
Abstract
Oxygen is directly involved in many key pathophysiological processes. Oxygen deficiency, also known as hypoxia, could have adverse effects on mammalian cells, with ischemia in vital tissues being the most significant (Michiels C. Physiological and pathological responses to hypoxia. Am J Pathol 164(6): 1875–1882, 2004); therefore, timely adaptive responses to variations in oxygen availability are essential for cellular homeostasis and survival. The most critical molecular event in hypoxic response is the activation and stabilization of a transcriptional factor termed hypoxia-induced factor-1 (HIF-1) that is responsible for the upregulation of many downstream effector genes, collectively known as hypoxia-responsive genes. Multiple key biological pathways such as proliferation, energy metabolism, invasion, and metastasis are governed by these genes; thus, HIF-1-mediated pathways are equally pivotal in both physiology and pathology.
As we gain knowledge on the molecular mechanisms underlying the regulation of HIF-1, a great focus has been placed on elucidating the cellular function of HIF-1, particularly the role of HIF-1 in cancer pathogenesis pathways such as proliferation, invasion, angiogenesis, and metastasis. In cancer, HIF-1 is directly involved in the shift of cancer tissues from oxidative phosphorylation to aerobic glycolysis, a phenomenon known as the Warburg effect. Although targeting HIF-1 as a cancer therapy seems like an extremely rational approach, owing to the complex network of its downstream effector genes, the development of specific HIF-1 inhibitors with fewer side effects and more specificity has not been achieved. Therefore, in this review, we provide a brief background about the function of HIF proteins in hypoxia response with a special emphasis on the unique role played by HIF-1α in cancer growth and invasiveness, in the hypoxia response context.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Hypoxic Response
Oxygen is directly involved in a wide range of physiological pathways essential for maintaining and promoting homeostasis such as injury response and blood pressure adaptation [2], as well as in pathological processes such as inflammation [3] and tumor formation. A key to understanding such regulations could be accomplished through elucidating the molecular mechanisms by which cells respond and adapt to insufficiency in oxygen supply, a phenomenon known as hypoxic response. Although hypoxia is characterized by suppression in both ATP and protein production as mechanisms to reserve energy, interestingly, there is an abundance of a wide spectrum of genes during the low oxygen status [4, 5]; these genes are referred to as hypoxia-responsive genes. It was reported that 2% of the entire human genome is involved in hypoxia response via interaction with what is known as hypoxia-inducible factors (HIFs), both in a direct and an indirect fashion [6]. Activation of the hypoxia-responsive genes serves to protect cells from the harmful ramifications of oxygen deficiency such as ischemia, particularly that many metabolic and energy-related pathways are controlled by these genes [7, 8]. In addition, hypoxia-responsive genes were found to be heavily involved in the embryonic development. For instance, the deletion of HIF-1α in a mouse embryo leads to death at day 10 [9, 10]. Altogether, hypoxic response is responsible for the activation of a global network of genes that through diverse mechanisms aim to maintain tissue integrity and promote cell survival [6, 11, 12]. Once activated, HIF transcription factors binds to specific DNA sequences unique to their target genes. These DNA regions are called hypoxia-response elements (HREs) [13,14,15,16]. Many factors could determine the potential binding between HIFs and HRE, including HIF-1 protein concentration, oxygen tension, availability of cofactors, and posttranslational protein modifications [17, 18].
2 Hypoxia-Inducible Factor
Hypoxia-inducible factors (HIFs) are members of a family of transcription factors that are involved in the adaptive responses to hypoxia. Structurally, all HIFs are composed of an alpha and a beta subunit with both subunits belong to the family of basic-helix-loop-helix PAS (Per-Ahr/ ARNT-Sim) family of transcription factors. The three HIF members are named HIF-1, HIF-2, and HIF-3. Both HIF-1 and HIF-2 are heavily involved in the response to hypoxia through their transcriptional activities, whereas the role of HIF-3 in this context remains ill-defined [19]. This family is characterized by its conserved domains for both DNA binding and target specificity [20]. Many characteristics such as heterodimerization, hypoxia-mediated stabilization, and transcriptional activity are shared among all three isoforms [21,22,23,24].
HIF-1 transcription factor is a heterodimer consisting of two subunits: an oxygen-labile alpha subunit (HIF-1α) and a stable, constitutively-expressed, oxygen-independent beta subunit (HIF-1β). In hypoxia, HIF-1α is the primary responder, and so, its stability is of greater impact when compared to ARNT [25,26,27,28,29]. Nevertheless, ARNT was shown to be required for the HIF1 overall activity such as binding to other bHLH proteins [30,31,32,33].
Structurally, HIF-1α contains two transactivational domains (TADs), the N-terminal (N-TAD) and the C-terminal (C-TAD), that drive the functional interaction with RNA polymerase. TADs also are the sites where the interaction with coactivators is established, a process that has an indispensable role in HIF-1α transcriptional activity. Furthermore, TADs are the domains where posttranslational modifications take place [17, 25, 34, 35]. Interestingly, upon hypoxia-mediated HIF1 activation, only its protein levels increase, while mRNA expression remains unchanged. This observation highlights the direct proportional relation between oxygen concentration and protein translation and stability [25, 36]. Lastly, the oxygen-dependent degradation domain (ODD domain) serves as an oxygen sensor site where oxygen-dependent interactions take place [37].
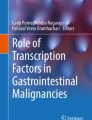
HIF-2 proteins have had many names, such as endothelial PAS protein 1 (EPAS1), HIF-related factor (HRF), HIF-1α-like factor (HLF), and member of PAS family 2 (MOP2) [21,22,23,24]. On the level of the protein’s primary structure, HIF-2α is very similar to HIF-1α with almost half the amino acids being identical between the two. In particular, the two proteins are sharing 70% and 83% homology in their PAS and bHLH domains, respectively. Moreover, both isoforms are subjected to the same regulatory mechanism owing to the presence of two critical proline residues in their ODD domains [38,39,40]. Moreover, both HIF-1α and HIF-2α contain N-TAD and C-TAD, while HIF-1β contains only C-TAD (Fig. 1).

Schematic of the structure of three HIFα and two HIFβ isoforms. NLS, nuclear localization signal; bHLH, basic helix-loop-helix domain; PAS, per-arnt-sim domain subdivided into PAS A and PAS B; ODD, oxygen-dependent degradation domain; TAD, transactivation domain. HIF-1α and HIF-2α have two distinct TADs, in the C- (C-TAD) and N- (N-TAD) terminal domains. The PAS and bHLH domains are dedicated to dimerization and recognition of target DNA sequences. (Reprinted with permission from [41])
HIF-2 expression was thought initially to be exclusive to vascular endothelial cells, specifically in embryonic tissues [35, 42, 43]. Later, HIF-2 protein expression was confirmed in several adult hypoxic tissues [42]. In cancer tissues, HIF-2 expression was also reported to be upregulated, suggesting a potential role in cancer angiogenesis [44] especially with the protein’s preference for vascular and stromal tissues [43, 45]. As such, higher levels of HIF-1 are observed in tumor epithelial cells when compared with HIF-2, whereas the opposite is true in macrophages and endothelial cells [46]. In cancer, HIF-2 expression was shown to be directly proportional to the pathological staging of a number of solid cancers such as non-Hodgkin lymphoma [45, 47] and bladder cancer [43]. One explanation for such correlation is that the presence of HIF-2-positive macrophage populations in cancer tissues is beneficial to the tumor microenvironment (TME), therefore inversely affecting patient’s survival. Another explanation is related to the role played by HIF-2 in promoting cancer angiogenesis and vascularization [45], since VEGF, the master angiogenic protein, co-reside in stromal tissues as well [48]. Many studies have confirmed the correlation between the HIF-2 and VEGF proteins [43, 49,50,51,52].
Noteworthy, many studies reported a contradicting role of HIF-2α in cancer. For example, loss of HIF-2α in KRAS lung tumor increased tumor aggressive behavior [53], whereas overexpression and stabilization of HIF-2α protein in an identical tumor model promoted tumor angiogenesis and invasion by increasing the expression of VEGF and SNAIL [54], respectively. The observation that opposite HIF-2α expression profiles mediated tumor growth in the same tumor context, albeit by different mechanisms, suggests that effective targeting of HIF-2α subunit in cancer treatment may be complicated.
The third isoform is referred to as HIF-3 [55], and although it shares a significant structural similarity with the other two isoforms, it is reported that its main function is to inhibit HIF pathway [56]. On the other hand, other studies showed that HIF-3 has a dual action of both stimulating and suppressing other HIF members. Therefore, the role of HIF-3 in hypoxic and cancer tissues in particular is yet to be elucidated [57,58,59,60].
HIF β protein was first discovered in the neural tissues where involvement with neural development was assumed [61]. It is also known as the aryl hydrocarbon receptor nuclear translocator (ARNT) [16, 62, 63]. There are two forms of ARNT termed ARNT1 and ARNT2 [64, 65] with both forms are capable of forming a heterodimer with the HIF α isoforms, an interaction crucial for HRE binding and subsequent downstream effector gene activation [65]. Currently, HIF-1α, HIF-2α, and ARNT1 are viewed as the key molecules involved in HIF pathway in response to hypoxia, especially in tumor tissues, while the function of both HIF-3α and ARNT2 is still under investigation. In this review, we will focus on the functional role of HIF-1α in driving hypoxia response in human cancer.
2.1 Discovery of HIF-1
HIF-1 was initially viewed as an essential and exclusive key element in the human erythropoietin (EPO) gene in response to oxygen insufficiency in renal tissues [66]. At that time, the concept of direct oxygen sensing, which cells can independently and directly sense and respond to changes in oxygen level, was still developing. Subsequently, the novel discovery that the function of HIF-1 is not EPO gene-restricted and that it regulates other genes is considered a milestone in the field of direct oxygen sensing. HIF-1 was later purified [14], and shortly, the protein molecule was further characterized [62].
Afterward, a wide spectrum of HIF-1 target genes and microRNAs (miRNAs) that were involved in hypoxic response were identified on both genetic and protein levels [67]. Both HIF-1 target gene’s activation and suppression were characterized as being tissue-specific [68]. Moreover, HIF-1-mediated activation of gene transcription may be in both direct and indirect fashion [6]. For instance, by activating miRNAs [67] and gene-suppressors such as DEC1/Stra13 [69], HIF-1 is indirectly silencing certain downstream effector genes. Key biological pathways such as proliferation, energy metabolism, invasion, and metastasis were found to be driven by HIF-1 downstream effector genes [70, 71] (Fig. 2), suggesting the important role of HIF-1-mediated pathways in cancer development and progression.

Representative target genes of HIF-1α and their functions
2.2 Regulation of HIF-1α
It was reported that many oncogenes activate HIF-1α pathway mainly via phosphorylation cascades through upregulating the transcription and translation of HIF-1α mRNA and protein, respectively, and independently of oxygen levels [72]. Similarly, growth factors and cytokines such as epidermal and fibroblast growth factors and insulin-like growth factor could activate HIF-1α through the same phosphorylation mechanism [73,74,75,76]. This phosphorylation cascade could promote HIF-1α expression via several pathways. One example is the PI3K/Akt/mTOR-mediated HIF-1α pathway activation as seen in many solid tumors such as in colon [77], prostate [78], and breast cancer [76]. Another mechanism is by enhancing the p300-HIF-1α-C-TAD activation complex [79] and favoring HIF-1α nuclear translocation as seen via MAPK-mediated phosphorylation [80]. MAPK-mediated phosphorylation also promotes HIF-1α transcriptional activity by blocking its nuclear export in an CRM1-dependent fashion [80]. HIF-1α pathway can also be activated by growth factors via ERK-dependent signaling [17]. In addition, vasoactive cytokines may promote HIF-1α transcriptional activity through diacylglycerol-sensitive protein kinase C [81]. Altogether, upregulation of HIF-1α exerted by growth factors and local hormones can overcome its oxygen-dependent degradation [76, 77].
Other kinases such as casein kinase 1 (CK1) were also reported to be involved in HIF-1α phosphorylation [82]. Moreover, it was reported that the phosphorylation status of HIF-1α is linked to the protein’s ability to repair DNA damage and reverse chromosomal instability, two characteristics that are extremely important in driving tumor progression and aggressiveness. For instance, dephosphorylation of HIF1α directly leads to repression of NBS1, a DNA mismatch repair gene [83].
In addition to the kinase signaling pathways, loss of function of the gene suppressor von Hippel-Lindau (VHL) results in activation of HIF-1α protein due to the associated lack of protein-degradation suppression [84]. A dysregulation of key carbohydrate metabolic intermediates was also shown to contribute to HIF-1α regulation independently to oxygen levels. For instance, α-ketoglutarate (α-KG) functions as a cofactor for PDH and FIH-1 (factor inhibiting HIF-1) hydroxylates [85] and is therefore directly involved in HIF-1α regulation.
Posttranslational modifications other than phosphorylation are also critical for HIF-1α protein activity. For instance, hydroxylation of HIF-1α protein by prolyl hydroxylase is viewed as the main regulatory mechanism that guards against HIF-1α protein activation in normoxic conditions. HIF hydroxylases exist in two forms: HIF-prolyl hydroxylase, also known as prolyl hydroxylase domain (PHD) proteins, and HIF-asparaginyl hydroxylase, also known as FIH-1 (factor inhibiting HIF-1) [86].
There are three closely-related isoforms of the PHD protein known as PHD1, PHD2, and PHD3, where PHD2 is considered the most critical under normoxic conditions [87]. PHD enzymes function by hydroxylation of two prolyl segments of HIF-1α protein, where oxygen concentration is an imperative determinant for the reaction initiation [34, 88,89,90]. This interaction takes place at the ODD domain where the two propyl residues reside. Once hydroxylated, HIF-1α develops a strong binding affinity for a part of an E3 ubiquitin ligase complex VHL protein leading to HIF-1α protein degradation by a proteasome. The reversal of this oxygen-dependent degradation process results in an observed increase in HIF-1α protein levels associated with hypoxia.
A second hydroxylation event targets the asparaginyl residue at the C-TAD of HIF-1α protein by FIH-1. FIH-1 reaction depends exclusively on oxygen availability in the ambient environment [86]. This reaction changes HIF-1α protein’s physical properties, such as its water affinity, hindering the interaction between the hydroxylated C-TAD and its coactivators p300/CREB binding protein (CBP) [91, 92]. This reaction will result in C-TAD domain blockage and ultimately HIF-1α transactivation activity inhibition, but not stability, in an oxygen-dependent reversible fashion (Fig. 3).

HIF-1 signaling cascade. Synthesis and constitutive expression of HIF-1α by a cascade involving a series of growth factors and signaling events are indicated. The major differences among the hypoxic and normoxic signaling and sequence of events are also depicted clearly in the flowchart. Normoxia leads to HIF-1α protein degradation whereas hypoxia leads to HIF-1α-regulated target gene expression. The downstream sequence of events leading to tumorigenesis is also portrayed (Modified with permission from [93])
Redox sensors are equally important to oxygen sensors in the regulation of HIF-1α-mediated hypoxic response. An example is the SIRT1-mediated acetylation process, which is another critical posttranslational modification of HIF-1α. SIRT1 deacetylates HIF-1α by targeting the lysine amino acid leading to the blocking of p300-recruitment and eventually HIF-1α inactivation [94].
2.3 HIF-1α Stability
Although oxygen tension is considered the main factor governing HIF-1α protein stability during hypoxia through the hydroxylation events discussed earlier, mitochondria can also act as a stabilizer of HIF-1α proteins via increased production of reactive oxygen species (ROS) [95,96,97]. ROS might play a role in protein stabilization mainly through the inactivation of PHD leading to HIF-1α accumulation [98]. Lastly, reports on nitric oxide (NO) effect on HIF are contradictory, with some advocating for HIF-1α stabilization [99,100,101,102], whereas others demonstrating an opposite effect on HIF-1α activity [103,104,105]. Once the protein is stabilized, nuclear translocated, and dimerized with ARNT, hypoxia-responsive genes are activated through HIF-1α binding to a characteristic consensus sequence 5′-(A/G) CGTG-3 termed HRE [106] located in the upstream region of hypoxia-inducible genes [15, 107, 108].
3 HIF-1α and Metabolic Reprogramming
A shift from glucose metabolism coupled with mitochondrial oxidative to anabolic respiration, known as the Warburg effect, is a hallmark of hypoxia. This metabolic shift takes place through the upregulation of oxygen-independent metabolic pathways, such as glycolysis and downregulation of the oxygen-dependent pathways such as mitochondrial respiration [109]. For instance, overexpression of key glycolytic enzymes such as the rate-limiting enzyme phosphofructokinase [110] and the glycolytic flux regulatory enzymes, 6- phosphofructo-2-kinase and fructose-2,6-bisphosphate, is HIF-1α-mediated in hypoxia [37,38,39,40]. Other enzymes such as glucose transporter protein1 (GLUT1) and GLUT3 that are involved in glucose trafficking processes are also the targets of HIF-1α in hypoxia [111, 112]. Noteworthy, there is a positive correlation among cancer pathological staging, GLUT3 and HIF-1α expression and activity levels, a measure that might serve as a prognostic tool [112]. HIF-1α activation also upregulates key enzymes that inhibit acetyl-coenzyme A (acetyl-CoA) production from glucose, therefore inhibiting oxidative phosphorylation. There are two isoforms of the enzyme pyruvate dehydrogenase kinase (PDK) known as PDK1 and PDK3 that directly inhibit acetyl-CoA production and entering into the TCA cycle leading to the shutdown of the oxidative phosphorylation associated with hypoxia. Another approach for cells to shift away from oxidative metabolism is through the activation of mitochondrial autophagy by protein BCL2/adenovirus E1B 19-kDa interacting protein 3 (BNIP3) [113]. BNIP3 functions by activating lactose dehydrogenase A (LDHA) enzyme that converts pyruvate to lactate, therefore promoting the anaerobic respiration.
Similarly, PDK1 and PDK3 were also found to play a role in mitochondrial autophagy [114,115,116]. In addition, miRNA targets of HIF-1α were found to directly favor the metabolic shift through inhibiting genes that are critical for the mitochondria oxidation machinery and independently of the metabolic enzymes [117]. For instance, miR-210 activation [118] inhibits the iron-sulfur cluster assembly enzyme ISCU, which is essential for the mitochondrial electron transport complex I activity [119, 120]. Noteworthy, due to the scarcity of acetyl-CoA in response to hypoxia, tissues with a high proliferation rate such as cancer will utilize glutamine, instead of glucose, to generate α-ketoglutarate essential for fatty acid synthesis [121, 122]. Glutamine utilization as the main source of energy for such high-energy-demanding cells acts as another repelling force for the pyruvate away from the TCA cycle [121, 122]. HIF-1α-mediated fatty acid metabolism dysregulation in cancer hypoxic tissues was associated with poor survival in many solid tumors such as renal cancer [123]. The high-glycolytic-flux signature in hypoxia serves a unique benefit for cancer tissues, other than solely energy benefit, and that is providing precursors of the pyrimidine/purine pathway needed for DNA synthesis for cell proliferation [124]. For example, it was reported that glucose utilization is directly proportional to increased cancer tissue mass and invasion property [125], suggesting a critical role played by glucose metabolism in tumorigenesis.
HIF-1α significantly contributes to the acidic environment of cancer tissues through the activation of plasma membrane proteins [126] such as monocarboxylate transporter 4 (MCT4), encoded by SLC16A3 gene, through controlling lactic acid transport [127]. Another membranous protein named sodium-hydrogen exchanger 1 (NHE1) that is encoded by the SLC9A gene regulates the pH of the environment through protons pumping [128], and the same mechanism is adopted by carbonic anhydrase 9 (CA9) [129]. In fact, the intracellular alkalinization and extracellular acidification enhance cellular proliferation and invasion [130].
An interesting aspect of HIF-1α regulation lies in its activation loop with pyruvate kinase M2 (PKM2) enzyme. PKM2 is a glycolytic enzyme that may play an important role in cancer progression [131] by promoting glycolysis as well as acting as a coactivator for HIF-1α [132]. HIF-1α also activates the transcription of PKM2 leading to the activation of key oncogenes such as STAT3 and its downstream genes, which further enhances the progression of cancer [133].
4 Hypoxia and Cancer
Tumor hypoxia is an example of a chronic, pathophysiological condition, in which response is insufficient to completely reverse the hypoxic insult [134]. Hypoxia in cancer could be defined on the basis of oxygen and energy levels present in tumors. For instance, a concomitant decrease in both oxygen partial pressure and ATP level occurs in a fibrosarcoma model [135]. A key player in cancer hypoxia dynamics is the hypoxia-induced vascular endothelial growth factor (VEGF). Due to the constant hypoxic insult that cancer tissues are exposed to, VEGF-mediated new blood vessel formation to overcome the oxygen deficiency is slow and disordered. This continuous cycle of defective blood vessel architecture and the activation of hypoxia-mediated pathways is a hallmark for tumor microenvironment (TME) [136] as well as its aggressive phenotype [137]. Many solid tumors such as breast and lung, among others, respond to the decrease in oxygen tension by upregulation of HIF-1α [138,139,140]. Correlation between hypoxia and tumor malignant transformation had also been observed [141,142,143].
5 HIF-1α and Immune Cells in Cancer
Many solid tumors are characterized by hypoxia [144] and tumor-associated macrophage (TAM) infiltration [145]. For example, in breast cancer, HIF-1α knockout in TAM caused overstimulation of nitrous oxide (NO) [145, 146], a phenomenon that can put T lymphocytes into anergy status. Hypoxia can also increase the expression of the immune checkpoint programmed death-ligand 1 (PD-L1) on macrophages, dendritic cells, and tumor cells in an HIF-1α-dependent fashion leading to the suppression of effector T-lymphocyte recruitment and activation [147]. Another mechanism that HIF-1α can dampen the antitumor effect of immunity through is the upregulation of regulatory T lymphocytes [148].
6 Role of HIF-1α in Key Cancer Pathways
6.1 Cell Adhesion
Adhesion molecules play a significant role in cancer initiation and progression through promoting its interaction with both intracellular and extracellular environment [149]. HIF-1α is directly involved in the regulation of key adhesion molecules such as β1 integrins and α5β3 and α5β5 expression [150,151,152]. E-cadherin is also regulated by HIF-1α via its direct regulation of TCF3, ZFHX1A, and ZFHX1B [153] and up-regulation of Snail [154] which inhibits E-cadherin gene expression.
6.2 Cell Proliferation
One of the defining characteristics of cancer cells is their uncontrollable proliferation coupled with impairment of cell death pathways and signals awing to overexpression of survival and growth factors; such changes enable cancer cells to adapt to nutritional deprivation or to escape their unfavorable environment. For instance, hypoxia stimulation of VEGF transcription, via the HIF pathway, was shown to be strongly associated with cellular proliferation and metastasis in tumors [155]. Additionally, the expression of hypoxia-mediated telomerase reverse transcriptase (TERT) promotes tumor cells’ immortal phenotype [156]. Simultaneously, hypoxia-induced downregulation of membranous integrins was reported to facilitate tumor cell detachment and new tumor growth [157]. A recent study of ARK5 expression in colon cancer showed that it was upregulated in a HIF-1α-dependent manner and that ARK5 serves an important player in cancer proliferation and migration under hypoxic stress [158]; similar effects were also reported in other solid cancers [159,160,161].
6.3 Metastasis and Invasion
Hypoxia can activate epithelial-to-mesenchymal transition (EMT) via HIF-1α in various types of solid tumors [162,163,164]. HIF-1α can directly or indirectly regulate key EMT regulators, including TWIST, Snail, carbonic anhydrase IX (CAIX), and GLUT-1 [165,166,167,168]. These molecules then trans-activate EMT-related genes, including vimentin, E-cadherin and N-cadherin, to facilitate the progression of the EMT [169, 170]. Matrix metalloproteinase MMP2 and MMP9 have also been reported to be regulated by HIF-1α. The impact of hypoxia-induced MMP-9 expression is extremely central for cellular migration [171, 172]. Besides, two major components of the fibrinolysis system and thus metastasis, named urokinase-type plasminogen activator receptor (uPAR) and plasminogen activator inhibitor-1 (PAI-1), have also been shown to be targets of HIF-1α [173, 174]. TWIST, another essential transcription factor that is involved in hypoxia-mediated EMT and tumor metastasis, is directly regulated by HIF-1α [165]. Other significant HIF-1α target genes directly involved in cancer metastasis are CXC chemokine receptor-4 (CXCR4), c-Met and CC chemokine receptor 7 (CCR7) [175,176,177], lysyl oxidase (LOX) [6, 178], fibronectin, cathepsin D, and urokinase plasminogen activator [11]. HIF-1α also promotes cell invasion through the upregulation of key invasion-promoting genes such as the autocrine motility factor [179], vimentin, and the receptor tyrosine kinase c-Met [175]. Meanwhile, the stromal-derived factor-1, keratins 14, 18, and 19, the cytokine receptor CXCR4P [180, 181], caveolin-1 (CAV1) [182], uPAR, MMP2, cathepsin D, and fibronectin 1, among others, are transcriptionally upregulated by HIF-1α [183].
6.4 Angiogenesis
Angiogenesis plays an essential role in tumorigenesis. HIF-1α can stimulate an angiogenic response by activating a number of growth factor-encoding genes, including VEGF, angiopoietin1 (ANGPT1) and ANGPT2, placental growth factor (PGF), calcitonin receptor-like receptor (CRLR) [184], and platelet-derived growth factor B (PDGFB) [68, 185]. HIF-1α deletion was reported to be associated with abnormal vasculature [186]. On the other hand, a recent report on pancreatic tumor revealed an alternative mechanism by which cancer cells could maintain angiogenesis in an HIF1α-independent manner [187]. Noteworthy, SUMO-specific protease 1 (SENP1), a HIF-1α target enzyme, is of great importance for HIF-1α stabilization in hypoxia. This positive feedback loop is significant for VEGF activation and angiogenesis [188, 189].
6.5 Apoptosis
Although programmed cell death can be directly triggered by deficiency in oxygen levels in both normal and cancer tissues [190], with accompanying DNA damage [191], the direct effect of HIF pathway on apoptosis is reported to range from apposing cell death [192] to promoting apoptosis [193]. One explanation for this variation in HIF pathway response might be related to the degree for hypoxia and the variation in oxygen tension [194]. A second factor for such fluctuation is the presence of several apoptosis-related proteins, such as cyclin D1, p21, and p27 that are targeted by HIF-1α upon activation, and that apoptosis response depends on the expression profiles of these apoptotic molecules [195]. Lastly, the initial energy level of hypoxic tissues is inevitably a key factor in the apoptosis pathway [196].
Other factors such as the mitochondrial membrane integrity could also trigger an apoptotic response through activating key apoptotic mediators, such as caspase 9, independently of HIF-1α pathway [197]. Wild-type tumor-suppressor gene p53 also plays a critical role in hypoxia-induced apoptosis through caspase 9 and Apaf-1 downstream effector [198, 199]. Other key apoptotic molecules such as BNIP3, a member of the Bcl-2 family [200], and Noxa which is a p53-downstream protein that could sense ROS levels [201] have also been identified as targets of HIF-1α.
7 Clinical Significance and HIF-1α Inhibitors for Cancer Therapy
HIF-1α expression levels were positively correlated with tumor progression in a variety of solid tumors such as glioma and breast cancer, where HIF-1α correlates with tumor pathological grade and invasion in the former [202], and overall poor survival rate in the later [203, 204]. HIF-1α is used as a prognostic marker for different treatment modalities in a variety of solid tumors [205,206,207].
The combination of HIF-1α expression with oncogenes or tumor suppressor genes is viewed as another powerful prognostic factor. For instance, in ovarian cancer, the coexistence of mutant p53 expression and HIF-1 overexpression was associated with a poor survival rate [208] and resistance to chemotherapy mainly due to p53-mediated activation of RAS signaling that leads to apoptosis impairment [209]. Recently, a correlation between HIF-1α and the tumor suppressor NEDD4L levels in gastric cancer has been proposed as a prognostic marker [210]. In addition, HIF-1α upregulation combined with the antiapoptotic protein Bcl-2 downregulation in esophageal cancer is associated with treatment failure [211].
HIF-1α inhibition provides an innovative approach for modifying tumor niche with promising clinical results. Unfortunately, and awing to the complex network of genes that are regulated by HIF-1α as well as the multilayered HIF-1α regulation mechanisms, it is challenging to develop a specific HIF-1α inhibitor with a high specificity [212]. Another factor that might tremendously affect the drug discovery process is accuracy and sensitivity of the screening methods. Currently, there are several anti-HIF-1α molecules that are classified according to their target site into direct and indirect inhibitors. Direct inhibitors refer to molecules that target the transcriptional activity of HIF-1α, whereas indirect inhibitors are molecules that target HIF-1α transcription and translation on the mRNA and protein levels, respectively [213]. HIF-1α inhibitors are also classified according to the targeted stage of HIF-1α ranging from the mRNA transcription to protein degradation [214]. In conclusion, the continuous search for the specific HIF-1α inhibitor with fewer side effects and better patient tolerance and survival rate is still ongoing. Noteworthy, combination therapy with other target molecules such as antiangiogenic drugs is showing promising results in animal model studies [215, 216]. A comprehensive understanding of the structure, molecular biology, and regulatory machinery of HIF-1α domains will undoubtedly aid in the development of specific HIF-1α inhibitors.
8 Conclusion
It has been nearly three decades since the novel discovery of HIF-1α as a master regulator of hypoxic response as well as its implication in cancer progression and survival in many solid tumors. Since then, HIF-1α was regarded as a significant and promising target in anticancer therapy. A great deal of research in this area as well as the development of HIF-1α inhibitors have clearly translated such impact. Unfortunately, none of these therapies were proven to be precisely and exclusively targeting cancer, leading to undesirable side effects. Indeed, the involvement of HIF-1α in many aspects of physiological pathways seems to be the main obstacle for perfectly targeting it. Therefore, future research may emphasize more on unfolding all the genes and proteins involved in the HIF-1α pathway, elucidating the molecular mechanisms that regulate other HIF members, and finally aim to discover and target a novel cancer-specific molecule from the HIF-1α downstream effectors expanding pool.
References
Michiels, C. (2004). Physiological and pathological responses to hypoxia. The American Journal of Pathology, 164(6), 1875–1882.
Warren, S. M., et al. (2001). Hypoxia regulates osteoblast gene expression. The Journal of Surgical Research, 99(1), 147–155.
Cramer, T., et al. (2003). HIF-1alpha is essential for myeloid cell-mediated inflammation. Cell, 112(5), 645–657.
Hochachka, P. W., et al. (1996). Unifying theory of hypoxia tolerance: Molecular/metabolic defense and rescue mechanisms for surviving oxygen lack. Proceedings of the National Academy of Sciences of the United States of America, 93(18), 9493–9498.
Denko, N., et al. (2003). Hypoxia actively represses transcription by inducing negative cofactor 2 (Dr1/DrAP1) and blocking preinitiation complex assembly. The Journal of Biological Chemistry, 278(8), 5744–5749.
Manalo, D. J., et al. (2005). Transcriptional regulation of vascular endothelial cell responses to hypoxia by HIF-1. Blood, 105(2), 659–669.
Semenza, G. L. (1998). Hypoxia-inducible factor 1: Master regulator of O2 homeostasis. Current Opinion in Genetics & Development, 8(5), 588–594.
Wenger, R. H. (2002). Cellular adaptation to hypoxia: O2-sensing protein hydroxylases, hypoxia-inducible transcription factors, and O2-regulated gene expression. The FASEB Journal, 16(10), 1151–1162.
Iyer, N. V., et al. (1998). Cellular and developmental control of O2 homeostasis by hypoxia-inducible factor 1 alpha. Genes & Development, 12(2), 149–162.
Ryan, H. E., Lo, J., & Johnson, R. S. (1998). HIF-1 alpha is required for solid tumor formation and embryonic vascularization. The EMBO Journal, 17(11), 3005–3015.
Semenza, G. L. (2003). Targeting HIF-1 for cancer therapy. Nature Reviews. Cancer, 3(10), 721–732.
Schofield, C. J., & Ratcliffe, P. J. (2004). Oxygen sensing by HIF hydroxylases. Nature Reviews. Molecular Cell Biology, 5(5), 343–354.
Semenza, G. L., et al. (1991). Hypoxia-inducible nuclear factors bind to an enhancer element located 3′ to the human erythropoietin gene. Proceedings of the National Academy of Sciences of the United States of America, 88(13), 5680–5684.
Semenza, G. L., & Wang, G. L. (1992). A nuclear factor induced by hypoxia via de novo protein synthesis binds to the human erythropoietin gene enhancer at a site required for transcriptional activation. Molecular and Cellular Biology, 12(12), 5447–5454.
Wang, G. L., & Semenza, G. L. (1993). Characterization of hypoxia-inducible factor 1 and regulation of DNA binding activity by hypoxia. The Journal of Biological Chemistry, 268(29), 21513–21518.
Wang, G. L., & Semenza, G. L. (1993). General involvement of hypoxia-inducible factor 1 in transcriptional response to hypoxia. Proceedings of the National Academy of Sciences of the United States of America, 90(9), 4304–4308.
Richard, D. E., et al. (1999). p42/p44 mitogen-activated protein kinases phosphorylate hypoxia-inducible factor 1alpha (HIF-1alpha) and enhance the transcriptional activity of HIF-1. Journal of Biological Chemistry, 274(46), 32631–32637.
Carrero, P., et al. (2000). Redox-regulated recruitment of the transcriptional coactivators CREB-binding protein and SRC-1 to hypoxia-inducible factor 1alpha. Molecular and Cellular Biology, 20(1), 402–415.
Duan, C. (2016). Hypoxia-inducible factor 3 biology: Complexities and emerging themes. American Journal of Physiology. Cell Physiology, 310(4), C260–C269.
Wang, G. L., et al. (1995). Hypoxia-inducible factor 1 is a basic-helix-loop-helix-PAS heterodimer regulated by cellular O2 tension. Proceedings of the National Academy of Sciences of the United States of America, 92(12), 5510–5514.
Ema, M., et al. (1997). A novel bHLH-PAS factor with close sequence similarity to hypoxia-inducible factor 1alpha regulates the VEGF expression and is potentially involved in lung and vascular development. Proceedings of the National Academy of Sciences of the United States of America, 94(9), 4273–4278.
Flamme, I., et al. (1997). HRF, a putative basic helix-loop-helix-PAS-domain transcription factor is closely related to hypoxia-inducible factor-1 alpha and developmentally expressed in blood vessels. Mechanisms of Development, 63(1), 51–60.
Hogenesch, J. B., et al. (1997). Characterization of a subset of the basic-helix-loop-helix-PAS superfamily that interacts with components of the dioxin signaling pathway. The Journal of Biological Chemistry, 272(13), 8581–8593.
Tian, H., McKnight, S. L., & Russell, D. W. (1997). Endothelial PAS domain protein 1 (EPAS1), a transcription factor selectively expressed in endothelial cells. Genes & Development, 11(1), 72–82.
Huang, L. E., et al. (1996). Activation of hypoxia-inducible transcription factor depends primarily upon redox-sensitive stabilization of its alpha subunit. The Journal of Biological Chemistry, 271(50), 32253–32259.
Jiang, B. H., et al. (1997). Transactivation and inhibitory domains of hypoxia-inducible factor 1alpha. Modulation of transcriptional activity by oxygen tension. The Journal of Biological Chemistry, 272(31), 19253–19260.
Salceda, S., & Caro, J. (1997). Hypoxia-inducible factor 1alpha (HIF-1alpha) protein is rapidly degraded by the ubiquitin-proteasome system under normoxic conditions. Its stabilization by hypoxia depends on redox-induced changes. The Journal of Biological Chemistry, 272(36), 22642–22647.
Jiang, B. H., et al. (1997). V-SRC induces expression of hypoxia-inducible factor 1 (HIF-1) and transcription of genes encoding vascular endothelial growth factor and enolase 1: Involvement of HIF-1 in tumor progression. Cancer Research, 57(23), 5328–5335.
Chilov, D., et al. (1999). Induction and nuclear translocation of hypoxia-inducible factor-1 (HIF-1): Heterodimerization with ARNT is not necessary for nuclear accumulation of HIF-1alpha. Journal of Cell Science, 112(Pt 8), 1203–1212.
Wood, S. M., et al. (1996). The role of the aryl hydrocarbon receptor nuclear translocator (ARNT) in hypoxic induction of gene expression. Studies in ARNT-deficient cells. The Journal of Biological Chemistry, 271(25), 15117–15123.
Maltepe, E., et al. (1997). Abnormal angiogenesis and responses to glucose and oxygen deprivation in mice lacking the protein ARNT. Nature, 386(6623), 403–407.
Swanson, H. I., & Bradfield, C. A. (1993). The AH-receptor: Genetics, structure and function. Pharmacogenetics, 3(5), 213–230.
Rowlands, J. C., & Gustafsson, J. A. (1997). Aryl hydrocarbon receptor-mediated signal transduction. Critical Reviews in Toxicology, 27(2), 109–134.
Bruick, R. K., & McKnight, S. L. (2001). A conserved family of prolyl-4-hydroxylases that modify HIF. Science, 294(5545), 1337–1340.
Jeong, J. W., et al. (2002). Regulation and destabilization of HIF-1alpha by ARD1-mediated acetylation. Cell, 111(5), 709–720.
Gradin, K., et al. (1996). Functional interference between hypoxia and dioxin signal transduction pathways: Competition for recruitment of the Arnt transcription factor. Molecular and Cellular Biology, 16(10), 5221–5231.
Huang, L. E., et al. (1998). Regulation of hypoxia-inducible factor 1alpha is mediated by an O2-dependent degradation domain via the ubiquitin-proteasome pathway. Proceedings of the National Academy of Sciences of the United States of America, 95(14), 7987–7992.
Pugh, C. W., et al. (1997). Activation of hypoxia-inducible factor-1; definition of regulatory domains within the alpha subunit. The Journal of Biological Chemistry, 272(17), 11205–11214.
O’Rourke, J. F., et al. (1999). Oxygen-regulated and transactivating domains in endothelial PAS protein 1: Comparison with hypoxia-inducible factor-1α. Journal of Biological Chemistry, 274(4), 2060–2071.
Srinivas, V., et al. (1999). Characterization of an oxygen/redox-dependent degradation domain of hypoxia-inducible factor alpha (HIF-alpha) proteins. Biochemical and Biophysical Research Communications, 260(2), 557–561.
Dayan, F., et al. (2008). A dialogue between the hypoxia-inducible factor and the tumor microenvironment. Cancer Microenvironment, 1(1), 53–68.
Wiesener, M. S., et al. (2003). Widespread hypoxia-inducible expression of HIF-2alpha in distinct cell populations of different organs. The FASEB Journal, 17(2), 271–273.
Onita, T., et al. (2002). Hypoxia-induced, perinecrotic expression of endothelial per-ARNT-Sim domain protein-1/hypoxia-inducible factor-2alpha correlates with tumor progression, vascularization, and focal macrophage infiltration in bladder cancer. Clinical Cancer Research, 8(2), 471–480.
Keith, B., Johnson, R. S., & Simon, M. C. (2011). HIF1alpha and HIF2alpha: Sibling rivalry in hypoxic tumour growth and progression. Nature Reviews. Cancer, 12(1), 9–22.
Leek, R. D., et al. (2002). Relation of hypoxia-inducible factor-2 alpha (HIF-2 alpha) expression in tumor-infiltrative macrophages to tumor angiogenesis and the oxidative thymidine phosphorylase pathway in human breast cancer. Cancer Research, 62(5), 1326–1329.
Wiesener, M. S., et al. (1998). Induction of endothelial PAS domain protein-1 by hypoxia: Characterization and comparison with hypoxia-inducible factor-1alpha. Blood, 92(7), 2260–2268.
Stewart, M., et al. (2002). Expression of angiogenic factors and hypoxia inducible factors HIF 1, HIF 2 and CA IX in non-Hodgkin’s lymphoma. Histopathology, 40(3), 253–260.
Fukumura, D., et al. (1998). Tumor induction of VEGF promoter activity in stromal cells. Cell, 94(6), 715–725.
Flamme, I., Krieg, M., & Plate, K. H. (1998). Up-regulation of vascular endothelial growth factor in stromal cells of hemangioblastomas is correlated with up-regulation of the transcription factor HRF/HIF-2alpha. The American Journal of Pathology, 153(1), 25–29.
Giatromanolaki, A., et al. (2001). Relation of hypoxia inducible factor 1 alpha and 2 alpha in operable non-small cell lung cancer to angiogenic/molecular profile of tumours and survival. British Journal of Cancer, 85(6), 881–890.
Xia, G., et al. (2001). Regulation of vascular endothelial growth factor transcription by endothelial PAS domain protein 1 (EPAS1) and possible involvement of EPAS1 in the angiogenesis of renal cell carcinoma. Cancer, 91(8), 1429–1436.
Favier, J., et al. (2002). Angiogenesis and vascular architecture in pheochromocytomas: Distinctive traits in malignant tumors. The American Journal of Pathology, 161(4), 1235–1246.
Mazumdar, J., et al. (2010). HIF-2alpha deletion promotes Kras-driven lung tumor development. Proceedings of the National Academy of Sciences of the United States of America, 107(32), 14182–14187.
Kim, W. Y., et al. (2009). HIF2alpha cooperates with RAS to promote lung tumorigenesis in mice. The Journal of Clinical Investigation, 119(8), 2160–2170.
Makino, Y., et al. (2002). Inhibitory PAS domain protein (IPAS) is a hypoxia-inducible splicing variant of the hypoxia-inducible factor-3alpha locus. The Journal of Biological Chemistry, 277(36), 32405–32408.
Hara, S., et al. (2001). Expression and characterization of hypoxia-inducible factor (HIF)-3alpha in human kidney: Suppression of HIF-mediated gene expression by HIF-3alpha. Biochemical and Biophysical Research Communications, 287(4), 808–813.
Maynard, M. A., et al. (2003). Multiple splice variants of the human HIF-3 alpha locus are targets of the von Hippel-Lindau E3 ubiquitin ligase complex. The Journal of Biological Chemistry, 278(13), 11032–11040.
Maynard, M. A., et al. (2007). Dominant-negative HIF-3 alpha 4 suppresses VHL-null renal cell carcinoma progression. Cell Cycle, 6(22), 2810–2816.
Tanaka, T., et al. (2009). The human HIF (hypoxia-inducible factor)-3alpha gene is a HIF-1 target gene and may modulate hypoxic gene induction. The Biochemical Journal, 424(1), 143–151.
Heikkila, M., et al. (2011). Roles of the human hypoxia-inducible factor (HIF)-3alpha variants in the hypoxia response. Cellular and Molecular Life Sciences, 68(23), 3885–3901.
Michaud, J. L., et al. (2000). ARNT2 acts as the dimerization partner of SIM1 for the development of the hypothalamus. Mechanisms of Development, 90(2), 253–261.
Wang, G. L., & Semenza, G. L. (1995). Purification and characterization of hypoxia-inducible factor 1. The Journal of Biological Chemistry, 270(3), 1230–1237.
Keith, B., Adelman, D. M., & Simon, M. C. (2001). Targeted mutation of the murine arylhydrocarbon receptor nuclear translocator 2 (Arnt2) gene reveals partial redundancy with Arnt. Proceedings of the National Academy of Sciences of the United States of America, 98(12), 6692–6697.
Drutel, G., et al. (1996). Cloning and selective expression in brain and kidney of ARNT2 homologous to the Ah receptor nuclear translocator (ARNT). Biochemical and Biophysical Research Communications, 225(2), 333–339.
Hirose, K., et al. (1996). cDNA cloning and tissue-specific expression of a novel basic helix-loop-helix/PAS factor (Arnt2) with close sequence similarity to the aryl hydrocarbon receptor nuclear translocator (Arnt). Molecular and Cellular Biology, 16(4), 1706–1713.
Wang, G. L., & Semenza, G. L. (1996). Molecular basis of hypoxia-induced erythropoietin expression. Current Opinion in Hematology, 3(2), 156–162.
Camps, C., et al. (2014). Integrated analysis of microRNA and mRNA expression and association with HIF binding reveals the complexity of microRNA expression regulation under hypoxia. Molecular Cancer, 13, 28.
Kelly, B. D., et al. (2003). Cell type-specific regulation of angiogenic growth factor gene expression and induction of angiogenesis in nonischemic tissue by a constitutively active form of hypoxia-inducible factor 1. Circulation Research, 93(11), 1074–1081.
Yun, Z., et al. (2002). Inhibition of PPAR gamma 2 gene expression by the HIF-1-regulated gene DEC1/Stra13: A mechanism for regulation of adipogenesis by hypoxia. Developmental Cell, 2(3), 331–341.
Balamurugan, K. (2016). HIF-1 at the crossroads of hypoxia, inflammation, and cancer. International Journal of Cancer, 138(5), 1058–1066.
Liu, W., et al. (2012). Targeted genes and interacting proteins of hypoxia inducible factor-1. International Journal of Biochemistry and Molecular Biology, 3(2), 165–178.
Pouyssegur, J., Dayan, F., & Mazure, N. M. (2006). Hypoxia signalling in cancer and approaches to enforce tumour regression. Nature, 441(7092), 437–443.
Zelzer, E., et al. (1998). Insulin induces transcription of target genes through the hypoxia-inducible factor HIF-1alpha/ARNT. The EMBO Journal, 17(17), 5085–5094.
Feldser, D., et al. (1999). Reciprocal positive regulation of hypoxia-inducible factor 1alpha and insulin-like growth factor 2. Cancer Research, 59(16), 3915–3918.
Hellwig-Burgel, T., et al. (1999). Interleukin-1beta and tumor necrosis factor-alpha stimulate DNA binding of hypoxia-inducible factor-1. Blood, 94(5), 1561–1567.
Laughner, E., et al. (2001). HER2 (neu) signaling increases the rate of hypoxia-inducible factor 1alpha (HIF-1alpha) synthesis: Novel mechanism for HIF-1-mediated vascular endothelial growth factor expression. Molecular and Cellular Biology, 21(12), 3995–4004.
Fukuda, R., et al. (2002). Insulin-like growth factor 1 induces hypoxia-inducible factor 1-mediated vascular endothelial growth factor expression, which is dependent on MAP kinase and phosphatidylinositol 3-kinase signaling in colon cancer cells. The Journal of Biological Chemistry, 277(41), 38205–38211.
Zhong, H., et al. (2000). Modulation of hypoxia-inducible factor 1alpha expression by the epidermal growth factor/phosphatidylinositol 3-kinase/PTEN/AKT/FRAP pathway in human prostate cancer cells: Implications for tumor angiogenesis and therapeutics. Cancer Research, 60(6), 1541–1545.
Sang, N., et al. (2003). MAPK signaling up-regulates the activity of hypoxia-inducible factors by its effects on p300. The Journal of Biological Chemistry, 278(16), 14013–14019.
Mylonis, I., et al. (2006). Identification of MAPK phosphorylation sites and their role in the localization and activity of hypoxia-inducible factor-1alpha. The Journal of Biological Chemistry, 281(44), 33095–33106.
Page, E. L., et al. (2002). Induction of hypoxia-inducible factor-1alpha by transcriptional and translational mechanisms. The Journal of Biological Chemistry, 277(50), 48403–48409.
Kalousi, A., et al. (2010). Casein kinase 1 regulates human hypoxia-inducible factor HIF-1. Journal of Cell Science, 123(Pt 17), 2976–2986.
To, K. K., et al. (2006). The phosphorylation status of PAS-B distinguishes HIF-1alpha from HIF-2alpha in NBS1 repression. The EMBO Journal, 25(20), 4784–4794.
Maxwell, P. H., et al. (1999). The tumour suppressor protein VHL targets hypoxia-inducible factors for oxygen-dependent proteolysis. Nature, 399(6733), 271–275.
Mailloux, R. J., Puiseux-Dao, S., & Appanna, V. D. (2009). Alpha-ketoglutarate abrogates the nuclear localization of HIF-1alpha in aluminum-exposed hepatocytes. Biochimie, 91(3), 408–415.
Lando, D., et al. (2002). FIH-1 is an asparaginyl hydroxylase enzyme that regulates the transcriptional activity of hypoxia-inducible factor. Genes & Development, 16(12), 1466–1471.
Berra, E., et al. (2003). HIF prolyl-hydroxylase 2 is the key oxygen sensor setting low steady-state levels of HIF-1alpha in normoxia. The EMBO Journal, 22(16), 4082–4090.
Jaakkola, P., et al. (2001). Targeting of HIF-alpha to the von Hippel-Lindau ubiquitylation complex by O2-regulated prolyl hydroxylation. Science, 292(5516), 468–472.
Schofield, C. J., & Ratcliffe, P. J. (2005). Signalling hypoxia by HIF hydroxylases. Biochemical and Biophysical Research Communications, 338(1), 617–626.
Koivunen, P., et al. (2007). An endoplasmic reticulum transmembrane prolyl 4-hydroxylase is induced by hypoxia and acts on hypoxia-inducible factor alpha. The Journal of Biological Chemistry, 282(42), 30544–30552.
Hewitson, K. S., et al. (2002). Hypoxia-inducible factor (HIF) asparagine hydroxylase is identical to factor inhibiting HIF (FIH) and is related to the cupin structural family. The Journal of Biological Chemistry, 277(29), 26351–26355.
Lee, C., et al. (2003). Structure of human FIH-1 reveals a unique active site pocket and interaction sites for HIF-1 and von Hippel-Lindau. The Journal of Biological Chemistry, 278(9), 7558–7563.
Soni, S., & Padwad, Y. S. (2017). HIF-1 in cancer therapy: Two decade long story of a transcription factor. Acta Oncologica, 56(4), 503–515.
Lim, J. H., et al. (2010). Sirtuin 1 modulates cellular responses to hypoxia by deacetylating hypoxia-inducible factor 1alpha. Molecular Cell, 38(6), 864–878.
Chandel, N. S., et al. (1998). Mitochondrial reactive oxygen species trigger hypoxia-induced transcription. Proceedings of the National Academy of Sciences of the United States of America, 95(20), 11715–11720.
Chandel, N. S., et al. (2000). Reactive oxygen species generated at mitochondrial complex III stabilize hypoxia-inducible factor-1alpha during hypoxia: A mechanism of O2 sensing. The Journal of Biological Chemistry, 275(33), 25130–25138.
Schroedl, C., et al. (2002). Hypoxic but not anoxic stabilization of HIF-1alpha requires mitochondrial reactive oxygen species. American Journal of Physiology. Lung Cellular and Molecular Physiology, 283(5), L922–L931.
Gerald, D., et al. (2004). JunD reduces tumor angiogenesis by protecting cells from oxidative stress. Cell, 118(6), 781–794.
Kimura, H., et al. (2000). Hypoxia response element of the human vascular endothelial growth factor gene mediates transcriptional regulation by nitric oxide: Control of hypoxia-inducible factor-1 activity by nitric oxide. Blood, 95(1), 189–197.
Palmer, L. A., Gaston, B., & Johns, R. A. (2000). Normoxic stabilization of hypoxia-inducible factor-1 expression and activity: Redox-dependent effect of nitrogen oxides. Molecular Pharmacology, 58(6), 1197–1203.
Sandau, K. B., Faus, H. G., & Brune, B. (2000). Induction of hypoxia-inducible-factor 1 by nitric oxide is mediated via the PI 3K pathway. Biochemical and Biophysical Research Communications, 278(1), 263–267.
Sandau, K. B., Fandrey, J., & Brune, B. (2001). Accumulation of HIF-1alpha under the influence of nitric oxide. Blood, 97(4), 1009–1015.
Liu, Y., et al. (1998). Carbon monoxide and nitric oxide suppress the hypoxic induction of vascular endothelial growth factor gene via the 5′ enhancer. The Journal of Biological Chemistry, 273(24), 15257–15262.
Sogawa, K., et al. (1998). Inhibition of hypoxia-inducible factor 1 activity by nitric oxide donors in hypoxia. Proceedings of the National Academy of Sciences of the United States of America, 95(13), 7368–7373.
Yin, J. H., et al. (2000). iNOS expression inhibits hypoxia-inducible factor-1 activity. Biochemical and Biophysical Research Communications, 279(1), 30–34.
Wenger, R. H., Stiehl, D. P., & Camenisch, G. (2005). Integration of oxygen signaling at the consensus HRE. Science’s STKE, 2005(306), re12.
Semenza, G. L., et al. (1994). Transcriptional regulation of genes encoding glycolytic enzymes by hypoxia-inducible factor 1. The Journal of Biological Chemistry, 269(38), 23757–23763.
Jiang, B. H., et al. (1996). Dimerization, DNA binding, and transactivation properties of hypoxia-inducible factor 1. The Journal of Biological Chemistry, 271(30), 17771–17778.
Wenger, R. H. (2000). Mammalian oxygen sensing, signalling and gene regulation. The Journal of Experimental Biology, 203(Pt 8), 1253–1263.
Minchenko, A., et al. (2002). Hypoxia-inducible factor-1-mediated expression of the 6-phosphofructo-2-kinase/fructose-2,6-bisphosphatase-3 (PFKFB3) gene. Its possible role in the Warburg effect. The Journal of Biological Chemistry, 277(8), 6183–6187.
Hayashi, M., et al. (2004). Induction of glucose transporter 1 expression through hypoxia-inducible factor 1alpha under hypoxic conditions in trophoblast-derived cells. The Journal of Endocrinology, 183(1), 145–154.
Liu, Y., et al. (2009). The expression and significance of HIF-1alpha and GLUT-3 in glioma. Brain Research, 1304, 149–154.
Zhang, H., et al. (2008). Mitochondrial autophagy is an HIF-1-dependent adaptive metabolic response to hypoxia. The Journal of Biological Chemistry, 283(16), 10892–10903.
Sowter, H. M., et al. (2001). HIF-1-dependent regulation of hypoxic induction of the cell death factors BNIP3 and NIX in human tumors. Cancer Research, 61(18), 6669–6673.
Lu, C. W., et al. (2008). Induction of pyruvate dehydrogenase kinase-3 by hypoxia-inducible factor-1 promotes metabolic switch and drug resistance. The Journal of Biological Chemistry, 283(42), 28106–28114.
Bellot, G., et al. (2009). Hypoxia-induced autophagy is mediated through hypoxia-inducible factor induction of BNIP3 and BNIP3L via their BH3 domains. Molecular and Cellular Biology, 29(10), 2570–2581.
Ivan, M., et al. (2008). Hypoxia response and microRNAs: No longer two separate worlds. Journal of Cellular and Molecular Medicine, 12(5A), 1426–1431.
Devlin, C., et al. (2011). miR-210: More than a silent player in hypoxia. IUBMB Life, 63(2), 94–100.
Chan, S. Y., et al. (2009). MicroRNA-210 controls mitochondrial metabolism during hypoxia by repressing the iron-sulfur cluster assembly proteins ISCU1/2. Cell Metabolism, 10(4), 273–284.
Favaro, E., et al. (2010). MicroRNA-210 regulates mitochondrial free radical response to hypoxia and Krebs cycle in cancer cells by targeting iron sulfur cluster protein ISCU. PLoS One, 5(4), e10345.
Metallo, C. M., et al. (2011). Reductive glutamine metabolism by IDH1 mediates lipogenesis under hypoxia. Nature, 481(7381), 380–384.
Wise, D. R., et al. (2011). Hypoxia promotes isocitrate dehydrogenase-dependent carboxylation of alpha-ketoglutarate to citrate to support cell growth and viability. Proceedings of the National Academy of Sciences of the United States of America, 108(49), 19611–19616.
Du, W., et al. (2017). HIF drives lipid deposition and cancer in ccRCC via repression of fatty acid metabolism. Nature Communications, 8(1), 1769.
Griffiths, J. R., et al. (2002). Metabolic changes detected by in vivo magnetic resonance studies of HEPA-1 wild-type tumors and tumors deficient in hypoxia-inducible factor-1beta (HIF-1beta): Evidence of an anabolic role for the HIF-1 pathway. Cancer Research, 62(3), 688–695.
Younes, M., Lechago, L. V., & Lechago, J. (1996). Overexpression of the human erythrocyte glucose transporter occurs as a late event in human colorectal carcinogenesis and is associated with an increased incidence of lymph node metastases. Clinical Cancer Research, 2(7), 1151–1154.
Semenza, G. L. (2009). Regulation of cancer cell metabolism by hypoxia-inducible factor 1. Seminars in Cancer Biology, 19(1), 12–16.
Pinheiro, C., et al. (2012). Role of monocarboxylate transporters in human cancers: State of the art. Journal of Bioenergetics and Biomembranes, 44(1), 127–139.
Chiche, J., Brahimi-Horn, M. C., & Pouyssegur, J. (2010). Tumour hypoxia induces a metabolic shift causing acidosis: A common feature in cancer. Journal of Cellular and Molecular Medicine, 14(4), 771–794.
Swietach, P., et al. (2008). Tumor-associated carbonic anhydrase 9 spatially coordinates intracellular pH in three-dimensional multicellular growths. The Journal of Biological Chemistry, 283(29), 20473–20483.
Gatenby, R. A., et al. (2007). Cellular adaptations to hypoxia and acidosis during somatic evolution of breast cancer. British Journal of Cancer, 97(5), 646–653.
Christofk, H. R., et al. (2008). The M2 splice isoform of pyruvate kinase is important for cancer metabolism and tumour growth. Nature, 452(7184), 230–233.
Luo, W., et al. (2011). Pyruvate kinase M2 is a PHD3-stimulated coactivator for hypoxia-inducible factor 1. Cell, 145(5), 732–744.
Gao, X., et al. (2012). Pyruvate kinase M2 regulates gene transcription by acting as a protein kinase. Molecular Cell, 45(5), 598–609.
Dvorak, H. F. (1986). Tumors: Wounds that do not heal. Similarities between tumor stroma generation and wound healing. The New England Journal of Medicine, 315(26), 1650–1659.
Vaupel, P., Schaefer, C., & Okunieff, P. (1994). Intracellular acidosis in murine fibrosarcomas coincides with ATP depletion, hypoxia, and high levels of lactate and total pi. NMR in Biomedicine, 7(3), 128–136.
Denko, N. C., & Giaccia, A. J. (2001). Tumor hypoxia, the physiological link between Trousseau’s syndrome (carcinoma-induced coagulopathy) and metastasis. Cancer Research, 61(3), 795–798.
Vaupel, P., & Mayer, A. (2014). Hypoxia in tumors: Pathogenesis-related classification, characterization of hypoxia subtypes, and associated biological and clinical implications. Advances in Experimental Medicine and Biology, 812, 19–24.
Zhong, H., et al. (1999). Overexpression of hypoxia-inducible factor 1alpha in common human cancers and their metastases. Cancer Research, 59(22), 5830–5835.
Talks, K. L., et al. (2000). The expression and distribution of the hypoxia-inducible factors HIF-1alpha and HIF-2alpha in normal human tissues, cancers, and tumor-associated macrophages. The American Journal of Pathology, 157(2), 411–421.
Koshikawa, N., et al. (2003). Constitutive upregulation of hypoxia-inducible factor-1alpha mRNA occurring in highly metastatic lung carcinoma cells leads to vascular endothelial growth factor overexpression upon hypoxic exposure. Oncogene, 22(43), 6717–6724.
Hockel, M., et al. (1996). Hypoxia and radiation response in human tumors. Seminars in Radiation Oncology, 6(1), 3–9.
Hockel, M., et al. (1998). Tumor hypoxia in pelvic recurrences of cervical cancer. International Journal of Cancer, 79(4), 365–369.
Hockel, M., et al. (1999). Hypoxic cervical cancers with low apoptotic index are highly aggressive. Cancer Research, 59(18), 4525–4528.
Semenza, G. L. (2011). Oxygen sensing, homeostasis, and disease. The New England Journal of Medicine, 365(6), 537–547.
Doedens, A. L., et al. (2010). Macrophage expression of hypoxia-inducible factor-1 alpha suppresses T-cell function and promotes tumor progression. Cancer Research, 70(19), 7465–7475.
Takeda, N., et al. (2010). Differential activation and antagonistic function of HIF-{alpha} isoforms in macrophages are essential for NO homeostasis. Genes & Development, 24(5), 491–501.
Noman, M. Z., et al. (2014). PD-L1 is a novel direct target of HIF-1α, and its blockade under hypoxia enhanced MDSC-mediated T cell activation. The Journal of Experimental Medicine, 211(5), 781–790.
Lee, J. H., et al. (2015). E3 ubiquitin ligase VHL regulates hypoxia-inducible factor-1α to maintain regulatory T cell stability and suppressive capacity. Immunity, 42(6), 1062–1074.
Okegawa, T., et al. (2004). The role of cell adhesion molecule in cancer progression and its application in cancer therapy. Acta Biochimica Polonica, 51(2), 445–457.
Cowden Dahl, K. D., et al. (2005). Hypoxia-inducible factor regulates alphavbeta3 integrin cell surface expression. Molecular Biology of the Cell, 16(4), 1901–1912.
Ryu, M. H., et al. (2010). Hypoxia-inducible factor-1alpha mediates oral squamous cell carcinoma invasion via upregulation of alpha5 integrin and fibronectin. Biochemical and Biophysical Research Communications, 393(1), 11–15.
Lee, S. H., Lee, Y. J., & Han, H. J. (2011). Role of hypoxia-induced fibronectin-integrin beta1 expression in embryonic stem cell proliferation and migration: Involvement of PI3K/Akt and FAK. Journal of Cellular Physiology, 226(2), 484–493.
Krishnamachary, B., et al. (2006). Hypoxia-inducible factor-1-dependent repression of E-cadherin in von Hippel-Lindau tumor suppressor-null renal cell carcinoma mediated by TCF3, ZFHX1A, and ZFHX1B. Cancer Research, 66(5), 2725–2731.
Zhang, Y., Fan, N., & Yang, J. (2015). Expression and clinical significance of hypoxia-inducible factor 1alpha, snail and E-cadherin in human ovarian cancer cell lines. Molecular Medicine Reports, 12(3), 3393–3399.
Barak, V., et al. (2011). VEGF as a biomarker for metastatic Uveal melanoma in humans. Current Eye Research, 36(4), 386–390.
Semenza, G. L. (2012). Hypoxia-inducible factors: Mediators of cancer progression and targets for cancer therapy. Trends in Pharmacological Sciences, 33(4), 207–214.
Hasan, N. M., et al. (1998). Hypoxia facilitates tumour cell detachment by reducing expression of surface adhesion molecules and adhesion to extracellular matrices without loss of cell viability. British Journal of Cancer, 77(11), 1799–1805.
Peng, J. K., et al. (2018). Etaypoxia-inducible factor 1-alpha promotes colon cell proliferation and migration by upregulating AMPK-related protein kinase 5 under hypoxic conditions. Oncology Letters, 15(3), 3639–3645.
Suzuki, A., et al. (2003). ARK5 suppresses the cell death induced by nutrient starvation and death receptors via inhibition of caspase 8 activation, but not by chemotherapeutic agents or UV irradiation. Oncogene, 22(40), 6177–6182.
Suzuki, A., et al. (2004). Regulation of caspase-6 and FLIP by the AMPK family member ARK5. Oncogene, 23(42), 7067–7075.
Lu, S., et al. (2013). ARK5 promotes glioma cell invasion, and its elevated expression is correlated with poor clinical outcome. European Journal of Cancer, 49(3), 752–763.
Lester, R. D., et al. (2005). Erythropoietin promotes MCF-7 breast cancer cell migration by an ERK/mitogen-activated protein kinase-dependent pathway and is primarily responsible for the increase in migration observed in hypoxia. The Journal of Biological Chemistry, 280(47), 39273–39277.
Cannito, S., et al. (2008). Redox mechanisms switch on hypoxia-dependent epithelial-mesenchymal transition in cancer cells. Carcinogenesis, 29(12), 2267–2278.
Matsuoka, J., et al. (2013). Hypoxia stimulates the EMT of gastric cancer cells through autocrine TGFbeta signaling. PLoS One, 8(5), e62310.
Yang, M. H., et al. (2008). Direct regulation of TWIST by HIF-1alpha promotes metastasis. Nature Cell Biology, 10(3), 295–305.
Lendahl, U., et al. (2009). Generating specificity and diversity in the transcriptional response to hypoxia. Nature Reviews Genetics, 10(12), 821–832.
Tsai, Y. P., & Wu, K. J. (2012). Hypoxia-regulated target genes implicated in tumor metastasis. Journal of Biomedical Science, 19, 102.
Chu, C. Y., et al. (2016). CA IX is upregulated in CoCl2-induced hypoxia and associated with cell invasive potential and a poor prognosis of breast cancer. International Journal of Oncology, 48(1), 271–280.
Evans, A. J., et al. (2007). VHL promotes E2 box-dependent E-cadherin transcription by HIF-mediated regulation of SIP1 and snail. Molecular and Cellular Biology, 27(1), 157–169.
de Herreros, A. G., et al. (2010). Snail family regulation and epithelial mesenchymal transitions in breast cancer progression. Journal of Mammary Gland Biology and Neoplasia, 15(2), 135–147.
Luo, Y., et al. (2006). Over-expression of hypoxia-inducible factor-1alpha increases the invasive potency of LNCaP cells in vitro. BJU International, 98(6), 1315–1319.
O’Toole, E. A., et al. (2008). Hypoxia induces epidermal keratinocyte matrix metalloproteinase-9 secretion via the protein kinase C pathway. Journal of Cellular Physiology, 214(1), 47–55.
Lin, M. T., et al. (2008). Involvement of hypoxia-inducing factor-1alpha-dependent plasminogen activator inhibitor-1 up-regulation in Cyr61/CCN1-induced gastric cancer cell invasion. The Journal of Biological Chemistry, 283(23), 15807–15815.
Buchler, P., et al. (2009). Transcriptional regulation of urokinase-type plasminogen activator receptor by hypoxia-inducible factor 1 is crucial for invasion of pancreatic and liver cancer. Neoplasia, 11(2), 196–206.
Pennacchietti, S., et al. (2003). Hypoxia promotes invasive growth by transcriptional activation of the met protooncogene. Cancer Cell, 3(4), 347–361.
Ishikawa, T., et al. (2009). Hypoxia enhances CXCR4 expression by activating HIF-1 in oral squamous cell carcinoma. Oncology Reports, 21(3), 707–712.
Li, Y., et al. (2009). Hypoxia induced CCR7 expression via HIF-1alpha and HIF-2alpha correlates with migration and invasion in lung cancer cells. Cancer Biology & Therapy, 8(4), 322–330.
Erler, J. T., et al. (2006). Lysyl oxidase is essential for hypoxia-induced metastasis. Nature, 440(7088), 1222–1226.
Funasaka, T., et al. (2005). Regulation of phosphoglucose isomerase/autocrine motility factor expression by hypoxia. The FASEB Journal, 19(11), 1422–1430.
Staller, P., et al. (2003). Chemokine receptor CXCR4 downregulated by von Hippel-Lindau tumour suppressor pVHL. Nature, 425(6955), 307–311.
Pan, J., et al. (2006). Stromal derived factor-1 (SDF-1/CXCL12) and CXCR4 in renal cell carcinoma metastasis. Molecular Cancer, 5, 56.
Castillo Bennett, J., et al. (2018). Hypoxia-induced Caveolin-1 expression promotes migration and invasion of tumor cells. Current Molecular Medicine, 18(4), 199–206.
Krishnamachary, B., et al. (2003). Regulation of colon carcinoma cell invasion by hypoxia-inducible factor 1. Cancer Research, 63(5), 1138–1143.
Nikitenko, L. L., et al. (2003). Transcriptional regulation of the CRLR gene in human microvascular endothelial cells by hypoxia. The FASEB Journal, 17(11), 1499–1501.
Pugh, C. W., & Ratcliffe, P. J. (2003). Regulation of angiogenesis by hypoxia: Role of the HIF system. Nature Medicine, 9(6), 677–684.
Kotch, L. E., et al. (1999). Defective vascularization of HIF-1alpha-null embryos is not associated with VEGF deficiency but with mesenchymal cell death. Developmental Biology, 209(2), 254–267.
Maruggi, M., et al. (2019). Absence of HIF1A leads to glycogen accumulation and an inflammatory response that enables pancreatic tumor growth. Cancer Research, 79(22), 5839–5848.
Cheng, J., et al. (2007). SUMO-specific protease 1 is essential for stabilization of HIF1alpha during hypoxia. Cell, 131(3), 584–595.
Xu, Y., et al. (2010). Induction of SENP1 in endothelial cells contributes to hypoxia-driven VEGF expression and angiogenesis. The Journal of Biological Chemistry, 285(47), 36682–36688.
Riva, C., et al. (1998). Cellular physiology and molecular events in hypoxia-induced apoptosis. Anticancer Research, 18(6b), 4729–4736.
Hammond, E. M., Dorie, M. J., & Giaccia, A. J. (2003). ATR/ATM targets are phosphorylated by ATR in response to hypoxia and ATM in response to reoxygenation. The Journal of Biological Chemistry, 278(14), 12207–12213.
Akakura, N., et al. (2001). Constitutive expression of hypoxia-inducible factor-1alpha renders pancreatic cancer cells resistant to apoptosis induced by hypoxia and nutrient deprivation. Cancer Research, 61(17), 6548–6554.
Carmeliet, P., et al. (1998). Role of HIF-1alpha in hypoxia-mediated apoptosis, cell proliferation and tumour angiogenesis. Nature, 394(6692), 485–490.
Santore, M. T., et al. (2002). Anoxia-induced apoptosis occurs through a mitochondria-dependent pathway in lung epithelial cells. American Journal of Physiology. Lung Cellular and Molecular Physiology, 282(4), L727–L734.
Kumar, H., & Choi, D. K. (2015). Hypoxia inducible factor pathway and physiological adaptation: A cell survival pathway? Mediators of Inflammation, 2015, 584758.
McClintock, D. S., et al. (2002). Bcl-2 family members and functional electron transport chain regulate oxygen deprivation-induced cell death. Molecular and Cellular Biology, 22(1), 94–104.
Yoo, B. H., et al. (2009). Hypoxia-induced downregulation of autophagy mediator Beclin 1 reduces the susceptibility of malignant intestinal epithelial cells to hypoxia-dependent apoptosis. Autophagy, 5(8), 1166–1179.
Soengas, M. S., et al. (1999). Apaf-1 and caspase-9 in p53-dependent apoptosis and tumor inhibition. Science, 284(5411), 156–159.
Li, F., et al. (2015). Curcumin induces p53-independent necrosis in H1299 cells via a mitochondria-associated pathway. Molecular Medicine Reports, 12(5), 7806–7814.
Shimizu, S., et al. (1995). Prevention of hypoxia-induced cell death by Bcl-2 and Bcl-xL. Nature, 374(6525), 811–813.
Kim, J. Y., et al. (2004). BH3-only protein Noxa is a mediator of hypoxic cell death induced by hypoxia-inducible factor 1alpha. The Journal of Experimental Medicine, 199(1), 113–124.
Zagzag, D., et al. (2000). Expression of hypoxia-inducible factor 1alpha in brain tumors: Association with angiogenesis, invasion, and progression. Cancer, 88(11), 2606–2618.
Schindl, M., et al. (2002). Overexpression of hypoxia-inducible factor 1alpha is associated with an unfavorable prognosis in lymph node-positive breast cancer. Clinical Cancer Research, 8(6), 1831–1837.
Bos, R., et al. (2003). Levels of hypoxia-inducible factor-1alpha independently predict prognosis in patients with lymph node negative breast carcinoma. Cancer, 97(6), 1573–1581.
Aebersold, D. M., et al. (2001). Expression of hypoxia-inducible factor-1alpha: A novel predictive and prognostic parameter in the radiotherapy of oropharyngeal cancer. Cancer Research, 61(7), 2911–2916.
Beasley, N. J., et al. (2002). Hypoxia-inducible factors HIF-1alpha and HIF-2alpha in head and neck cancer: Relationship to tumor biology and treatment outcome in surgically resected patients. Cancer Research, 62(9), 2493–2497.
Koukourakis, M. I., et al. (2002). Hypoxia-inducible factor (HIF1A and HIF2A), angiogenesis, and chemoradiotherapy outcome of squamous cell head-and-neck cancer. International Journal of Radiation Oncology, Biology, Physics, 53(5), 1192–1202.
Birner, P., et al. (2001). Expression of hypoxia-inducible factor 1alpha in epithelial ovarian tumors: Its impact on prognosis and on response to chemotherapy. Clinical Cancer Research, 7(6), 1661–1668.
Zhang, X., et al. (2019). Interaction between p53 and Ras signaling controls cisplatin resistance via HDAC4- and HIF-1alpha-mediated regulation of apoptosis and autophagy. Theranostics, 9(4), 1096–1114.
Jiang, X., et al. (2019). The correlation between NEDD4L and HIF-1alpha levels as a gastric cancer prognostic marker. International Journal of Medical Sciences, 16(11), 1517–1524.
Koukourakis, M. I., et al. (2001). Hypoxia inducible factor (HIF-1a and HIF-2a) expression in early esophageal cancer and response to photodynamic therapy and radiotherapy. Cancer Research, 61(5), 1830–1832.
Wigerup, C., Pahlman, S., & Bexell, D. (2016). Therapeutic targeting of hypoxia and hypoxia-inducible factors in cancer. Pharmacology & Therapeutics, 164, 152–169.
Masoud, G. N., & Li, W. (2015). HIF-1alpha pathway: Role, regulation and intervention for cancer therapy. Acta Pharmaceutica Sinica B, 5(5), 378–389.
Hu, Y., Liu, J., & Huang, H. (2013). Recent agents targeting HIF-1alpha for cancer therapy. Journal of Cellular Biochemistry, 114(3), 498–509.
Falchook, G. S., et al. (2014). Targeting hypoxia-inducible factor-1alpha (HIF-1alpha) in combination with antiangiogenic therapy: A phase I trial of bortezomib plus bevacizumab. Oncotarget, 5(21), 10280–10292.
Ban, H. S., et al. (2016). Hypoxia-inducible factor (HIF) inhibitors: A patent survey (2011–2015). Expert Opinion on Therapeutic Patents, 26(3), 309–322.
Author information
Authors and Affiliations
Corresponding authors
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Elzakra, N., Kim, Y. (2021). HIF-1α Metabolic Pathways in Human Cancer. In: Hu, S. (eds) Cancer Metabolomics. Advances in Experimental Medicine and Biology, vol 1280. Springer, Cham. https://doi.org/10.1007/978-3-030-51652-9_17
Download citation
DOI: https://doi.org/10.1007/978-3-030-51652-9_17
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-51651-2
Online ISBN: 978-3-030-51652-9
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)