists. A prototype measurement system was introduced in practicing therapy rooms and captured behavior during ongoing therapy for children with ASD. This study confirmed that approaching behavior and, to a lesser extent, interpersonal distance can be effectively estimated using the proposed motion capture system. Additional system improvements are required to capture face-to-face behavior.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others

Keywords
1 Introduction
Interpersonal distance is an important factor in nonverbal communication. High demands exist for quantitative evaluation of nonverbal communication in social skills development training for children with autism spectrum disorders (ASD). In the field of psychology, researchers have evaluated personal space and interpersonal distance for children with ASD who have difficulties using nonverbal cues [1–3]. In these prior studies, interpersonal distance data were collected by human observers reviewing videos. Data captured using this human-based method was investment of time. Regarding intervention for children with ASD, an easy and quantitative understanding of children’s behavior and dynamic response–such as approaching or avoiding in response to each therapeutic activity–is essential. This study proposes a technology-based method for the quantitative estimation of interpersonal distances and face-to-face behavior. The technology, Social Imaging [4], was used to identify and represent social behaviors. We designed a soft marker cap that can be easily worn by children and used with the motion capture technology to record changes in interpersonal distance between the child with ASD and their therapist. This prototype measurement system was introduced in a practicing therapy room and captured ongoing therapy for children with ASD. In this paper, we report the analysis results regarding the quantitative estimation of interpersonal distance from captured data.
2 Method
2.1 Measurement
The most common quantitative evaluation method for interpersonal distance is the stop-distance method [1]. This method requires two persons to approach one another until they feel discomfort or unpleasantness; the distance between their toe positions at this final point is measured. Although commonly used, this method presents an unnatural situation for measuring interpersonal distance. Motion capture systems, similar to the one proposed in this study, show promise for accurately measuring interpersonal distance in a natural environment without observation. However, many ASD children have hypersensitivity [5, 6] that makes them resist multiple motion capture markers on their body. In Japan, children wear caps in school and during physical education. Most ASD children are also accustomed to wearing a cap without elastic straps. Based on these observations, Fig. 1 shows the marker cap developed in this study capable of measuring children’s position and orientation.

Soft marker cap for motion capture (Color figure online)
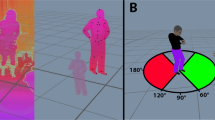
Optitrack’s Flex3 motion capture system and Motive software [7] were used in this study. When estimating interpersonal distance, close (approaching) and away (avoiding) motions for both children and therapists are important. Equations (1–3) describe these motions, where C(t) is the position of the child and T(t) is the position of the therapist, both at time t.
If both the child and therapist remain stationary (do not move), \(\alpha = 0 \cap \beta =~0\). If only the child moves, \(\alpha \ne \beta \ne 0 \cap \alpha - \beta = 0\). If only the therapist moves, \(\alpha > 0 \cap \beta = 0\). If both the child and therapist move, \(\alpha ( t) - \alpha (t - \tau ) = 0 \cap \beta \ne 0\). If \(D(t) > 0\), the subjects are approaching. If \(D(t) < 0\), the subjects are avoiding. Motion capture technologies can also calculate position and orientation. Researchers in one prior study determined the field of view (FOV) for face-to-face communication to be 129 [8]. This study used this criterion when estimating interpersonal distances with and without face-to-face communication.
2.2 Experimentation
Figure 2 shows the experimental setup used in this study to quantitatively estimate interpersonal distance. Children with ASD and their therapists wore the marker cap (shown previously in Fig. 1) for motion capture during the one-hour therapy session. Four children with ASD participated in this experiment. Table 1 summarizes participant characteristics. All participants were male with chronological ages (CA) ranging from approximately 4 to 6 years old. Developmental ages (DA)-derived using the Kyoto Scale of Psychological Development [9]-ranged from approximately 2 to 4 years old. The Kyoto Scale scores various subcategories of physical motion, verbal-social skills, cognitive-adaptation skills, and total developmental age. Participants were also assessed using the Pervasive Development Disorders Autism Society Japan Rating Scale (PARS) [10] and the Childhood Autism Rating Scale (CARS) [11]. Both assessments are used to confirm ASD diagnosis. This experiment was approved by the Institutional Review Board, and participants joined in the experiment after providing informed consent.
Both two video cameras for human coder (professional psychologist) and the motion capture system recorded motion behavior of the child participants and their therapists during the standing therapy sessions. Physical motion under 0.5 m/s is considered stagnant movement in preschool-aged children [12]. The human coder observed and recorded (in ms) predefined behaviors during therapy activities. Table 2 lists the predefined behaviors captured by the human observer. The frame rate of motion capture for the technology was set to 60 fps.

Experimental setup in therapy room
3 Result
Figures 3, 4, 5 and 6 show the participating children’s approach (value in Eqs. 1–3) and face-to-face behavior recorded by both the human coder and motion capture system. Table 3 shows the rate of agreement between the human coder and the motion capture system when recording approaching behavior. For each of the participants, behavior data captured by the human coder and technology were similar when recording approaching behavior with one exception–participant B (Fig. 4). Comparatively, the rate of agreement when recording face-to-face behaviors was not as high.

Participant A results for approaching and face-to-face behavior

Participant B results for approaching and face-to-face behavior

Participant C results for approaching and face-to-face behavior

Participant D results for approaching and face-to-face behavior
4 Discussion
This study confirmed that approaching behavior can be effectively captured using the proposed motion capture system. Additionally, we confirmed that the system can dynamically estimate changes in interpersonal distance, but the agreement rate is not as high likely because of the limited capture frame. More differences were observed between the human coder and technology when recording face-to-face behavior. The human observer considered face-to-face behavior for a shorter period of time compared with the motion capture system in many cases. The obtained motion data may be used to develop an advanced behavior model that improves face-to-face behavior recognition. In addition, the marker cap was occasionally out of alignment due to the actions of the children. Design enhancements are needed to reduce this occurrence.
5 Conclusion
In this study, a method and prototype system for quantitatively estimating interpersonal distance by using motion capture technology and a marker cap for children with ASD was proposed. Future work includes design improvements to the marker cap so that it remains in place and further analysis of the experimental data to improve upon estimation methods.
References
Gessaroli, E., Santelli, E., di Pellegrino, G., Frassinetti, F.: Personal space regulation in childhood autism spectrum disorders. PloS One 8(9), e74959 (2013)
Pedersen, J., Livoir-Petersen, M., Schelde, J.: An ethological approach to autism: an analysis of visual behaviour and interpersonal contact in a child versus adult interaction. Acta Psychiatr. Scand. 80(4), 346–355 (1989)
Rogers, A.L., Fine, H.J.: Personal distance in play therapy with an autistic and a symbiotic psychotic child. Psychother. Theor. Res. Pract. 14(1), 41 (1977)
Suzuki, K.: Social imaging technology to identify and represent social behaviors. In: Proceedings of the 2015 ACM International Joint Conference on Pervasive and Ubiquitous Computing and Proceedings of the 2015 ACM International Symposium on Wearable Computers, pp. 907–908. ACM (2015)
Rogers, S.J., Hepburn, S., Wehner, E.: Parent reports of sensory symptoms in toddlers with autism and those with other developmental disorders. J. Autism Dev. Disord. 33(6), 631–642 (2003)
Tomchek, S.D., Dunn, W.: Sensory processing in children with and without autism: a comparative study using the short sensory profile. Am. J. Occup. Ther. 61(2), 190–200 (2007)
Optitrack. http://www.optitrack.com/
Pan, Y., Hirokawa, M., Suzuki, K.: Measuring k-degree facial interaction between robot and children with autism spectrum disorders, Robot and Human Interactive Communication (RO-MAN). In: 2015 24th IEEE International Symposium on IEEE, pp. 48–53 (2015)
Ikuzawa, M., Matsushita, Y., Nakase, A.: Kyoto scale of psychological development 2001. Kyoto International Social Welfare Exchange Centre, Kyoto (2002)
Ito, H., Tani, I., Yukihiro, R., Adachi, J., Hara, K., Ogasawara, M., Inoue, M., Kamio, Y., Nakamura, K., Uchiyama, T., et al.: Validation of an interview-based rating scale developed in japan for pervasive developmental disorders. Res. Autism Spectr. Disord. 6(4), 1265–1272 (2012)
Schopler, R.J.R.E., Renner, B.R.: The childhood autism rating scales (cars). Western Psychological Services, Los Angeles, Calif, USA (1988)
DeJaeger, D., Willems, P.A., Heglund, N.C.: The energy cost of walking in children. Pflügers Archiv 441(4), 538–543 (2001)
Acknowledgments
This study was supported by JST-CREST “Social Imaging for All Children’s Education Supporting Creative Activities and Facilitating Social Interaction.”
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this paper
Cite this paper
Tsuji, A., Matsuda, S., Suzuki, K. (2016). Interpersonal Distance and Face-to-face Behavior During Therapeutic Activities for Children with ASD. In: Miesenberger, K., Bühler, C., Penaz, P. (eds) Computers Helping People with Special Needs. ICCHP 2016. Lecture Notes in Computer Science(), vol 9759. Springer, Cham. https://doi.org/10.1007/978-3-319-41267-2_52
Download citation
DOI: https://doi.org/10.1007/978-3-319-41267-2_52
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-41266-5
Online ISBN: 978-3-319-41267-2
eBook Packages: Computer ScienceComputer Science (R0)