
Abstract
PTHrP was first discovered as the most common mediator of malignancy-associated hypercalcemia. Subsequently, the discovery of its ubiquitous expression in normal tissues unraveled its role as a physiological autocrine/paracrine regulator. The significance of PTHrP in cancer is not confined to malignancy-associated hypercalcemia, and sufficient evidence now also supports its role in skeletal metastasis through its modulation of bone turnover. Furthermore, our own studies have recently shown the critical role of PTHrP in breast cancer initiation, growth, and metastasis. More recently, we have provided new evidence that overexpression of PTHrP is associated with higher incidence of brain metastasis and decreased overall survival in triple-negative breast cancer patients. Further mechanistic studies in human and mouse model are necessary to fully understand the role of PTHrP in tumor progression and metastasis.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


PTHrP Background, Discovery, and Gene Structure
Background and Discovery
PTHrP was first identified after a nearly four-decade search of humoral factors that underlie the development of hypercalcemia in malignancy, a severe complication in patients with advanced-stage cancers. Fuller Albright, in 1941, was the first to postulate that ectopic production of parathyroid hormone (PTH), or a PTH-like factor, could be responsible for this “humoral hypercalcemia of malignancy” (HHM). He reported the case of a patient with renal carcinoma and a solitary bone metastasis associated with hypercalcemia and hypophosphatemia mimicking primary hyperparathyroidism [1]. PTH is an 84-amino acid hormone secreted exclusively by parathyroid cells, and it plays a key role in regulating Vitamin D, phosphate, and calcium homeostasis. Albright’s hypothesis that cancer-secreted PTH was the putative etiological factor in HHM was a logical explanation due to its similarity to PTH actions. However, he was unable at that time to prove his hypothesis in the absence of specific immunoassay for the detection of PTH in the blood circulation of patients with HHM. Subsequently, several groups using PTH immunoassays determined that PTH blood levels in HHM were suppressed in response to calcium-induced inhibition of PTH by the parathyroid gland [2]. It was not until 1987, after great efforts were devoted to identifying and isolating this putative tumor-secreted factor, that three independent groups simultaneously identified a protein with similar biological activities and homology to the amino terminus of PTH, therefore named PTHrP. An active peptide with a molecular weight of 18-kDa was isolated by one group from a human lung cancer cell line, a second group from a 6-kDa active peptide from human renal carcinoma cells, and a third group from a 17-kDa active peptide from human breast carcinoma [3,4,5]. Subsequently, the complementary DNA (cDNA) encoding these peptides confirmed that eight of the initial 13 N-terminal amino acids of PTHrP were identical to those of human PTH [6,7,8]. These findings explained the biochemical similarities between primary hyperparathyroidism due to excessive production of PTH and HHM from cancer-producing PTHrP.
Gene Structure
The human PTHrP gene (PTHLH) is located on the short arm of chromosome 12, distinct from the human PTH gene, which is located on the short arm of chromosome 11. The similarities in overall genomic organization and similar exon–intron boundaries of PTHLH and PTH genes give compelling evidence of their origin from a common ancestral gene which evolved from a gene duplication event during evolution [9] (Fig. 1). The human PTHLH gene spans ~15 kb of genomic DNA and includes nine exons that are transcribed by three functionally distinct promoters (Fig. 1). The canonical TATA promoters (P1 and P3) are located upstream of the noncoding exon 1 and exon 4, respectively, whereas 5′ to noncoding exon 3 is a GC-rich promoter (P2) (Fig. 1). Although it is not completely understood whether PTHrP transcription is controlled by each of these promoters in a tissue-specific manner, all species identified to date share only one functional promoter equivalent to the human P3, but not P1 or P2 promoters. Therefore, it is likely that the dominant transcriptional regulation of PTHrP operates through the P3 promoter [10]. Gene sequence comparison reveals that exons equivalent to human exons 4, 5, 6, and 9 are highly conserved among species, which suggests that these exons may constitute the basic PTHLH gene structure with important biological functions (Fig. 1).

Gene structures of human, mouse, rat, chicken, and fugu PTHLH with the human PTH genes. The coding regions and untranslated sequences are indicated by the black and gray boxes, respectively. Exons are noted with Arabic numerals. The positions of the three promoters (red arrow) of human PTHLH are shown (P1, TATA; P2, GC-rich; P3, TATA). The known splicing events in human PTHLH are shown
Alternative splicing gives rise to three separate human PTHrP isoforms which differ at their carboxyl-terminal ends and contain either 139, 141, or 173 amino acids. Although there is no intron between exons 6 and 7 in the human PTHLH gene, the junction provides a splice donor site for acceptors at the beginning of exons 8 and 9 (Fig. 1). Exon 6 encodes a region, common to all three isoforms, whereas exons 8 and 9 encode the exclusive carboxy termini of PTHrP 1-173 and 1-141 isoforms (Fig. 1). The mRNAs for each of these isoforms are commonly expressed in various normal and cancer tissues in humans, but the full characterization of their tissue distribution, processing, and function remains to be established. In contrast to the human PTHLH gene organization, the gene organization in other species is relatively simple, with a single promoter producing one single isoform. In rat and mice, mature peptides of 141 and 139 amino acids, respectively, are expressed [11, 12]. The PTHLH gene yields a single mature peptide of 139 amino acids in chicken and 126 amino acids in fugu [13, 14].
PTHrP Physiology
PTHrP Protein Structure, Functional Domains and Its Receptor
PTHrP amino acid sequences uncovered several functional domains including a prepro sequence, a PTH-like region, a nuclear localizing sequence (NLS), and a C-terminal domain named osteostatin (Fig. 2). The intracellular “prepro” precursors −36 to −1 of the mature peptide are necessary for intracellular trafficking and secretion of the PTHrP polypeptide [10]. The PTH-like region is essential for nearly all the agonist actions of PTHrP at the classical PTH/PTHrP type 1 receptor (PTH1R), a class II G-protein coupled receptor, expressed on classic PTH target tissues (bone and kidney) that regulate calcium and phosphate homeostasis. This PTH-like region covers the first N-terminal domain of PTHrP (amino acids 1–13), which shares the highest degree of primary sequence homology with PTH (8 of the first 13 residues are identical). The following 14–36 region of PTHrP has no homology with the primary amino acid sequence of PTH; however, it is critical for the binding of PTHrP to the PTH1R. Competitive binding assays have shown that PTH (1–34) and PTHrP (1–36) bind PTH1R with almost equal affinity, whereas shorter N-terminal fragments of either PTH or PTHrP do not [15]. This indicates that the binding domain of PTHrP (14-36) has a similar secondary structure to PTH, regardless of the differences in primary structure.

Human PTHrP functional domains and amino acid sequences . The three isoforms resulting from alternative splicing have 139, 141, and 173 amino acids (aa), respectively. The prepro region (gray) includes the signal sequence (aa −36 to −1). The PTH-like region (yellow) binds to the PTH1R receptor (aa 1–34). The region responsible for nuclear localizing sequence (NLS) (green) is (aa 67–94). The osteostatin region (orange) is (aa 107–111)
Upon binding to the PTH1R in bone and kidney, PTHrP can activate intracellular cyclic 3′, 5′-adenosine monophosphate (cAMP) which further activates both the adenylyl cyclase/protein kinase A (PKA) pathway as well as the calcium/inositol phosphate/protein kinase C pathway [16]. PTHrP is frequently coexpressed in the same cells or expressed in those immediately adjacent to PTH1R. Such close juxtaposition of cells expressing PTH1R and PTHrP highlights its function as a paracrine/autocrine factor in many tissues [10]. For example, PTHrP/PTH1R signaling system is crucial not only for physiological functions of PTHrP in bone and mammary gland development but also for pathological effects of PTHrP as a circulating, tumor-derived factor in HHM, as well as a locally produced factor at metastatic sites.
The mid-region (amino acids 37–106) of PTHrP includes a nuclear localization sequence (NLS) within residuals 67–94, which can translocate cytoplasmic PTHrP into the nucleus. The NLS of PTHrP contains a basic amino acid sequence, so called cell-penetrating peptides (CPPs), which is homologous to the NLS found in human retroviral regulatory protein [17]. The putative length of NLS was defined by Lam and colleagues to reside between residues 67–94 [18]. The PTHrP import mechanism involves the NLS forming a complex composed of importin β and the monomeric GTP-binding protein Ran which is then transported into the nucleus through the nuclear port complex [10]. PTHrP residues 83–93 are essential for importin β recognition, with residues 71–82 required for high-affinity binding [19]. The crystal structure of a fragment of importin β bound to the non-classical NLS of PTHrP provides the most important molecular evidence for supporting this region as the NLS [20]. This is a strong evidence to support the intracrine role of PTHrP aside from its autocrine/paracrine actions.
Although the actions of PTHrP in the nucleus are not fully understood, current evidence indicates that it plays important roles in both normal and malignant cells. PTHrP can be targeted to the nucleus in vascular smooth muscle cells and this nuclear targeting is associated with an increase of vascular smooth muscle cell proliferation [21]. In breast, colon, and prostate cancer cells, the nuclear pathway was found to stimulate cell proliferation, prevent tumors cells from apoptosis or anoikis, and stimulate cell migration [22].
Finally, the C-terminal region consisting of amino acids 107–139 is associated with inhibition of osteoclast function and stimulation of osteoblast proliferation [23,24,25]. It has also been found that this region together with the NLS can increase mitogenesis in vascular smooth muscle cells [26]. However, it should be noted that this C-terminal region is the least conserved domain among all species, the human and mouse having only seven residues, and rat and human having 13 residues in common. The functions of the C-terminal region of PTHP remain controversial and need further investigation.
Normal Physiological Functions of PTHrP
PTHrP is expressed in many normal cell types and tissues and therefore normal physiological functions have been proposed. In normal physiological condition, PTHrP acts as an endocrine factor only in two identified circumstances: (1) in lactation where PTHrP is produced by the breast and reaches the circulation [27]; (2) in the fetus, where it regulates maternal fetal calcium transport [28]. In most cases, PTHrP is regarded as having an autocrine or paracrine role in normal development and postnatal physiology. Here, we will focus on the functions of PTHrP in bone and mammary gland development in order to better examine its pathological role in breast tumor initiation, progression, and bone metastasis.
PTHrP in Mammary Gland Development
A human monogenetic disorder and animal models have shed light on the crucial role of PTHrP in mammary gland development [29]. Fetuses with Blomstrand chondrodysplasia lack breast tissue, indicating that PTHrP is essential for breast development in humans [30]. Studies in Pthlh- and Pth1r-null mice show that PTHrP signaling is indispensable for the formation of mammary glands [29]. The mammary gland formation in embryos is regulated by a cross-talk between the epithelial cells in the bud and ducts and adjacent mesenchymal cells in the stroma [29]. In mice and human fetuses, PTHrP is expressed by the epithelial cells in the mammary bud, which interacts with the PTH1R expressed by the surrounding mesenchyme [31]. PTHrP–PTH1R cross-talk is required for the differentiation of the mesenchymal cells, which in turn stimulates the outgrowth of the epithelial ducts [31]. Disruption of either PTHrP or PTH1R interrupts the cross-talk between epithelium and mesenchyme, leading to a failure of mammary development in mice and humans [31]. Potential downstream signaling regulated by PTHrP includes Wnt and bone morphogenetic protein 4 (BMP4) as well as upregulation of several transcription factors including muscle segment homeobox 2 (Msx2), androgen receptor, and lymphoid enhancer-binding factor 1 (Lef1) [32, 33]. After embryogenesis, PTHrP is highly expressed by alveolar epithelial cells during lactation and is secreted into milk and into the circulation [27].
PTHrP in Bone Development
Generation of mice homozygous for a disrupted Pthlh gene established the first direct evidence for a critical role for PTHrP in the process of normal skeletal development. Pthlh-null mice die at birth, probably of asphyxia, and exhibit widespread abnormalities of endochondral bone development [34]. Subsequent studies characterized this phenotype of chondrodysplasia as a consequence of diminished proliferation, accelerated differentiation, and premature apoptotic death of chondrocytes [16]. Jansen’s metaphyseal chondrodysplasia (JMC) , a rare autosomal dominant human disorder, provided the first evidence that PTHrP actions in endochondral ossification are mediated by PTH1R [35]. Four different mutations in the PTH1R gene have been described in patients with JMC which lead to a constitutive, PTHrP-independent receptor activation [35]. Such activating PTH1R mutations in humans with JMC and overexpression of the same constitutively active receptor in the growth plate of transgenic mice gave rise to a delayed endochondral bone formation phenotype [35, 36]. Overexpression of Pthrp in chondrocyte of transgenic mice results in a similar pattern as observed in mice with active Pth1r overexpression in chondrocyte [37]. Alternatively, mice with homozygous Pth1r disruption exhibit accelerated differentiation of chondrocytes, and a more severe but similar phenotype to the one observed in Pthlh-null mice [38]. Together, loss-of-function mutations in PTH1R gene causes skeletal abnormalities observed in infants with Blomstrand chondrodysplasia, which are mirror images to those observed with JMC [39]. These findings provide sufficient proof that PTH1R mediates most of the cartilaginous effects of PTHrP.
It is interesting to note that the phenotype of Pth1r-null mice does not fully recapitulate the one observed in Pthlh-null mice, indicating that PTHrP may exert additional effects in a PTH1R-independent fashion. Knock-in mice homozygous for a truncated Pthrp 1–84, missing the NLS and the C-terminal region but preserving their ability to bind with Pth1r were generated [40]. These knock-in mice displayed retarded growth, early senescence, and malnutrition leading to their rapid postnatal demise [40]. This model established a pivotal role for nuclear PTHrP in promoting cellular proliferation while inhibiting pathways leading to senescence.
Pthlh-null mice not only unraveled the central role of PTHrP in endochondral bone formation but also revealed the importance of PTHrP postnatally in bone remodeling. Bone is a dynamic organ that undergoes continuous remodeling. Bone homeostasis depends on the balanced activities between osteoblasts (mesenchymal stem cell-derived bone-forming cells) and bone-resorbing cells of monocyte and macrophage lineage known as osteoclasts (Fig. 3). First, in the Pthlh-null mice, osteoblastic progenitor cells contain an inappropriate accumulation of glycogen, which indicates a metabolic defect in cells of the osteogenic lineage secondary to PTHrP deficiency [41]. Second, heterozygous Pthlh-null mice are born phenotypically normal, but exhibit a low bone mass by 3 months of age characterized by a marked decreased in trabecular thickness and connectivity, and an abnormally high number of adipocytes in the bone marrow [42]. Third, PTHrP and PTH1R are expressed at different stages of the osteogenic lineage, indicating its pivotal role in the regulation of the maturation of pluripotential bone marrow stromal cells toward the osteogenic lineage [16].

Paracrine actions of PTHrP in bone remodeling. PTHrP produced by cells of the early osteoblast lineage acts on more advanced differentiated cells possessing the PTH1R, therefore promoting their differentiation and bone formation and while inhibiting apoptosis of mature osteoblasts. Moreover, PTHrP increases production of RANKL and binding of RANKL to RANK on hematopoietic progenitors leading to enhanced differentiation of osteoclast precursors and osteoclasts activation
During times of bone homeostasis , osteoclast activity and maturation is regulated by the interaction between its receptor activator of nuclear factor κB (RANK) surface receptor and that of the receptor activator of nuclear factor κB ligand (RANKL) protein expressed by osteoblasts and other bone marrow stromal cells; whereas osteoprotegerin (OPG), a decoy receptor for RANKL, diverts RANKL binding to RANK, reduces the half-life of membranous RANKL, and therefore inhibits bone resorption induced by osteoclasts [43]. PTHrP can stimulate bone resorption indirectly by upregulating the expression of RANKL in stromal osteoprogenitors [44] (Fig. 3). Binding of RANKL to RANK, a membrane protein expressed by hematopoietic progenitors, results in increased differentiation of osteoclast precursors and maturation (Fig. 3).
PTHrP and Cancer Biology
PTHrP and Malignancy-Associated Hypercalcemia (MAH)
MAH is a well-known complication of cancer and occurs in about 20–30% of cancer patients [45]. MAH is classified into four groups: humoral hypercalcemia of malignancy (HHM), local osteolytic hypercalcemia (LOH), excess 1,25(OH)2D production, and ectopic PTH secretion. In 1936, Gutman et al. identified LOH in patients suffering from multiple myeloma and breast cancer (BC) with extensive bone lesions [45]. In 1941, Fuller Albright proposed a mechanism of hypercalcemia independent of bone metastasis [1]. The existence of a systematic factor with PTH bioactivity was suggested when Albright described a patient with renal carcinoma, hypercalcemia, and hypophosphatemia following an irradiation of bone [1]. At present, hypercalcemia secondary to PTH-like mediators accounts for approximately 80% of the cases, whereas LOH accounts for most of the remaining cases in cancer patients [45]. Excess 1,25(OH)2D production accounts for <1% of all cases and ectopic PTH secretion by tumor cells is an even rarer event [45].
The classic signs and symptoms of severe hypercalcemia include confusion, constipation, nausea, anorexia, and coma. Elevated PTHrP in the context of hypercalcemia is almost always associated with PTH suppression [45]. A low or low-normal serum phosphorus level, if present, confirms the diagnosis [45]. There is still some controversy about the 1,25(OH)2D circulating level in HHM which has been found to be either suppressed, normal, or even elevated [46,47,48]. Breast, renal, and squamous carcinomas are the most common solid cancers associated with hypercalcemia [45]. Among hematological malignancies, multiple myeloma is the most commonly associated with hypercalcemia, followed by leukemia and non-Hodgkin’s lymphoma [45]. Circulating PTHrP levels have been reported to be elevated in 50–90% of hypercalcemic cancer patients with solid tumors and in 25–60% of patients with hematological malignancies [49]. In addition, circulating PTHrP may also have prognostic value. A prospective study conducted by our team in patients with MAH indicated that elevated circulating PTHrP is an indicator of poor prognosis and is associated with reduced survival (Fig. 4) [51]. Several other studies also confirmed the prognostic value of PTHrP [52, 53].

Serum levels of PTHrP and survival of patients with MAH. (a) Survival in 76 hypercalcemic cancer patients, by PTHrP status and pretreatment calcium levels. Numbers shown in the inset are total numbers of deaths/number of patients at baseline. Numbers of patients at risk were 40 at 100 days, 22 at year 1, and 3 at year 3. (b) Survival in hypercalcemic cancer patients, by PTHrP status and age group. Numbers of patients at risk were 41 at 100 days, 22 at year 1, and 3 at year 3. CA ≤ 12 = pretreatment serum calcium levels 10.3–12 mg/dL; CA > 12 = pretreatment calcium levels >12 mg/dL; PTHrP 0 = PTHrP not elevated; PTHrP >0 = PTHrP elevated. PTHrP and calcium levels are two independent prognostic factors for patient survival, and the effect of PTHrP is only significant in patients younger than 65. (Reproduce from [50])
However, measurement of serum PTHrP presents few challenges. First, tumors may express several isoforms of PTHrP which could either circulate intact or be subjected to further metabolism. The nature of these potential circulating forms is still elusive. Second, it has been challenging to establish appropriate immunoassays that can recognize these multiple circulating either bioactive or inactive forms. Shortly after the discovery and characterization of PTHrP, immunoassays were developed which focused on the recognition of both the N-terminal (1–36) bioactive region and the inactive C-terminal (109–136) region of PTHrP [54]. However, little or no immunoreactivity was detected in the circulation of patients with MAH indicating that the three intact isoforms were likely metabolized. Burtis et al. also designed a two-site immunoassay using two polyclonal antibodies, a capture antibody raised against PTHrP 37–74, and a radiolabelled signal antibody raised against PTHrP 1–36 [54]. Most patients with HHM had elevated PTHrP levels indicating that PTHrP fragments containing at least the first 74 amino acids were present in a variety of hypercalcemic cancer conditions [54]. In addition, Burtis et al. also developed yet another C-terminal radioimmunoassay using a polyclonal antibody raised against PTHrP 109-138 and were able to detect high levels of PTHrP in the circulation of renal failure patients with MAH [54]. An ultrasensitive multiplex two-site immunoassay has recently been reported capable of simultaneously measuring several circulating forms of PTHrP with a limit of detection (LODs) of 150 aM (~1000 fold lower than current immunoradiometric assay) [55]. The clinical value of such ultrasensitive multiplex two-site immunoassay for the diagnosis and prognosis of cancer patients needs further evaluation in well-established populations.
Current therapies in MAH in individuals suffering from moderate to severe hypercalcemia are aimed at lowering serum calcium levels, and specifically act by inhibiting bone resorption [45]. Bisphosphonates are the standard of care in the treatment of MAH since their approval in the late 1980s, and include mainly pamidronate and zoledronic acid administered intravenously [45]. In 2014, the monoclonal antibody denosumab, directed against RANKL, was approved for the treatment of bisphosphonate refractory hypercalcemia [56]. Even though these currently approved therapies can successfully control blood calcium levels and markedly decrease the symptoms of hypercalcemia, such modalities have had little effect on the patients’ mortality associated with the underlying malignancy [45]. However, in the case of HHM, all therapies mentioned above do not target the primary underlying cause of hypercalcemia, namely PTHrP, and it is therefore not yet established whether therapies targeting PTHrP will have an additional benefit. Ogata infused chimeric anti-PTHrP antibodies into nude mice transplanted with PTHrP-secreting human cancer tissues and found this treatment resulted in a prompt and sustained decline in serum calcium [57]. This response was accompanied by improvements in food intake, water intake, body weight gain, and general behavior [57]. Compared to the effects of either bisphosphonates or calcitonin, the author found that some beneficial effects of the antibody were independent of blood calcium levels [57]. These additional benefits of using anti-PTHrP antibodies need further investigation.
PTHrP and Cancer Development
The significance of PTHrP expression by different malignancies is likely not confined to MAH. Overexpression of PTHrP in the absence of hypercalcemia is very common in breast, prostate, lung, and colon cancers [50]. In contrast, normal or non-neoplastic tissues express low levels of PTHrP [50]. This correlation between PTHrP expression and tumor progression suggests that it could be mechanistically linked.
PTHrP expression has been shown to be under the control of numerous growth and angiogenic factors such as transforming growth factor beta (TGF-β), epidermal growth factor (EGF), platelet-derived growth factor (PDGF), and vascular endothelial growth factor (VEGF) [50]. Various in vitro studies have provided mounting evidence of the multifunctional role of PTHrP in cancer cell biology including regulation of tumor cell growth, differentiation, and invasion as well as regulation of tumor cell survival factors and interference with apoptotic signaling pathways [50].
PTHrP in Breast Cancer Development
BC is a heterogeneous disease characterized by different pathological and molecular subtypes that have different treatment responses and clinical outcomes. Breast cancer receptor status, most commonly defined by estrogen-receptor (ER), progesterone-receptor (PR), and human epidermal growth factor receptor 2 (HER2) status in the clinical setting, is critical for determining therapeutic intervention and prevention strategies. In addition to the receptor status, five distinct human subtypes have been defined based on gene expression profiling. These include the luminal A (ER and/or PR positive and HER2 negative) and B (ER and/or PR positive and HER2 negative/positive), basal-like (ER, PR, and HER2 negative), claudin-low (ER, PR, and HER2 negative), and HER2/ERBB2-positive (ER and PR negative and HER2 positive) tumors [58]. Most basal-like tumors have a ‘triple-negative’ immunophenotype (defined by absence of ER, PR, and HER2 expression) and their gene expression signatures are similar to those of normal basal/myoepithelial cells [59].
Studies investigating the role of PTHrP in BC progression have reported conflicting results. Our most recent in silico gene expression analyses using 36 public datasets and 5861 patients identified for the first time significant positive correlations between PTHLH expression and components of signaling pathways enriched in the triple-negative breast cancer (TNBC) subtypes including mesenchymal and luminal androgen receptor (LAR) subtypes [60, 61]. Notably, TNBC (ER, PR, and HER2 negative) is characterized by aggressive clinical course, increased rate of metastasis, and lack of targeted therapy, highlighting the need for novel prognostic biomarkers and molecular targets for this disease [62,63,64]. Therefore, we explored the clinical significance of PTHrP in TNBC using a population-based cohort of treatment-naive patients with newly diagnosed TNBC [65]. Immunohistochemical analysis of PTHrP expression in a tissue microarray constructed for 523 TNBC patients from this cohort revealed that PTHrP is overexpressed in 55.2% of TNBC tumors and its overexpression was significantly associated with decreased overall survival [66]. Consistent with our previously published results in the MMTV-PyMT mouse model, we found that loss of PTHrP expression dramatically prolongs tumor latency and slows tumor growth and metastasis [67]. Additionally, we developed a blocking monoclonal antibody against PTHrP and demonstrated that it could inhibit primary tumor growth and lung metastasis in a human BC xenograft model [67].
These data are in line with several studies showing that PTHrP expression in BC is correlated with poor patient survival [68,69,70,71,72]. In contrast, one study has suggested that PTHrP expression decreases the malignant potential of human breast tumors [73]. In this latter study, Henderson et al. carried out a 10-year prospective analysis of consecutive breast patients at the Breast Unit of St. Vincent’s Hospital in Australia, and found that positive PTHrP staining was an independent predictor of improved survival, and reduced metastasis at all sites [73]. Similarly, a study from the same group using an MMTV-neu BC mouse model found that disruption of PTHrP resulted in higher tumor occurrence [74].
By contrast, additional pre-clinical and clinical studies appear to support a detrimental role of PTHrP in tumor progression. First, one large genome-wide association study (GWAS) has implicated the PTHLH gene as a major BC susceptible locus [75]. Second, Kim et al. found that ablation of the calcium-sensing receptor (CaSR) in the MMTV-PyMT mouse model and in BC cell lines inhibited PTHrP expression and slowed tumor cell growth [76]. Their findings convincingly show that the CaSR-PTHrP pathway contributes to the growth of breast tumors in the MMTV-PyMT mice in vivo. They also documented a positive correlation between CaSR and PTHrP mRNA expression not only in this animal model but also in human samples [76]. This is particularly interesting since the MMTV-PyMT mouse model has been shown to share many characteristics of human basal-like cancer [77]. Finally, using RNAseq analyses, another group has shown that overexpression of PTHrP in MCF7 cells downregulates eight pro-dormancy genes likely through calcium signaling pathways in BC [78].
In summary, based on these observations, PTHrP appears to play a crucial role in BC development. The apparent divergent clinical results between the study published by Henderson et al. and other groups, including ours, could be attributed to features unique to this study, such as the ethnicity/race of the patients or the cut-off for PTHrP positivity in IHC staining analysis.
Pthlh Gene Ablation in Mammary Epithelial Cells and Its Consequences on Tumor Initiation, Growth, and Metastasis
PTHrP is expressed in normal mammary epithelial cells and its expression increased during BC development. To unravel the mechanistic role of PTHrP in BC initiation and progression, we ablated the Pthlh gene in mammary epithelial cells and examined its consequence on tumor progression in the MMTV-PyMT mouse model.
The MMTV-PyMT transgenic mouse is an excellent model mimicking many of the biological steps of human BC progression. Lin et al. identified four distinct BC stages, which are comparable to the human diseases from the premalignant stage to advanced disease [79]. Polyomavirus middle T antigen (PyMT) is a membrane-attached protein encoded by the mouse polyomavirus (PyV). PyV expresses three T antigens: a Large T (LT, 100-kDa), a Middle T (MT, 55-Kda), and a Small T (ST, 22-KDa), but only MT is the PyV oncogene that targets key cellular regulators promoting uncontrolled cell proliferation [80]. Previously, the MMTV-PyMT mouse model was regarded as being mainly associated with human luminal B subtype characterized by expression of the luminal K8/18, and overexpression of ErBB2 and low levels of ER [81]. However, a recently published paper showed that MMTV-PyMT mouse has heterogeneous transcriptomes with both luminal B and basal-like phenotypes [77]. During tumor progression, in MMTV-PyMT mouse model, ER and PR receptors status were lost whereas the HER2 receptor was overexpressed [79].
PyMT PTHrPflox/flox; Cre+ mT/mG Mouse Model
MMTV-Cre transgenic mice have been used extensively to obtain consistently high expression of Cre recombinase in the mammary epithelium [82]. To study the function of PTHrP in BC progression, we used a Cre-Lox recombination system to delete exon 4 of PTHrP [83]. Li et al. constructed Pthrpflox/flox; Cre+ (KO) tumor-bearing mouse model specifically inactivating the Pthlh gene in the mammary epithelium by crossing homozygous (flox/flox) Pthlh mice with MMTV-Cre; MMTV-PyMT mice [67].
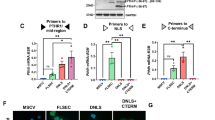
The availability of the conditional fluorescent reporter mouse model (mT/mG) has also enabled us to trace Cre expression at a cell-specific level [84]. In this model, the mT/mG reporter transgene is driven by a strong ubiquitous promotor (ACTB) from the well-characterized Gt(ROSA)26Sor genomic locus in which transgene expression of tdTomato (a red fluorescent protein) converts to the expression of enhanced green fluorescent protein (GFP) after Cre recombinase-mediated intramolecular rearrangement of the fluorescent protein-encoding transgene [84]. The activation of the GFP marks Cre expressing cells and all their descendants, since the ROSA26 promoter is expressed in all embryonic and adult mouse tissues [84]. We constructed Pthrpflox/flox; Cre+ and Pthrpwt/wt; Cre+ mT/mG mice models which can exclusively activate Cre expression in mammary epithelium and specifically express membrane-targeted GFP [85]. The advantage of this approach is to distinguish the membrane-targeted GFP from the membrane-targeted red fluorescent backlight of stromal and nonepithelial-derived mammary tissues during tumor progression (Fig. 5) [85]. Moreover, we will be able to trace and enrich the GFP-positive tumor cells from the primary site to the blood and metastatic site. This model will also help us to further investigate the mechanistic link between PTHrP and tumor progression process from initiation to metastasis .

Cell tracing approaches using PyMT, mT/mG mouse model . (a) H&E staining and immunofluorescence staining of tumor tissues at the three stages of tumor development in PyMT flox/flox;Cre + mT/mG mouse model (H hyperplasia, A adenoma, C carcinoma). (b) Methods of preparation of tumor cells for fluorescence-activated cell sorting
Role of PTHrP in Breast Cancer Metastasis to Bone
Almost 70% of advanced-stage BC patients will develop bone metastasis that is commonly associated with pain, hypercalcemia, and pathologic fractures [43]. In 1889, Dr. Stephen Paget proposed the “seed and soil” hypothesis, which states that disseminated tumor cells (“the seeds”) need the proper microenvironment (“the soil”) for them to grow [86]. Cancer metastasis is a complex and multi-step process that involves two major factors: tumor cells and the metastatic site. The tumor cells must detach from the primary tumor, lose their epithelial polarity, invade the basement membrane and extracellular matrix, reach the capillary blood, survive and finally extravasate into a distant site. The metastatic site plays a role as a fertile soil that provides sufficient support for tumor cells to grow. Once metastatic BC cells are in the bone marrow , they can effectively ‘hijack’ the normal bone homeostatic signals and therefore result in excessive osteoclast activation leading to enhanced bone resorption [43]. Current findings have revealed that there is a ‘vicious cycle’ in which metastatic cells residing in the bone marrow secrete factors that induce osteolytic bone resorption, and growth factors released from resorbed bone further stimulate tumor growth (Fig. 6).

PTHrP-dependent vicious cycle of bone metastasis. Tumor-derived PTHrP acts in a paracrine manner to stimulate osteoblasts within the bone microenvironment. Stimulated osteoblasts express RANKL, which binds to RANK on osteoclast precursors leading to the formation of multinucleated, bone-resorbing osteoclasts. Finally, osteoclastic bone resorption releases growth factors from the mineralized matrix (bone-derived growth factors), further enhancing tumor growth and survival. This creates a ‘vicious cycle’ in which tumor-derived PTHrP deregulates bone remodeling and accelerates bone resorption. This self-perpetuating cycle results in increased tumor burden and bone destruction
More than 50% primary BCs and 90% of bone metastasis show strong positivity for PTHrP expression [87]. These have provided the rationale that PTHrP expression in the bone marrow by BC cells promotes bone resorption and tumor cell growth. Due to the complexity of the vicious cycle in the bone metastatic process, the fundamental molecular mechanisms of the role of PTHrP in BC metastasis to bone remain elusive. Previous studies showed that PTHrP is a crucial regulator of bone metastasis and together with other growth factors such as TGF-β and chemokine C-C motif ligand 2 (CCL2) accelerates tumor growth and bone metastasis progression [88, 89]. A series of studies showed that overexpression of PTHrP converted human MCF7 BC cells from a dormant phenotype into a more aggressive metastatic phenotype [90]. Subsequent RNAseq analyses indicated that such overexpression of PTHrP in MCF7 cells downregulated several pro-dormancy genes [78]. The author further confirmed that differential gene expression responses to PTHrP overexpression do not signal through the activation of the cAMP/PKA/CREB pathway mediated by PTH1R [78]. Interestingly, the authors using RNAseq analyses found that the PTHrP overexpression upregulates calcium signaling pathway, but the specific intracellular pathways that mediate these non-PTH1R-mediated actions remain unknown [78]. It has also been shown that CaSR activation stimulated PTHrP production by breast cancer cells in vitro and in vivo which suggests that CaSR acts upstream of PTHrP [76]. These results raised a possibility that PTHrP exerts its osteolytic effect in bone through the activation CaSR signaling, possibly in a feed-forward loop. Furthermore, how exactly PTHrP produced by tumor cells interacts with other tumor-derived factors into the bone microenvironment is still unclear.
Role of PTHrP in Breast Cancer Metastasis to Brain
BC is the second most frequent cause of brain metastasis after lung cancer, with a risk of 10–16% in advanced BC patients [91]. Previous studies revealed that patients with TNBC or HER2-positive tumors have an increased risk of brain metastasis [91]. Brain metastasis from BC is a catastrophic event associated with a median survival of ~15 months despite treatment [91]. Identification of prognostic biomarkers associated with BC brain metastasis could be beneficial to identify patients at risk and inform appropriate clinical management decisions to improve their survival outcomes. Interestingly, we reported a strong association between high PTHrP expression in archived primary tumors of patients newly diagnosed with TNBC and higher propensity for brain progression [66]. These clinical results were also validated using in silico analyses, which showed that PTHLH expression positively correlated with signature genes not only involved in bone and lung metastasis in all BC subtypes examined but also, for the first time, correlated with brain metastatic genes: HBEGF (heparin-binding EGF-like growth factor) and ANGPTL4 (angiopoietin-like 4) selectively in TNBC and basal-like subtypes [60]. Collectively, these results reveal for the first time a possible role of PTHrP in TNBC-associated brain metastasis.
Summary and Conclusion
PTHrP was first discovered as the most common mediator of MAH. Subsequently, the discovery of its ubiquitous expression in normal tissues unraveled its role as a physiological autocrine/paracrine regulator. During the bone metastatic process, tumor-produced PTHrP plays a critical role in perpetuating the ‘vicious cycle’ that was created between the tumor cells and bone microenvironment. Furthermore, mounting evidence appears to indicate that PTHrP regulates most if not all the critical steps of tumor progression within and outside the skeleton. The strong correlation that we identified between PTHrP expression and breast cancer progression in addition to survival in TNBC suggests that PTHrP-targeted therapies representing a promising strategy, which should be further explored in this subtype with limited therapeutic options.
References
Mundy, G. R., & Edwards, J. R. (2008). PTH-related peptide (PTHrP) in hypercalcemia. Journal of the American Society of Nephrology, 19, 672–675.
Powell, D., Singer, F. R., Murray, T. M., et al. (1973). Nonparathyroid humoral hypercalcemia in patients with neoplastic diseases. The New England Journal of Medicine, 289, 176–181.
Strewler, G. J., Stern, P. H., Jacobs, J. W., et al. (1987). Parathyroid hormonelike protein from human renal carcinoma cells. Structural and functional homology with parathyroid hormone. The Journal of Clinical Investigation, 80, 1803–1807.
Burtis, W. J., Wu, T., Bunch, C., et al. (1987). Identification of a novel 17,000-dalton parathyroid hormone-like adenylate cyclase-stimulating protein from a tumor associated with humoral hypercalcemia of malignancy. The Journal of Biological Chemistry, 262, 7151–7156.
Moseley, J. M., Kubota, M., Diefenbach-Jagger, H., et al. (1987). Parathyroid hormone-related protein purified from a human lung cancer cell line. Proceedings of the National Academy of Sciences of the United States of America, 84, 5048–5052.
Suva, L. J., Winslow, G. A., Wettenhall, R. E., et al. (1987). A parathyroid hormone-related protein implicated in malignant hypercalcemia: Cloning and expression. Science, 237, 893–896.
Mangin, M., Ikeda, K., Dreyer, B. E., et al. (1988). Two distinct tumor-derived, parathyroid hormone-like peptides result from alternative ribonucleic acid splicing. Molecular Endocrinology, 2, 1049–1055.
Thiede, M. A., Strewler, G. J., Nissenson, R. A., et al. (1988). Human renal carcinoma expresses two messages encoding a parathyroid hormone-like peptide: Evidence for the alternative splicing of a single-copy gene. Proceedings of the National Academy of Sciences of the United States of America, 85, 4605–4609.
Yasuda, T., Banville, D., Hendy, G. N., et al. (1989). Characterization of the human parathyroid hormone-like peptide gene. Functional and evolutionary aspects. The Journal of Biological Chemistry, 264, 7720–7725.
Martin, T. J. (2016). Parathyroid hormone-related protein, its regulation of cartilage and bone development, and role in treating bone diseases. Physiological Reviews, 96, 831–871.
Mangin, M., Ikeda, K., & Broadus, A. E. (1990). Structure of the mouse gene encoding parathyroid hormone-related peptide. Gene, 95, 195–202.
Karaplis, A. C., Yasuda, T., Hendy, G. N., et al. (1990). Gene-encoding parathyroid hormone-like peptide: Nucleotide sequence of the rat gene and comparison with the human homologue. Molecular Endocrinology, 4, 441–446.
Thiede, M. A., & Rutledge, S. J. (1990). Nucleotide sequence of a parathyroid hormone-related peptide expressed by the 10 day chicken embryo. Nucleic Acids Research, 18, 3062.
Power, D. M., Ingleton, P. M., Flanagan, J., et al. (2000). Genomic structure and expression of parathyroid hormone-related protein gene (PTHrP) in a teleost, Fugu rubripes. Gene, 250, 67–76.
Orloff, J. J., Wu, T. L., & Stewart, A. F. (1989). Parathyroid hormone-like proteins: Biochemical responses and receptor interactions. Endocrine Reviews, 10, 476–495.
Karaplis, A. C., & Goltzman, D. (2000). PTH and PTHrP effects on the skeleton. Reviews in Endocrine & Metabolic Disorders, 1, 331–341.
Ohshima, K., Takeda, S., Hirose, M., et al. (2012). Structure-function relationship of the nuclear localization signal sequence of parathyroid hormone-related protein. Biomedical Research, 33, 191–199.
Lam, M. H., Thomas, R. J., Martin, T. J., et al. (2000). Nuclear and nucleolar localization of parathyroid hormone-related protein. Immunology and Cell Biology, 78, 395–402.
Lam, M. H., Hu, W., Xiao, C. Y., et al. (2001). Molecular dissection of the importin beta1-recognized nuclear targeting signal of parathyroid hormone-related protein. Biochemical and Biophysical Research Communications, 282, 629–634.
Cingolani, G., Bednenko, J., Gillespie, M. T., et al. (2002). Molecular basis for the recognition of a nonclassical nuclear localization signal by importin beta. Molecular Cell, 10, 1345–1353.
Massfelder, T., Dann, P., Wu, T. L., et al. (1997). Opposing mitogenic and anti-mitogenic actions of parathyroid hormone-related protein in vascular smooth muscle cells: A critical role for nuclear targeting. Proceedings of the National Academy of Sciences of the United States of America, 94, 13630–13635.
Soki, F. N., Park, S. I., & McCauley, L. K. (2012). The multifaceted actions of PTHrP in skeletal metastasis. Future Oncology, 8, 803–817.
Fenton, A. J., Kemp, B. E., Hammonds, R. G., Jr., et al. (1991). A potent inhibitor of osteoclastic bone resorption within a highly conserved pentapeptide region of parathyroid hormone-related protein; PTHrP[107-111]. Endocrinology, 129, 3424–3426.
Fenton, A. J., Kemp, B. E., Kent, G. N., et al. (1991). A carboxyl-terminal peptide from the parathyroid hormone-related protein inhibits bone resorption by osteoclasts. Endocrinology, 129, 1762–1768.
Fenton, A. J., Martin, T. J., & Nicholson, G. C. (1994). Carboxyl-terminal parathyroid hormone-related protein inhibits bone resorption by isolated chicken osteoclasts. Journal of Bone and Mineral Research, 9, 515–519.
de Miguel, F., Fiaschi-Taesch, N., López-Talavera, J. C., et al. (2001). The C-terminal region of PTHrP, in addition to the nuclear localization signal, is essential for the intracrine stimulation of proliferation in vascular smooth muscle cells. Endocrinology, 142, 4096–4105.
Budayr, A. A., Halloran, B. P., King, J. C., et al. (1989). High levels of a parathyroid hormone-like protein in milk. Proceedings of the National Academy of Sciences of the United States of America, 86, 7183–7185.
Kovacs, C. S., Lanske, B., Hunzelman, J. L., et al. (1996). Parathyroid hormone-related peptide (PTHrP) regulates fetal-placental calcium transport through a receptor distinct from the PTH/PTHrP receptor. Proceedings of the National Academy of Sciences of the United States of America, 93, 15233–15238.
Wysolmerski, J. J. (2012). Parathyroid hormone-related protein: An update. The Journal of Clinical Endocrinology and Metabolism, 97, 2947–2956.
Wysolmerski, J. J., Cormier, S., Philbrick, W. M., et al. (2001). Absence of functional type 1 parathyroid hormone (PTH)/PTH-related protein receptors in humans is associated with abnormal breast development and tooth impaction. The Journal of Clinical Endocrinology and Metabolism, 86, 1788–1794.
Hens, J. R., & Wysolmerski, J. J. (2005). Key stages of mammary gland development: Molecular mechanisms involved in the formation of the embryonic mammary gland. Breast Cancer Research, 7, 220–224.
Hens, J., Dann, P., Hiremath, M., et al. (2009). Analysis of gene expression in PTHrP−/− mammary buds supports a role for BMP signaling and MMP2 in the initiation of ductal morphogenesis. Developmental Dynamics, 238, 2713–2724.
Hens, J. R., Dann, P., Zhang, J. P., et al. (2007). BMP4 and PTHrP interact to stimulate ductal outgrowth during embryonic mammary development and to inhibit hair follicle induction. Development, 134, 1221–1230.
Karaplis, A. C., Luz, A., Glowacki, J., et al. (1994). Lethal skeletal dysplasia from targeted disruption of the parathyroid hormone-related peptide gene. Genes & Development, 8, 277–289.
Schipani, E., Langman, C., Hunzelman, J., et al. (1999). A novel parathyroid hormone (PTH)/PTH-related peptide receptor mutation in Jansen’s metaphyseal chondrodysplasia. The Journal of Clinical Endocrinology and Metabolism, 84, 3052–3057.
Schipani, E., Lanske, B., Hunzelman, J., et al. (1997). Targeted expression of constitutively active receptors for parathyroid hormone and parathyroid hormone-related peptide delays endochondral bone formation and rescues mice that lack parathyroid hormone-related peptide. Proceedings of the National Academy of Sciences of the United States of America, 94, 13689–13694.
Weir, E. C., Philbrick, W. M., Amling, M., et al. (1996). Targeted overexpression of parathyroid hormone-related peptide in chondrocytes causes chondrodysplasia and delayed endochondral bone formation. Proceedings of the National Academy of Sciences of the United States of America, 93, 10240–10245.
Lanske, B., Karaplis, A. C., Lee, K., et al. (1996). PTH/PTHrP receptor in early development and Indian hedgehog-regulated bone growth. Science, 273, 663–666.
Jobert, A. S., Zhang, P., Couvineau, A., et al. (1998). Absence of functional receptors for parathyroid hormone and parathyroid hormone-related peptide in Blomstrand chondrodysplasia. The Journal of Clinical Investigation, 102, 34–40.
Miao, D., Su, H., He, B., et al. (2008). Severe growth retardation and early lethality in mice lacking the nuclear localization sequence and C-terminus of PTH-related protein. Proceedings of the National Academy of Sciences of the United States of America, 105, 20309–20314.
Amizuka, N., Warshawsky, H., Henderson, J. E., et al. (1994). Parathyroid hormone-related peptide-depleted mice show abnormal epiphyseal cartilage development and altered endochondral bone formation. The Journal of Cell Biology, 126, 1611–1623.
Amizuka, N., Karaplis, A. C., Henderson, J. E., et al. (1996). Haploinsufficiency of parathyroid hormone-related peptide (PTHrP) results in abnormal postnatal bone development. Developmental Biology, 175, 166–176.
Guise, T. A., Kozlow, W. M., Heras-Herzig, A., et al. (2005). Molecular mechanisms of breast cancer metastases to bone. Clinical Breast Cancer, 5, S46–S53.
Yasuda, H., Shima, N., Nakagawa, N., et al. (1999). A novel molecular mechanism modulating osteoclast differentiation and function. Bone, 25, 109–113.
Sternlicht, H., & Glezerman, I. G. (2015). Hypercalcemia of malignancy and new treatment options. Therapeutics and Clinical Risk Management, 11, 1779–1788.
Ralston, S. H., Cowan, R. A., Robertson, A. G., et al. (1984). Circulating vitamin D metabolites and hypercalcaemia of malignancy. Acta Endocrinologica, 106, 556–563.
Schweitzer, D. H., Hamdy, N. A., Frölich, M., et al. (1994). Malignancy-associated hypercalcaemia: Resolution of controversies over vitamin D metabolism by a pathophysiological approach to the syndrome. Clinical Endocrinology, 41, 251–256.
Donovan, P. J., Achong, N., Griffin, K., et al. (2015). PTHrP-mediated hypercalcemia: Causes and survival in 138 patients. The Journal of Clinical Endocrinology and Metabolism, 100, 2024–2029.
Kremer, R., & Goltzman, D. (2017). Parathyroid hormone-related peptide and other mediators of skeletal manifestations of malignancy. In Principles of bone biology. Cambridge: Elsevier.
Kremer, R., Li, J., Camirand, A., & Karaplis, A. C. (2011). Parathyroid hormone related protein (PTHrP) in tumor progression. Advances in Experimental Medicine and Biology, 720, 145–160.
Truong, N. U., deB Edwardes, M. D., Papavasiliou, V., et al. (2003). Parathyroid hormone-related peptide and survival of patients with cancer and hypercalcemia. The American Journal of Medicine, 115, 115–121.
Hiraki, A., Ueoka, H., Bessho, A., et al. (2002). Parathyroid hormone-related protein measured at the time of first visit is an indicator of bone metastases and survival in lung carcinoma patients with hypercalcemia. Cancer, 95, 1706–1713.
Pecherstorfer, M., Schilling, T., Blind, E., et al. (1994). Parathyroid hormone-related protein and life expectancy in hypercalcemic cancer patients. The Journal of Clinical Endocrinology and Metabolism, 78, 1268–1270.
Burtis, W. J., Brady, T. G., Orloff, J. J., et al. (1990). Immunochemical characterization of circulating parathyroid hormone-related protein in patients with humoral hypercalcemia of cancer. The New England Journal of Medicine, 322, 1106–1112.
Otieno, B. A., Krause, C. E., Jones, A. L., et al. (2016). Cancer diagnostics via ultrasensitive multiplexed detection of parathyroid hormone-related peptides with a microfluidic immunoarray. Analytical Chemistry, 88, 9269–9275.
Castellano, D., Sepulveda, J. M., García-Escobar, I., et al. (2011). The role of RANK-ligand inhibition in cancer: The story of denosumab. The Oncologist, 16, 136–145.
Ogata, E. (2000). Parathyroid hormone-related protein as a potential target of therapy for cancer-associated morbidity. Cancer, 88(12 Suppl), 2909–2911.
Vargo-Gogola, T., & Rosen, J. M. (2007). Modelling breast cancer: One size does not fit all. Nature Reviews. Cancer, 7, 659–672.
Badve, S., Dabbs, D. J., Schnitt, S. J., et al. (2011). Basal-like and triple-negative breast cancers: A critical review with an emphasis on the implications for pathologists and oncologists. Modern Pathology, 24, 157–167.
Assaker, G., Camirand, A., Sabri, S., et al. (2018). In silico gene expression analysis of PTHrP and its association with molecular subtypes and organ-specifıc metastasis in human triple-negative breast cancer [abstract]. In Proceedings of the 109th annual meeting of the American Association for Cancer Research; April 14–18. Chicago, IL: AACR. Abstract no. 2598.
Jézéquel, P., Frénel, J. S., Campion, L., et al. (2013). bc-GenExMiner 3.0: New mining module computes breast cancer gene expression correlation analyses. Database: The Journal of Biological Databases and Curation, 2013, bas060.
Bauer, K. R., Brown, M., Cress, R. D., et al. (2007). Descriptive analysis of estrogen receptor (ER)-negative, progesterone receptor (PR)-negative, and HER2-negative invasive breast cancer, the so-called triple-negative phenotype: A population-based study from the California cancer registry. Cancer, 109, 1721–1728.
Sorlie, T., Perou, C. M., Tibshirani, R., et al. (2001). Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proceedings of the National Academy of Sciences of the United States of America, 98, 10869–10874.
Viale, G. (2012). The current state of breast cancer classification. Annals of Oncology, 23(Suppl 10), x207–x210.
Abdulkarim, B. S., Cuartero, J., Hanson, J., et al. (2011). Increased risk of locoregional recurrence for women with T1-2N0 triple-negative breast cancer treated with modified radical mastectomy without adjuvant radiation therapy compared with breast-conserving therapy. Journal of Clinical Oncology, 29, 2852–2858.
Assaker, G., Camirand, A., Abdulkarim, B., et al. (2018). Identifıcation of PTHrP as a biomarker of short survival & brain metastasis in a tissue microarray retrospective analysis of triple-negative breast cancer [abstract]. In Proceedings of the 109th annual meeting of the American Association for Cancer Research; April 14–18. Chicago, IL: AACR. Abstract no. 2632.
Li, J., Karaplis, A. C., Huang, D. C., et al. (2011). PTHrP drives breast tumor initiation, progression, and metastasis in mice and is a potential therapy target. The Journal of Clinical Investigation, 121, 4655–4669.
Bouizar, Z., Spyratos, F., Deytieux, S., et al. (1993). Polymerase chain reaction analysis of parathyroid hormone-related protein gene expression in breast cancer patients and occurrence of bone metastases. Cancer Research, 53, 5076–5078.
Kohno, N., Kitazawa, S., Fukase, M., et al. (1994). The expression of parathyroid hormone-related protein in human breast cancer with skeletal metastases. Surgery Today, 24, 215–220.
Linforth, R., Anderson, N., Hoey, R., et al. (2002). Coexpression of parathyroid hormone related protein and its receptor in early breast cancer predicts poor patient survival. Clinical Cancer Research, 8, 3172–3177.
Takagaki, K., Takashima, T., Onoda, N., et al. (2012). Parathyroid hormone-related protein expression, in combination with nodal status, predicts bone metastasis and prognosis of breast cancer patients. Experimental and Therapeutic Medicine, 3, 963–968.
Xu, C., Wang, Z., Cui, R., et al. (2015). Co-expression of parathyroid hormone related protein and TGF-beta in breast cancer predicts poor survival outcome. BMC Cancer, 15, 925.
Henderson, M. A., Danks, J. A., Slavin, J. L., et al. (2006). Parathyroid hormone-related protein localization in breast cancers predict improved prognosis. Cancer Research, 66, 2250–2256.
Fleming, N. I., Trivett, M. K., George, J., et al. (2009). Parathyroid hormone-related protein protects against mammary tumor emergence and is associated with monocyte infiltration in ductal carcinoma in situ. Cancer Research, 69, 7473–7479.
Ghoussaini, M., Fletcher, O., Michailidou, K., et al. (2012). Genome-wide association analysis identifies three new breast cancer susceptibility loci. Nature Genetics, 44, 312–318.
Kim, W., Takyar, F. M., Swan, K., et al. (2016). Calcium-sensing receptor promotes breast cancer by stimulating Intracrine actions of parathyroid hormone-related protein. Cancer Research, 76, 5348–5360.
Hollern, D. P., Swiatnicki, M. R., & Andrechek, E. R. (2018). Histological subtypes of mouse mammary tumors reveal conserved relationships to human cancers. PLoS Genetics, 14, e1007135.
Johnson, R. W., Sun, Y., Ho, P. W. M., et al. (2018). Parathyroid hormone-related protein negatively regulates tumor cell dormancy genes in a PTHR1/cyclic AMP-independent manner. Frontiers in Endocrinology (Lausanne), 9, 241.
Lin, E. Y., Jones, J. G., Li, P., et al. (2003). Progression to malignancy in the polyoma middle T oncoprotein mouse breast cancer model provides a reliable model for human diseases. The American Journal of Pathology, 163, 2113–2126.
Dilworth, S. M. (2002). Polyoma virus middle T antigen and its role in identifying cancer-related molecules. Nature Reviews. Cancer, 2, 951–956.
Fluck, M. M., & Schaffhausen, B. S. (2009). Lessons in signaling and tumorigenesis from polyomavirus middle T antigen. Microbiology and Molecular Biology Reviews, 73, 542–563.
Wagner, K. U., McAllister, K., Ward, T., et al. (2001). Spatial and temporal expression of the Cre gene under the control of the MMTV-LTR in different lines of transgenic mice. Transgenic Research, 10, 545–553.
He, B., Deckelbaum, R. A., Miao, D., et al. (2001). Tissue-specific targeting of the pthrp gene: The generation of mice with floxed alleles. Endocrinology, 142, 2070–2077.
Muzumdar, M. D., Tasic, B., Miyamichi, K., et al. (2007). A global double-fluorescent Cre reporter mouse. Genesis, 45, 593–605.
Zhang, R., Li, J., Badescu, D., et al. (2018). PTHrP drives tumor initiation signaling pathways in the PyMT model of breast cancer progression [abstract]. In Proceedings of the 109th annual meeting of the American Association for Cancer Research; 2018 April 14–18. Chicago IL: AACR. Abstract no. 1995.
Paget, S. (1989). The distribution of secondary growths in cancer of the breast. 1889. Cancer Metastasis Reviews, 8, 98–101.
McCauley, L. K., & Martin, T. J. (2012). Twenty-five years of PTHrP progress: From cancer hormone to multifunctional cytokine. Journal of Bone and Mineral Research, 27, 1231–1239.
Li, X., Loberg, R., Liao, J., et al. (2009). A destructive cascade mediated by CCL2 facilitates prostate cancer growth in bone. Cancer Research, 69, 1685–1692.
Yin, J. J., Selander, K., Chirgwin, J. M., et al. (1999). TGF-beta signaling blockade inhibits PTHrP secretion by breast cancer cells and bone metastases development. The Journal of Clinical Investigation, 103, 197–206.
Johnson, R. W., Finger, E. C., Olcina, M. M., et al. (2016). Induction of LIFR confers a dormancy phenotype in breast cancer cells disseminated to the bone marrow. Nature Cell Biology, 18, 1078–1089.
Rostami, R., Mittal, S., Rostami, P., et al. (2016). Brain metastasis in breast cancer: A comprehensive literature review. Journal of Neuro-Oncology, 127, 407–414.
Acknowledgments
This study was supported by grants from the Canadian Institutes for Health Research (CIHR MOP142287; MOP130370) and the U.S. Department of Defense Breast Cancer Research Program (W81XWH-15-1-0723) to R. Kremer.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Zhang, R. et al. (2019). Parathyroid Hormone-Related Protein (PTHrP): An Emerging Target in Cancer Progression and Metastasis. In: Rhim, J., Dritschilo, A., Kremer, R. (eds) Human Cell Transformation. Advances in Experimental Medicine and Biology, vol 1164. Springer, Cham. https://doi.org/10.1007/978-3-030-22254-3_13
Download citation
DOI: https://doi.org/10.1007/978-3-030-22254-3_13
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-22253-6
Online ISBN: 978-3-030-22254-3
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)