
Abstract
This chapter focuses on mesenchymal stem cells (MSCs), a multipotent stem cell type that has been found in a variety of tissues and organs of the human body since their discovery in 1970. Their main function is to maintain and repair the respective tissue in vivo. Mesenchymal stem cells can be easily isolated from different tissues and can undergo extensive self-proliferation prior to differentiation into various mesodermal cell types such as osteoblasts, chondrocytes, adipocytes, tenocytes, myocytes, and fibroblasts. Because of this vast differentiation potential, mesenchymal stem cells are a promising tool for regenerative medicine approaches. They could play an important role in cellular therapy, tissue replacement and regeneration in the future. Mesenchymal stem cells will be compared for their application and differentiation potential to embryonic stem cells and induced pluripotent stem cells and the limitations and challenges using scaffolds for tissue repair will be presented. In addition, legal and ethical aspects of the use of mesenchymal stem cells will be discussed. Moreover, isolation protocols for mesenchymal stem cells from the most common sources namely bone marrow, adipose tissue and umbilical cord are included.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



This chapter focuses on mesenchymal stem cells (MSCs), a multipotent stem cell type that has been found in a variety of tissues and organs of the human body since their discovery in 1970. Their main function is to maintain and repair the respective tissue in vivo. Mesenchymal stem cells can be easily isolated from different tissues and can undergo extensive self-proliferation prior to differentiation into various mesodermal cell types such as osteoblasts, chondrocytes, adipocytes, tenocytes, myocytes, and fibroblasts. Because of this vast differentiation potential, mesenchymal stem cells are a promising tool for regenerative medicine approaches. They could play an important role in cellular therapy, tissue replacement and regeneration in the future. Mesenchymal stem cells will be compared for their application and differentiation potential to embryonic stem cells and induced pluripotent stem cells and the limitations and challenges using scaffolds for tissue repair will be presented. In addition, legal and ethical aspects of the use of mesenchymal stem cells will be discussed.
Moreover, isolation protocols for mesenchymal stem cells from the most common sources namely bone marrow, adipose tissue and umbilical cord are included.
2.1 Localization, Characterization and Storage of Mesenchymal Stem Cells
A stem cell is an unspecialized cell that has the ability for self-renewal for a long time period with or without senescence and for differentiation into cells of various lineages (Till and McCulloch 1961; Gordon 1972), generally. Stem cells can have diverse plasticity. Totipotent stem cells from the fertilized egg can give rise to a complete organism and in addition to the extra embryonal tissues, while pluripotent stem cells like embryonic stem cells (ESCs) and induced pluripotent stem cells (iPSCs) can differentiate into any cell type from all three germ layers but can not form an organism without transferring them into a blastocyst (Hanna et al. 2010). By contrast, the most commonly known adult stem cells, the mesenchymal stem cells (MSCs) and hematopoietic stem cells (HSCs), have a more limited differentiation potential and are thus called multipotent. As the name suggests, MSCs can give rise to several cell types of the mesenchyme which is derived from the mesoderm during development. They form then cell types from bone, muscle, and cartilage but also to cells from tissue of other origin (◘ Fig. 2.1) (Pittenger et al. 1999; Pansky et al. 2007).

Major sources and differentiation linages of MSCs. The main isolation sources are bone marrow of the iliac crest, subcutaneous adipose tissue and Wharton’s jelly from umbilical cord (shown with arrows). Mesenchymal stem cells from diverse tissues can have a different plasticity and might be pre-committed already towards different lineages (depicted with different colors of the MSCs). The acknowledged differentiation potential of MSCs is shown in the lower part of the figure
Mesenchymal stem cells were first discovered by Friedenstein in 1970 (1970). He and his research team were interested in isolating hematopoietic stem cells (HSCs) from bone marrow as a treatment for leukemia and thereby found an unknown cell type. This unknown cell type seemed to be responsible for the microenvironment typical for hematopoietic tissue (Friedenstein et al. 1974), and today it’s known that it is a major part of the HSC niche. Due to the capacity of these cells to form stromal tissue, they named them “stromal precursors” (Friedenstein et al. 1970). Later the term “mesenchymal stromal cells” was established (Prockop 1997; Baksh et al. 2004).
In the last years, it was discussed whether mesenchymal stem cells are actually stem cells or just stromal precursors. That MSCs were first found exclusively in the connective tissue and that they influence the surrounding cells are among the strongest arguments towards conserving the name “mesenchymal stromal cells”. The most prominent argument to name them mesenchymal stem cells is their capacity to differentiate into several lineages. The reason that they can be found in so many tissues are that they are needed for maintenance and repair. The idea to use the same mechanism artificially to replace tissues or even organs came up. It had been expected that this will work similar to the treatment of certain cancers such as leukemia and other diseases using hematopoietic stem cell transplantation.
As mentioned, MSCs were first found in the bone marrow a semi-solid tissue (Friedenstein et al. 1970), which has high cell turnover and regeneration rate. Later, it was discovered that other tissues with high cell turnover and regeneration rate like the epidermis (Rheinwald and Green 1975; Huang et al. 2013; Salerno et al. 2017) and the intestinal tissue (Lanzoni et al. 2009) also possess MSCs. So, scientist thought that those are the prerequisites for tissues to have the cells. Much later, scientists found that MSCs could also be isolated from fat tissue where cells have a low cell turnover and a high regeneration rate (Zuk et al. 2002). Finally, MSCs were also found in tissues of organs with a low cell turnover and a low regeneration rate like the kidney (Bruno et al. 2009). Besides the mentioned tissues, there are further sources where MSCs can be isolated from, such as dental pulp (Alkhalil et al. 2015) or follicle (Haddouti et al. 2009), peripheral blood (Cao et al. 2005), hair follicle (Liu et al. 2010) and several neonatal tissues (da Silva Meirelles et al. 2006) such as umbilical cord (Lee et al. 2004), Wharton’s jelly (Wang et al. 2004), amniotic fluid (Steigmann and Fauza 2007; Moraghebi et al. 2017), and placenta (In’t Anker et al. 2004). The vast differentiation potential makes them a promising stem cell type for use in regenerative medicine.
In response to the recent unraveled series of MSC sources and isolation procedures from various tissue types, combined with an interest in MSCs for research and application in regenerative medicine, the Mesenchymal and Tissue Stem Cell Committee of the International Society for Cellular Therapy proposed a set of minimal criteria to define MSCs. The first criterion is that MSCs must adhere to plastic, which also simplifies the isolation procedure. As they unfortunately resemble fibroblasts, the expression (higher than 95%) of at least three specific markers on the cell surface, i.e. cluster of differentiation (CD)73, CD90, CD105 and CD133 and the lack expression (lower than 5%) of surface markers like CD14, CD34, CD45 or CD11b, CD19 or CD79α and human leucocyte antigen-DR (HLA-DR) defines the second criterion. The third criterion demands that MSCs possess the ability for differentiation into osteoblasts, adipocytes, and chondrocytes in vitro confirmed by specific staining usually Alizarin Red S, Oil Red O, and Alcian Blue (Horwitz et al. 2005; Dominici et al. 2006). These features should be valid for all MSCs, however there are some differences existing between MSCs isolated from diverse tissues.
In line with the promising prospect that MSCs might be used for tissue and organ repair or replacement in the future also a new business model came up. Parents can use the offer of companies to cryopreserve mesenchymal stem cells isolated from Wharton’s jelly of the umbilical cord, cord blood, and placenta of their newborn child to store them. Solely for the potential use by the child or the donor family members. These MSCs are advantageous due to their early age due to e.g. long telomeres. On the other hand, those cells can also be donated to be collected in stem cell banks for future research and use.
To ensure the safety and efficacy of the cells during banking and cryopreservation, optimal conditions for cryopreservation must be selected, for further detail see Ullah and co-workers (2015).
For efficient storage there must be an optimal cryopreservation medium as well as a defined (1 °C/min) constant and strict drop in temperature as for other cells as well (Thirumala et al. 2005) using a controlled rate freezer or other appropriate storage devices (Ullah et al. 2015). Due to the possible impact with new approaches for various treatments in regenerative medicine, the Food and Drug Administration (FDA) in the U.S.A. and the European Medicines Agency (EMA) in Europe take responsibility by monitoring the large-scale banking next to supervising MSC based cell therapy products (Hourd et al. 2008).
2.2 Mesenchymal Stem Cells in Regenerative Medicine
2.2.1 The Application of Mesenchymal Stem Cells
MSCs are promising tools in the field of regenerative medicine (Tobiasch 2008), so approaches for the clinical use of mesenchymal stem cells are in progress. The number of clinical trials using mesenchymal stem cells has risen over the last years. Currently there are 711 registered clinical trials in different clinical phases (phase I, II, III, IV) worldwide, exhibiting the huge potential of MSC-based cell therapy (► www.clinicaltrials.gov).
Most of these clinical trials are still in the early stages phase I or II. Only few clinical trials are in phase III (36 studies) or phase IV (2 studies), the stages preceding the potential use in regenerative medicine such as tissue engineering to the replacement or reconstruction of damaged human tissues. Clinical trials using mesenchymal stem cells encompass many different diseases. The most common diseases registered for cell therapy with mesenchymal stem cells are shown in ◘ Fig. 2.2.

Percentage distribution of clinical trials with mesenchymal stem cells. There are 711 clinical trials for different diseases in phase I – IV ongoing in the world (► www.clinicaltrials.gov). 104 of these clinical trials address cardiovascular disorders, 77 autoimmune diseases, 67 osteoarthritis, 55 liver disorders, 47 respiratory disorders, 43 skin diseases, 36 graft versus host diseases (GvHD), 27 spinal cord injuries, 20 kidney failures and 9 Alzheimer disease. The other diseases include i.e. muscular dystrophies, aplastic anemia, osteogenesis imperfecta, Parkinson’s disease and ulcerative colitis
One example, for a clinical phase III study in Germany is lead by research team of Professor Steinhoff in Rostock. In cooperation with several leading university heart centers, they applied autologous CD133+ bone marrow stem cells intramyocardially during bypass surgery to patients that had a myocardial infarction (heart attack). Following the application of the stem cells, the patients had an improved cardiac function. That led to a positive completion of the clinical trial and the establishment of a reference standard for future cell therapies of this illness (White et al. 2016; Steinhoff et al. 2017).
Another example is a clinical trial with ten patients using MSCs as therapy against spinal cord injuries. In this approach, autologous MSCs were harvested, culturally expanded and injected directly into the spinal cord. After a second injection a few weeks later, the motor power of the upper extremities was improved. Moreover, after a six-month follow-up, none of the patients experienced any permanent complication associated with MSCs transplantation (Park et al. 2012).
Normally new treatments have to enter the marketing-authorization process starting with clinical trials to create a safety profile and dosage guidelines. However, there is also individual medical treatment, where patients after getting sufficient clarification have the chance to receive a treatment which is not authorized yet. In accordance with Declaration of Helsinki from 1964, this is only possible for patients with life-threatening, long-lasting or seriously debilitating illnesses that can not be medicated with any of the currently authorized treatments. In 2011 Prasad and coworkers described the first individual curative trial for the treatment of pediatric patients with acute graft versus host disease (aGvHD) of refractory grades III-IV. Twelve patients that were resistant against steroids and other immunosuppressive therapies received a therapy with allogenic human MSCs. Seven of the patients showed a positive response to the treatment while five did not. The seven responders stayed alive almost 700 days after the treatment and eventually passed away due to other causes such as an irreversible organ failure. From this study the researchers concluded that therapy with human MSCs appears to be a safe and potentially effective treatment for patients with aGvHD (Prasad et al. 2011).
Taken together various researchers try to use mesenchymal stem cells in cell replacement therapies hoping to get similar results as with hematopoietic stem cells for treating e.g. leukemia. However, most therapy approaches do not replace the damaged tissue cells. Some time after the injection of MSCs, there is no trace left of them. They seem to be lost in the liver and lung, and in addition it is postulated that they undergo apoptosis in the tissues, where they should replace the damaged cells. Next to this some MSCs seem to be pre-committed towards specific cell types, resulting in a mixture of various pre-committed stem cells at a specific localization site. Where the mixture composition depends on the tissue it was isolated from. For example, mesenchymal stem cells isolated from dental follicle are pre-committed towards hard tissues (Haddouti et al. 2009; Zippel et al. 2012) such as bone cells, while MSCs isolated from adipose tissue of lower body parts are pre-committed towards soft tissues (Sakaguchi et al. 2005). The purinergic receptor pattern can be a useful tool to uncover whether the MSCs are pre-committed and towards which direction (Zhang et al. 2014; Kaebisch et al. 2015). This pre-commitment might as well be the reason why MSCs in vitro never differentiate to 100% into the required cell type as could be expected. At least a small number of cells stays in the stem cell state. Nevertheless, they seem to be beneficial in clinical trials. So, the question arises – why?
The reason might be that MSCs have a paracrine effect on the surrounding tissue (Cotter et al. 2018; Linero and Chaparro 2014). It was shown in different, previously described studies, that the administration of MSCs prevented injuries and led, in some cases, to tissue recovery (Bartholomew et al. 2002; Herrera et al. 2007; Yao et al. 2016). Next to this MSCs are hardly causing an immunogenic response. MSCs are therefore more often (53.91%) used in autologous (from the patient itself) but also (46.09%) allogenic (from a donor) approaches are promising (► www.clinicaltrials.gov; Haubner et al. 2015). Taken the beneficial effect of MSCs into consideration various studies nowadays take a new approach by using more than cell type for replacements. They either use MSCs differentiated towards the desired tissue type, such as cardiomyocytes and combine these cells with e.g. fibroblasts or undifferentiated MSCs.
However not only MSCs are used in regenerative medicine. Other stem cell types like embryonic stem cells (ESCs) and induced pluripotent stem cells (iPSCs) can be used as well.
2.2.2 Pros and Cons of Mesenchymal Stem Cells Compared to Embryonic Stem Cells and Induced Pluripotent Stem Cell
Next to multipotent mesenchymal stem cells, there are two pluripotent stem cell types often used in regenerative medicine: embryonic stem cells (ESCs) and induced pluripotent stem cells (iPSCs). ESCs are generated by isolating the cells of the inner cell mass of a blastocyst from an early embryo (around day five to seven). However, the generation of ESCs arises ethical issues (Evans and Kaufman 1981; Thomson et al. 1998). Since 2006 there is an artificial method creating very similar cells by reprogramming adult somatic cell using the four Yamanaka transcription factors Oct3/4, Sox2, Klf4 and c-Myc or the Thomson factors Oct3/4, Sox2, Nanog, Lin28 (Takahashi and Yamanaka 2006; Takahashi et al. 2007; Yu et al. 2007; Nakagawa et al. 2008).
Embryonic stem cells are the original and therefore the gold standard to understand early development, and also diseases where they play a role. Due to their higher plasticity compared to MSCs, some scientists claim that they are needed for the replacement of cells and tissues which can not be differentiated from less plastic cells such as MSCs. A commonly mature cell type where this is claimed are nervous. However, as ESCs also do not all differentiate in vitro, they also pertain to the increased risk for cancer development, particularly teratomas.
The induced pluripotent stem cell type has the advantage that it can be obtained from the patient himself and thus cause only little unwanted immunogenic reactions and hardly any ethical issues. They do have, similar to ESCs, the high potential being able to differentiate into all tissues of an organism, but related to this, also the high risk for teratoma formation. In addition, if retroviruses are used to express the mentioned transcription factors their use increase the risk for cancerogenesis due to random integration into the genome. Another risk is that this cell type is barely understood today. It was only recently unraveled that their epigenetic pattern is different to ESCs, specifically a mixture of the initial cell type and ESC.
Nevertheless, today 121 clinical studies are on the way with ESCs (in the USA) and 21 studies have been tested using iPSCs. Two of them used in 2018 iPSCs for spinal cord injury and for macular degeneration (► www.clinicaltrials.gov; Tsuji et al. 2018; Takagi et al. 2018).
2.3 Scaffolds for Tissue Repair in Combination with MSCs
2.3.1 Scaffold Requirement for MSC-Based Tissue Repair
Mesenchymal stem cells are affected by extracellular matrix (ECM) that defines the microenvironment that surrounds them. ECM defines geometry, topography and morphology that the cells are facing. But other molecules with similar properties such as extracellular nucleotides, growth factors and cytokines, for instance transforming growth factor-β (TGF-β), tension induced proteins (TIPs), integrins and transient receptor potential (TRP), can also regulate cytoskeleton tension successively activate a series of mechanical transduction events and thus influence stem cell fate. Mechanical forces such as shear stress and blood pressure influence stem cell proliferation and differentiation as well as chemical and physical factors such as pH or oxygen levels. ◘ Figure 2.3 gives a detailed overview on stem cells and their micro-environment (Schulze and Tobiasch 2012).

Stem cells and their natural micro-environment. There are roughly three groups into which cell-influencing factors can be categorized: physical factors such as shear forces, elasticity and topography, cellular interactions such as immune and nerve cells, nearby blood vessels and neighboring stem cells and biochemical factors such as oxygen, glucose, hormones and growth factors (Schulze and Tobiasch 2012). (Copyright 2012 Springer Verlag)
A scaffold for tissue repair should resemble or mimic original tissue as closely as possible. This means that not only the chemical structure, but also other aspects such as morphology, mechanical properties, technical functionality, stability against physiological conditions and biocompatibility have to be tuned to match the implant site. “Gold standard” for implants are usually autografts: implants taken from another site of the patient itself since they have the lowest adverse effects. However, these grafts are rarely available. Allografts, implants coming from a different donor, are also widely being used, with a limited risk of rejection. But as they also rely on limited donor material, research focuses on synthetic substitute material that should also lower risks of infections or implant rejections (Henkel et al. 2013).
Depending on the tissue that is going to be repaired, a scaffold has to fulfil quite different requirements. A bone scaffold, for instance, has to provide much more mechanical stability than a scaffold for vascular tissue and an implant for tendon repair has to provide both tensile strength and flexibility. Cell attachment and proliferation is crucial for vascularization of the scaffold and a successful implantation.
This may be ensured by choosing cell-friendly, non-cytotoxic materials such as (bio-)ceramics and or (bio-)polymers that have proven to be cytocompatible. Depending on the application, scaffolds can be made of either ceramic or polymer, a composite of both or even certain metals. There have been studies where synthetic polymers (e.g. polycaprolactone, poly lactic acid), polymers from renewable sources (such as polysaccharides or collagen) or copolymers of different types of polymers were used for bone, tendon, vascular tissue and cartilage repair. Many polymers tend to be biocompatible and their flexibility makes them useful candidates with regard to a tunable morphology. However, using only a polymer as scaffold material can also have certain disadvantages. Some polymer materials have rather low cell attachment properties or are not suitable for load bearing applications due to a low stiffness and mechanical resistance. Similarly to polymers, there are different ceramic substances that are being used especially for bone scaffolds, however, most studies use some variation of calcium phosphates. This makes sense, since 70% of original bone is comprised of calcium phosphate. It has great cell attachment properties and high mechanical stiffness although being brittle. Generating scaffolds with a defined hierarchical porosity on the other hand is often challenging. Plus, pure ceramic scaffolds lack the flexibility of polymer scaffolds. This leads to a composite approach, where the advantages of both polymers and ceramics are combined, overcoming most of the individual disadvantages. Here, a polymer is used to create a flexible, porous network, while the ceramic (often calcium phosphates) are added to enhance stability and cell attachment (Schulze and Tobiasch 2012; Henkel et al. 2013; Hielscher et al. 2018).
Additionally, certain drugs or growth factors can be incorporated into the scaffold to accelerate cell differentiation or prevent infections and inflammation. However, drug delivery, especially a sustained release over several days remains a great challenge. Current research focuses on different methods of encapsulation and release of drugs. Basic release mechanisms include: matrix tortuosity-controlled diffusion, membrane-controlled diffusion for small molecules, hydrogel network swelling (◘ Fig. 2.4) and scaffold or capsule degradation (Wong and Choi 2015; Fenton et al. 2018; Witzler et al. 2018).

Examples of controlled release platforms and their materials: a Matrix tortuosity-controlled diffusion out of porous materials; b Membrane-controlled diffusion from capsules and reservoirs; c Hydrogels (Fenton et al. 2018). (Copyright 2018 John Wiley and Sons)
2.3.2 Current Approaches in Scaffold Development
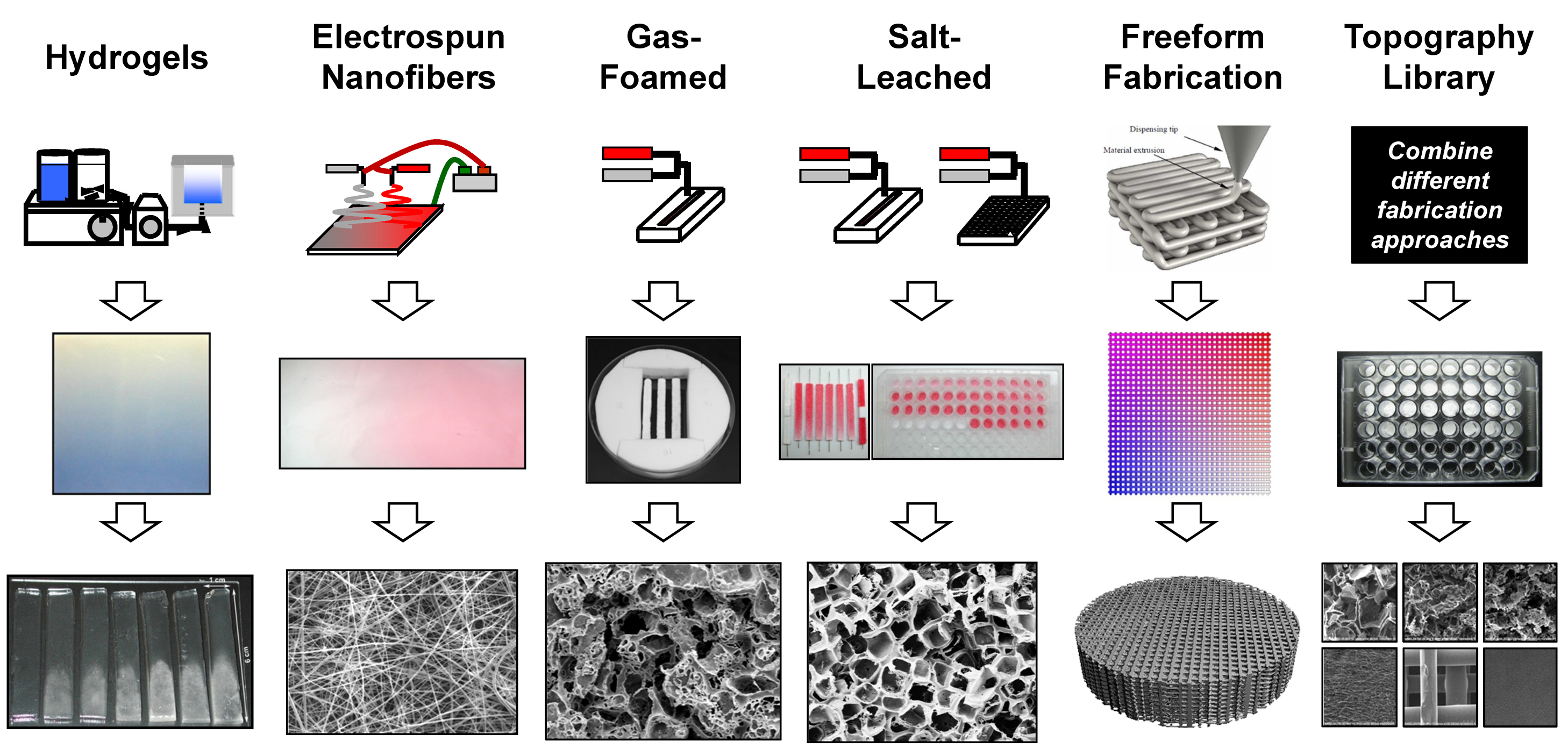
As already mentioned, current approaches in scaffold development focus mainly on composite scaffolds that serve different functions. Most of these are produced using so-called “additive fabrication techniques”. This can range from simple cross-linking and sometimes mineralizing of hydrogels to foams, to electrospinning of fibers and mats and ultimately to freeform fabrication of complete scaffolds (◘ Fig. 2.5). Depending on the fabrication technique, additives (such as drugs or growth factors) can be added directly in the forming process or have to be added in a second step (Grotheer et al. 2014; Velasco et al. 2015; Simon 2018).

Overview on different techniques for additive scaffold manufacturing. (Printed with permission of C.D. Simon Jr. (2018)). Schematic description of the technique (top line), macroscopic result (middle line) and microscale structure of the samples (bottom line)
Hydrogel formation is a simple way of creating a porous polymer network. There are natural polysaccharides such as gelatin and agarose that form hydrogels by simple heating and cooling and there are natural polymers like chitosan and collagen or synthetic polymers such as poly(acrylamide), poly(ethylene glycol) or poly(lactic acid) that have to be somehow crosslinked. By varying concentration and degree of crosslinking, the stiffness of the hydrogel can be tuned. Mineralization of these scaffolds for bone applications then takes place in a second step, either by coating the polymer with ceramic or simply by mixing-in the ceramic particles into the solution prior to gelling. Incorporation of other active ingredients can be achieved by simple adding to the solution (Paris et al. 2015; Hu et al. 2016).
Foaming or leaching processes are also used for generating porous structures. Here, porogens (such as ice crystals, liquid CO2 or salts) are added to the polymer or ceramic paste and removed after hardening of the scaffold by varying temperature, pressure or simple washing steps (Chen et al. 2018).
Electrospinning is often used for fibers and mats or fleeces that can be used for tendon, cartilage and bone applications and are often mineralized in a second step. Polymers, both natural and synthetic, are spun into fibers from a solution by acceleration in an electric field. Depending on the collector of the fiber, single strands or up to large mats of varying thickness can be created. It is also possible to incorporate growth factors or other active ingredients into the scaffold. The resulting porous fleeces can be seeded with cells and have been reported to show improved cell adhesion and proliferation (Rajzer et al. 2017).
Freeform fabrication or “3D printing” is on the rise for creating structures with a well-defined structure and porosity for cell in-growth. There are several possibilities to alter shape, functionality or mechanical properties by choosing different materials for separate sections of the scaffold. Ceramic parts can be added both directly to the printing mass or in a separate mineralization step. Active ingredients may be added directly to the printing feed or have to be added in a later step if the substance is heatsensitive (Grémare et al. 2018). Novel manufacturing techniques have comprehensively been reviewed focusing scaffold development for stem cell-based therapies (Schipper et al. 2017; El Khaldi-Hansen et al. 2017; Ottensmeyer et al. 2018).
2.3.3 Limitations and Challenges of Scaffolds
Current tissue repair research focuses on mimicking original tissue and its properties. While many aspects are already being considered, there are still a lot of limitations and challenges: the “perfect” biocompatible scaffold with ideal porosity, morphology, technical and mechanical properties has still not been created yet. There are also the questions of which cell types and which growth factors will ensure proper vascularization and host integration. Aside from these fundamental challenges there are other things still unknown: what are possible side effects of scaffolds, donor cells and growth factors? What is the most appropriate animal model? Which quality and functionality will the regenerated tissue have and what are its long-terms properties? And then there are of course clinical and regulatory questions: how can a patient-specific scaffold be generated? How to get FDA (and other) approval for these systems? How will the costs be covered?
2.4 Ethical and Legal Aspects of Mesenchymal Stem Cells
Interestingly, there are no specific regulations concerning research with human embryonic stem cells on the level of the United Nations (UNESCO/UN) or Europe (Council of Europe/European Union). On both levels, however, there are suggestions and regulatory efforts concerning the use of cloning methods in humans.
Due to this it is not astonishing that nearly each EU country has a different regulation. For example, the German signed the Embryo Protection Act from first January 1991 into law which prohibits the import, production and use of human ESCs for any purpose. In addition, each totipotent stem cell having the capacity to develop into an organism given circumstances is considered to be an embryo in Germany. After a long and controversial discussion, the German Bundestag agreed to a due date and some years later the due day was moved to first May 2007. Furthermore, an alteration of the specific stem cell law allows the use of imported ESCs which were generated before the due date and were produced from surplus embryos through in-vitro-fertilization. The Robert Koch Institute is the corresponding ordinance giving permission for projects with ESCs and the authority for all ethical questions related to human embryonic stem cells. In contrast in Great Britain embryos generated by using somatic cell nuclear transfer (keyword therapeutical cloning), and thereby even producing a chimera (e.g. cow egg with human nucleus) can be used for research.
Many Asian countries and Israel have the least restrictive laws. Singapore, for example, is widely considered as Asia’s stem cell center because it is allowed to use embryos up to 2 weeks of age for therapeutical purposes (Dhar and Hsi-En 2009; Poulos 2018). In Israel it is legal to use an embryo up to 40 days after fertilization. The differences in the restriction and use of ESCs are enormous between different countries. Depending on the country, an ethical committee has to agree upon the project and the approval of the donor must be obtained. In China, a scientist stated in November 2018 that two twin girls were born where the genome was altered using CRISPR-Cas9 to generate a partical resistance against HIV infection by altering the CCR5 receptor. This led to a heated debate in most societies because it alters the human genome also for following generations (keyword human cloning).
MSCs on the other hand can be isolated and used worldwide with very few ethical controversies. Two different regulations have to be considered with the Regularity of the EU if stem cells are combined with a scaffold. Whereas the rule of the so called “medical devices” are easy to meet, the rule for a “medicinal product” were tight regulated leading to only few stem cell products on the market. In addition, the EU legislation created a regulatory gap between medical devices and medicinal products which hinders the approval of advanced-therapy products. However, there are only a few mesenchymal stem cell products approved so far. The EMA (Europe) authorized the first stem cell product called Holoclar which is used in the eye to replace damaged cells of the epithelium of the cornea (Pellegrini et al. 2018). Also, mesenchymal stem cells have secured conditional approval since 2012 for treating children with graft versus host diseases (GvHD). Health Canada and also MedSafe in New Zealand and the regulatory agency in Japan (Najima and Ohashi 2017) authorized the application. Osiris Therapeutics (U.S.A) completed the first major clinical phase III trial, sponsored by industry, of allogeneic, marrow-derived MSCs for treatment of steroid-refractory GvHD (NCT00366145) (Galipeau and Sensébé 2018). The Therapeutic Goods Administration in Australia admitted one mesenchymal stem cell product called Prochymal which is also used in acute GvHD in pediatric patients (Patel and Genovese 2011). The Korean Food and Drug Administration approved in total three medical treatments based on MSCs. NeuroNata-R which is only available in South Korea and Hearticellgram®-AMI (Yang 2011) are bone marrow mesenchymal stem cell therapies. NeuroNata-R has a neuroprotective effect and is indicated for amyotrophic lateral sclerosis while Hearticellgram®-AMI is used to treat acute myocardial infarction through intracoronary injection (Yang 2011). Further Cartistem, is the first allogenic stem cell drug. The mesenchymal stem cells drug is derived from allogenic umbilical cord blood and is used for treatment of knee cartilage defects in patients with osteoarthritis (Park et al. 2017).
In line with this, surgeon prefer to use stem cells with and without scaffolds using a technique which allow a “one step” procedure. During surgery, the operating physician may isolate mesenchymal stem cells from patient’s bone marrow or rarer fat tissue and apply the cells back to the patient during surgery. The physician is allowed to treat the cells using an apheresis device or aspirator. The cells can also be separated by different on-site separation methods (magnetic antibodies, by filtration, or by gradient centrifugation) (Ruiz-Navarro and Kobinia 2017; Heinrichsohn 2017). Besides that, cells can be processed by activation through ultrasound or lasers. Also, mixing the mesenchymal stem cells with scaffolds or washing them before administration and using clinical syringes or other delivering tools e.g. for collection, separation, processing, delivery is allowed. This procedure is called Point-of-Care, and it allows the physician to apply a new cellular therapy to a patient. However, if the mesenchymal stem cell preparation is taken out of the operating room and the cells are expanded or treated in other ways, the application back to the patient has to follow another rule, which hampers the procedure as it is an elaborate process (◘ Fig 2.6).

Point-of-Care cell therapy with mesenchymal stem cells. During surgery, physicians are allowed to isolate the patients’ cells and apply them back. Only a few modifications and processing steps are allowed in this process (shown on the left side) namely collecting cells from the patient, separate them via density gradient centrifugation or magnetic beads, and apply the cells back to the patient using syringes or other delivering tools. If the cells have to be further processed such as being cultured or modified otherwise, they may not be given back to the patient without an official permission, where multiple obstacles have to be overcome (shown on the right side)
2.5 Perspectives for Future Use of Mesenchymal Stem Cells
MSCs are a promising tool for future use in regenerative medicine approaches. However, there are several obstacles which still have to be overcome.
Against expectations which have arisen from the success of hematopoietic stem cell treatments for cancers such as leukemia in the last 50 years, combined with the more recent findings that most tissues have adult stem cells, that MSCs will replace the loss of tissue cells in the respective organs or tissues, this is not the case (Eggenhofer et al. 2014). The cells are rapidly lost over time after transplantation into the recipient. Nevertheless, there seem to be a benefit for the patient which presumably is due to paracrine effect of the MSCs (Linero and Chaparro 2014; Baraniak and McDevitt 2010).
Another hurdle is that MSCs as other stem cells never differentiate completely in vitro which results in a potential risk for the recipient since they seem to be pre-committed to several lineages already in the tissue they are derived from. This might lead to unwanted differentiations within the tissue they are transplanted in.
Further, in opposite to pluripotent stem cells, they cannot differentiate unlimited in culture, so they must be replaced with newly isolates cells after some time. However, legal aspects in the EU are a major hindrance if the cells have to be cultured, expanded, or treated otherwise more than what is necessary for the isolation procedure leading to a quite difficult procedure necessary to be allowed to transplant them afterwards into a patient.
Last not least thinking about tissue or organ replacement the necessary procedure gets even more complex and thus complicated. Cells are not proliferating in vitro in three dimensions (and if this is unwanted as it is a sign for tumorigenicity). The extracellular matrix of the tissue or organ is needed for the cells to do so. If it cannot be obtained, it must be constructed artificially by either using natural or artificial substrates or a combination thereof to produce a biomaterial/scaffold for the cells. The scaffold must have interconnected pores to direct vascularization for nutrient and oxygen supply and disposal of metabolic waste and a lot of other features to eventually mimic the highly complex architecture of a “simple” tissue – not to forget that biomolecules and other cells than the specific tissue cell type are needed as well, such nerve cells, fibroblasts and the cells of the blood vessels namely endothelial cells and smooth muscle cells.
Nevertheless, ongoing clinical trials are encouraging to proceed using MSCs for future treatment of a variety of different diseases. Their great potential to differentiate in several lineages, their low immunogenicity, the easy accessibility, and their higher safety compared to pluripotent stem cells gives great hope that the obstacles can be overcome. More time is needed for basic research and thus a better understanding of the underlying signaling pathways within the cells and with their environment composed of other cell types, the matrix and biomolecules to make the huge step from bench to bedside safe.
2.6 Isolation Protocol of Mesenchymal Stem Cells
To get you started, step by step isolation protocols of MSCs from the most commonly used tissues are listed below. Be aware that you first need an ethical committee to give you permission if you want to use human tissue and that you need a permission for animal experiments as well if the cell source is not human.
Protocol
Isolation of MSCs from bone marrow (BM) (Susa et al. 2004; Secunda et al. 2015)
-
1.
Collect 20 mL of BM and fill into a Falcon tube containing anti-coagulant citrate dextrose (ACD) in a ration 1:5.
-
2.
Isolate the mononuclear cells by using the Ficoll-Paque gradient method: Pipet 15 mL of the Ficoll solution into a Falcon tube and overlay with 30 mL of the collected BM mixed with ACD.
Don’t mix the layers. Centrifuge at 400 x g for 30 minutes at room temperature without breaks. Five layers will be resulting after the centrifugation, namely from top to bottom: plasma phase, peripheral blood mononuclear cells (PBMCs), Ficoll, granulocytes, erythrocytes.
-
3.
Collect the PBMC in the interphase, put them in a new Falcon tube and wash them twice with phosphate buffered saline.
-
4.
The cell pellet can be resuspended in DMEM, supplemented with 10% fetal bovine serum and 1% antibiotics (100 U/mL streptomycin and 100 μg/mL penicillin) and the cells can be seeded on plates with a density of 15 × 104/cm2 at 37 °C in a humidified atmosphere with 5% CO2.
Protocol
Isolation of MSCs from umbilical cord (UC) (Secunda et al. 2015):
-
1.
The cord can be gained after pregnancy must be devoid of blood. Cut it into pieces (thickness: 0.5 mm) and placed into PBS, supplemented with 1% antibiotics (100U/mL streptomycin and P100 μg/mL penicillin). proceed within 2 hours.
-
2.
Transfer the pieces of the UC to 50 mL Falcon tubes with serum-free DMEM (Sigma) and centrifuge at 400 × g for 10 minutes at RT.
-
3.
Discard the supernatant and add 0.1% collagenase (0.15 U/mL) solved in serum-free DMEM and incubate overnight.
-
4.
Add the double volume of PBS and centrifuge at 400 × g for 10 minutes at RT.
-
5.
Discard the supernatant and treat the pellet with 2.5% trypsin in PBS at 37 °C for 30 minutes.
-
6.
Add at least threefold FBS to neutralize the trypsin and wash with serum-free DMEM culture medium.
-
7.
Resuspend the cell pellet in 10 mL DMEM, supplemented with 10% FBS and 1% antibiotics (100 U/mL streptomycin and 100 μg/mL penicillin) and seeded on plates with a density of 15 × 104/cm2 at 37 °C in a humidified atmosphere with 5% CO2.
This method uses an enzymatic digest. An explant method can be used as well, were the UC pieces were culture in DMEM-low glucose with 20% FBS at 37 °C in a humidified atmosphere with 5% CO2 and left undisturbed for 7 days to allow the migration of the cells from the explant.
Protocol
Isolation of MSCs from adipose tissue from liposuction material (Pittenger et al. 1999; Secunda et al. 2015):
-
1.
Determine the amount of received fat solution.
-
2.
Add PBS to the fat tissue (ratio 1:1), shake well and incubate for 30 minutes at RT to separate the phases.
-
3.
Discard the bottom layer and add PBS (ratio 1:1) and add 0.1% collagenase (0.15 U/mL) in PBS to the upper phase and incubate for 60 minutes at 37 °C while shaking in the water bath.
-
4.
Centrifuge the incubated suspension at 200 × g at RT for 10 minutes.
-
5.
Discard the supernatant and resuspend the pellet in 10 mL erolysis buffer (0.5 M EDTA, pH 8.0, 0.154 M ammonium chloride, 1 × 10−2 M potassium hydrogen carbonate) and incubate for 10 minutes at RT.
-
6.
Centrifuge again at 200 × g, RT for 10 minutes and discard the supernatant afterwards.
-
7.
Resuspend the cell pellet in 10 mL DMEM, supplemented with 10% FBS and 1% antibiotics (300 U/mL streptomycin and 300 μg/mL penicillin) and seed them at in a density of 15 × 104/cm2 on plates at 37 °C in a humidified atmosphere with 5% CO2.
-
8.
Change medium after 24 hours to remove non-adherent cells and debris.
If necessary, the bottom layer (from 3.) can be used as well following the same procedure to increase the MSC yield.
Additional Comment
The mesenchymal stem cells isolated from different tissues were all cultured in DMEM, supplemented with 10% FBS and 1% antibiotics (300 U/mL streptomycin and 300 μg/mL penicillin) at 37 °C in a humidified atmosphere with 5% CO2. Reaching > 75% confluence, the cells were trypsinised with 0.05% trypsin in 0.2% EDTA and subsequently frozen or passaged by splitting them in two or more new flasks (Freshney et al. 2007). Adapted and slightly altered methods can also be used for the isolation of MSCs from other tissues.
Take Home Message
-
Mesenchymal stem cells can be found in various tissues and have a vast differentiation potential which is interesting for approaches in regenerative medicine.
-
Mesenchymal stem cells are defined by a set of three minimal criteria proposed by the Mesenchymal and Tissue Stem Cell Committee of the International Society for Cellular Therapy
-
Mesenchymal stem cells can be used in autologous therapy approaches, have a low immunogenicity, are easily accessible, quickly expandable and they cause no major ethical problems.
-
Mesenchymal stem cells can be used in cell therapy approaches during a surgery at the Point-of-Care. If they must be expanded or treated otherwise, the application in humans causes additional obstacles which have to be overcome.
-
Many clinical trials for the treatment of various diseases are ongoing. At the moment, almost all of them are in clinical trials phase I or II.
-
The beneficial effect of mesenchymal stem cells in regenerative medicine seem to be due to paracrine effects since over time the cells get lost, thus not replacing the tissue cells.
-
New approaches in regenerative medicine for tissue repair often use two cell types e.g. tissue cell and mesenchymal stem cells.
-
Scaffold composition and properties should closely resemble original tissue.
-
Scaffolds must be biocompatible and have suitable morphology, mechanical properties, technical functionality, stability against physiological conditions.
-
Today, scaffolds are often produced via additive manufacturing including 3D printing and electrospinning.
-
Major difficulties remain in proper vascularization, bio resorption and in transferring the scaffold into clinical trials.
References
Alkhalil, M., Smajilagić, A., & Redžić, A. (2015). Human dental pulp mesenchymal stem cells isolation and osteoblast differentiation. Medicinski Glasnik, 12(1), 27–32.
Baksh, D., Song, L., & Tuan, R. S. (2004). Adult mesenchymal stem cells. Characterization, differentiation, and application in cell and gene therapy. Journal of Cellular and Molecular Medicine, 8(3), 301–316.
Baraniak, P. R., & McDevitt, T. C. (2010). Stem cell paracrine actions and tissue regeneration. Regenerative Medicine, 5(1), 121–143.
Bartholomew, A., Sturgeon, C., Siatskas, M., et al. (2002). Mesenchymal stem cells suppress lymphocyte proliferation in vitro and prolong skin graft survival in vivo. Experimental Hematology, 30(1), 42–48.
Bruno, S., Bussolati, B., Grange, C., et al. (2009). Isolation and characterization of resident mesenchymal stem cells in human glomeruli. Stem Cells and Development, 18(6), 867–880.
Cao, C., Dong, Y., & Dong, Y. (2005). Study on culture and in vitro osteogenesis of blood-derived human mesenchymal stem cells. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi, 19(8), 642–647.
Chen, Y., Kawazoe, N., & Chen, G. (2018). Preparation of dexamethasone-loaded biphasic calcium phosphate nanoparticles/collagen porous composite scaffolds for bone tissue engineering. Acta Biomaterialia, 67, 341–353.
Cotter, E. J., Wang, K. C., Yanke, A. B., et al. (2018). Bone marrow aspirates concentrate for cartilage defect of the knee: From bench to bedside evidence. Cartilage., 9(2), 161–170.
da Silva Meirelles, L., Chagastelles, P. C., & Nardi, N. B. (2006). Mesenchymal stem cells reside in virtually all postnatal organs and tissues. Journal of Cell Science, 119(11), 2204–2213.
Dhar, D., & Hsi-En, H. O. (2009). Stem cell research policies around the world. The Yale Journal of Biology and Medicine, 82(3), 113–115.
Dominici, M., Le Blanc, K., Mueller, I., et al. (2006). Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy, 8(4), 315–317.
Eggenhofer, E., Luk, F., Dahlke, M. H., et al. (2014). The life and fate of mesenchymal stem cells. Frontiers in Immunology, 5, 148.
El Khaldi-Hansen, B., El-Sayed, F., Tobiasch, E., et al. (2017). Functionalized 3D scaffolds for template-mediated biomineralization in bone regeneration. In Atta-ur-Rahman & S. Anjum (Eds.), Frontiers in stem cell and regenerative medicine research (pp. 130–178). Sharjah: Bentham Science Publishers.
Evans, M. J., & Kaufman, M. H. (1981). Establishment in culture of pluripotential cells from mouse embryos. Nature, 292(5819), 154–156.
Fenton, O. S., Olafson, K. N., Pillai, P. S., et al. (2018). Advances in biomaterials for drug delivery. Advanced Materials, 30, 1705328.
Freshney, R. I., Stacey, G. N., & Auerbach, J. M. (2007). Culture of human stem cells. Hoboken: Wiley.
Friedenstein, A. J., Chailakhjan, R. K., & Lalykina, K. S. (1970). The development of fibroblast colonies in monolayer cultures of guinea-pig bone marrow and spleen cells. Cell and Tissue Kinetics, 3(4), 393–403.
Friedenstein, A. J., Chailakhyan, R. K., Latsinik, N. V., et al. (1974). Stromal cells responsible for transferring the microenvironment of the hemopoietic tissues. Cloning in vitro and retransplantation in vivo. Transplantation, 17(4), 331–340.
Galipeau, J., & Sensébé, L. (2018). Mesenchymal stromal cells. Clinical challenges and therapeutic opportunities. Cell Stem Cell, 22(6), 824–833.
Gordon, A. S. (1972). Haemopoietic cells. In D. Metcalf, M. A. S Moore (Eds.) Frontiers of biology (vol. 178(4064), pp. 974–975). Elsevier.
Grémare, A., Guduric, V., Bareille, R., et al. (2018). Characterization of printed PLA scaffolds for bone tissue engineering. Journal of Biomedical Materials Research. Part A, 106(4), 887–894.
Grotheer, V., Schulze, M., & Tobiasch, E. (2014). Trends in bone tissue engineering: Proteins for osteogenic differentiation and the respective scaffolding. In: Protein purification – Principles and trends. iConcept Press Ltd, Hong Kong.
Haddouti, E. M., Skroch, M., Zippel, N., et al. (2009). Human dental follicle precursor cells of wisdom teeth. Isolation and differentiation towards osteoblasts for implants with and without scaffolds. Materialwissenschaft und Werkstofftechnik, 40(10), 732–737.
Hanna, J. H., Saha, K., & Jaenisch, R. (2010). Pluripotency and cellular reprogramming. Facts, hypotheses, unresolved issues. Cell, 143(4), 508–525.
Haubner, F., Muschter, D., Pohl, F., et al. (2015). A co-culture model of fibroblasts and adipose tissue-derived stem cells reveals new insights into impaired wound healing after radiotherapy. International Journal of Molecular Sciences, 16(11), 25947–25958.
Heinrichsohn, F. (2017). Cellular therapy, an autologous cellular point of care approach to satisfy patient needs. Journal of Translational Science, 3(1).
Henkel, J., Woodruff, M. A., Epari, D. R., et al. (2013). Bone regeneration based on tissue engineering conceptions – A 21st century perspective. Bone Research, 1(3), 216–248.
Herrera, M. B., Bussolati, B., Bruno, S., et al. (2007). Exogenous mesenchymal stem cells localize to the kidney by means of CD44 following acute tubular injury. Kidney International, 72(4), 430–441.
Hielscher, D., Kaebisch, C., Braun, B. J. V., et al. (2018). Stem cell sources and graft material for vascular tissue engineering. Stem Cell Reviews, 14(5), 642–667.
Horwitz, E. M., Le Blanc, K., Dominici, M., et al. (2005). Clarification of the nomenclature for MSC. The International Society for Cellular Therapy position statement. Cytotherapy, 7(5), 393–395.
Hourd, P., Chandra, A., Medcalf, N., et al. (2008). Regulatory challenges for the manufacture and scale-out of autologous cell therapies. StemBook, Harvard Stem Cell Institute, Cambridge, MA, USA.
Hu, J., Zhu, Y., Tong, H., et al. (2016). A detailed study of homogeneous agarose/hydroxyapatite nanocomposites for load-bearing bone tissue. International Journal of Biological Macromolecules, 82, 134–143.
Huang, B., Li, K., Yu, J., et al. (2013). Generation of human epidermis-derived mesenchymal stem cell-like pluripotent cells (hEMSCPCs). Scientific Reports, 3, 1933.
In’t Anker, P. S., Scherjon, S. A., Kleijburg-van der Keur, C., et al. (2004). Isolation of mesenchymal stem cells of fetal or maternal origin from human placenta. Stem Cells, 22(7), 1338–1345.
Kaebisch, C., Schipper, D., Babczyk, P., et al. (2015). The role of purinergic receptors in stem cell differentiation. Computational and Structural Biotechnology Journal, 13, 75–84.
Lanzoni, G., Alviano, F., Marchionni, C., et al. (2009). Isolation of stem cell populations with trophic and immunoregulatory functions from human intestinal tissues. Potential for cell therapy in inflammatory bowel disease. Cytotherapy, 11(8), 1020–1031.
Lee, O. K., Kuo, T. K., Chen, W.-M., et al. (2004). Isolation of multipotent mesenchymal stem cells from umbilical cord blood. Blood, 103(5), 1669–1675.
Linero, I., & Chaparro, O. (2014). Paracrine effect of mesenchymal stem cells derived from human adipose tissue in bone regeneration. PLoS One, 9(9), e107001.
Liu, J. Y., Peng, H. F., Gopinath, S., et al. (2010). Derivation of functional smooth muscle cells from multipotent human hair follicle mesenchymal stem cells. Tissue Engineering. Part A, 16(8), 2553–2564.
Moraghebi, R., Kirkeby, A., Chaves, P., et al. (2017). Term amniotic fluid: An unexploited reserve of mesenchymal stromal cells for reprogramming and potential cell therapy applications. Stem Cell Research & Therapy, 8(1), 190.
Najima, Y., & Ohashi, K. (2017). Mesenchymal stem cells. The first approved stem cell drug in Japan. Journal of Hematopoietic Stem Cell Transplantation, 6(3), 125–132.
Nakagawa, M., Koyanagi, M., Tanabe, K., et al. (2008). Generation of induced pluripotent stem cells without Myc from mouse and human fibroblasts. Nature Biotechnology, 26(1), 101–106.
Ottensmeyer, P. F., Witzler, M., Schulze, M., et al. (2018). Small molecules enhance scaffold-based bone grafts via purinergic receptor signaling in stem cells. International Journal of Molecular Sciences, 19(11), 3601.
Pansky, A., Roitzheim, B., & Tobiasch, E. (2007). Differentiation potential of adult human mesenchymal stem cells. Clinical Laboratory, 53(1–2), 81–84.
Paris, J. L., Román, J., Manzano, M., et al. (2015). Tuning dual-drug release from composite scaffolds for bone regeneration. International Journal of Pharmaceutics, 486(1–2), 30–37.
Park, J. H., Kim, D. Y., Sung, I. Y., et al. (2012). Long-term results of spinal cord injury therapy using mesenchymal stem cells derived from bone marrow in humans. Neurosurgery, 70(5), 1238–1247.
Park, Y.-B., Ha, C.-W., Lee, C.-H., et al. (2017). Cartilage regeneration in osteoarthritic patients by a composite of allogeneic umbilical cord blood-derived mesenchymal stem cells and hyaluronate hydrogel. Results from a clinical trial for safety and proof-of-concept with 7 years of extended follow-up. Stem Cells Translational Medicine, 6(2), 613–621.
Patel, A. N., & Genovese, J. (2011). Potential clinical applications of adult human mesenchymal stem cell (Prochymal®) therapy. Stem Cells Cloning., 4, 61–72.
Pellegrini, G., Ardigò, D., Milazzo, G., et al. (2018). Navigating market authorization. The path Holoclar took to become the first stem cell product approved in the European Union. Stem Cells Translational Medicine, 7(1), 146–154.
Pittenger, M. F., Mackay, A. M., Beck, S. C., et al. (1999). Multilineage potential of adult human mesenchymal stem cells. Science, 284(5411), 143–147.
Poulos, J. (2018). The limited application of stem cells in medicine: A review. Stem Cell Research & Therapy, 9(1), 1.
Prasad, V. K., Lucas, K. G., Kleiner, G. I., et al. (2011). Efficacy and safety of ex vivo cultured adult human mesenchymal stem cells (Prochymal™) in pediatric patients with severe refractory acute graftversus-host disease in a compassionate use study. Biology of Blood and Marrow Transplantation, 17(4), 534–541.
Prockop, D. J. (1997). Marrow stromal cells as stem cells for nonhematopoietic tissues. Science, 276(5309), 71–74.
Rajzer, I., Menaszek, E., & Castano, O. (2017). Electrospun polymer scaffolds modified with drugs for tissue engineering. Materials Science & Engineering. C, Materials for Biological Applications, 77, 493–499.
Rheinwald, J. G., & Green, H. (1975). Serial cultivation of strains of human epidermal keratinocytes. The formation of keratinizing colonies from single cells. Cell, 6(3), 331–343.
Ruiz-Navarro, F., & Kobinia, G. (2017). Point-of-care stem cell therapy (pocst). Multisite transplantation of autologous bone marrow-derived mononuclear cells in 85 patients with amyotrophic lateral sclerosis improves survival. Journal of Stem Cell Research & Therapy, 2(3), 98–110.
Sakaguchi, Y., Sekiya, I., Yagishita, K., et al. (2005). Comparison of human stem cells derived from various mesenchymal tissues. Superiority of synovium as a cell source. Arthritis and Rheumatism, 52(8), 2521–2529.
Salerno, S., Messina, A., Giordano, F., et al. (2017). Dermal-epidermal membrane systems by using human keratinocytes and mesenchymal stem cells isolated from dermis. Materials Science & Engineering, C: Materials for Biological Applications, 71, 943–953.
Schipper, D., Babczyk, P., El-Sayed, F., et al. (2017). The effect of nanostructured surfaces on stem cell fate. In A. M. Grumezescu & D. Ficai (Eds.), Nanostructures for novel therapy (Vol. 1, pp. 567–589). Amsterdam, Cambridge: Elsevier.
Schulze, M., & Tobiasch, E. (2012). Artificial scaffolds and mesenchymal stem cells for hard tissues. Advances in Biochemical Engineering/Biotechnology, 126, 153–194.
Secunda, R., Vennila, R., Mohanashankar, A. M., et al. (2015). Isolation, expansion and characterisation of mesenchymal stem cells from human bone marrow, adipose tissue, umbilical cord blood and matrix. A comparative study. Cytotechnology, 67(5), 793–807.
Simon, C. G. Jr. 3D scaffold fabrication approaches. Available online: https://www.nist.gov/sites/default/files/images/mml/bbd/biomaterials/scaffoldomics.jpg. Accessed 29 Aug 2018.
Steigmann, S. A., & Fauza, D. O. (2007). Isolation of mesenchymal stem cells from amniotic fluid and placenta. Current Protocols in Stem Cell Biology, 1, 1E.2.1–1E.212.
Steinhoff, G., Nesteruk, J., Wolfien, M., et al. (2017). Cardiac function improvement and bone marrow response: Outcome analysis of the randomized PERFECT phase III clinical trial of intramyocardial CD133+ application after myocardial infarction. eBioMedicine, 22, 208–224.
Susa, M., Luong-Nguyen, N.-H., Cappellen, D., et al. (2004). Human primary osteoclasts: In vitro generation and applications as pharmacological and clinical assay. Journal of Translational Medicine, 2(1), 6.
Takagi, S., Mandai, M., Hirami, Y., et al. (2018). Frequencies of human leukocyte antigen alleles and haplotypes among Japanese patients with age-related macular degeneration. Japanese Journal of Ophthalmology, 62, 568–575.
Takahashi, K., & Yamanaka, S. (2006). Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell, 126(4), 663–676.
Takahashi, K., Tanabe, K., Ohnuki, M., et al. (2007). Induction of pluripotent stem cells from adult human fibroblasts by defined factors. Cell, 131(5), 861–872.
Thirumala, S., Zvonic, S., Floyd, E., et al. (2005). Effect of various freezing parameters on the immediate postthaw membrane integrity of adipose tissue derived adult stem cells. Biotechnology Progress, 21(5), 1511–1524.
Thomson, J. A., Itskovitz-Eldor, J., Shapiro, S. S., et al. (1998). Embryonic stem cell lines derived from human blastocysts. Science, 282(5391), 1145–1147.
Till, J. E., & McCulloch, E. A. (1961). A direct measurement of the radiation sensitivity of normal mouse bone marrow cells. Radiation Research, 14(2), 213.
Tobiasch, E. (2008). Adult human mesenchymal stem cells as source for future tissue engineering. In C. Zacharias, et al. (Eds.) Forschungsspitzen und Spitzenforschung (pp. 329–338). Physica-Verlag HD, Heidelberg, Germany.
Tsuji, O., Sugai, K., Yamaguchi, R., et al. (2018). Laying the groundwork for a first-in-human study of an induced pluripotent stem cell-based intervention for spinal cord injury. Stem Cells, 37, 6–13.
Ullah, I., Subbarao, R. B., & Rho, G. J. (2015). Human mesenchymal stem cells – Current trends and future prospective. Bioscience Reports, 35(2), e00191.
Velasco, M. A., Narváez-Tovar, C. A., & Garzón-Alvarado, D. A. (2015). Design, materials, and mechanobiology of biodegradable scaffolds for bone tissue engineering. BioMed Research International, 2015, 729076.
Wang, H.-S., Hung, S.-C., Peng, S.-T., et al. (2004). Mesenchymal stem cells in the Wharton’s jelly of the human umbilical cord. Stem Cells, 22(7), 1330–1337.
White, I. A., Sanina, C., Balkan, W., et al. (2016). Mesenchymal stem cells in cardiology. Methods in Molecular Biology, 1416, 55–87.
Witzler, M., Alzagameem, A., Bergs, M., et al. (2018). Lignin-derived biomaterials for drug release and tissue engineering. Molecules, 23(8), E1885.
Wong, P. T., & Choi, S. K. (2015). Mechanisms of drug release in nanotherapeutic delivery systems. Chemical Reviews, 115(9), 3388–3432.
www.clinicaltrials.gov. Accessed 27 May 2019.
Yang, H. (2011). South Korea’s stem cell approval. Nature Biotechnology, 29(10), 857.
Yao, W., Lay, Y.-A. E., Kot, A., et al. (2016). Improved mobilization of exogenous mesenchymal stem cells to bone for fracture healing and sex difference. Stem Cells, 34(10), 2587–2600.
Yu, J., Vodyanik, M. A., Smuga-Otto, K., et al. (2007). Induced pluripotent stem cell lines derived from human somatic cells. Science, 318(5858), 1917–1920.
Zhang, Y., Lau, P., Pansky, A., et al. (2014). The influence of simulated microgravity on purinergic signaling is different between individual culture and endothelial and smooth muscle cell coculture. BioMed Research International, 2014, 413708.
Zippel, N., Limbach, C. A., Ratajski, N., et al. (2012). Purinergic receptors influence the differentiation of human mesenchymal stem cells. Stem Cells and Development, 21(6), 884–900.
Zuk, P. A., Zhu, M., Ashjian, P., et al. (2002). Human adipose tissue is a source of multipotent stem cells. Molecular Biology of the Cell, 13(12), 4279–4295.
Acknowledgements
This article was supported by the Bundesministerium für Bildung und Forschung (BMBF) FHprofUnt to E.T., FKZ: 13FH012PB2; EFRE co-financed NRW Ziel 2: “Regionale Wettbewerbsfähigkeit und Beschäftigung”, 2007-2013, Ministerium für Innovation, Wissenschaft und Forschung (MIWF) NRW FH-Extra to E.T., FKZ: z1112fh012; DAAD PPP Vigoni to E.T., FKZ: 314-vigoni-dr and FKZ: 54669218; Bundesministerium für Bildung und Forschung (BMBF)-AIF to E.T., FKZ: 1720X06; Bundesministerium für Bildung und Forschung (BMBF) IngenieurNachwuchs to E.T., FKZ: 13FH019IX5; Ministerium für Innovation, Wissenschaft und Forschung (MIWF) NRW FH Zeit für Forschung to E.T., FKZ 005-1703-0017.
Bundesministerium für Bildung und Forschung (BMBF) IngenieurNachwuchs to S.W.; FKZ: 13FH569IX6.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

{kind=link}
Cite this chapter
Tonk, C.H., Witzler, M., Schulze, M., Tobiasch, E. (2020). Mesenchymal Stem Cells. In: Brand-Saberi, B. (eds) Essential Current Concepts in Stem Cell Biology. Learning Materials in Biosciences. Springer, Cham. https://doi.org/10.1007/978-3-030-33923-4_2
Download citation
DOI: https://doi.org/10.1007/978-3-030-33923-4_2
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-33922-7
Online ISBN: 978-3-030-33923-4
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)