
Abstract
Nanomaterials have been shown to have physical and chemical properties that have opened new avenues for cancer diagnosis and therapy. Nanoconstructs that enhance existing treatments for cancer, such as radiation therapy, are being explored in several different ways. Two general paths toward nanomaterial-enabled radiosensitization have been explored: (1) improving the effectiveness of ionizing radiation and (2) modulating cellular pathways leading to a disturbance of cellular homeostasis, thus rendering the cells more susceptible to radiation-induced damage. A variety of different agents that work via one of these two approaches have been explored, many of which modulate direct and indirect DNA damage (gold), radiosensitivity through hyperthermia (Fe), and different cellular pathways. There have been many in vitro successes with the use of nanomaterials for radiosensitization, but in vivo testing has been less efficacious, predominantly because of difficulty in targeting the nanoparticles. As improved methods for tumor targeting become available, it is anticipated that nanomaterials can become clinically useful radiosensitizers for radiation therapy.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Physical and chemical peculiarities of nanomaterials and their distinct differences from biological molecules upon internalization by cells or tissues open new avenues for anticancer treatments in all fields of oncology including radiation oncology. Considering that radiation is used for treatment of over 50 % of all cancers, agents that could modulate the effects of radiotherapy generate much interest in the field. Probably the most drastic differences between biological molecules and nanomaterials can be observed with respect to their “response” to ionizing radiation. While chemical bonds of most organic polymers suffer radiation damage, most nanomaterials accept or release electrons and photons without significant structural changes following radiation exposure. Moreover, depending on their surface modifications, the same nanostructures sometimes have opposite effects on their immediate (bio)chemical surroundings. Thus, for example, fullerenes (C60) increase reactive oxygen species (ROS) accumulation in cells in conjunction with ionizing radiation (e.g. [44]) leading to increased cell death, while hydroxyl group-modified fullerenes (C60OH24) have been found to be antioxidative and antiapoptotic (e.g. [55]).
In whole cells, ROS generated from the radiolysis of water is one of most pronounced, though not the only effect of ionizing radiation (e.g. [14]). ROS can cause damage to any one of the cellular components—nucleic acids, proteins, sugars and lipids, as well as direct energy deposition and ionization. Due to their short half-life in cells ROS traverse no more than 6 nm on average [53]; therefore ROS formation inside cell nuclei, close to the DNA is the most damaging for cells as it leads to the formation of DNA single-strand and double-strand breaks (DNA SSBs and DSBs). The extent of DNA damage in cells is most often measured by single cell gel electrophoresis (or “comet assay”) which is extremely sensitive or, for “bulk” cells, with pulsed field electrophoresis, a technique much less sensitive to DNA damage which requires high doses of radiation for detection [46]. Repair of DNA DSBs, completeness and accuracy of the repair make up the critical decision moment for irradiated cells. Misrepaired or unrepaired DNA damage can lead to cell death via apoptosis, autophagy, necrosis, or mitotic catastrophe. While cell death is often evaluated with clonogenic survival assays, the numbers and persistence of DNA DSB foci—complexes of proteins making up the DNA repair machinery, detected by immunocytochemistry—are used as a measure of the cellular ability to repair damage induced by irradiation [54]. The presence of nanomaterials in cells, in different subcellular compartments, can perturb either (or both) the physicochemical outcomes of radiation or the cellular capacity to repair radiation-induced damage. While some nanoconstructs may protect cells from the effects of radiation or have no “interactions” with radiation, nanoconstructs that increase cytotoxic effects of radiation—the radiosensitizing nanoconstructs, have opened a new area of study in the field of radiation oncology.
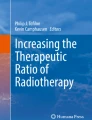
Two general paths for nanomaterial-enabled radiosensitization include: (a) the improvement of the effectiveness of ionizing radiation (e.g. by increasing energy deposition or by fortifying production of ROS) (Fig. 1) and (b) the modulation of cellular pathways and the disturbance of cellular homeostasis to render cells more susceptible to radiation (Fig. 2).

Schematic drawing of radiocatalysis by nanoparticles. Exposure of nanoparticles to ionizing radiation (e.g. X-rays) causes Compton and Photoelectric effects—photoelectrons and Auger electrons (e−) are ejected from the nanoparticles as well as photons of different energies, including secondary fluorescent X-rays. In addition, in semiconductor nanoparticles release of electrons leads to formation of reactive electropositive holes (h+) on nanoparticle surface. Free electrons and electropositive holes on nanoparticle surface can damage cellular components directly or lead to production of reactive oxygen species (superoxide \({\text{O}}_{{ 2 }}^{\cdot { - }}\), hydroxyl radical \({^{\cdot}}{\text{OH}}\), hydrogen peroxide H2O2) which are also formed by radiolysis of water (adapted from [2, 24, 39])

Cellular effects of radiosensitizing nanomaterials. Several different “pathways” to radiosensitization by nanoparticles exist. In the first place, free electrons (released by nanoparticle ionization) are absorbed by surrounding molecules within 15–200 nm from particle surface (e.g. [2, 73]) and ROS (which on average traverse 6 nm distances in cytosol [53]) produced by nanoparticles damage cellular components in addition to incident ionizing radiation and products of water radiolysis. Free electrons and ROS oxidize proteins, peroxidize lipid membranes (cell and organelle membranes both), and produce SSBs and DSBs in DNA [14]. Secondly, nanomaterials may be used to develop hyperthermia under the influence of alternating magnetic field or near infrared light (e.g. [1, 33]). Thirdly, physical interactions between nanomaterials and cellular components, biomolecules, molecular assemblies, and organelles modulate behavior of these cellular elements in different ways leading to such outcomes as perturbations in cell cycle or DNA repair (e.g. [2, 69]). Fourthly, nanomaterials can be made of components (or carry a cargo) specifically designed to make the recipient cells more sensitive to radiation, such as, e.g. delivery of anisense oligonucleotides for DNA repair regulating genes, miRs, or delivery of weak ligands for UPS machinery (e.g. [3, 27, 74])
It should also be emphasized that for optimal nanoparticle-mediated radiosensitization, targeting of nanomaterials to specific cell types or subcellular organelles plays a significant role. While selection of best targeting moiety is in and of itself a complicated task, it should be remembered that surface modifications on nanomaterials are not static—nanomaterials accumulate and exchange components of tightly and loosely bound surface protein corona as they progress through cells and their environment (e.g. [40]). According to the “therapeutic ratio” concept, modulating radiation effects on all the cells in the organism equally would provide no advantage over radiation alone if radiation could not be targeted. Therefore, precise in vivo tissue-specific and subcellular delivery of nanomaterials plays a big role in the development of radiosensitizing nanoparticle constructs. However, while (some type) of targeting is absolutely essential for other anticancer nanoparticle formulations (for reviews see e.g. [47]), fortunately that is not so for radiosensitizing nanoconstructs. Ionizing radiation delivery has become so sophisticated that different treatment modalities enable dose delivery closely matching tumor topology. In such a scenario radiosensitizing nanoconstructs would further potentiate such dose differences. In any event, several other chapters of this book discuss nanoparticle targeting more directly, hence this topic will not be specifically addressed here. Rather, this chapter will focus on molecular and biochemical events that occur when nanoparticles are placed in the path of ionizing radiation quality photons. In the interest of brevity, we will not discuss either the basics of radiation physics and radiation biology or the molecular mechanisms relevant for cellular responses to radiation. Much more on these topics can be found in several radiation biology textbooks, e.g. [14, 25]. Finally, the use of nanoparticles for delivery of radionuclides (e.g. [45]) or the delivery of “small molecule” radiosensitizers (e.g. cisplatin [71], paclitaxel [61, 64], docetaxel [63], or curcumin [67]) will also not be covered in this chapter, as this research belongs more appropriately into the topic of “cargo delivery” with nanoparticles, covered conceptually in other chapters of this book. We will touch only very briefly upon nanoconstruct-mediated nucleic acids delivery focusing on those cases where nucleic acids are especially relevant for regulating susceptibility toward ionizing radiation exposure.
Elemental and molecular compositions of nanoparticles discussed in this chapter will include gold, platinum, silver, cerium oxide nanoparticles, gadolinium-doped titanium dioxide and titanium dioxide, iron oxides, copper oxide, gadolinium-carrying nanoparticles, as well as a few polymeric nanoparticles made of elements with small Z values. In response to ionizing radiation elements with higher atomic numbers (greater Z value) produce energetic secondary X-rays, photoelectrons and Auger electrons, while lower Z elements release predominantly Auger electrons; the same is true for nanomaterials made of these materials [2]. Several high Z materials that have been tested as radiosensitizers, e.g. iodine [34] or germanium oxide [29], were found to work as radiosensitizers equally well as single molecules or as nanoparticle formulations.
Finally, we will also speculate about additional, potentially radiosensitizing (but not yet tested with radiation), nanoparticles. One can predict, for example, that nanoparticles that perturb the cell cycle may serve as radiosensitizers. Chemotherapeutic drugs with such properties have been in use for chemoradiotherapy for many years. For example, paclitaxel treatment favors accumulation of cancer cells in G2 and M phases, the most radiation-sensitive phases of the cell cycle, and for that reason it synergistically interacts with ionizing radiation [57]. Incidentally, poly(D,L-lactide-coglycolide)(PLGA) nanoparticles containing taxols are currently being developed as radiosensitizers [18].
1.1 Irradiation in the Presence of Nanomaterials—Effects on Specific (Sub)Cellular Structures and Chemical Milieu
Genomic DNA is the most important target of radiation-induced cellular killing, and therefore we will begin by reviewing work that investigated interactions between DNA and nanoparticles in vitro in the course of exposure to ionizing radiation [73]. The formation of single-strand and double-strand (SSBs and DSBs) DNA breaks in an in vitro setup, using plasmid DNA and gold nanoparticles was used as a proxy for the physicochemical processes governing gold-mediated increase in DNA damage. The basic mechanisms underlying this DNA sensitization were evaluated with electron bombardment with different electron energies [73]. In this study, low electron energies of 1, 10, and 100 eV as well as high energy 60 keV electrons were used. In addition to “standard” DNA lesions such as the SSB and DSB, loss of supercoiled DNA was also used as an index of DNA damage. In this work, considerations for the use of appropriate controls led the authors to compare pure plasmid DNA with “salted DNA” (three Na+ per base) and 1:1 (one particle per plasmid) complexes of DNA with gold nanoparticles (solid gold particles 5 ± 2 nm in size). The yields of all three types of DNA damage (SSB, DSB, and supercoil loss) were enhanced by a factor of 2 or more when plasmid–nanoparticle complexes were compared to the salted DNA sample. This increase was the greatest when 10 eV electrons were used to irradiate DNA–nanoparticle complexes. This finding was explained by the fact that the damage to DNA with 10 eV electrons comes from transient anions forming in the DNA molecule (i.e., the bases, sugar, and phosphate groups) and the gold nanoparticles as well. These anions are resolved either by dissociative electron attachment (DEA), or by deposition of energy into local chemical bonds, resulting in bond breakage. Because DNA damage increased when electrons of 1 and 10 eV are used with nanoparticle–DNA complexes, the authors contended that the gold nanoparticles greatly increase the DEA cross section. Overall, the mechanisms responsible for plasmid DNA damage caused by gold nanoparticles and radiation included: [1] the production of short-range secondary electrons by the gold that has absorbed incoming electrons, with a high probability of interacting with the DNA if the gold particles are in complex with it, and [2] the efficient absorption of low energy electrons by the gold nanoparticles. Moreover, Sanche and collaborators consider these mechanisms critical for gold nanoparticle-dependent DNA damage caused by exposure to X-rays as well, especially for photon energies of 100–110 keV (produced at 100–250 kVp) [73]. It is worth noting, however, that any increase in the distance between the gold nanoparticle surface and plasmid DNA led to a decrease in DNA damage as well. For example, gold nanoparticles coated either with thiolated undecane, dithiolated diethylenetriaminepentaacetic or gadolinium chelating agents reduce (for the same nanoparticle size, particle:plasmid ratio and irradiation conditions) DNA damage enhancement from 2.3 to 1.6 [66].
Using a nucleic acid free system, i.e., gold and silver nanoparticles embedded in an alanine matrix, one recent study used electron spin resonance spectroscopy (ESR) to evaluate dose enhancement in the presence of gold and silver nanoparticles [11]. A conclusion from this work was that, irrespective of X-ray energy, larger and distantly spaced nanoparticles do not cause dose enhancement compared to smaller and closely clustered nanoparticles. Both silver and gold nanoparticles were used in numerous in vitro and in vivo assays (see Sect. 1.2).
In addition to low linear energy transfer (low LET) irradiation (X-rays and gamma rays and free electrons), heavy ion irradiation can be combined with the nanoparticles use as well. Two recent studies by Porcel and others [49, 50] with plasmid DNA and 3 nm platinum nanoparticles coated with polyacrylic acid compared effects of gamma rays with particulate, high linear energy transfer (high LET) irradiation. In this case SSBs and DSBs in plasmid DNA were caused by exposure to gamma rays (with LET = 0.2 keV/μm) and several heavy ions (He2+ LET = 2.3 keV/μm and C6+ LET = 13 keV/μm and LET = 110 keV/μm) alone or in combination with platinum nanoparticles. In all cases nanoparticle addition increased the effects of radiation damage. Use of high Z element (HZE) nanoparticles may be an interesting way to increase the efficiency of high LET radiation treatments.
A comprehensive cell-free study on gold nanoparticles in aqueous solution (without addition of nucleic acids) was also done recently by Misawa and Takahashi [39]. Diagnostic quality X-rays (with a dose rate of 1 Gy/min) in the presence of gold nanoparticles (5–250 nm in diameter) produced increased amounts of reactive oxygen species (ROS), compared to irradiation of aqueous media alone; this increase reached 1.46 for ∙OH and 7.68 for \({\text{O}}_{{ 2^{ - } }}\). This finding was explained in part by electron emission of both photo- and Auger electrons and emission of photons of secondary fluorescent X-rays. The authors found that fluorescent X-ray production (which may lead to secondary excitations) and ionization along the X-ray path depended primarily on the volume of the gold particles. More dramatically, however, ROS generation in the presence of gold nanoparticles was inversely proportional to particle diameter indicating that the dominant parameter for ROS production is the surface area of nanoparticles, and not their weight percentage, possibly due to catalytic effects at the particle–water interface. The ROS species evaluated were ∙OH, \({\text{O}}_{{ 2^{ - } }}\) and 1O2, all of them biologically relevant, with diffusion lengths reaching no more than a few hundreds of nanometers in aqueous media. As mentioned earlier, in a more complex environment of cytosol or nucleosol most ROS progress no more than 6 nm on average [53]. In general, ∙OH species interact with lipids, polysaccharides, proteins, and nucleic acids rapidly and locally. \({\text{O}}_{{ 2^{ - } }}\) radicals react more slowly with lipids, however, in the presence of iron and hydrogen peroxide these radicals can lead to production of ∙OH radicals (these chemical processes are described by Haber–Weiss and Fenton reactions). Finally, 1O2 radicals react with unsaturated fatty acids, beta-carotene, amino acids, and methionine. Each one of these interactions damages biomolecules and causes stress than can lead to cell death or genomic instability.
1.2 Irradiation in the Presence of Nanomaterials—Effects on Cells in Vitro and/or Tumors in Vivo
While it is known that irradiation of gold nanoparticles in complexes with DNA leads to DNA damage, the effects of gold nanoparticles on whole cells are far more complex and have rarely been fully investigated in a single research paper. Most frequently, in cellular in vitro studies changes in cell viability are the primary endpoint of investigation, and the exact mode of action of nanoparticles has received relatively little attention. A few examples of such work (see Sect. 2) suggest that biochemical/biological effects of gold nanoparticles play perhaps an even greater role in radiosensitization than the production of secondary electrons.
In an effort to investigate the exact radiation parameters for increased radiation-dependent cell killing in vitro in the presence of gold nanoparticles, Rahman and others [51] used 1.9 nm gold nanoparticles (mixed at 0.197 mg/ml) with bovine aortic cells and exposed such cells to monochromatic, synchrotron-generated X-rays of 30, 40, 50, 60, 70, 81, and 100 keV. The greatest dose enhancement in cell killing was found for the combination of gold nanoparticles with 40 keV X-rays, followed by 50 and 60 keV dose enhancement values. Gold nanoparticles were also tested in combination with proton irradiation [48], and increased cell killing was found in samples of cells that had internalized the nanoparticles. (It should be noted that prolific ROS production outside of cells but close to cellular membrane can lead to cell death as well.)
Increased efficiency of radiation was also noted when radioactive seed therapy (I-125 brachytherapy seeds) was combined with gold nanoparticles [43]. Dose ranges varied between 2.1 and 4.5 cGy/h with an even dose distribution in adherent layers of HeLa cells. These cells were treated with 50 nm gold nanoparticles, and the number of gamma H2AX foci (signifying DNA DSBs) following irradiation in nanoparticle treated cells was 1.7–2.3 fold greater compared to controls.
Nanoconstructs prepared by simple one-pot synthesis as silver nanoparticles coated with egg white proteins were used to radiosenistize breast adenocarcinoma cells [30]; increasing concentration of nanoparticles with a fixed (4 Gy) irradiation led to increased cell killing even though no cytotoxicity was recorded in the absence of radiation, even at the maximal concentration of conjugates (12 mg/L).
Silver was also used to make the shell on the surface of carbon nanodots [24]. These nanoconstructs (5–100 nm in size including polyethylene glycol (PEG) coating) were tested in vitro both for photodynamic therapy and as radiosensitizers. Reduction in cell survival of Du145 prostate cancer cells with combination treatment, compared to radiation alone, was twofold with 15 Gy.
A growing body of literature shows promising data on nanoparticle-mediated radiosensitization in vivo. For example, syngeneic EMT-6 mammary tumors implanted subcutaneously into the hind limb of Balb/c mice and injected intravenously with 1.9 nm gold nanoparticles were irradiated 2 min later with 110 keV X-rays (produced at 250 KVp) by Hainfeld and others [12]. At gold concentration of 2.7 g/kg and 26 Gy dose complete tumor regression for 1 year was obtained for 86 % of mice compared to 20 % of mice given irradiation alone. In their more recent work, the same group of investigators used 11 nm gold nanoparticles administered intravenously at 4 g/kg to B6C3F1 mice bearing syngeneic orthotopic Tu-2449 brain tumors. Fifteen hours after nanoparticle administration, these mice were exposed to local 30 Gy (at 100 KVp) irradiation. A year after treatment 50 % of mice exposed to radiation in the presence of nanoparticles were still alive [13].
Among the nanomaterials that radiosensitize cells by potentiating the physicochemical effects of radiation is cerium oxide. Cerium oxide particles (5–8 nm) engage in different chemical reactions with different reactive oxygen species in a pH-dependent manner. At acidic pH, cerium oxide nanoparticles scavenge superoxide radical and produce hydrogen peroxide. At neutral pH values, cerium oxide nanoparticles scavenge H2O2 in a chemical reaction resembling the decomposition of hydrogen peroxide to water and oxygen mediated by catalase [62]. This pH-dependent behavior of cerium oxide leads to radioprotection of healthy tissues and cells living under “neutral pH” conditions, and confers radiosensitization of cancer cells that are characterized by an acidic intracellular milieu. This was shown not only with clonogenic assays in vitro, but also in vivo, using mice carrying orthotopic pancreatic tumor (human cell line L2.6pl) xenografts. While nanoparticles alone delivered intraperitonealy (IP) caused tumor volume reduction and apoptotic cell death as determined by TUNEL staining, administration of cerium oxide nanoparticles prior to ionizing radiation lead to increased tumor regression and enhanced apoptotic cell death [62]. As the production of ROS in acidic subcellular environment could lead to increased toxicity, one of the potentially interesting approaches to increase the usability of cerium oxide nanoparticles is to target them to acidic lysosomes by covering them with a negative surface charge [8].
Increased production of ROS and the subsequent increase of cell death monitored by in vitro assays were found both with gold nanoparticles and nanoparticles made of other materials. For example, lanthanide-doped titanium oxide nanoparticles increased radiation-induced cell death of several human cell lines [59]. Levels of radiosensitization differed from cell type to cell type (embryonal rhabdomyosarcoma cell lines RD, alveolar rhabdomyosarcoma RH30 and breast cancer cell line MCF7), suggesting that the cellular capacity for nanoparticle uptake as well the ability to cope with ROS burdens play very significant roles in any radiosensitization by means of nanomaterials. The same nanoparticle type (silica coated and rare earth doped TiO2 crystals 3–10 nm in size) was injected into tumors in vivo. Tumor-bearing mice were irradiated with 10 fractions of 2.5 Gy followed by 3 fractions of 2 Gy over the same period [60]. Hind limb xenograft tumors grown in SCID mice were human lung adenocarcinoma cell line A459; in the presence of nanoparticles (three injections of 50 ml of 1 mg/ml nanoparticles each) an additional twofold reduction of tumor volume upon radiation was found.
An interesting research direction with regard to rare earth elements and nanoparticle-based radiosensitization is the use of gadolinium-based nanoparticles [5, 36, 37]. These 2.9 nm particles consist of a polysiloxane core and gadolinium–DTPA chelates (with cyanine 5.5 added to allow optical imaging) and have been tested first in orthotopically implanted 9L gliosarcoma (9LGS) brain tumors in Fisher 344 rats. Following intravenous delivery these nanoconstructs had good renal excretion and could be used both for magnetic resonance imaging and radiosensitization [5]. The importance of timing between nanoparticle delivery and irradiation (delivered with a microbeam) was very noticeable in this study; a 5 min delay increased radiation damage to normal tissue and decreased overall survival of rats compared to radiation alone, while a 20 min delay lead to improved survival of animals compared to radiation alone. A recent study using the same type of nanoparticles in xenograft head and neck cancer models (subcutaneous implantation of human head and neck cancer cell line SQ20B into flank of nude mice) showed that intratumor injection of gadolinium nanoparticles followed immediately with 10 Gy dose of ionizing radiation had a synergistic effect on tumor size reduction [37]. In vitro experiments with the same cell line as well as FaDu and Cal33 head and neck carcinoma cell lines, demonstrated that the use of gadolinium nanoparticles was associated with an increase in nonreparable DNA DSBs and the shortening of G2/M arrest, leading to increased genomic instability, appearance of polyploid and then hypoploid cell populations and increased apoptosis.
It should also be noted that radiation itself can alter delivery of nanomaterials. For example, Joh et al. [19] found that exposure to ionizing radiation increases the permeability of the neovasculature for nanoparticles. When nude mice orthotopically inocculated with the human glioma cell line U251 received 20 Gy (focused through a 1.5 cm collimator of the small animal irradiator) prior to injection of 22 nm PEG-coated gold nanoparticles, increased extravasation and in-tumor deposition of nanoparticles occurred, suggesting that radiation can improve the passive tumor tissue targeting of nanoparticles [19]. Radiation induced a three-fold increase of enhanced permeability retention in irradiated versus nonirradiated tumors.
2 Modulation of Radiosensitivity by Hyperthermia
Modulation of temperature conditions in the body (especially increased tumor temperature) at the time of radiation treatment has been noted to be a potential radiosensitizer, as reviewed by Wust and others [65]. Though hyperthermia was used in the treatment of various diseases including cancer since ancient times, one of the first carefully recorded local applications of hyperthermia alone for cancer treatment was performed in 1898 by Swedish gynecologist Westermark, who treated cervical cancer by running hot water through an intracavitary spiral tube and noted an excellent clinical response in seven patients [41].
On a molecular and cellular level, temperatures of 40–45 °C trigger various cellular responses, including protein denaturation [22], alterations in the cytoskeleton and membrane [15] and cell death and permanent arrest [22]. Temperatures equal to or higher than the transition temperature of 42.5 °C are considered to be optimal for generating protein damage to cells, but these temperatures are difficult to achieve in vivo [14]. In combination with ionizing radiation, hyperthermia is particularly potent predominantly because the two have different targets, with radiation damaging DNA and hyperthermia damaging proteins. For example, temperatures near the transition temperature (42 °C) increase tumor vascular perfusion [15] leading to an increase in tumor oxygenation, which increases the efficiency of radiation as formulated by oxygen enhancement ratio (OER). Protein denaturation and aggregation in the nucleus caused by hyperthermia perturb DNA synthesis and repair [23]. Regardless of the precise molecular mechanisms, chemo- and radiosensitizing effects of hyperthermia are significant, and hyperthermia treatment is considered to be among the most potent radiosensitizers discovered to date. Furthermore, thermal radiosensitization appears to be most pronounced in cells that are hypoxic and those that are in S phase, i.e., in those cells that tend to be the most resistant to radiotherapy alone [15].
Magnetic nanoparticles in combination with magnetic field exposure can be used to induce a site-specific hyperthermia [70]. After localizing in a tumor, magnetic nanoparticles can be activated by an alternating magnetic field (AMF), causing a local increase in temperature. Such nanoconstructs can heat their immediate submicron environment through eddy currents (circular electric currents induced within conductors by a changing magnetic field), magnetic hysteresis, and Neel or Brownian relaxation (complex physical phenomena that depend on the size of the particles). There is also evidence of additive magnetic effects via electromagnetic coupling through nanoconstruct aggregation either extracellularly or in endosomes [21, 56, 70]. This is most likely caused by the increase in “aggregated size” of magnetic material. Deliberately designed magnetic nanoparticle assemblies, such as, e.g. magnetic nanoparticle–adenovirus assemblies, have an increased capacity for thermal ablation [70].
Three recent studies illustrate the promise for magnetic nanoparticles-dependent hyperthermia-induced radiosensitization. The first study involved nanoparticles with a hematite core and hydrodynamic diameter of 117 nm injected into syngeneic mouse breast cancer tumors implanted into hind limb of C3H/He mice. Tumors were first subjected to AMF at 169 kHz or microwave exposure and then to irradiation—15 Gy of 6 MeV electrons within 30 min of hyperthermia. While tumor volume tripling time after the best single treatment was 18.7–25 days, combination therapy showed a tumor tripling time of 42.6 days [9]. A more recent study by Lin and others used Mn0.5Zn0.5Fe2O4 nanoparticles coated with poly(ethyleneimine) to deliver gene therapy [28]. The DNA construct was a combination of a promoter region of radiation responsive early growth response protein 1 (Egr-1) and the “suicide gene complex” HSV-TK/GCV. Expression of herpes simplex virus thymidine kinase (HSV-TK) converts the prodrug ganciclovir (GCV) into GCV triphosphate, a DNA synthesis and cell cycle inhibitor. In a hepatoma xenograft model (HepG2 tumors in BALB/c nude mice) use of these nanoconstructs with induction of hyperthermia and combined with irradiation lead to tumor volume decrease greater than 90 %, two times better than radiotherapy alone [28].
The final study to be mentioned here is a phase II clinical trial using magnetic nanoparticles in 66 human patients, 59 with recurrent glioblastoma multiforme. Nanoparticles consisted of 12 nm magnetite with aminosilane coating, at iron concentration of 112 mg/ml, injected directly into tumors. Six one-hour long hyperthermia sessions (induced by AMF) were done semiweekly, with median tumor temperature of 52 °C. These sessions were immediately preceded or followed with stereotactic beam radiotherapy (SBRT) with a median dose 30 Gy, delivered as five 2 Gy fractions each week. The primary study endpoint was overall survival (OS) after recurrence—it reached 13.4 months, which is a significant improvement compared to, e.g. 6.2 months recoded in a metastudy on temozolomide as a salvage treatment [33].
It should be noted that hyperthermia has also been combined with radiation treatments with the aid of nanoconstructs with optical properties [1, 4]. Gold nanoshells, for example, have tunable optical resonance which allows them to be thermally activated by near infrared (NIR) light and be appropriate for thermal ablative therapy [16]. Such nanoconstructs, prepared with a silica core coated with gold, at the size of 150 nm have plasmon resonance for NIR wavelengths of 808 nm. This leads to intense NIR absorption and conversion to thermal energy. In one of the first examples of in vivo study with these constructs, nanoconstruct delivery to tumors depended only on enhanced permeability retention (EPR) [4], and the tumor model was a xenograft (human colorectal cell line HCT 116 in nude mice). In this setup, local hyperthermia (lasting 20 min) was induced by NIR laser illumination 24 h after IV injection of nanoconstructs. Hyperthermia was followed 5 min later by irradiation with 10 Gy. In comparison with irradiation alone, combination treatment doubled the time of the tumor growth delay. Similarly, in in vivo orthotopic models of breast cancer (syngeneic mouse breast cancer cells p53/from GEM transgenic mice in immunocompetent mice and primary human breast tumor xenografts in nude mice) Krishnan and collaborators achieved reduction in tumor size [1]. In this case, irradiation with 6 Gy was immediately followed with local hyperthermia (20 min at 42 °C), using a local NIR illumination of the tumor after an intravenous administration of gold nanoshells. A twofold decrease in tumorigenicity (measured as the number of cells with purported stem-like properties and as a number of cells forming colonies in cell culture) of cells isolated from these tumors at 48 h after treatment was statistically significant in comparison with cells isolated from ionizing radiation only treated tumors.
3 Modulation of Cellular Biochemistry and Biochemical Homeostasis by Nanomaterials
3.1 DNA Repair Modulation
The effect of nanoparticles on cells is largely modulated by their acquisition of a protein corona and the subsequent intracellular modification of such corona through interactions with intracellular proteins. For example, an in vitro study found that several different sizes of polyethylene glycol and tetraethylene glycol-coated iron oxide and titanium dioxide nanoparticles interact with proteasome [6] and alter its activity. Similarly, corona of silica nanoparticles was found to contain proteasomal subunits as well [31]. Considering that ubiquitin proteasome system regulates DNA synthesis and repair as well as countless other processes relevant for radiation-induced stress [35], it is possible that the rate of DNA repair in irradiated cells may be altered in the presence of such nanoparticles.
DNA repair can also be deliberately modified by nanoparticles with surface modifications designed to do so. In their recent publication Li and others modified 2 nm gold nanoparticles by the addition of weak SUMO (Small Ubiquitin-like Modifier)-2∕3 ligands, at a density of 100 per particle [27]. Through this approach, (because of high density of a weak ligand on the particle surface) nanoparticles became able to interact with multiple SUMO molecules in a poly-SUMO chain; inside cells these constructs could be found both in cytoplasm and nucleus. Because SUMOylation is a very important molecular modification pathway in the oxidative stress response, use of this type of nanoparticle, in comparison to same type of nanoparticles without SUMO ligand, led to an increase in radiation sensitivity in cancer cells in vitro as established by clonogenic assays. Comparisons between nanoparticles loaded with control scrambled molecules and nanoparticles loaded with SUMO interacting peptide demonstrated delayed DNA repair by comet assays in breast cancer MCF7 cells exposed to 4 Gy and incubated for 2 h.
Modulation of DNA repair with nanoparticles that release nucleic acid cargo is discussed in Sect. 4.
3.2 Nanoparticle Induced Cell Stress
Increased biocompatibility of PEG-coated gold nanoparticles compared to their “naked” counterparts (e.g. [42]) inspired the development of nanogel particles of about 100 nm in size, composed of a cross-linked poly(2-[N,N,-diethylamino]ethyl methacrylate) (PEAMA) core tethered with PEG and loaded with an average of 15 gold nanoparticles (8 nm in size) per each nanogel particle. The ability of these nanoconstructs to enhance radiation-induced tumor cell killing was investigated in several human and animal cell lines (human lung adenocarcinoma A549, Chinese hamster V79 and mouse squamous cell carcinoma SCCVII) [69]. Cells incubated for 14 h with nanogel particles (gold content in cell media varied between 20 and 50 μg/ml) were irradiated with doses between 2 and 15 Gy. Cell survival curves for each treatment were constructed; gold nanogel particles intensified cell killing by 1.2–1.5 fold across different irradiation doses. However, the initial DNA DSB damage in all cells depended only on the radiation dose, even though subsequently DNA DSB foci lasted longer in nanoparticle treated cells. Cellular uptake of nanogel particles as shown by TEM was associated with cytoplasmic vesicles. Starting with these findings, the authors investigated protein concentrations of critical DNA repair molecules (e.g. Rad51 and Ku70) and endoplasmic reticulum (ER) stress proteins (IRE1alpha, BiP, PERK, and calnexin) finding a reduction of the former and increase of the latter. In short, this study indicated that the 8 nm gold nanoparticles inside cells deregulate cellular homeostasis in ways that cause increased ER stress and decreased capacity for DNA damage repair [69]. Whether these changes are responsible for increased cell killing following ionizing radiation or not is not conclusive; nevertheless, the fact remains that the gold nanogels do act as radiosensitizers. It should be mentioned, however, that in another study (not including nanomaterials), Yamamori and others [68] found that ER stress is itself responsible for Rad51 degradation and general suppression of DNA DSB repair.
Cellular stress in many cases leads to cell death. Copper oxide, one of the most recent additions to the group of metal oxide nanoparticles, for example, was found to increase on its own both autophagy and apoptosis [26]. It is appealing, then, to speculate that CuO nanoparticles would have an additive or possibly even synergistic effect with ionizing radiation exposure. We can probably expect an increase in number of such studies in the future.
3.3 Cell Cycle
Using the prostate carcinoma cell line DU-145, Roa and others have documented changes in cell cycle distribution following treatment with ~10 nm gold nanoparticles coated with 6-deoxy-6-fluoro-1-thio-D-glucose [52]. As in most other studies, gold nanoparticles were found in cytoplasmic vesicles and it is difficult to decide which exact mechanism is responsible for cell cycle perturbation after nanoparticle treatment. Inhibition of glucose uptake by cytochalasin B and with it, inhibition of uptake of glucose-coated nanoparticles partially reversed the nanoparticle effects. Cell cycle perturbations were most noticeable in G2/M phase of cell cycle during which cells are the most radiation sensitive. It is, therefore, very possible that the increase in radiosensitivity noted in nanoparticle treated cells could be associated with cell cycle perturbations, especially when one considers that nanoparticles never came closer than 6 nm from the nuclear DNA.
Increased number of cells in G2/M phase of cell cycle was noted also in glioblastoma cells (SNB-19 and U87MG) in culture after treatment with titanium dioxide nanotubes [38]. Moreover, in this study it was noted that the DNA repair was reduced in glioblastoma cell lines after they engulfed TiO2 nanorods (approximately 10 nm in diameter and up to 500 nm long). As nanorods remained in vesicles inside the cytoplasm in these cells, actual mechanism(s) responsible for these changes in cellular homeostasis are as of yet unclear. Increased numbers and persistence of DNA DSBs indicated by gamma H2AX foci (specifically in nanorods treated and irradiated cells) described in this study is similar to findings of others with other types of nanomaterials (e.g. [19, 20, 43, 69]). Many possible avenues for speculations about decrease of DNA repair in this work can be envisioned. Interaction of these nanoconstructs with the proteasome, for example, is quite possible considering that TiO2 nanorods of 6 and 20 nm alter proteasomal activity [6], which, in turn, regulates DNA repair (e.g. [35]).
Perturbation of cell cycle by nanomaterials, however, does not always lead to increased numbers of cells in G2/M phase of the cell cycle. On the contrary, Mackey and El-Sayed used 30 and 15 nm gold nanoparticles (suitable for plasmon resonance and conjugated with nucleus targeting and cytoplasm-targeting peptides) in human oral squamous carcinoma cells (HSC-3) and found an accumulation of cells in the S phase with a depletion of cells in the G2/M phase [32]. These particles were not used for radiosenitization (where they could even have caused increased radioresistance); they have been tested in combination with 5-fluorouracil. Because this chemotherapeutic drug kills the cells in S phase most effectively (unlike ionizing radiation), drug and nanoparticle use had synergistic effects in this study.
4 Radiosensitization Through Modulation of Gene Expression by Nanomaterials
Polymeric nanoparticles were used as carriers for nucleic acids that can alter gene activity in cells; e.g. [74]. Ataxia-telangiectasia-mutated (ATM) protein is critical for DNA repair following ionizing radiation; inactivation of this gene increases radiation sensitivity, and a possible approach to achieve this goal is by delivering antisense oligonucleotides to cells using polymeric Poly(D,L-lactide-co-glycolide) (PLGA) nanoparticles. In mice, an initially spontaneously arising head and neck squamous cell carcinoma cell line SCCVII can be implanted into syngeneic C3H/HeJ mice and used as a model for human HNSCC. Such mice with tumors of about 200 mm3 were treated with anti ATM oligonucleotides encapsulated in PLGA particles of approximately 100 nm in diameter. The nanoparticles (2.5 mg/kg) were administered 24 h before and immediately preceding irradiation; three pairs of intratumoral nanoparticle injections were followed with three 2 Gy fractions over a period of 15 days. Animals were sacrificed 15 days after the treatments; tumor volumes were significantly reduced in mice treated with PLGA particles with anti-ATM oligonucleotides compared to mice treated with “mutated” oligonucleotide nanoparticles.
Another protein playing a significant role in radiation resistance is survivin, and plasmids encoding an antisurvivin siRNA have been used for the development of radiosensitizing nanoconstructs. Monodisperse 180–220 nm nanoparticles composed of human serum albumin loaded with siRNA plasmids were decorated for targeting with an antibody against heat shock protein 70. In two glioblastoma cell lines U87MG and LN229 these nanoconstructs lead to radiosensitization of 1.64 and 1.25, respectively; accompanied by survivin suppression and induction of survivin regulated caspases 3 and 7 [7].
A more broad approach to gene expression modulation was employed by investigators who delivered microRNAs with pleiotropic effects into tumors using nanomaterials as a delivery system. For example, miR200c is considered to be a negative regulator of cancer stem cell behavior and epithelial—mesenchymal transition, and cancer stem cells are considered to be more radiation resistant than their “non-stem” counterparts. Nanoconstucts were prepared with miR200c loaded into PEG—peptide (gelatinase substrate)—poly (ε-caprolactone) copolymer nanoparticles and given to several gastric adenocarcinoma cell lines. Nanoparticle treatment combined with radiation decreased numbers of “stem-like” cells in the different cell populations. A decrease of CD44 and increase of E-cadherin were noted in cells treated with nanoconstructs in combination with irradiation, as well as changes in expression of many other apoptosis relevant proteins. In short, miR200c loaded copolymer nanoparticles radiosensitized human gastric adenocarcinoma cell lines BGC823, SGC7901, and MKN45 with 1.13–1.25 sensitization enhancement ratio [3].
A similar study with antagomirs against miR21 used locked nucleic acid—lipid nanocapsules to radiosensitize U87MG glioblastoma cells in culture [10]. In cells treated with these nanoconstructs viability was suppressed and reduced to 50 % after 4 Gy irradiation.
5 Conclusions
Despite impressive in vitro successes, nanomaterials are still showing only moderately interesting results as radiosensitizers in vivo. One reason for this lies in the fact that delivery of nanomaterials must be specific enough that the radiosensitizing nanoparticles do not accumulate in healthy tissues that need to be protected from (and not sensitized to) irradiation (e.g. see [5]). Nevertheless, the radiosensitizing nanomaterials are not as limited by this requirement as are chemotherapy and other anticancer therapies. Because radiation is targeted to the cancer with very precise delivery and dosimetry approaches, if the radiosensitizers are outside the radiation field, they will not be effective. Hence, targeting the cancer specifically is not a firm requirement of radiosensitizers. Second, to be good radiosensitizers nanoparticles must reach most of the cells that need to be radiosensitized. Considering that the most radiation resistant cells in solid tumors are the ones most distant from blood supply, it is very probable that the same cells will also be the most difficult to reach with nanomaterials. In addition to often sparse neovascularization, interstitial pressure in tumors and accumulation of collagen also present significant barriers to nanoparticle distribution in tumors in vivo. Collagen density was found to be a critical feature limiting delivery of 40 nm carboxylate modified FluoroSpheres to hind limb tumors in SCID mice [58]. Interestingly, radiation itself may be leveraged against nanoparticle delivery problems. For example, focused radiation delivery can permeabilize brain tumor blood barrier and increase tumor deposition of pegylated nanoparticles (e.g. [19]). Thirdly, nanoparticle uptake comparisons between cells grown under normoxia (21 % oxygen) versus hypoxia (0.1 % oxygen) show significant differences. Uptake of the same nanoparticles (1.9 nm “Auravist”) by three different cell lines (DU145 prostate cancer, MDA-MB-231 breast cancer, and L132 lung epithelial cells) varied drastically under different oxygen conditions. These differences in uptake, combined with the importance of oxygen in production of reactive oxygen species, resulted in reduction of sensitizer enhancement ratio for Auravist from 1.41 for normoxia to 1.1 for hypoxia [17].
Finally, even if a nanoparticle formulation is found that is suitable for radiosensitization, general concerns regarding nanoparticle use may still prevent wide application of nanomaterials as radiosensitizers. Potential complications pertaining, e.g. to renal clearance of nanoparticles may obviate any potential benefits that would stem from radiosensitization. A recent review on renal clearance of nanomaterials [72], especially gold nanoparticles, suggests that both the size (currently “set” as less than 5.5 nm) and surface coating of nanoparticles dictates their elimination by kidneys. For example, while coating with PEG aids the nanoparticles to evade the cells of reticuloendothelial system (RES), it also prevents nanoparticle removal through kidneys regardless of their dimensions [72].
References
Atkinson RL, Zhang M, Diagaradjane P, Peddibhotla S, Contreras A, Hilsenbeck SG, Woodward WA, Krishnan S, Chang JC, Rosen JM (2010) Thermal enhancement with optically activated gold nanoshells sensitizes breast cancer stem cells to radiation therapy. Sci Trans Med 2:55ra79
Butterworth KT, McMahon SJ, Currell FJ, Prise KM (2012) Physical basis and biological mechanisms of gold nanoparticle radiosensitization. Nanoscale 4:4830–4838
Cui F, Liu Q, Li R, Shen J, Wu P, Yu L, Hu W, Wu F, Jiang C, Yue G et al (2014) Enhancement of radiotherapy efficacy by miR-200c-loaded gelatinase-stimuli PEG-Pep-PCL nanoparticles in gastric cancer cells. Int J Nanomed 13:2345–2358
Diagaradjane P, Shetty A, Wang JC, Elliott AM, Schwartz J, Shentu S, Park HC, Deorukhkar A, Stafford RJ, Cho SH et al (2008) Modulation of in vivo tumor radiation response via gold nanoshell-mediated vascular-focused hyperthermia: characterizing an integrated antihypoxic and localized vascular disrupting targeting strategy. Nano Lett 8:1492–1500
Le Duc G, Miladi I, Alric C, Mowat P, Bräuer-Krisch E, Bouchet A, Khalil E, Billotey C, Janier M, Lux F et al (2011) Toward an image-guided microbeam radiation therapy using gadolinium-based nanoparticles. ACS Nano 5:9566–9574
Falaschetti CA, Paunesku T, Kurepa J, Nanavati D, Chou SS, De M, Song M, Jang J-T, Wu A, Dravid VP et al (2013) Negatively charged metal oxide nanoparticles interact with the 20S proteasome and differentially modulate its biologic functional effects. ACS Nano 7:7759–7772
Gaca S, Reichert S, Multhoff G, Wacker M, Hehlgans S, Botzler C, Gehrmann M, Rödel C, Kreuter J, Rödel F (2013) Targeting by cmHsp70.1-antibody coated and survivin miRNA plasmid loaded nanoparticles to radiosensitize glioblastoma cells. J Control Release 172:201–206
Gao Y, Chen K, Ma J-L, Gao F (2014) Cerium oxide nanoparticles in cancer. Onco Targets Ther 7:835–840
Giustini AJ, Petryk AA, Hoopes PJ (2011) Comparison of microwave and magnetic nanoparticle hyperthermia radiosensitization in murine breast tumors. Proc SPIE 7901:1–11
Griveau A, Bejaud J, Anthiya S, Avril S, Autret D, Garcion E (2013) Silencing of miR-21 by locked nucleic acid-lipid nanocapsule complexes sensitize human glioblastoma cells to radiation-induced cell death. Int J Pharm 454:765–774
Guidelli EJ, Baffa O (2014) Influence of photon beam energy on the dose enhancement factor caused by gold and silver nanoparticles: An experimental approach. Med Phys 41:032101
Hainfeld JF, Slatkin DN, Smilowitz HM (2004) The use of gold nanoparticles to enhance radiotherapy in mice. Phys Med Biol 49:N309–N315
Hainfeld JF, Smilowitz HM, O’Connor MJ, Dilmanian FA, Slatkin DN (2013) Gold nanoparticle imaging and radiotherapy of brain tumors in mice. Nanomed (Lond) 8:1601–1609
Hall EJ, Giaccia AJ (2011) Radiobiology for the radiologist Lippincott Williams & Wilkins
Hildebrandt B, Wust P, Ahlers O, Dieing A, Sreenivasa G, Kerner T, Felix R, Riess H (2002) The cellular and molecular basis of hyperthermia. Crit Rev Oncol Hematol 43:33–56
Hirsch LR, Stafford RJ, Bankson JA, Sershen SR, Rivera B, Price RE, Hazle JD, Halas NJ, West JL (2003) Nanoshell-mediated near-infrared thermal therapy of tumors under magnetic resonance guidance. Proc Natl Acad Sci USA 100:13549–13554
Jain S, Coulter JA, Butterworth KT, Hounsell AR, McMahon SJ, Hyland WB, Muir MF, Dickson GR, Prise KM, Currell FJ et al (2014) Gold nanoparticle cellular uptake, toxicity and radiosensitisation in hypoxic conditions. Radiother Oncol 110:342–347
Jin C, Bai L, Wu H, Liu J, Guo G, Chen J (2008) Paclitaxel-loaded poly(D, L-lactide-co-glycolide) nanoparticles for radiotherapy in hypoxic human tumor cells in vitro. Cancer Biol Ther 7:911–916
Joh DY, Sun L, Stangl M, Al Zaki A, Murty S, Santoiemma PP, Davis JJ, Baumann BC, Alonso-Basanta M, Bhang D et al (2013) Selective targeting of brain tumors with gold nanoparticle-induced radiosensitization. PLoS ONE 8:e62425
Joh DY, Kao GD, Murty S, Stangl M, Sun L, Zaki AA, Xu X, Hahn SM, Tsourkas A, Dorsey JF (2013) Theranostic gold nanoparticles modified for durable systemic circulation effectively and safely enhance the radiation therapy of human sarcoma cells and tumors. Trans Oncol 6:722–IN32
Johannsen M, Thiesen B, Wust P, Jordan A (2010) Magnetic nanoparticle hyperthermia for prostate cancer. Int J Hyperth 26:790–795
Kampinga HH (2006) Cell biological effects of hyperthermia alone or combined with radiation or drugs: a short introduction to newcomers in the field. Int J Hyperth 22:191–196
Kampinga HH, Dikomey E (2001) Review: Hyperthermic radiosensitization: mode of action and clinical relevance. Int J Radiat Biol 77:399–408
Kleinauskas A, Rocha S, Sahu S, Sun Y-P, Juzenas P (2013) Carbon-core silver-shell nanodots as sensitizers for phototherapy and radiotherapy. Nanotechnology 24:325103
Van der Kogel A, Joiner M (2009) Basic clinical radiobiology. A Hodder Arnold Publication, London
Laha D, Pramanik A, Maity J, Mukherjee A, Pramanik P, Laskar A, Karmakar P (2014) Interplay between autophagy and apoptosis mediated by copper oxide nanoparticles in human breast cancer cells MCF7. Biochim Biophys Acta 1840:1–9
Li Y, Perkins A, Su Y, Ma Y, Colson L, Horne D, Chen Y (2012) Gold nanoparticles as a platform for creating a multivalent poly-SUMO chain inhibitor that also augments ionizing radiation. Proc Natl Acad Sci USA 109:4092–4097
Lin M, Huang J, Zhang J, Wang L, Xiao W, Yu H, Li Y, Li H, Yuan C, Hou X et al (2013) The therapeutic effect of PEI-Mn0.5Zn0.5Fe2O4 nanoparticles/pEgr1-HSV-TK/GCV associated with radiation and magnet-induced heating on hepatoma. Nanoscale 5:991–1000
Lin M-H, Hsu T-S, Yang P-M, Tsai M-Y, Perng T-P, Lin L-Y (2009) Comparison of organic and inorganic germanium compounds in cellular radiosensitivity and preparation of germanium nanoparticles as a radiosensitizer. Int J Radiat Biol 85:214–226
Lu R, Yang D, Cui D, Wang Z, Guo L (2012) Egg white-mediated green synthesis of silver nanoparticles with excellent biocompatibility and enhanced radiation effects on cancer cells. Int J Nanomed 7:2101–2107
Lundqvist M, Stigler J, Cedervall T, Berggård T, Flanagan MB, Lynch I, Elia G, Dawson K (2011) The evolution of the protein corona around nanoparticles: A test study. ACS Nano 5:7503–7509
Mackey MA, El-Sayed MA (2014) Chemosensitization of cancer cells via gold nanoparticle-induced cell cycle regulation. Photochem Photobiol 90:306–312
Maier-Hauff K, Ulrich F, Nestler D, Niehoff H, Wust P, Thiesen B, Orawa H, Budach V, Jordan A (2010) Efficacy and safety of intratumoral thermotherapy using magnetic iron-oxide nanoparticles combined with external beam radiotherapy on patients with recurrent glioblastoma multiforme. J Neurooncol 103:317–324
Matsudaira H, Ueno AM, Furuno I (1980) Iodine contrast medium sensitizes cultured mammalian cells to X-rays but not to gamma rays. Radiat Res 84:144–148
McBride WH, Iwamoto KS, Syljuasen R, Pervan M, Pajonk F (2003) The role of the ubiquitin/proteasome system in cellular responses to radiation. Oncogene 22:5755–5773
Miladi I, Duc G Le, Kryza D, Berniard A, Mowat P, Roux S, Taleb J, Bonazza P, Perriat P, Lux F et al (2013) Biodistribution of ultra small gadolinium-based nanoparticles as theranostic agent: application to brain tumors. J Biomater Appl 28:385–394
Miladi I, Aloy M-T, Armandy E, Mowat P, Kryza D, Magné N, Tillement O, Lux F, Billotey C, Janier M et al (2014) Combining ultrasmall gadolinium-based nanoparticles with photon irradiation overcomes radioresistance of head and neck squamous cell carcinoma. Nanomedicine 11:247–257
Mirjolet C, Papa AL, Créhange G, Raguin O, Seignez C, Paul C, Truc G, Maingon P, Millot N (2013) The radiosensitization effect of titanate nanotubes as a new tool in radiation therapy for glioblastoma: a proof-of-concept. Radiother Oncol 108:136–142
Misawa M, Takahashi J (2011) Generation of reactive oxygen species induced by gold nanoparticles under X-ray and UV Irradiations. Nanomedicine 7:604–614
Monopoli M, Åberg C, Salvati A, Dawson K (2012) Biomolecular coronas provide the biological identity of nanosized materials. Nat Nanotechnol 7:779–786
Moyer HR, Delman KA (2008) The role of hyperthermia in optimizing tumor response to regional therapy. Int J Hyperth 24:251–261
Naahidi S, Jafari M, Edalat F, Raymond K, Khademhosseini A, Chen P (2013) Biocompatibility of engineered nanoparticles for drug delivery. J Control Release 166:182–194
Ngwa W, Korideck H, Kassis AI, Kumar R, Sridhar S, Makrigiorgos GM, Cormack RA (2013) In vitro radiosensitization by gold nanoparticles during continuous low-dose-rate gamma irradiation with I-125 brachytherapy seeds. Nanomedicine 9:25–27
Ni J, Wu Q, Li Y, Guo Z, Tang G, Sun D, Gao F, Cai J (2007) Cytotoxic and radiosensitizing effects of nano-C60 on tumor cells in vitro. J Nanopart Res 10:643–651
Nikolić N, Vranjes-Ethurić S, Janković D, Ethokić D, Mirković M, Bibić N, Trajković V (2009) Preparation and biodistribution of radiolabeled fullerene C60 nanocrystals. Nanotechnology 20:385102
Olive PL, Banáth JP (2006) The comet assay: a method to measure DNA damage in individual cells. Nat Protoc 1:23–29
Patra HK, Turner APF (2014) The potential legacy of cancer nanotechnology: cellular selection. Trends Biotechnol 32:21–31
Polf JC, Bronk LF, Driessen WHP, Arap W, Pasqualini R, Gillin M (2011) Enhanced relative biological effectiveness of proton radiotherapy in tumor cells with internalized gold nanoparticles. Appl Phys Lett 98:193702
Porcel E, Liehn S, Remita H, Usami N, Kobayashi K, Furusawa Y, Le Sech C, Lacombe S (2010) Platinum nanoparticles: a promising material for future cancer therapy? Nanotechnology 21:85103
Porcel E, Li S, Usami N, Remita H, Furusawa Y, Kobayashi K, Sech C Le, Lacombe S (2012) Nano-Sensitization under gamma rays and fast ion radiation. J Phys: Conf Ser 373:012006
Rahman WN, Corde S, Yagi N, Abdul Aziz SA, Annabell N, Geso M (2014) Optimal energy for cell radiosensitivity enhancement by gold nanoparticles using synchrotron-based monoenergetic photon beams. Int J Nanomed 9:2459–2467
Roa W, Zhang X, Guo L, Shaw A, Hu X, Xiong Y, Gulavita S, Patel S, Sun X, Chen J et al (2009) Gold nanoparticle sensitize radiotherapy of prostate cancer cells by regulation of the cell cycle. Nanotechnology 375101:9 pp
Roots R, Okada S (1975) Estimation of life times and diffusion distances of radicals involved in X-Ray-induced DNA strand breaks or killing of mammalian cells. Radiat Res 64:306–320
Rothkamm K, Löbrich M (2003) Evidence for a lack of DNA double-strand break repair in human cells exposed to very low X-ray doses. Proc Natl Acad Sci USA 100:5057–5062
Stankov K, Borisev I, Kojic V, Rutoljski L, Bogdanovic G, Djordjevic A (2013) Modification of antioxidative and antiapoptotic genes expression in irradiated K562 cells upon fullerenol C60 (OH) 24 nanoparticle treatment. J Nanosci Nanotechnol 13:105–113
Stigliano RV, Shubitidze F, Kekalo K, Baker I, Giustini AJ, Hoopes PJ (2013) Understanding mNP hyperthermia for cancer treatment at the cellular scale. Proc SPIE 8584:85840E
Tishler RB, Schiff PB, Geard CR, Hall EJ (1992) Taxol: a novel radiation sensitizer. Int J Radiat Oncol Biol Phys 22:613–617
Torosean S, Flynn B, Axelsson J, Gunn J, Samkoe KS, Hasan T, Doyley MM, Pogue BW (2013) Nanoparticle uptake in tumors is mediated by the interplay of vascular and collagen density with interstitial pressure. Nanomedicine 9:151–158
Townley HE, Rapa E, Wakefield G, Dobson PJ (2012) Nanoparticle augmented radiation treatment decreases cancer cell proliferation. Nanomedicine 8:526–536
Townley HE, Kim J, Dobson PJ (2012) In vivo demonstration of enhanced radiotherapy using rare earth doped titania nanoparticles. Nanoscale 4:5043–5050
Vinchon-Petit S, Jarnet D, Paillard A, Benoit J-P, Garcion E, Menei P (2010) In vivo evaluation of intracellular drug-nanocarriers infused into intracranial tumours by convection-enhanced delivery: distribution and radiosensitisation efficacy. J Neurooncol 97:195–205
Wason MS, Colon J, Das S, Seal S, Turkson J, Zhao J, Baker CH (2013) Sensitization of pancreatic cancer cells to radiation by cerium oxide nanoparticle-induced ROS production. Nanomedicine 9:558–569
Werner M, Copp J, Karve S (2011) Folate-targeted polymeric nanoparticle formulation of docetaxel is an effective molecularly targeted radiosensitizer with efficacy dependent on the Timing of Radiotherapy. ACS 5:8990–8998
Wiedenmann N, Valdecanas D, Hunter N, Hyde S, Buchholz TA, Milas L, Mason KA (2007) 130 Nm albumin-bound paclitaxel enhances Tumor radiocurability and therapeutic gain. Clin Cancer Res 13:1868–1874
Wust P, Hildebrandt B, Sreenivasa G, Rau B, Gellermann J, Riess H, Felix R, Schlag PM (2002) Hyperthermia in combined treatment of cancer. Lancet Oncol 3:487–497
Xiao F, Zheng Y, Cloutier P, He Y, Hunting D, Sanche L (2011) On the role of low-energy electrons in the radiosensitization of DNA by gold nanoparticles. Nanotechnology 22, 465101:10 pp
Yallapu MM, Maher DM, Sundram V, Bell MC, Jaggi M, Chauhan SC (2010) Curcumin induces chemo/radio-sensitization in ovarian cancer cells and curcumin nanoparticles inhibit ovarian cancer cell growth. J Ovarian Res 3:11
Yamamori T, Meike S, Nagane M, Yasui H, Inanami O (2013) ER stress suppresses DNA double-strand break repair and sensitizes tumor cells to ionizing radiation by stimulating proteasomal degradation of Rad51. FEBS Lett 587:3348–3353
Yasui H, Takeuchi R, Nagane M, Meike S, Nakamura Y, Yamamori T, Ikenaka Y, Kon Y, Murotani H, Oishi M et al (2014) Radiosensitization of tumor cells through endoplasmic reticulum stress induced by PEGylated nanogel containing gold nanoparticles. Cancer Lett 347:151–158
Yoo D, Lee J-H, Shin T-H, Cheon J (2011) Theranostic magnetic nanoparticles. Acc Chem Res 44:863–874
Zhang X, Yang H, Gu K, Chen J, Rui M, Jiang G-L (2011) In vitro and in vivo study of a nanoliposomal cisplatin as a radiosensitizer. Int J Nanomed 6:437–444
Zhang X-D, Yang J, Song S-S, Long W, Chen J, Shen X, Wang H, Sun Y-M, Liu P-X, Fan S (2014) Passing through the renal clearance barrier: toward ultrasmall sizes with stable ligands for potential clinical applications. Int J Nanomed 9:2069–2072
Zheng Y, Cloutier P, Hunting DJ, Sanche L (2008) Radiosensitization by gold nanoparticles: comparison of DNA damage induced by low and high-energy electrons. J Biomed Nanotechnol 4:469–473
Zou J, Qiao X, Ye H, Zhang Y, Xian J, Zhao H, Liu S (2009) Inhibition of ataxia-telangiectasia mutated by antisense oligonucleotide nanoparticles induces radiosensitization of head and neck squamous-cell carcinoma in mice. Cancer Biother Radiopharm 24:339–346
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Paunesku, T., Gutiontov, S., Brown, K., Woloschak, G.E. (2015). Radiosensitization and Nanoparticles. In: Mirkin, C., Meade, T., Petrosko, S., Stegh, A. (eds) Nanotechnology-Based Precision Tools for the Detection and Treatment of Cancer. Cancer Treatment and Research, vol 166. Springer, Cham. https://doi.org/10.1007/978-3-319-16555-4_7
Download citation
DOI: https://doi.org/10.1007/978-3-319-16555-4_7
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-16554-7
Online ISBN: 978-3-319-16555-4
eBook Packages: MedicineMedicine (R0)