
Abstract
Age-related chronic inflammation is characterized as the unresolved low-grade inflammatory process underlying the ageing process and various age-related diseases. In this chapter, we review the age-related changes in the oxidative stress-sensitive pro-inflammatory NF-κB signaling pathways causally linked with chronic inflammation during ageing based on senoinflammation schema. We describe various age-related dysregulated pro- and anti-inflammatory cytokines, chemokines, and senescence-associated secretory phenotype (SASP), and alterations of inflammasome, specialized pro-resolving lipid mediators (SPM), and autophagy as major players in the chronic inflammatory intracellular signaling network. A better understanding of the molecular, cellular, and systemic mechanisms involved in chronic inflammation in the ageing process would provide further insights into the potential anti-inflammatory strategies.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
The chronic inflammatory response is an essential immune defense function that has evolved to promote survival under specific stressors. Acutely activated inflammation is the first line of defense against harmful agents such as pathogens, toxins, and allergens. Normal conditions enable the elimination of pathogens, infected cells, and damaged tissue for full recovery through the tightly coordinated actions of various defense components, including immune cell function and tissue remodeling processes (Freire and Van Dyke 2013).
When the acute inflammatory response does not subside, the immune system responds in a more complex, long-term manner. The chronic inflammatory response is usually low in intensity and involves many proinflammatory cellular components, including leukocytes enriched with macrophages and lymphocytes (Chen and Xu 2015). The ageing process and numerous age-related chronic diseases are characterized by chronic inflammation due to changes in the cellular redox state and cell death signaling pathways (Chung et al. 2006).
One of the well-known characteristics of age-related dysregulation of immune response is low-grade systemic inflammatory activity. Cytokines and chemokines are among the many dysregulated proinflammatory mediators that contribute to prolonged chronic inflammation and immunosenescence. According to previous studies, the expression of cytokines, such as interleukin-6 and tumor necrosis factor (TNF)-α, increases substantially in aged tissues (Chung et al. 2006; Franceschi et al. 2000). Several studies have linked high levels of chemokines, C-reactive protein (CRP), and prostanoid synthesis to age-related diseases and ageing development (Wyczalkowska-Tomasik et al. 2016). We have previously reported that several important intra- or intercellular signaling pathways are closely associated with chronic inflammation and age-related inflammatory changes in cellular status during ageing (Park et al. 2013; Kim et al. 2016).
In the literature on ageing, two major hypotheses exist regarding chronic inflammation associated with ageing: inflammageing (Franceschi et al. 2000) and senoinflammation (Chung et al. 2019). These two hypotheses are complementary, as the widely observed inflammatory phenomenon with ageing is the major point of the inflammageing hypothesis, whereas senoinflammation focuses on a broad spectrum of proinflammatory molecular, cellular, and systemic components that underlie the chronic inflammatory process. Importantly, recent research on chronic inflammation has produced more supportive experimental data for senoinflammatory hypothesis, necessitating an in-depth discussion of molecular, cellular, and systemic aspects of chronic inflammation, as described in this chapter.
Key Factors Influencing Chronic Inflammation in Ageing
Pro- and Anti-inflammatory Cytokines and SASP
Inflammation is an essential aspect of the body’s immune response and defense. An acute state of inflammation over a short period promotes immunity and protects the host in various ways (Chung et al. 2019). Because of its potentially adverse effects, inflammation is generally transient and tightly regulated. The development of chronic diseases, such as cancer, dementia, and atherosclerosis, is an inevitable consequence when inflammation is prolonged and unresolved, that is when it becomes chronically dysregulated immune system (Chung et al. 2019). Therefore, the disruption of the homeostatic inflammatory response is a significant risk factor for ageing process. The influence of the major mediators of chronic inflammation and immunosenescence, cytokines, and chemokines persists throughout this scenario. Chronic inflammation has a much more complex and intricate connection to ageing. M1-like macrophages have been found to release proinflammatory molecules such as TNFα, IL-1β, and IL-12 as a result of prolonged overeating and obesity, which have been linked to numerous metabolic disorders (Li et al. 2018). Additionally, PPARα and SREBP-1c have been implicated in lipid accumulation associated with proinflammatory IL-1β activation by inflammasomes (Chung et al. 2015). Moreover, chronic adipokine-mediated systemic inflammation is widely recognized to be exacerbated by chronic inflammation in adipose tissues (Bluher 2016).
Senescence-associated secretory phenotype (SASP) has recently proved to be a major proinflammatory contributor to numerous pathophysiological conditions (Wiley and Campisi 2021). Senescent cells secrete extracellular modulators such as cytokines, chemokines, proteases, growth factors, and bioactive lipids (Lopes-Paciencia et al. 2019). As a result, macrophages are activated to eliminate senescent cells that produce a senescence-associated (SA) secretome containing inflammatory senescence-associated protein. However, aged macrophages may not properly eliminate senescent cells, leading to a chronic inflammatory state (Oishi and Manabe 2016).
The secretion of inflammatory mediators such as cytokines and chemokines is dependent on the activation of redox-sensitive nuclear factor (NF-κB) (Chung et al. 2019). NF-κB is now regarded as one of the most important proinflammatory transcription factors. NF-κB signaling during ageing has been shown to involve cytokines (IL-1β, IL-2, and IL-6), chemokines (IL-8, RANTES, and T cells), and adhesion molecules, all of which contribute to chronic diseases and symptoms associated with ageing (Chung et al. 2006). Substantial evidence suggests that NF-κB plays an important role in cancer progression and initiation (Xia et al. 2014). Many other proinflammatory mediators are also induced by NF-κB stimulation, leading to major age-related chronic diseases (Wang et al. 2022; Esparza-Lopez et al. 2019).
NF-κB also interacts with various factors such as signal transduction factors and transcriptional activators 3 (STAT3) and p53. These factors are implicated in age-related chronic inflammatory diseases such as cancer and type 2 diabetes mellitus (Fan et al. 2013; Lowe et al. 2014). Crosstalk has been reported between upstream signaling components as well as at the transcriptional level. In addition to GSK3, MAPK, and protein kinase B (PKB), kinases that regulate NF-κB transcription can also regulate the activity of other cancer-related kinases (Park and Hong 2016). Numerous proinflammatory genes, metabolic signaling pathways, and SASP have been identified to be systemically involved in inflammatory and metabolic disorders (Wiley and Campisi 2021). A more detailed discussion on NF-κB is presented below.
Anti-inflammatory cytokines also play essential roles in balancing the immune response and preventing immune homeostasis from falling into proinflammatory ageing and disease-induced states. These cytokines play a key role in alleviating inflammation. By blocking or modulating IL-1α, TNF, and other major proinflammatory cytokines, they dampen and ultimately resolve the inflammation response. In addition to soluble receptor antagonists, chemokines, microRNAs, and siRNAs, specific cytokine receptors for IL-1, TNF-α, and IL-18 also inhibit proinflammatory cytokines (Rea et al. 2018). The anti-inflammatory cytokines interleukin 10 (IL-10) and IL-37, members of the IL-1 family, are crucial factors in controlling inflammation, along with TGF-β released by monocytes and platelets. Inflammatory pathways are reduced by the soluble receptors TNFR and IL-1 receptor (IL-1R), which bind to cytokines and neutralize them (Levine 2008). Many other anti-inflammatory mediators are observed, including stress hormones—primarily corticosteroids and catecholamines—and negative regulators such as microRNAs (MiR-146 and MiR-125) (Schulze et al. 2014; Lee et al. 2016). Previously reported observations clearly demonstrate that proinflammatory and anti-inflammatory cytokines and SASP modulate the outcome of chronic inflammation underlying the ageing process and age-related disease pathogenesis.
Changes in Endogenous Anti-inflammatory Lipid Mediators During Ageing
The complete resolution of an inflammatory response is essential for maintaining cellular homeostasis, and inflammation resolution is a highly sophisticated process that involves important anti-inflammatory mediators. Endogenous anti-inflammatory mediators, including lipoxins, resolvins, and protectins, play key roles in resolving inflammation (Basil and Levy 2016). These mediators are derived from lipid precursors and produced by the enzymatic activity of lipoxygenases. Among these mediators, lipoxins are the most well-characterized. Lipoxins and their epimers are bioactive autacoid metabolites of arachidonic acid that are produced by several cell types. Initially, two lipoxins were identified: lipoxin A4 (LXA4) and lipoxin B4 (LXB4), and further studies have identified epimers of these two lipoxins. In addition, other lipid mediators including resolvins and protectins were found to be derived from omega 3 fatty acids or other families of polyunsaturated fatty acids with functions and activities similar to those of lipoxins (Kohli and Levy 2009). Because of their specific role in inflammation resolution, these anti-inflammatory lipid mediators are often called specialized pro-resolving lipid mediators (SPMs). In addition to the chemical properties of SPMs, their physiological roles and mechanisms at the site of inflammation have been extensively studied during the last decade (Basil and Levy 2016).
Accumulating evidence suggests that changes in lipid mediators are age-related. Gangemi et al. (2005) first reported that ageing was associated with reduced LXA4 levels. They evaluated urinary arachidonic acid metabolites, including anti-inflammatory LXA4 and proinflammatory cysteinyl leukotrienes in volunteers aged 26 to over 100 years. A significant inverse correlation between age and LXA4 levels was found, suggesting that reduced LXA4 levels over the course of ageing may contribute to the development of disease. Another study conducted by Dunn et al. (2015) showed a similar reduction in LXA4 levels in the ageing brain. The same researchers assessed age-related changes in proinflammatory leukotriene B4 (LTB4) and pro-resolving LXA4 levels in the brain. Age-dependent increases in LTB4 levels and decreases in LXA4 levels have been detected during brain ageing. Furthermore, these changes were exacerbated in the 3xTG Alzheimer mouse model. Pamplona et al. (2021) showed interesting results in aged brains by showing that neurons and microglia are responsible for LXA4 production in the brain, and ageing reduces the brain and systemic LXA4 levels in mice. Also, LXA4 levels in cerebrospinal fluid decrease with age and dementia in humans.
Crucial Role of Oxidative Stress in Age-Related Chronic Inflammation
Among the several well-known hypotheses of ageing, the most widely accepted theory is that ageing is caused by oxidative stress (Yu 1996). The oxidative stress hypothesis explains the characteristic changes during ageing as a net effect of redox imbalances caused by the difference between oxidative stress and reactive antioxidant forces (Kim et al. 2002). This redox imbalance is likely due to an increase in ROS and reactive lipid aldehydes associated with a weakened antioxidant defense system. The main contributors to the redox imbalance caused by age-related oxidative stress are uncontrolled production of reactive species such as reactive oxygen species (ROS), reactive nitrogen species, and reactive lipid species, in conjunction with a weakened antioxidant defense capacity. A gradual increase in oxidative stress due to impaired redox regulation during ageing may affect gene transcription and signal transduction pathways.
A seminal finding in oxidative stress and inflammatory processes is the profound activation of NF-κB, a highly sensitive and critical proinflammatory mediator (Kim et al. 2002). By activating proinflammatory cells and expressing various cytokines and chemokines, NF-κB plays a crucial role in maintaining an immune response while ageing. According to motif mapping of gene promoters, NF-κB is the transcription factor most closely associated with ageing (Adler et al. 2007). Furthermore, chronic activation of NF-κB has been demonstrated in various tissues, such as the skin, kidneys, cardiac muscle, and brain (cerebellum and hypothalamus) (Helenius et al. 1996; Korhonen et al. 1997; Zhang et al. 2013; Tilstra et al. 2012).
Molecular and Cellular Constituents in Inflammation-Related Pathophysiological Conditions
NF-κB Involvement
The NF-κB signaling pathway is implicated in ageing, along with the insulin-like growth factor-1 (IGF-1), mTOR, SIRT, and p53 pathways. Several lines of evidence have shown that NF-κB activity increases with age. NF-κB/p65 DNA binding increased in the skin, liver, kidney, muscle, and gastric mucosa of aged mice. In addition, chronic NF-κB activation has been observed in various age-related diseases, including muscular atrophy, atherosclerosis, osteoporosis, heart diseases, type 1 and type 2 diabetes, osteoarthritis, and neurodegenerative diseases, such as Alzheimer’s disease and Parkinson’s disease (Chung et al. 2019).
Another line of evidence further demonstrated the tissue-specific role of NF-κB in ageing phenotypes. Cai et al. (2004) identified NF-κB activation through muscle-specific transgenic expression of activated IKK beta. These mice exhibited profound muscle wasting resembling clinical cachexia. Muscle loss occurred due to increased protein breakdown through E3 ligase MuRF1 expression, and pharmacological or genetic inhibition of the NF-κB pathway reversed muscle atrophy. Similar results were also obtained in the Duchenne muscular dystrophy model. Another study, by Zhang and colleagues, showed that IKK-NF-κB signaling is involved in the hypothalamic programming of systemic ageing (Zhang et al. 2013). They found ageing-dependent hypothalamic NF-κB activation with an increase in the innate immune pathway. NF-κB inhibition in genetically engineered mice increased lifespan with a less age-related phenotype, suggesting that hypothalamus NF-κB activation has a unique role in the development of systemic ageing. They further showed that activation of NF-κB mediates gonadotropin-releasing hormone (GnRH) decline in the aged hypothalamus, and GnRH treatment adjusts ageing-impaired neurogenesis and decelerates ageing.
Inflammasome in Chronic Inflammation
Recent studies have revealed that NACHT, LRR, and PYD domain-containing protein 3 (NLRP3) inflammasome are major regulators of age-related inflammation (Gritsenko et al. 2020). The inflammasome is activated by a wide range of extra and intracellular stimuli include pathogen-associated molecular patterns and danger-associated molecular patterns (Broz and Dixit 2016). Activation of NLRP3 proteins further oligomerizes and recruits an adaptor protein known as ASC, which consists of two death-fold domains, a pyrin domain (PYD) and a caspase recruitment domain (CARD). These domains allow ASC to bridge the upstream inflammasome sensor molecule with caspase 1. Activated caspase 1 further facilitates the release of interleukin-1β (IL-1β) and IL-18 and induces inflammation and pyroptosis, which is a lytic form of cell death. Inflammasome activation plays a crucial role in host defense against pathogens; however, dysregulated inflammasomes are also linked to the development of numerous age-related diseases.
Experimental data clearly demonstrated the role of inflammasome in ageing-associated phenotypic changes. Youm et al. (2013) utilized Nlrp3 deficient mice to observe age-related functional changes. NLRP3 inflammasome-deficient mice were protected from age-related increases in innate immune activation, alterations in CNS transcriptomes, and astrogliosis. They further demonstrated that increased IL-1 expression plays an essential role in regulating age-related CNS inflammation and functional decline. They also demonstrated that the NLRP3 inflammasome promotes ageing-related thymic demise and immunosenescence. Another study, by Camell et al. (2019), revealed the role of the NLRP3-inflammasome in age-related adipose tissue B-cell expansion. They identified unique resident aged adipose B cells that impair the basal role of adipose tissue during ageing. The accumulation of unique B cells and age-induced defects in lipolysis are dependent on the NLRP3 inflammasome and IL-1 signaling. The acetylation status of NLRP3 during ageing was reported by He et al. (2020). These authors showed that NLRP3 is deacetylated during the ageing process owing to decreased SIRT2 expression in macrophages. Deacetylated NLRP3 facilitates hyperactivation of the NLRP3 inflammasome, increasing inflammation during ageing. They provided evidence that the acetylation switch of the inflammasome, regulated by SIRT2, is a physiological factor that regulates age-associated chronic inflammation.
Role of Autophagy in Inflammation
Autophagy is an evolutionarily conserved process that occurs in all eukaryotic cells from yeast to humans. The highly complex autophagy machinery and related signaling pathways have been extensively studied over the last 30 years. The primary function of autophagy is to degrade self-components; once activated, autophagy involves the sequestration of cytosolic components, including damaged cell organelles, proteins, or other macromolecule nutrients, and provides energy to maintain cell homeostasis. In ageing and age-related diseases, there are significant reductions in these processes that lead to the accumulation of damaged molecules, proteins, DNA, and lipids, leading to the loss of cellular integrity, as defective autophagy has been implicated in various age-associated diseases (Aman et al. 2021).
Understanding the relationship between autophagy and inflammation provides insights into ageing and age-related diseases. Reviewing studies that use animal models and human samples support the important role of autophagy in maintaining tissue homeostasis through inflammation suppression. Impaired autophagy often results in increased inflammation and has been demonstrated as a major driver of age-related tissue damage using evidence obtained from studies on the role of autophagy in modulating the differentiation and metabolic state of inflammatory cells (Aman et al. 2021). It has been shown that immune cell differentiation is dependent on the balance between mTOR and AMPK signaling activation (Riffelmacher et al. 2018). When mTOR is activated, autophagic flux decreases and the cells exhibit proinflammatory phenotypes. In contrast, shifting the balance toward AMPK signaling results in increased autophagic activity with differentiation into non- or anti-inflammatory immune cells. Because overall autophagy responses decrease during ageing, this may be an important mechanism for promoting proinflammatory responses during ageing (Aman et al. 2021).
Senoinflammation Schema: Exacerbation by SASP and Suppression by Calorie Restriction (CR)
Previous literature has extensively shown the role of low-grade inflammation in ageing and age-related diseases. To clarify distinctions among widely used explanations and concepts, a number of terms and perspectives have been proposed. Chronic inflammation associated with ageing has been suggested to occur through a variety of mechanisms, including molecular inflammation, micro-inflammation, pan-inflammation, and gero-inflammation, which describe the actions of chronic inflammation and proinflammatory mediators (Fulop et al. 2017; Chhetri et al. 2018). Despite these attempts, the precise age-related chronic inflammatory processes remain poorly understood and under-characterized.
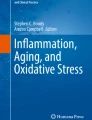
The senoinflammation (senescent chronic inflammation) schema presented herein (see Fig. 3.1) was developed in 2019, based on available data showing the initiation of the chronic inflammatory process triggered by oxidative stress-induced redox imbalance, which is associated with ageing and numerous chronic diseases (Chung et al. 2019). By understanding molecular, cellular, and systemic senoinflammation, one could gain a better understanding of how chronic inflammation exacerbates the age-related functional declines and metabolic alterations that occur.

Chronic inflammation as an underlying mechanism of ageing and ageing-related diseases. CR: calorie restriction, SPM: specialized pro-resolving lipid mediators, SASP: senescence-associated secretory phenotype
As described earlier, senescent cells secrete soluble mediators called SASP (Coppe et al. 2010). Recent studies have shown that SASP is a significant pathophysiological risk factor exacerbating the ageing process and metabolic diseases (Chung et al. 2019). The SASP plays a multifaceted role as an active mediator in the senoinflammatory process and metabolic changes associated with ageing (Shakeri et al. 2018). Despite considerable progress in understanding the cellular mechanisms of the SASP, its precise role and contribution to ageing and proinflammatory molecular pathways require further exploration. Reports have shown that senolysis (i.e., senescent cell removal) improves glucose metabolism and β-cell function while reducing SASP and senescent biomarker expression in mice (Aguayo-Mazzucato et al. 2019).
Senescence-associated secretory proinflammatory mediators and SASP are released by senescent cells (Salminen et al. 2012). To remove senescent cells from the secretome, macrophages are recruited by chemotactic factors (Childs et al. 2017). However, the polarized M2 phenotype of senescent macrophages secretes proinflammatory cytokines, exhibits impaired phagocytosis, and is characterized by lower growth rates (Yarbro et al. 2020). In keratinocytes, melanocytes, monocytes, fibroblasts, and epithelial cells, IL-1β, IL-6, and IL-8 are the most potent proinflammatory cytokines secreted by SA-induced stress (Freund et al. 2010). Most senescent cells contain elevated levels of matrix metalloproteases (MMPs), another proinflammatory component of SASP. MMPs regulate the production of cytokines and chemokines that are associated with inflammation (Coppe et al. 2010). Several recent studies have reported that PTBP1 and HSP90 regulate the SASP (Georgilis et al. 2018; Fuhrmann-Stroissnigg et al. 2018). In summary, SASP and related mediators impose a substantial impact on senoinflamatory process with ageing.
Caloric restriction (CR) has been demonstrated to be effective in combating the ageing process and age-related diseases such as diabetes, obesity, cardiovascular disease, rheumatoid arthritis, and Alzheimer’s disease (Chung et al. 2013). It is the only known intervention of ageing that extends not only the mean lifespan but also the maximum life span of experimental animals. Our lab reported the first experimental evidence showing CR’s potent and broad anti-inflammatory action by suppressing key proinflammatory NF-κB activation (Kim et al. 2002). Recent work also showed CR’s powerful modulation of many proinflammatory factors, including IL-1β, IL-6, TNF, and COX-2 (inducible nitric oxide synthase) (Allen et al. 2019). After two monthly applications of 30% CR to obese mice, cytokines, and chemokines such as IL-6, IL-2, IL1Rα, MCP-1, and CXCL16, which are important components of the SASP (Kurki et al. 2012). The expression of proinflammatory and lipogenic genes, such as MCP-1, SREBPs, and peroxisome proliferator-activated receptor (PPAR)-γ, was significantly suppressed by even mild CR in liver tissue (Park et al. 2017). As a result, CR has been shown to regulate the symptomatic prevalence of senoinflammation, which progresses to pathological conditions such as chronic inflammation, insulin resistance, and low energy metabolism resulting from chronic inflammation (Chung et al. 2019; Johansson et al. 2019).
Researchers have studied the effects of CR on inflammatory and metabolic signaling pathways as well as the relationship between ageing and CR. According to evidence from previous studies, CR modulates nuclear signaling pathways by regulating NF-κB, SIRT, and other nuclear molecules, which results in reduced senoinflammation during ageing. Such evidence strongly supports the notion that CR’s unique anti-ageing action may be based on its diversified anti-inflammatory capability.
Conclusion
Considering the available evidence and data on age-related chronic inflammation through biochemical, molecular, and systems biology analyses, we concluded that chronic inflammation is a major factor underlying ageing and age-related disease processes. The proinflammatory cytokines and chemokines that comprise the SASP increase stress on the intracellular signaling network, tissues, organs, and systems, leading to various metabolic disorders and chronic inflammation. Alterations in inflammasome, SPM, and autophagy trigger chronic inflammation, thus leading to accelerated ageing and age-related chronic diseases. Therefore, a better understanding of the molecular mechanisms involved in chronic inflammation may provide a fundamental platform for developing effective interventions that delay ageing-related dysfunction and prevent age-related proinflammatory, i.e., senoinflammatory diseases.
References
Adler AS, Sinha S, Kawahara TL, Zhang JY, Segal E, Chang HY (2007) Motif module map reveals enforcement of ageing by continual NF-kappaB activity. Genes Dev 21(24):3244–3257. https://doi.org/10.1101/gad.1588507
Aguayo-Mazzucato C, Andle J, Lee TB Jr, Midha A, Talemal L, Chipashvili V et al (2019) Acceleration of beta cell ageing determines diabetes and senolysis improve disease outcomes. Cell Metab 30(1):129–142 e4. https://doi.org/10.1016/j.cmet.2019.05.006
Allen BD, Liao CY, Shu J, Muglia LJ, Majzoub JA, Diaz V et al (2019) Hyperadrenocorticism of calorie restriction contributes to its anti-inflammatory action in mice. Ageing Cell 18(3):e12944. https://doi.org/10.1111/acel.12944
Aman Y, Schmauck-Medina T, Hansen M, Morimoto RI, Simon AK, Bjedov I et al (2021) Autophagy in healthy ageing and disease. Nat Ageing 1(8):634–650. https://doi.org/10.1038/s43587-021-00098-4
Basil MC, Levy BD (2016) Specialized pro-resolving mediators: endogenous regulators of infection and inflammation. Nat Rev Immunol 16(1):51–67. https://doi.org/10.1038/nri.2015.4
Bluher M (2016) Adipose tissue inflammation: a cause or consequence of obesity-related insulin resistance? Clin Sci (Lond) 130(18):1603–1614. https://doi.org/10.1042/CS20160005
Broz P, Dixit VM (2016) Inflammasomes: mechanism of assembly, regulation, and signaling. Nat Rev Immunol 16(7):407–420. https://doi.org/10.1038/nri.2016.58
Cai D, Frantz JD, Tawa NE Jr, Melendez PA, Oh BC, Lidov HG et al (2004) IKKbeta/NF-kappaB activation causes severe muscle wasting in mice. Cell 119(2):285–298. https://doi.org/10.1016/j.cell.2004.09.027
Camell CD, Gunther P, Lee A, Goldberg EL, Spadaro O, Youm YH et al (2019) Ageing induces an Nlrp3 inflammasome-dependent expansion of adipose B cells that impairs metabolic homeostasis. Cell Metab 30(6):1024–1039 e6. https://doi.org/10.1016/j.cmet.2019.10.006
Chen M, Xu H (2015) Parainflammation, chronic inflammation, and age-related macular degeneration. J Leukoc Biol 98(5):713–725. https://doi.org/10.1189/jlb.3RI0615-239R
Chhetri JK, de Souto Barreto P, Fougere B, Rolland Y, Vellas B, Cesari M (2018) Chronic inflammation and sarcopenia: a regenerative cell therapy perspective. Exp Gerontol 103:115–123. https://doi.org/10.1016/j.exger.2017.12.023
Childs BG, Gluscevic M, Baker DJ, Laberge RM, Marquess D, Dananberg J et al (2017) Senescent cells: an emerging target for diseases of ageing. Nat Rev Drug Discov 16(10):718–735. https://doi.org/10.1038/nrd.2017.116
Chung HY, Sung B, Jung KJ, Zou Y, Yu BP (2006) The molecular inflammatory process in ageing. Antioxid Redox Signal 8(3-4):572–581. https://doi.org/10.1089/ars.2006.8.572
Chung KW, Kim DH, Park MH, Choi YJ, Kim ND, Lee J et al (2013) Recent advances in calorie restriction research on ageing. Exp Gerontol 48(10):1049–1053. https://doi.org/10.1016/j.exger.2012.11.007
Chung KW, Lee EK, Kim DH, An HJ, Kim ND, Im DS et al (2015) Age-related sensitivity to endotoxin-induced liver inflammation: implication of inflammasome/IL-1beta for steatohepatitis. Ageing Cell 14(4):524–533. https://doi.org/10.1111/acel.12305
Chung HY, Kim DH, Lee EK, Chung KW, Chung S, Lee B et al (2019) Redefining chronic inflammation in ageing and age-related diseases: proposal of the senoinflammation concept. Ageing Dis 10(2):367–382. https://doi.org/10.14336/AD.2018.0324
Coppe JP, Desprez PY, Krtolica A, Campisi J (2010) The senescence-associated secretory phenotype: the dark side of tumor suppression. Annu Rev Pathol 5:99–118. https://doi.org/10.1146/annurev-pathol-121808-102144
Dunn HC, Ager RR, Baglietto-Vargas D, Cheng D, Kitazawa M, Cribbs DH et al (2015) Restoration of lipoxin A4 signaling reduces Alzheimer’s disease-like pathology in the 3xTg-AD mouse model. J Alzheimers Dis 43(3):893–903. https://doi.org/10.3233/JAD-141335
Esparza-Lopez J, Alvarado-Munoz JF, Escobar-Arriaga E, Ulloa-Aguirre A, de Jesus Ibarra-Sanchez M (2019) Metformin reverses mesenchymal phenotype of primary breast cancer cells through STAT3/NF-kappaB pathways. BMC Cancer 19(1):728. https://doi.org/10.1186/s12885-019-5945-1
Fan Y, Mao R, Yang J (2013) NF-kappaB and STAT3 signaling pathways collaboratively link inflammation to cancer. Protein Cell 4(3):176–185. https://doi.org/10.1007/s13238-013-2084-3
Franceschi C, Bonafe M, Valensin S, Olivieri F, De Luca M, Ottaviani E et al (2000) Inflamm-ageing. An evolutionary perspective on immunosenescence. Ann N Y Acad Sci 908:244–254. https://doi.org/10.1111/j.1749-6632.2000.tb06651.x
Freire MO, Van Dyke TE (2013) Natural resolution of inflammation. Periodontol 2000 63(1):149–164. https://doi.org/10.1111/prd.12034
Freund A, Orjalo AV, Desprez PY, Campisi J (2010) Inflammatory networks during cellular senescence: causes and consequences. Trends Mol Med 16(5):238–246. https://doi.org/10.1016/j.molmed.2010.03.003
Fuhrmann-Stroissnigg H, Niedernhofer LJ, Robbins PD (2018) Hsp90 inhibitors as senolytic drugs to extend healthy ageing. Cell Cycle 17(9):1048–1055. https://doi.org/10.1080/15384101.2018.1475828
Fulop T, Larbi A, Dupuis G, Le Page A, Frost EH, Cohen AA et al (2017) Immunosenescence and inflamm-ageing as two sides of the same coin: friends or foes? Front Immunol 8:1960. https://doi.org/10.3389/fimmu.2017.01960
Gangemi S, Pescara L, D’Urbano E, Basile G, Nicita-Mauro V, Davi G et al (2005) Ageing is characterized by a profound reduction in anti-inflammatory lipoxin A4 levels. Exp Gerontol 40(7):612–614. https://doi.org/10.1016/j.exger.2005.04.004
Georgilis A, Klotz S, Hanley CJ, Herranz N, Weirich B, Morancho B et al (2018) PTBP1-mediated alternative splicing regulates the inflammatory secretome and the pro-tumorigenic effects of senescent cells. Cancer Cell 34(1):85–102 e9. https://doi.org/10.1016/j.ccell.2018.06.007
Gritsenko A, Green JP, Brough D, Lopez-Castejon G (2020) Mechanisms of NLRP3 priming in inflammageing and age-related diseases. Cytokine Growth Factor Rev 55:15–25. https://doi.org/10.1016/j.cytogfr.2020.08.003
He M, Chiang HH, Luo H, Zheng Z, Qiao Q, Wang L et al (2020) An acetylation switch of the NLRP3 inflammasome regulates ageing-associated chronic inflammation and insulin resistance. Cell Metab 31(3):580–591 e5. https://doi.org/10.1016/j.cmet.2020.01.009
Helenius M, Hanninen M, Lehtinen SK, Salminen A (1996) Changes associated with ageing and replicative senescence in the regulation of transcription factor nuclear factor-kappa B. Biochem J 318(Pt 2):603–608. https://doi.org/10.1042/bj3180603
Johansson HE, Edholm D, Kullberg J, Rosqvist F, Rudling M, Straniero S et al (2019) Energy restriction in obese women suggests a linear reduction of hepatic fat content and time-dependent metabolic improvements. Nutr Diabetes 9(1):34. https://doi.org/10.1038/s41387-019-0100-2
Kim HJ, Jung KJ, Yu BP, Cho CG, Choi JS, Chung HY (2002) Modulation of redox-sensitive transcription factors by calorie restriction during ageing. Mech Ageing Dev 123(12):1589–1595. https://doi.org/10.1016/s0047-6374(02)00094-5
Kim CH, Lee EK, Choi YJ, An HJ, Jeong HO, Park D et al (2016) Short-term calorie restriction ameliorates genomewide, age-related alterations in DNA methylation. Ageing Cell 15(6):1074–1081. https://doi.org/10.1111/acel.12513
Kohli P, Levy BD (2009) Resolvins and protectins: mediating solutions to inflammation. Br J Pharmacol 158(4):960–971. https://doi.org/10.1111/j.1476-5381.2009.00290.x
Korhonen P, Helenius M, Salminen A (1997) Age-related changes in the regulation of transcription factor NF-kappa B in rat brain. Neurosci Lett 225(1):61–64. https://doi.org/10.1016/s0304-3940(97)00190-0
Kurki E, Shi J, Martonen E, Finckenberg P, Mervaala E (2012) Distinct effects of calorie restriction on adipose tissue cytokine and angiogenesis profiles in obese and lean mice. Nutr Metab (Lond) 9(1):64. https://doi.org/10.1186/1743-7075-9-64
Lee HM, Kim TS, Jo EK (2016) MiR-146 and miR-125 in the regulation of innate immunity and inflammation. BMB Rep 49(6):311–318. https://doi.org/10.5483/bmbrep.2016.49.6.056
Levine SJ (2008) Molecular mechanisms of soluble cytokine receptor generation. J Biol Chem 283(21):14177–14181. https://doi.org/10.1074/jbc.R700052200
Li C, Xu MM, Wang K, Adler AJ, Vella AT, Zhou B (2018) Macrophage polarization and meta-inflammation. Transl Res 191:29–44. https://doi.org/10.1016/j.trsl.2017.10.004
Lopes-Paciencia S, Saint-Germain E, Rowell MC, Ruiz AF, Kalegari P, Ferbeyre G (2019) The senescence-associated secretory phenotype and its regulation. Cytokine 117:15–22. https://doi.org/10.1016/j.cyto.2019.01.013
Lowe JM, Menendez D, Bushel PR, Shatz M, Kirk EL, Troester MA et al (2014) p53 and NF-kappaB coregulate proinflammatory gene responses in human macrophages. Cancer Res 74(8):2182–2192. https://doi.org/10.1158/0008-5472.CAN-13-1070
Oishi Y, Manabe I (2016) Macrophages in age-related chronic inflammatory diseases. NPJ Ageing Mech Dis 2:16018. https://doi.org/10.1038/npjamd.2016.18
Pamplona FA, Vitória G, Ribeiro FC, Moraes CA, Ledur PF, Karmirian K et al (2021) Age-linked suppression of lipoxin A4 mediates cognitive deficits in mice and humans. bioRxiv, 2021.11.12.468379. https://doi.org/10.1101/2021.11.12.468379
Park MH, Hong JT (2016) Roles of NF-kappaB in cancer and inflammatory diseases and their therapeutic approaches. Cells 5(2). https://doi.org/10.3390/cells5020015
Park D, Lee EK, Jang EJ, Jeong HO, Kim BC, Ha YM et al (2013) Identification of the dichotomous role of age-related LCK in calorie restriction revealed by integrative analysis of cDNA microarray and interactome. Age (Dordr) 35(4):1045–1060. https://doi.org/10.1007/s11357-012-9426-6
Park CY, Park S, Kim MS, Kim HK, Han SN (2017) Effects of mild calorie restriction on lipid metabolism and inflammation in liver and adipose tissue. Biochem Biophys Res Commun 490(3):636–642. https://doi.org/10.1016/j.bbrc.2017.06.090
Rea IM, Gibson DS, McGilligan V, McNerlan SE, Alexander HD, Ross OA (2018) Age and age-related diseases: role of inflammation triggers and cytokines. Front Immunol 9:586. https://doi.org/10.3389/fimmu.2018.00586
Riffelmacher T, Richter FC, Simon AK (2018) Autophagy dictates metabolism and differentiation of inflammatory immune cells. Autophagy 14(2):199–206. https://doi.org/10.1080/15548627.2017.1362525
Salminen A, Kauppinen A, Kaarniranta K (2012) Emerging role of NF-kappaB signaling in the induction of senescence-associated secretory phenotype (SASP). Cell Signal 24(4):835–845. https://doi.org/10.1016/j.cellsig.2011.12.006
Schulze J, Vogelgesang A, Dressel A (2014) Catecholamines, steroids and immune alterations in ischemic stroke and other acute diseases. Ageing Dis 5(5):327–339. https://doi.org/10.14336/AD.2014.0500327
Shakeri H, Lemmens K, Gevaert AB, De Meyer GRY, Segers VFM (2018) Cellular senescence links ageing and diabetes in cardiovascular disease. Am J Physiol Heart Circ Physiol 315(3):H448–H462. https://doi.org/10.1152/ajpheart.00287.2018
Tilstra JS, Robinson AR, Wang J, Gregg SQ, Clauson CL, Reay DP et al (2012) NF-kappaB inhibition delays DNA damage-induced senescence and ageing in mice. J Clin Invest 122(7):2601–2612. https://doi.org/10.1172/JCI45785
Wang C, Zhou Z, Song W, Cai Z, Ding Z, Chen D et al (2022) Inhibition of IKKbeta/NF-kappaB signaling facilitates tendinopathy healing by rejuvenating inflammageing induced tendon-derived stem/progenitor cell senescence. Mol Ther Nucleic Acids 27:562–576. https://doi.org/10.1016/j.omtn.2021.12.026
Wiley CD, Campisi J (2021) The metabolic roots of senescence: mechanisms and opportunities for intervention. Nat Metab 3(10):1290–1301. https://doi.org/10.1038/s42255-021-00483-8
Wyczalkowska-Tomasik A, Czarkowska-Paczek B, Zielenkiewicz M, Paczek L (2016) Inflammatory markers change with age, but do not fall beyond reported normal ranges. Arch Immunol Ther Exp (Warsz) 64(3):249–254. https://doi.org/10.1007/s00005-015-0357-7
Xia Y, Shen S, Verma IM (2014) NF-kappaB, an active player in human cancers. Cancer Immunol Res 2(9):823–830. https://doi.org/10.1158/2326-6066.CIR-14-0112
Yarbro JR, Emmons RS, Pence BD (2020) Macrophage immunometabolism and inflammageing: roles of mitochondrial dysfunction, cellular senescence, CD38, and NAD. Immunometabolism 2(3):e200026. https://doi.org/10.20900/immunometab20200026
Youm YH, Grant RW, McCabe LR, Albarado DC, Nguyen KY, Ravussin A et al (2013) Canonical Nlrp3 inflammasome links systemic low-grade inflammation to functional decline in ageing. Cell Metab 18(4):519–532. https://doi.org/10.1016/j.cmet.2013.09.010
Yu BP (1996) Ageing and oxidative stress: modulation by dietary restriction. Free Radic Biol Med 21(5):651–668. https://doi.org/10.1016/0891-5849(96)00162-1
Zhang G, Li J, Purkayastha S, Tang Y, Zhang H, Yin Y et al (2013) Hypothalamic programming of systemic ageing involving IKK-beta, NF-kappaB and GnRH. Nature 497(7448):211–216. https://doi.org/10.1038/nature12143
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Chung, K.W., Kim, D.H., Jung, H.J., Arulkumar, R., Chung, H.Y., Yu, B.P. (2023). Chronic Inflammation as an Underlying Mechanism of Ageing and Ageing-Related Diseases. In: Harris, J.R., Korolchuk, V.I. (eds) Biochemistry and Cell Biology of Ageing: Part IV, Clinical Science. Subcellular Biochemistry, vol 103. Springer, Cham. https://doi.org/10.1007/978-3-031-26576-1_3
Download citation
DOI: https://doi.org/10.1007/978-3-031-26576-1_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-26575-4
Online ISBN: 978-3-031-26576-1
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)