
Abstract
The anatomy of the neurovascular system is presented. The aortic arch and great vessels, common carotid arteries, external carotid artery, internal carotid artery, circle of Willis, vertebral artery, basilar artery, venous system, and spinal neurovascular anatomy are discussed.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Posterior Inferior Cerebellar Artery (PICA)
- Middle Deep Temporal Artery
- Accessory Meningeal Artery
- Transverse Facial Artery
- Anterior Inferior Cerebellar Artery (AICA)
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Aortic Arch and Great Vessels
Aortic arch anatomy is pertinent to neuroangiography because variations of arch anatomy can affect access to the cervicocranial circulation:
-
1)
Branches
-
a)
Innominate (aka brachiocephalic) artery
-
b)
Left common carotid artery
-
c)
Left subclavian artery
-
a)
-
2)
Variants (Fig. 1.1):
Fig. 1.1 
Common aortic arch configurations. Clockwise from upper left: (a) Normal arch; (b) bovine arch; (c) aberrant right subclavian artery, and (d) origin of the left vertebral artery from the arch
-
a)
Bovine arch (Figs. 1.1b and 1.2). The innominate artery and left common carotid artery (CCA) share a common origin (up to 27% of cases), or the left CCA arises from the innominate artery (7% of cases).1 The bovine variant is more common in blacks (10–25%) than whites (5–8%).2
Fig. 1.2 
What exactly is a “bovine arch?” Drawing of an arch from a cow. In cattle, a single great vessel originates from the aortic arch286. Presumably, the long brachiocephalic artery is due to the relatively long distance from the aorta to the thoracic inlet in cattle. Because humans do not have a true “bovine arch,” Layton and colleagues proposed that the more precise term, “Common-Origin-of-the-Innominate-Artery-and-Left-Common-Carotid-Artery” and “Origin-of-the-Left-Common-Carotid-Artery-from-the-Innominate-Artery” supplant the term bovine arch287. This is akin to proposing that the universally understood term, “p-comm aneurysm” be replaced by the more accurate “aneurysm-arising-from-the-internal-carotid-artery-adjacent-to-the-origin-of-the-posterior-communicating-artery.” The authors of this handbook will continue to use the well understood but anatomically imprecise terms, bovine arch and p-comm aneurysm
-
b)
Aberrant right subclavian artery. The right subclavian artery arises from the left aortic arch, distal to the origin of the left subclavian artery. It usually passes posterior to the esophagus on its way to the right upper extremity. This is the most common congenital arch anomaly, incidence: 0.9%3 associated with Down syndrome.
-
c)
Origin of the left vertebral artery from the arch is seen in 0.5% of cases.1
-
d)
Less common variants (Fig. 1.3). Some of these rare anomalies can lead to formation of a vascular ring in which the trachea and esophagus are encircled by connecting segments of the aortic arch and its branches.
Fig. 1.3 
Selected aortic arch anomalies. (a) Double aortic arch. The arches encircle the trachea and esophagus to form the descending aorta, which is usually on the left. The right arch is larger than the left in up to 75% of cases1. (b) Double aortic arch with left arch atresia. (c) Right aortic arch with a mirror configuration. The descending aorta is on the right side of the heart. This anomaly does not form a vascular ring, but is associated with other anomalies such as tetralogy of Fallot1. (d) Right aortic arch with a nonmirror configuration and an aberrant left subclavian artery. The descending aorta is on the right side of the heart, and the left subclavian artery arises from the proximal aorta. A common cause of a symptomatic vascular ring288. (e) Bi-innominate artery
-
a)
-
3)
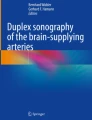
Effects of aging and atherosclerosis on the aortic arch and great vessels. The aortic arch and great vessels become elongated and tortuous with age (Fig. 1.4); this can have practical implications for neurointervention in the elderly, as a tortuous vessel can be difficult to negotiate with wires and catheters. Although atherosclerosis has been implicated in the etiology of this phenomenon, more recent data suggest that the cervical internal carotid artery (ICA) may undergo metaplastic transformation, in which elastic and muscular tissue in the artery wall is replaced by loose connective tissue.4
Fig. 1.4 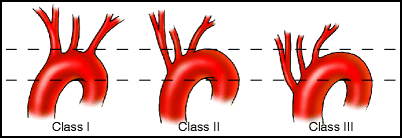
Aortic arch elongation classification scheme




The most common subclavian artery configuration is shown in Fig. 1.5. Major branches are:

Subclavian artery
-
Vertebral artery (1)
-
Thyrocervical trunk
-
Inferior thyroid artery (2)
-
Ascending cervical artery (most commonly a branch of transverse cervical) (3)
-
Transverse cervical artery (4)
-
Suprascapular artery (5)
-
-
Costocervical trunk
-
Deep cervical artery (6)
-
Superior or supreme intercostal artery (7)
-
-
Dorsal scapular artery (may also arise from transverse cervical)5 (8)
-
Internal thoracic (mammary) artery (9)
2 Common Carotid Arteries
The CCAs travel within the carotid sheath, which also contains the internal jugular vein and the vagus nerve. The right CCA is usually shorter than the left. The CCAs typically bifurcate at the C3 or C4 level (upper border of the thyroid cartilage), although the bifurcation may be located anywhere between T2 and C2.6 The CCAs do not usually have branches, although anomalous branches can include the superior thyroid, ascending pharyngeal, or occipital arteries.1
3 External Carotid Artery
The external carotid artery (ECA) originates at the common carotid bifurcation. From its origin, the ECA usually curves forward medial to the internal carotid, then immediately begins a cephalad ascent, curving laterally and slightly posteriorly until it ends behind the mandible in its terminal bifurcation into the internal maxillary and superficial temporal arteries.7 Thus, on a frontal radiographic view, the external carotid begins medially and swings cephalad and laterally, and on a lateral view it begins anteriorly and then ascends, angling slightly posteriorly.
Mnemonic for the external carotid |
|---|
Branches |
After reading this book … |
Some Angry Linguists Find Our Paragraphs |
Somewhat Irritating |
Superior thyroid |
Ascending pharyngeal |
Lingual |
Facial |
Occipital |
Posterior auricular |
Superficial temporal |
Internal maxillary |
More amusing and off-color mnemonics are available to assist the novice in remembering these branches. If the readers’ imaginations fail them, the authors would be more than happy to supply additional memory aids for this purpose |
-
1.
Branches
There are eight major branches of the ECA (Fig. 1.6). Commonly, the branches are listed in order by their point of origin from proximal to distal.

External carotid artery. (1) Superior thyroid artery; (2) ascending pharyngeal artery; (3) lingual artery; (4) facial artery; (5) posterior auricular artery; (6) internal maxillary artery; (7) occipital artery; (8) superficial temporal artery
-
1.
Superior thyroid artery
-
2.
Ascending pharyngeal artery
-
3.
Lingual artery
-
4.
Facial artery
-
5.
Occipital artery
-
6.
Posterior auricular artery
-
7.
Superficial temporal artery
-
8.
Internal maxillary artery
Occasionally, these branches arise from the ECA trunk. The ventral group arises anteriorly from the ECA and the dorsal group of branches arises posteriorly from the ECA. Therefore, grouping the ECA branches based on their ventral or dorsal axis is more useful and more consistent.
Ventral external carotid branches:
-
Superior thyroid artery
-
Lingual artery
-
Facial artery
-
Internal maxillary artery
Dorsal external carotid branches
-
Ascending pharyngeal artery
-
Occipital artery
-
Posterior auricular artery
-
Superficial temporal artery
-
4.
Territories
The ECA supplies much of the soft tissue and bony structures of the head and face, the deep structures of the upper aero-digestive tract, and much of the dura of the intracranial compartment. Numerous anastamoses are present between ECA branches and the branches of the internal carotid and vertebral arteries. These anastamoses provide collateral flow to the vascular territories distal to a proximal occlusion. Anastamoses to carotid or vertebral arteries can also be considered “dangerous anastamoses” when attempting to embolize vascular lesions in the head and neck via external carotid branches. See below for discussion of individual ECA branch anastamoses and Tables 1.1, 1.2, 1.3, and 1.4.
Table 1.1 Anastamoses to anterior circulation Table 1.2 Common anastamoses to ophthalmic artery Table 1.3 Common anastamoses to posterior circulation Table 1.4 More trouble: cranial nerve blood supply -
5.
Variants:
-
(a)
The most frequent branching pattern seen at the common carotid bifurcation (in 48.5%) is the external carotid arises anteromedially while the internal carotid arises posterolaterally. The most frequent branching pattern seen at the common carotid bifurcation finds the external carotid arising anteromedially. Occasionally, the ECA arises posterolaterally or directly laterally.8,9
-
(b)
The ECA and ICA may rarely arise as separate branches of the aortic arch.7,10
-
(c)
Some ECA branches, especially the superior thyroid artery, may arise from the CCA.
-
(d)
Some branches (especially the ascending pharyngeal or occipital arteries) may originate from the ICA.
-
(e)
A common origin of superior thyroid, occipital, and ascending pharyngeal arteries from the ICA has been reported.11
-
(f)
Rarely, all external carotid branches may arise from the ICA.12
-
(g)
External carotid branches may arise as common trunks with other branches including: linguofacial trunk (20% of cases), thyrolingual trunk (2.5% of cases), thyrolinguofacial trunk (2.5% of cases), and occipitoauricular trunk (12.5% of cases).13
-
(h)
Persistent stapedial artery,14 or, for the anatomic purist, the persistent hyoido-stapedial artery,15 arises from the petrous ICA, passes through the middle ear, and forms the middle meningeal. The prevalence of persistent stapedial arteries in 1,000 temporal bones that were studied was 0.48%.16 This anomaly can be associated with the so-called aberrant course of the ICA in the middle ear, which probably really represents a collateral pathway involving the inferior tympanic branch of the ascending pharyngeal artery bypassing a segmental agenesis of the true ICA.17,18
-
(a)
3.1 Superior Thyroid Artery
Whether it arises above or below the common carotid bifurcation, the superior thyroid artery originates from the anterior surface of the parent artery and immediately turns caudally to supply the anterior soft tissue structures of the neck.
-
1.
Branches
-
(a)
Infrahyoid artery
The infrahyoid (hyoid) artery travels medially from its origin, and then follows along the lower hyoid bone. It can anastamose with the submental artery, providing a collateral pathway to the facial artery.19
-
(b)
Superior laryngeal artery
The superior laryngeal artery travels alongside the internal laryngeal nerve inferomedially from its origin and pierces the thyrohyoid membrane to supply the mucosa of the larynx superior to the vocal cords and taste buds of the epiglottis.20
-
i.
Branches
The superior thyroid artery has two major branches and a small epiglottic branch. Its ventral branch anastomoses with the both the cricothyroid artery and superior laryngeal arcade. The dorsal branch anastamoses with the longitudinal laryngeal arcade.19
-
ii.
Territory
The superior laryngeal artery supplies the pharyngeal and laryngeal structures as well as the internal laryngeal nerve. It anastamoses with its contralateral partner and with the inferior laryngeal artery from the inferior thyroid artery.
-
iii.
Variants
-
i.
-
(c)
Sternocleidomastoid artery
The sternocleidomastoid artery feeds the middle part of the sternocleidomastoid muscle. It anastamoses superiorly with the muscular branches of the occipital and posterior auricular and inferiorly with the thyrocervical trunk and suprascapular. It can also connect with the glandular branches of the superior thyroid artery.
-
(d)
Cricothyroid artery
Anastamoses with the superior laryngeal artery and feeds the upper trachea.
-
(e)
Glandular branches
These are a continuation of the superior thyroid trunk with superior, medial and lateral arcades to supply the thyroid gland. They freely anastamose with their contralateral counterparts.
-
(a)
-
2.
Territories
-
(a)
The superior thyroid artery supplies the majority of the blood to the larynx, its associated musculature, and the upper pole of the thyroid gland.7 In a minority of cases the superior thyroid provides blood flow to the parathyroid glands.22 The superior laryngeal branch accompanies and can supply the internal laryngeal nerve. The superior thyroid branches freely anastamose with their contralateral counterparts and the inferior thyroid artery (from the thyrocervical trunk).
-
(a)
-
3.
Variants
3.2 Ascending Pharyngeal Artery
The ascending pharyngeal artery is a thin, slender branch that arises from the very proximal posterior aspect of the ECA or in the crotch of the CCA (Fig. 1.7). It travels cephalad parallel to the ICA. Its termination in the superior pharynx creates a forward and medial right angle turn.

Ascending pharyngeal artery. A common branching pattern of the ascending pharyngeal artery is shown. Note internal carotid (ICA), external carotid (ECA), superior thyroid (STh), ascending pharyngeal (AscPh), inferior pharyngeal (IP), middle pharyngeal (MP), superior pharyngeal (SP), inferior tympanic (IT), musculospinal branches (MS), neuromeningeal trunk (NMT), jugular branch (JB) entering the jugular foramen, hypoglossal branch (HG) entering the hypoglossal foramen, and prevertebral (not shown)
-
1.
Branches
-
(a)
Inferior pharyngeal artery
A relatively small vessel arising from the proximal ascending pharyngeal, the inferior pharyngeal travels anteriorly in a zigzag fashion. It supplies the pharyngeal muscles and mucosa. It anastamoses with its contralateral counterpart.
-
(b)
Musculospinal artery
The vessel may arise from the ascending pharyngeal itself or from the neuromeningeal trunk. It extends posteriorly and superiorly for a short distance before curving inferiorly. It primarily supplies muscles, but also may supply the ipsilateral upper spinal nerve roots, the eleventh cranial nerve, and superior sympathetic ganglion. In addition, it may anastamose with the ascending and deep cervical and vertebral arteries.19,24
-
(c)
Neuromeningeal trunk
This is a major branch of the ascending pharyngeal artery that continues cephalad but angles gently to the posterior. It has several important branches that pass through foramina in the skull base.
-
(i)
Branches
-
Musculospinal artery
This branch may variably arise from the neuromeningeal trunk instead of originating from the ascending pharyngeal artery.
-
Jugular artery
Often the largest branch of the neuromeningeal trunk, this vessel heads straight cephalad to the jugular foramen. It supplies the ninth through the eleventh cranial nerves and their ganglia. A medial branch ascends on the clivus to supply the eleventh cranial nerve. Its lateral branch travels along the dura around the sigmoid sinus. It can be a major contributor to the dura of the posterior fossa. Anastamoses with the lateral clival branch of the meningohypohyseal trunk and dural branches of the vertebral artery are possible.19
-
Hypoglossal artery
This branch enters the hypoglossal canal and supplies the twelfth cranial nerve. It also supplies the dura in the posterior cranial fossa and anastamoses with the jugular branch, medial clival branches of the meningohypohyseal trunk, the contralateral hypoglossal artery, and the odontoid arcade.19,25
-
Prevertebral artery
It often arises from the neuromeningeal trunk and contributes to the odontoid arcade. It anastamoses with its contralateral counterpart, the anterior meningeal branch of the vertebral and hypoglossal artery branches.25
-
-
ii.
Territories
The very important neuromeningeal trunk of the ascending pharyngeal artery supplies cranial nerves VI, IX, X, XI, and XII, and potentially collateralizes to the upper three spinal nerves and the superior sympathetic ganglion. Its meningeal territory includes a large portion of the posterior fossa meninges. Anastamotic channels exist to its contralateral counterpart and meningeal branches of the vertebral artery and the meningohypophyseal trunk.24
-
iii.
Variants
All branches of the neuromeningeal trunk are in vascular equilibrium with each other and with their anastamotic connecting vessels. Hypoplasia or absence of one or more vessels is accompanied by hypertrophy of the existing branches.
-
(i)
-
(d)
Prevertebral artery
Occasionally, this artery arises directly from the ascending pharyngeal artery and contributes to the odontoid arcade.25
-
(e)
Inferior tympanic artery
-
i.
Branches
There are three common branches of the inferior tympanic artery.19
-
Ascending branch connects to petrosal branch of middle meningeal artery
-
Anterior branch connects to the caroticotympanic branch
-
Posterior branch connects to the stylomastoid artery, a branch of the posterior auricular artery
-
-
ii.
Territories
Supplies the middle ear cavity and associated nerves, including the twelfth nerve and tympanic branch of the ninth cranial nerve (aka Jacobson’s nerve).
-
iii.
Variants
May arise from the neuromeningeal branch, the ascending pharyngeal artery, or it may appear as a trifurcation with the inferior tympanic artery arising in between neuromeningeal and pharyngeal divisions.19
-
i.
-
(f)
Middle pharyngeal artery
-
i.
Branches
No named branches.
-
ii.
Territories
Supplies mucosa and muscles of the naso- and oropharynx as well as the soft palate.26 Anastamoses with contralateral middle pharyngeal artery, ipsilateral ascending palatine artery, greater palatine artery, and branches of the accessory meningeal artery.
-
iii.
Variants
May arise from ascending pharyngeal artery proximal or occasionally distal to the origin of neuromeningeal trunk.
-
i.
-
(g)
Superior pharyngeal artery
As the most cephalad anterior branch of the ascending pharyngeal artery, this tends to be a small vessel. The pharyngeal branches take an abrupt anterior and medial angulation from the vertical ascending pharyngeal artery.
-
i.
Branches
There are several common branches of the superior pharyngeal artery, but only one is named.
-
The carotid branch actually traverses the cartilage filling the foramen lacerum and connects to the cavernous ICA via the inferolateral trunk.
-
Anterior unnamed branches to the upper nasopharynx and adjacent tissues.
-
-
ii.
Territories
Supplies upper nasopharynx including the orifice of the Eustachian tube as well as associated muscles, including superior constrictor. Has many potential anastamoses, including accessory meningeal, pterygovaginal, and contralateral superior pharyngeal. If a Vidian branch is present, this is a potentially dangerous anastamosis during embolization procedures and it may also contribute to cavernous carotid fistulas via the petrous ICA.
-
iii.
Variants
Pharyngeal territories of the superior pharyngeal artery may be primarily supplied by the accessory meningeal artery, Vidian artery, and other nasopharyngeal feeders.
-
i.
-
(a)
-
2.
Territories
Ascending pharyngeal artery supplies the mucosa and adjacent muscles of the pharynx, soft palate, odontoid process, bones, and muscles and nerve roots at C1 and C2. It also supplies the lower cranial nerves (IX–XII and potentially VI and VII); lower clivus and medial skull base; meninges of the posterior fossa; portions of the middle cranial fossa; and the middle ear. The ascending pharyngeal artery has extensive anastamoses with its contralateral counterpart, the occipital, middle and accessory meningeal and distal internal maxillary arteries. Moreover, it has particularly dangerous anastamoses with the internal carotid and vertebral arteries.24 This is a very busy little artery.
-
3.
Variants
-
(a)
The ascending pharyngeal artery may arise from the ICA.
-
(b)
Often arises as a common trunk with the occipital artery.
-
(c)
Ascending cervical artery may supply the territory of the ascending pharyngeal artery.19
-
(d)
Can contribute to the persistent hypoglossal artery variant.
-
(e)
Can reconstitute an occluded or aplastic vertebral artery.
-
(f)
The so-called “aberrant ICA” in the middle ear cavity is probably more appropriately termed the ascending pharyngeal artery, providing a collateral pathway for the territory of a segmentally occluded ICA.17,18
-
(a)
3.2.1 Angio-Anatomic Correlate! Ascending Pharyngeal Artery Collaterals (Fig. 1.8)

Lateral view selective injections of the ascending pharyngeal artery in a patient with a dural arteriovenous fistula. Early arterial phase (a) starts to show faint anastamotic fi lling of the vertebral artery at the C1 level (arrow). Later arterial phase (b) shows considerable fi lling of the vertebral and basilar arteries (arrows)
Lateral view selective injections of the ascending pharyngeal artery in a patient with a dural arteriovenous fistula. Early arterial phase (a) starts to show faint anastamotic filling of the vertebral artery at the C1 level (arrow). Later arterial phase (b) shows considerable filling of the vertebral and basilar arteries (arrows).
3.3 Lingual Artery
Arises from the ventral aspect of the external carotid and takes a gentle anterior-inferior path creating a characteristic “U” shaped curve on both frontal and lateral angiographic projections. It then curves upward, as the dorsal lingual branch forms an arc through the tongue with an arcade of radiating branches.
-
1.
Branches
-
(a)
Suprahyoid artery
This small branch runs along the superior aspect of the hyoid bone and anastamoses with the contralateral suprahyoid artery.7
-
(b)
Dorsal lingual artery
May consist of two or three upwardly arching branches that curve up over the tongue – forming radiating branches that follow the pattern of the radiating intrinsic lingual muscle. The dorsal lingual artery anastamoses with its contralateral counterpart.7
-
(c)
Sublingual artery
This branch angles anteriorly to supply the sublingual gland and floor of the mouth. It anastamoses with the submental branch of the facial artery and with its contralateral counterpart. A small branch pierces the lingual foramen of the mandible and supplies the adjacent bone.7
-
(d)
Deep lingual artery
This is a small terminal branch to the frenulum of the tongue.7
-
(a)
-
2.
Territories
The lingual artery provides generous arterial supply to the tongue and floor of the mouth. There are anastamoses with the contralateral lingual and ipsilateral facial arteries via the submental branch. However, remember that branches extending to the tip of the tongue are effectively end arteries. Distal embolization with small particles or liquid agents can produce ischemic necrosis of the tip of the tongue, especially if the emboli are forced across the midline via the side-to-side anastamosis, or if bilateral embolization is intentionally done.
-
3.
Variants
-
(a)
The lingual artery often arises with the facial artery from a common facial-lingual trunk (20% of cases).13
-
(b)
Occasionally, can arise with the superior thyroid artery as a common thyrolingual trunk (2.5% of cases), or thyrolinguofacial trunk (2.5% of cases).13
-
(c)
It rarely arises from the CCA.
-
(d)
The lingual artery can supply variable amounts of the submental artery’s supply to the floor of the mouth.
-
(a)
3.4 Facial Artery
The facial artery is usually one of the larger ECA branches and arises from the anterior aspect of the ECA. It then curves in a slightly redundant fashion through the submandibular gland, under and around the angle of the mandible, and then angles forward and cephalad, as well as medially to extend up along the angle of the nose as the angular artery. The facial artery has a number of named and unnamed branches that anastamose freely from one to the other and with other vessels in the face (Fig. 1.9).

Facial artery. (1) Ascending palatine artery; (2) tonsillar artery; (3) submental artery; (4) inferior masseteric artery; (5) jugal trunk; (6) middle mental artery; (7) inferior labial artery; (8) anterior jugal artery (not shown); (9) superior labial artery; (10) lateral nasal artery; (11) angular artery
-
1)
Branches
-
a)
Ascending palatine artery
-
i)
This artery ascends for a few centimeters from its origin, and then takes a right angle forward to the soft palate by making a small loop-de-loop as it curves around the tonsils. Consequently, the ascending palatine artery can be a casualty of tonsillectomy or palatal surgery,26 and, along with the smaller tonsillar arteries, a source of post-op bleeding.
-
(1)
Branches
-
(a)
A cadaver study of palatine blood supply found three fairly constant and several less constant branches.27
-
(i)
Glossal branch. Arises at the level of the upper border of the tongue and supplies the palatoglossus muscle.
-
(ii)
Tonsillar branch. Arises at the level of the oropharyngeal tonsil and supplies the tonsil and palatopharyngeus muscle and sometimes the palatoglossal muscles.
-
(iii)
Hamular branch. Arises adjacent to the hamulus of the medial pterygoid plate and mucosa and palatoglossus muscle.
-
(iv)
Variable branches to uvula, levator palatini, palatoglossus, and palatopharyngeus muscles.
-
(i)
-
(a)
-
(1)
-
ii)
Territories
-
(1)
Supplies mucosa and muscles of the lateral oropharynx and soft palate. Anastamoses with contralateral ascending palatine artery, ipsilateral middle pharyngeal artery, the greater palatine artery, and the branches of accessory meningeal artery.
-
(1)
-
iii)
Variants
-
(1)
Usually arises from the proximal facial artery. May arise directly from the ECA, from a common trunk with the submandibular branch, occasionally from the middle pharyngeal artery (from the ascending pharyngeal artery) or even from the accessory meningeal artery.19
-
(1)
-
i)
-
b)
Tonsillar artery
-
i)
This artery is comprised of one or more small proximal facial branches to the tonsils. The tonsillar artery, along with the ascending palatine artery, pharyngeal branches of the ascending pharyngeal, dorsal lingual branch of the lingual, and greater palatine branch of the internal maxillary, provide the dominant supply to the palatine (oropharyngeal) tonsil.7 The tonsillar artery must, therefore, be considered a culprit in postoperative bleeding after tonsillectomy, along with the ascending palatine artery. The tonsillar branches of the facial artery can also contribute to the nasopharyngeal tonsils, but most of the blood supply to that tonsil comes from the superior pharyngeal artery, ascending palatine artery, pterygo-vaginal artery, and occasionally the inferior hypophyseal branch of the meningohypohyseal trunk.7
-
i)
-
c)
Submandibular branches
-
i)
A small branch or branches to the submandibular gland region may arise from the submental artery and anastamose to the lingual and superior thyroid branches.28
-
i)
-
d)
Submental artery
-
i)
This fairly large artery travels along the inferior margin of the mandible. It supplies the floor of the mouth in conjunction with the lingual artery. The submental artery anastamoses with the lingual artery via its submandibular branch and with the superior thyroid artery via its infrahyoid branch. It also has side-to-side anastamoses with its contralateral partner.28 Its terminal branches curve up to the chin to anastamose with the middle mental and inferior labial arteries.7
-
i)
-
e)
Inferior masseteric artery
-
i)
This anterior-superior angling branch follows and supplies the lower masseter muscle. It may have a small amount of collateral flow to the superior masseteric branch of the internal maxillary.28
-
i)
-
f)
Jugal trunk
-
i)
The name is derived from the Latin jugālis, and refers to the zygoma or cheek. The jugal trunk is one of the three main superior-to-inferior anastamoses in the soft tissues of the cheek.
-
(1)
Branches
-
(2)
Two angiographically visible branches arise from the jugal trunk:
-
(a)
Bucco-masseteric (aka buccal). Arises from the jugal trunk at the level of the ramus of the mandible, then heads in a cephalad direction and deeply into the cheek. It gives rise to a buccal branch that supplies the mucosa and deep parts of the cheek and a masseteric branch that feeds its namesake – the masseter. The buccal artery anastomoses with the distal internal maxillary artery via its buccal branch and the superior masseteric. The masseteric branch anastamoses with the transverse facial and infraorbital arteries. It characteristically crosses the transverse facial artery at a right angle on lateral angiographic views.28
-
(b)
Posterior jugal. This branch travels obliquely anterior-superiorly and anastamoses with the infraorbital branch of the internal maxillary, superior alveolar, and the transverse facial.28
-
(a)
-
(1)
-
i)
-
g)
Middle mental artery
-
i)
A small horizontal branch along the body of the mandible that supplies skin and adjacent subcutaneous tissues. It anastamoses to adjacent facial artery branches and the inferior alveolar branch of the internal maxillary artery.28
-
i)
-
h)
Inferior labial artery
-
i)
Middle jugal artery
-
i)
An inconstant branch that parallels and potentially anastamoses with the anterior and posterior jugal trunks.28
-
i)
-
j)
Superior labial artery
-
i)
Anterior and medially directed branch to the upper lip. It runs parallel to the inferior labial artery and is usually larger than that artery. It has septal and alar branches to the nose. It freely anastamoses with the contralateral superior labial artery and has potentially dangerous anastamoses with nasal branches of the ophthalmic artery.7,28
-
i)
-
k)
Anterior jugal artery
-
i)
The anterior-most of the upward angulated branches in the cheek, it supplies the anterior cheek and lateral aspect of the upper lip and nose. It freely anastamoses with the infraorbital, the posterior and middle jugal arteries, the transverse facial artery, and superior alveolar artery.28
-
i)
-
l)
Lateral nasal (aka alar) artery
-
i)
This small branch extends anteriorly to supply the nostril and anastamoses with the contralateral alar artery.7
-
i)
-
m)
Nasal arcade
-
i)
These arteries are a network of anastamotic channels curving over and across the nose. They collect and connect inputs bilaterally from the facial and ophthalmic arteries.28
-
i)
-
n)
Angular artery
-
i)
Travels up along the angle lateral to the nose, hence it’s name. It supplies the cheek beside the nose and the lateral aspect of the nose, contributing to the nasal arcade. It has dangerous anastamoses with inferior palpebral and nasal branches of the ophthalmic artery.28
-
i)
-
a)
-
2)
Territories
-
a)
The facial artery is the major supplier to the superficial soft tissues of the face and contributes to the masseter muscle, parotid gland, palate and tonsils, floor of the mouth, and portions of the buccal mucosa. It provides vasa nervora to distal facial artery branches in the face. There are numerous anastamoses between facial branches and to virtually every other artery in the facial region, including major connections to the internal maxillary artery, transverse facial artery, and important collaterals to distal ophthalmic artery branches.
-
a)
-
3)
Variants
-
4)
Lasjaunias proposed a theory of hemodynamic balance in the face to explain the variety of arterial configurations.19,28 At six regions in the face (termed jugal, infraorbital, and ophthalmic superiorly, and mandibular, labial and nasal inferiorly), dominance of blood flow to the region by one or the other potential inputs determines the course and size of the facial artery. For instance, there is balance between the buccal and masseteric arteries in the posterolateral aspect of the face and balance between the infraorbital and transverse facial arteries in the mid-portion. Numerous variations are possible.
-
a)
The facial artery frequently arises as a common trunk with the lingual (20% of cases).13
-
b)
The proximal facial artery may have a posterolateral “jugal” course through the jugal region.19
-
c)
The facial artery may also travel anteromedially through the labial point for a “labial course.”19
-
d)
The left and right facial arteries are symmetrical in 68% of autopsy cases.30
-
e)
The facial artery terminates in the:30
-
i)
Angular artery (68%)
-
ii)
Lateral nasal branch (26%)
-
iii)
Superior labial artery (4%)
-
i)
-
a)
3.5 Occipital Artery
The occipital artery is a large branch of the posterior aspect of the ECA and travels posteriorly and superiorly. The initial segment is straight as it goes up through the upper neck, and the artery becomes more tortuous and redundant as it travels up the posterior scalp (Fig. 1.10).

Occipital artery. (A) Sternocleidomastoid branches; (B) stylomastoid artery; (C) mastoid branch; (D) descending branch; (E) lateral meningeal branch; (F) occipital branches
-
1)
Branches
-
(a)
Sternocleidomastoid branches (aka muscular branches)
There may be multiple muscular branches. The hypoglossal nerve hooks around the lowest branch of this artery as the nerve first heads inferiorly and then anteriorly toward the tongue.7 Each muscular branch characteristically tends to curve cephalad for a short distance before taking an abrupt turn posteroinferiorly. Each muscular branch corresponds to a vertebral level and provides segmental supply to the muscles, nerves, and bone at the corresponding levels. The occipital artery shares segmental vertebral blood supply with the vertebral artery, ascending pharyngeal artery, and deep cervical artery, which all anastomose extensively with the occipital artery muscular branches. The muscular branches that usually come from the occipital artery may also arise from the posterior auricular artery or directly from the ECA.19
-
(b)
Stylomastoid artery
The stylomastoid artery arises from the occipital artery in 20–50% of cases.19,31 It is a common source of blood flow to the facial nerve and middle ear and it has anastamoses with the inferior tympanic, anterior tympanic, and superior tympanic arteries.
-
(c)
Mastoid artery
This vessel angles cephalad and medially from the occipital artery, giving some supply to the soft tissue in the adjacent scalp before entering the skull via the occipital foramen.
-
i.
Branches
After it enters the skull, the mastoid commonly divides into three groups of branches:19
-
Descending branches.
These approach the jugular foramen and anastamose with the jugular branch of the ascending pharyngeal.
-
Ascending branches.
These approach the internal auditory canal and can anastamose with the subarcuate branch of the anterior-inferior cerebellar artery.
-
Posteromedial branches.
These spread out into the lateral dura of the posterior fossa and anastomose with branches of the hypoglossal branch of the ascending pharyngeal artery or the posterior meningeal branch arising from the vertebral (or posterior-inferior cerebellar) artery.19
-
-
ii.
Territories
The mastoid artery supplies the superficial soft tissue, bone and dura in the mastoid and temporal bone region. It may supply large areas of the dura in the posterior fossa.
-
iii.
Variants
The mastoid artery may be absent or hypoplastic. Its territory may be supplied by middle meningeal artery, hypoglossal artery, jugular branches, or the meningeal branches of the vertebral artery.
-
i.
-
(d)
Descending branch
The most cephalad muscular branch at the occipital-C1 junction tends to be quite prominent, usually with large anastamotic connections to the vertebral artery and a descending branch connecting to the deep cervical artery.
-
(e)
Lateral meningeal branches
Distal to the origin of the mastoid branch, there may be one or more branches entering the skull via a small parietal foramen to supply the supratentorial dura. There are usually anastamoses with middle meningeal branches.
-
(f)
Occipital branches
Multiple scalp vessels, with a redundant zigzag configuration, arise from the occipital to supply the scalp, muscles, and pericranium. These anastamose with the contralateral occipital branches, the scalp branches of the posterior auricular, and the superficial temporal arteries.7
-
(a)
-
2)
Territories
The occipital artery travels 3 cm lateral to the inion. It generally supplies the posterior third of the scalp, the occipital-frontalis, trapezius, and sternocleidomastoid muscles, portions of the occipital, mastoid and temporal bones, dura, the seventh and ninth cranial nerves, and the first few spinal nerves. There are numerous anastamoses to the contralateral occipital artery, the ipsilateral ascending pharyngeal artery, vertebral artery, middle meningeal artery, superficial temporal artery, posterior auricular artery, deep cervical artery and even the anterior–inferior cerebellar artery.
-
3)
Variants
-
(a)
The ascending pharyngeal may arise from the occipital artery.
-
(b)
There can be a common origin of the occipital with the posterior auricular artery as an occipitoauricular trunk (12.5% of cases).13
-
(c)
The occipital artery may arise from the ICA.
-
(d)
The occipital artery can be a part of persistent carotid-vertebral anastamoses, such as a persistent proatlantal artery.
-
(e)
The occipital artery may originate from C1 or C2 segmental branches of the vertebral artery or from the ascending cervical artery.19,32
-
(a)
3.6 Posterior Auricular Artery
This posterior branch of the distal external carotid is fairly small and can be identified angiographically by the tortuous scalp branch curving cephalad behind the ear.
-
1)
Branches
-
(a)
Sternocleidomastoid (aka muscular) branch
Proximal branch of the posterior auricular can assist the occipital in providing blood flow to the sternocleidomastoid, digastric, and stylohyoid muscles.7
-
(b)
Parotid branches
Small branches from the proximal posterior auricular to the parotid that can supply portions of the facial nerve.
-
(c)
Stylomastoid branch
The stylomastoid artery arises from the posterior auricular in 50–70% of cases.31,33 In order of frequency; it may also arise from the occipital or directly from the external carotid. It feeds the facial nerve and middle ear, mastoid air cells and portions of the inner ear.7 It can anastamose with anterior tympanic artery (from middle meningeal) and inferior tympanic (from ascending pharyngeal) artery.
-
(d)
Auricular branch
A fairly constant branch seen in 65% of cases, this vessel supplies much of the posterior aspect of the pinna.34 Its branches from a dense arterial network in the ear.
-
(e)
Occipital (aka retroauricular) branch
Also a fairly constant branch and is seen in 65% of cases. It supplies the scalp behind the ear.
-
(f)
Parietal branch
A fairly inconstant branch seen only when the superficial temporal does not have a dominant parietal branch. It has the typical ascending, tortuous appearance of a scalp vessel.
-
(a)
-
2)
Territories
The posterior auricular artery supplies the auricle and enters the middle part of the ear posteriorly.35 It is the major supplier of blood flow to the ear.36 It can supply portions of the parotid gland, facial nerve, sternocleidomastoid, digastric and stylohyoid muscles.7 It has variable supply to the scalp posterior and superior to the ear, depending on the dominance of the superficial temporal and occipital arteries. It anastamoses with the superficial temporal and occipital arteries via the scalp and auricular branches. It also anastomoses with the middle meningeal artery (anterior tympanic branch) and ascending pharyngeal artery (inferior tympanic branch) via the stylomastoid artery.
-
3)
Variants
-
(a)
Shares a common origin with the occipital artery (occipitoauricular trunk) in 12.5% of cases.13
-
(b)
The scalp territories of the posterior auricular artery are in a hemodynamic balance with the superficial temporal and occipital arteries. If one is hypoplastic, the adjacent vessels are hypertrophic, and vice versa.
-
(a)
3.7 Superficial Temporal Artery
One of the two terminal branches of the external carotid (the other is the internal maxillary artery), this vessel continues the general vertical course of the ECA. The superficial temporal artery arises behind the neck of the mandible within the parotid gland. It is easily palpable anterior to the ear at the tragus.7 The superficial temporal artery typically provides two major branches that then angle cephalad in a wavy, redundant fashion typical of scalp vessels.
-
1)
Branches
-
(a)
Transverse facial artery
Originating anteriorly from the superficial temporal artery (within the parotid gland) the transverse facial artery travels anteriorly and slightly inferiorly between the parotid duct and zygomatic arch, supplying facial structures.7 On a lateral angiogram it crosses the buccal artery at a right angle.19 With agenesis or diminution of the facial artery, this branch may be the dominant artery of the face.
-
i.
Branches
The transverse facial artery commonly has a number of branches, but only one (superior masseteric) has a well-described formal name.
-
Parotid branches.
These supply the parotid gland and duct and may contribute to facial nerve branches.
-
Superior masseteric.
Prominent branch to the masseter muscle that anastamoses with the buccal artery (from the facial artery).19
-
Jugal branches.
One or more descending branches to the cheek that may anastamose with the jugal branches of the facial artery.
-
Zygomatic branches.
These spread out into the face and anastamose with branches of the zygomatico-orbital branch of the superficial temporal artery.19 Distally, these terminal branches may anastamose with the infraorbital and lacrimal arteries.7
-
-
ii.
Territories
The transverse facial artery supplies the superficial soft tissues of the upper face. It anastamoses with other superficial temporal and facial branches, as well as collaterals to the infraorbital and ophthalmic arteries.
-
iii.
Variants
The transverse facial artery may arise directly from the ECA.
-
i.
-
(b)
Anterior auricular artery
It is a proximal branch of the superficial temporal, supplying blood primarily to the anterior aspect of the ear. It has three branches, the most superior of which curves up over the helix to anastamose with posterior auricular artery. The lower two branches only provide limited supply to the anterior ear.35
-
(c)
Zygomatico-orbital artery (aka zygomaticotemporal)
This variably prominent, anteriorly directed branch of the superficial temporal artery runs just superior to the zygomatic arch toward the lateral aspect of the orbit. It supplies the scalp and the orbicularis occuli muscles.7 It has numerous anastamoses with the frontal branch of the superficial temporal artery, transverse facial artery, and the supraorbital, frontal, palpebral, and lacrimal branches of the ophthalmic artery.19
-
(d)
Middle temporal artery
Also called the posterior deep temporal by some authors, this is a relatively small branch supplying the temporalis muscle, specifically its posterior aspect.37 It potentially anastamoses with the deep temporal branches of the internal maxillary.7
-
(e)
Frontal branch
One of the two large terminal branches of the superficial temporal takes a tortuous course over the frontal scalp and supplies tissue from skin down to pericranium. It anastamoses with its contralateral counterpart across the midline, the ipsilateral zygomatico-orbital branch of the superficial temporal, and the supraorbital and supratrochlear branches of the ophthalmic artery.7 The distal frontal branch over the vertex can also provide branches that pass through foramina for emissary veins to anastamose with middle meningeal branches.19 This is why superficial temporal arteries sometimes supply intracranial lesions such as meningiomas.
-
(f)
Parietal branch
The other, usually larger terminal branch of the superficial temporal, angles more posteriorly to supply the parietal scalp. It anastamoses with the contralateral parietal branch, ipsilateral frontal branch, posterior auricular, and occipital branches. It can also provide some transcranial anastamoses with the middle meningeal branches.
-
(a)
-
2)
Territories
The superficial temporal is a major contributor of blood flow to the scalp and is in a hemodynamic equilibrium with the occipital and posterior auricular arteries. There are extensive anastamoses between the superficial temporal branches and branches of the occipital, posterior auricular, middle meningeal, ophthalmic and facial arteries.
-
3)
Variants
The major superficial branches vary considerably in size and territory. Hemodynamic balance exists between individual superficial temporal artery branches and competing scalp arteries. Therefore, when one artery is large and covers a wide territory, adjacent arteries may be small or absent.
3.8 Internal Maxillary Artery
The internal maxillary artery (IMA) is the larger of the two terminal branches of the ECA. Inclusion of the term internal may seem superfluous, although in earlier days, the facial artery was referred to as the external maxillary artery. The IMA arises at a right angle from the external carotid behind the neck of the mandible and travels anteriorly.7 Anatomically, it can be divided into three segments: (1) the proximal mandibular part that travels horizontally, first posterior and then medial to the mandible; (2) the middle pterygoid part that travels anteriorly and cephalad (in a slightly oblique fashion) adjacent to the lateral pterygoid muscle (medial or lateral to it depending on whether it is the superficial or deep variant as described below); (3) the distal pterygopalatine part that passes between the upper and lower heads of the lateral pterygoid, curves medially, and travels through the pterygomaxillary fissure into the pterygopalatine fossa.7
The IMA is found in two configurations:
-
1)
The superficial-type IMA travels lateral to the lateral pterygoid. In this variant, the accessory meningeal artery arises from the middle meningeal artery. The inferior alveolar and the middle deep temporal arteries arise separately from the IMA (Fig. 1.11).38,39
Fig. 1.11 
Internal maxillary artery, superficial-type variant. The internal maxillary artery (IMA) travels lateral to the lateral pterygoid muscle, and is characterized by separate origins of the middle deep temporal (MDT) and inferior alveolar artery (IAA). The accessory meningeal (AMA) arises from the proximal middle meningeal (MMA). Other IMA branches include deep auricular (DA), anterior tympanic (AT), posterior deep temporal (PDT), pterygoid branches (not shown), masseteric branches (MaB), buccal artery (BuA), anterior deep temporal (ADT), posterior superior alveolar (PSA), infraorbital (IOA), greater palatine (GPA), pterygo-vaginal (PVA), artery of foramen rotundum (AFR), sphenopalatine (Sph)
-
2)
The deep-type IMA travels medial to the lateral pterygoid. It gives rise to a common origin of the inferior alveolar and middle deep temporal arteries. The accessory meningeal artery, in this variant, arised directly from IMA.38,39 Hint: Remember that the Deep-type IMA has a common origin of the inferior alveolar and middle deep temporal arteries (Fig. 1.12).
Fig. 1.12 
Internal maxillary artery, deep-type variant. The deep type internal maxillary (IMA) is medial to the lateral pterygoid muscle. This variant has a common trunk (arrow) that gives rise to the middle deep temporal (MDT) and inferior alveolar artery (IAA). Also note separate origins of the accessory meningeal (AMA) and middle meningeal artery (MMA). Superficial temporal origin (STA) and distal external carotid (ECA) are also shown


-
1)
Branches
The mandibular part of the IMA gives rise to the deep auricular, anterior tympanic, middle meningeal, accessory meningeal, and inferior alveolar arteries (i.e., branches that traverse foramina or fissures). The pterygoid part usually has deep temporal, pterygoid, masseteric, and buccal branches (i.e., muscular branches). The pterygopalatine part provides the posterior superior alveolar, infraorbital, artery of foramen rotundum, pterygovaginal, descending palatine, Vidian, and sphenopalatine arteries.7
-
a)
Deep auricular artery
-
i)
Tiny branch of very proximal internal maxillary
-
ii)
Branches
-
(1)
No named branches.
-
(1)
-
iii)
Territories
-
(1)
Supplies external auditory meatus, tympanic membrane, and temporomandibular joint.7
-
(1)
-
iv)
Variants
-
v)
May arise in a common trunk with the anterior tympanic artery
-
i)
-
b)
Anterior tympanic artery
-
i)
Very small branch of very proximal internal maxillary
-
ii)
Branches
-
(1)
No named branches.
-
(1)
-
iii)
Territories
-
(1)
Supplies tympanic cavity and anastamoses with the stylomastoid artery, pterygovaginal branch of the IMA, and caroticotympanic artery from petrous ICA.7
-
(1)
-
iv)
Variants
-
(1)
Analysis of 104 cadaveric specimens revealed extremely variable anterior tympanic artery origins.40
-
(2)
May arise as a common trunk with deep auricular artery, middle meningeal artery, accessory meningeal artery, or posterior deep temporal artery.
-
(3)
The anterior tympanic artery is a branch of the right IMA in 78% of cases and a branch of the left IMA in 45% of cases.
-
(4)
Next most common site of origin: superficial temporal artery.
-
(5)
1–4% arise directly from the ECA.
-
(6)
Rarely, the anterior tympanic artery may be duplicated, triplicated, or absent.40
-
(1)
-
i)
-
c)
Middle meningeal artery (Fig. 1.13)
Fig. 1.13 
Middle meningeal artery: branches and anastamoses. The middle meningeal artery (MMA) often has a large extracranial branch, the accessory meningeal artery (AMA), which, in turn has anastamoses with the greater palatine (Gr. Palatine) and ascending palatine (Asc. Palatine) arteries before entering the skull via the foramen ovale and anastamosing with cavernous branches of the internal carotid (ICA). The middle meningeal artery continues into the skull via the foramen spinosum. The petrous branch (Petrous Br.) is the first intracranial branch and anastamoses with ascending pharyngeal branches in the temporal bone and with ICA branches via its cavernous branch (CB). Petrosquamosal (PSB), temporal, parietal, and frontal branches supply the dura over the middle and anterior fossa. Transcranial anastamoses with the superficial temporal (STA) and midline anastamoses with the anterior falx (AFA) branch of the ophthalmic (Ophth.) are depicted. The sphenoidal branch (Sph. Br.) is a major collateral to the ophthalmic
-
i)
The first substantial ascending branch of the internal maxillary enters the cranial cavity through foramen spinosum. It then takes a characteristic right-angle turn. In the sagittal plane, it turns anteriorly and in the coronal plane it turns laterally.
-
ii)
Branches
-
(1)
Accessory meningeal branch
-
(a)
This may be a major extracranial branch of the middle meningeal or may arise separately from the internal maxillary. The accessory meningeal is discussed in detail below.
-
(a)
-
(2)
Petrous branch
-
(a)
The small but important petrous branch first gives a medial cavernous branch to the cavernous sinus that can anastamose with the posterior branch of the inferolateral trunk. It then gives a posterior basal tentorial branch, which anastamoses with basal tentorial branches of the petrosquamosal branch of the middle meningeal artery and cavernous branches of the ICA.19 The artery then follows along the greater petrosal nerve and sends the superior tympanic branch to the facial nerve and geniculate ganglion. This portion of the artery anastamoses with the stylomastoid artery.7
-
(a)
-
(3)
Petrosquamosal branch
-
(a)
A posteriorly directed branch of the proximal intracranial middle meningeal artery, the petrosquamosal branch supplies the middle cranial fossa dura. It can have a basal tentorial branch to the dura of the posterior fossa, and it anastamoses with the jugular branch of the ascending pharyngeal.19
-
(a)
-
(4)
Sphenoidal branch
-
(5)
Meningolacrimal branch
-
(6)
Temporo-occipital (aka temporal) branch
-
(a)
This branch arises distal to the sphenoidal branch and curves posteriorly. It supplies skull and dura of the middle cranial fossa. It may extend completely around the calvaria to the midline and contribute to the posterior falx and tentorium, but this is generally seen only in pathological states. It anastamoses with the petrosquamosal and parietal branches of the middle meningeal artery and with scalp arteries via transcranial collaterals.
-
(a)
-
(7)
Parietal branch
-
(a)
One of the two terminal branches of the middle meningeal artery, this vessel supplies the anterior cranial fossa dura. It can vary in size and distribution, since it anastomoses with and is in a hemodynamic balance with the frontal and temporo-occipital branches. The parietal branch reaches the vertex and contributes to the walls of the superior sagittal sinus and falx. At the midline, it anastamoses with the contralateral middle meningeal artery. Transcranial anastamoses with scalp arteries (superficial temporal and occipital) are present in nearly all cadaveric specimens.43
-
(a)
-
(8)
Frontal branch
-
(a)
Usually the last branch of the middle meningeal artery, this branch is in hemodynamic balance with the parietal branch; therefore, it can vary in size and distribution. It is a major contributor to the anterior cranial fossa dura. It can reach the midline and frequently anastamoses with the anterior falx branch of the ophthalmic artery. Other anastamoses include the ipsilateral parietal branch, the contralateral frontal branch, and transcranial collaterals of the scalp arteries, especially the frontal branch of the superficial temporal artery.
-
(a)
-
(1)
-
iii)
Territories
-
(1)
The middle meningeal artery provides extensive flow to the calvaria and meninges of the anterior and middle fossae (Table 1.5). It has important collaterals to the ICA circulation.44 The middle meningeal artery also contributes to the cranial nerves in the cavernous sinus via the cavernous branch and also to the facial nerve via the superior tympanic branch.
Table 1.5 Intracranial dural vascular supply
-
(1)
-
iv)
Variants
-
(1)
The middle meningeal artery develops from the fetal stapedial artery. The stapedial artery arises from the fetal hyoid artery, a branch that becomes the petrous ICA, and passes through the mesenchyma that later becomes the stapes (hence the name). The stapedial artery gives off supraorbital, maxillary, and mandibular branches, which are later incorporated into the ECA. The supraorbital artery anastamoses with the developing ophthalmic artery.7 Persistence of portions of fetal arteries that usually regress and/or regression of segments that usually persist, results in a number of congenital variants.45
-
(2)
The distal middle meningeal artery frequently arises from the ophthalmic artery.46
- (3)
-
(4)
The ophthalmic artery may arise from the middle meningeal artery.49–52
-
(5)
A number of extracranial branches may arise from the middle meningeal artery, including a palatine branch,53 as well as the posterior superior alveolar artery.54
-
(6)
Tentorial branches (usually arising from cavernous ICA) may arise from the middle meningeal artery.55
-
(7)
Occasionally, the middle meningeal artery may arise from the basilar artery.56–58
-
(8)
The size and direction of the distal middle meningeal branches is extremely variable.
-
(9)
Dural-to-pial collateral flow from middle meningeal artery branches to anterior or middle cerebral branches can occur. However, these variants are usually seen in the presence of occlusive disease (such as carotid occlusion with impaired collateral flow)59 or with high-flow lesions (such as brain arteriovenous malformations). These are likely acquired connections due to high flow demand and release of angiogenic factors, rather than true congenital variants.
-
(1)
-
i)
-
d)
Accessory meningeal artery
-
i)
This small branch arising either from the proximal middle meningeal or, less commonly, from the IMA just distal to the middle meningeal artery takes a characteristic gently curving antero-superior course. Ironically, in spite of its name, only about 10% (range 0–40%) of its blood supply is intracranial.60
-
ii)
Branches
-
(1)
Terminal branches of the accessory meningeal vary in size and configuration and are variably named in the literature.61 The major branches, ascending, descending, and recurrent rami, are named for the direction they take after arising from the accessory meningeal artery.60
-
(2)
Lateral territory ascending ramus (aka posterior branch)
-
(3)
Medial territory ascending ramus (aka inferomedial branch)
-
(4)
Intracranial ascending ramus (aka intracranial branch)
-
(5)
Small branch usually enters the skull via foramen ovale
-
(6)
Descending companion ramus to the medial pterygoid nerve (aka arteria pterygoida medialis)
-
(7)
Anterior descending ramus (aka inferopalatine branch). This is the continuation of the main accessory meningeal artery and supplies the soft palate and the nasal cavity.
-
(8)
Variable recurrent rami to mandibular nerve and otic ganglion
-
(1)
-
iii)
Territories
-
(1)
There are lateral, medial, and intracranial territories. Most of the blood supply is extracranial supplying lateral and medial pterygoid, the levator veli palatine muscles, the pteryoid plates, the greater wing of the sphenoid bone, the mandibular nerve, and otic ganglion. The artery also supplies the posterior nasal cavity and can be a source of nasal bleeding.62 The intracranial contribution is usually small and enters the skull through foramen ovale (most commonly) or the sphenoidal emissary foramen of Vesalius (in 22% of cases).60 The intracranial rami supply the meninges of variable portions of the middle cranial fossa, portions of the cavernous sinus and the trigeminal nerve and its ganglion. It can anastamose with the posterior limb of the inferolateral trunk of the cavernous ICA.63
-
(1)
-
iv)
Variants
-
(1)
The origin of the accessory meningeal artery is from the middle meningeal artery when the internal maxillary artery is lateral to the lateral pterygoid muscle (superficial type IMA).
-
(2)
The origin is from the internal maxillary artery when IMA is medial to the lateral pterygoid (deep type IMA).
-
(3)
There can be multiple accessory meningeal arteries (25% of cases), but the artery is rarely absent (4% of cases).60
-
(4)
The rare persistent trigeminal variant consists of an anastamosis from the accessory meningeal artery to the superior cerebellar artery.64
-
(1)
-
i)
-
e)
Inferior alveolar artery (aka dental artery)
-
i)
This branch takes an anterior-inferior angulation from its origin from the proximal internal maxillary artery. It then enters the mandibular foramen, following along the mandibular canal.
-
ii)
Branches
-
(1)
Mylohyoid branch. This is a small branch to the mylohoid muscle arising from the inferior alveolar artery before entering the mandibular canal. It anastamoses with the submental branch of the facial artery.7
-
(2)
Incisive branch. One of two terminal branches of the inferior alveolar. Under the incisor teeth, the incisive branch reaches the midline, anastomosing with the contralateral incisive branch.7
-
(3)
Mental branch. This branch travels out through the mental foramen of the mandible to anastamose with the submental and inferior labial branches of the facial artery.7
-
(1)
-
iii)
Territories
-
(1)
The inferior alveolar supplies the mylohyoid muscle, the mandible, mandibular teeth, inferior alveolar nerve, and the soft tissues of the chin.
-
(1)
-
iv)
Variants
-
(1)
The inferior alveolar artery arises as a common trunk with the middle deep temporal artery in the deep type internal maxillary artery variant.
-
(2)
The inferior alveolar artery may arise directly from the ECA.65
-
(1)
-
i)
-
f)
Middle deep temporal artery
-
i)
Complicating things further, some authors refer to this branch as the posterior deep temporal artery, but most authorities refer to it as the middle deep temporal artery. The deep temporal arteries ascend in a relatively straight course unlike the redundant superficial temporal branches. The middle deep temporal artery provides approximately one-half of the blood flow to the temporalis muscle.37 It anastamoses with the superficial temporal artery and occasionally the transcranial collaterals from this vessel can anastamose with the middle meningeal artery branches. A component of the deep-type internal maxillary variant is a common origin of the inferior and middle deep temporal arteries.38,39
-
i)
-
g)
Pterygoid branches
-
i)
Small inferiorly directed branches of the distal pterygoid part to the pterygoid muscles that are not often visualized angiographically.
-
i)
-
h)
Masseteric artery
-
i)
Small, inferiorly directed branch to the masseter that anastamoses with masseteric branches of the facial and the transverse facial arteries.
-
i)
-
i)
Buccal artery
-
i)
Inferiorly directed branch that connects to the jugal trunk of the facial artery and supplies the soft tissues of the cheek from mucosa to skin. It provides collateral flow between the distal internal maxillary and facial arteries and has a connection to the transverse facial artery.
-
i)
-
j)
Anterior deep temporal artery
-
i)
This artery angles cephalad in a fairly straight course to provide approximately 30% of the blood supply to the temporalis muscle.37 This artery has important anastamoses to the lacrimal branch of the ophthalmic artery.
-
i)
-
k)
Posterior superior alveolar artery
-
i)
This artery descends behind the maxilla before sending branches to bone, teeth, and gingiva in the posterior aspect of the maxilla.
-
i)
-
l)
Infraorbital artery
-
i)
Anterior-most branch of the IMA that passes through the inferior orbital fissure, then enters the infraorbital canal to outline the roof of the maxillary sinus.7
-
ii)
Branches
-
(1)
Middle superior alveolar branch. Contributes to the alveolar process of the mandible.
-
(2)
Anterior superior alveolar branch. Also contributes to the supply of the maxillary teeth.
-
(3)
Orbital branch. This artery primarily supplies the adipose tissue in the inferior aspect of the orbit and can anastamose with the ophthalmic artery.66
-
(4)
Palpebral branch. Distal branch to the lower eyelid. It anastamoses with the dorsal nasal branch of the ophthalmic artery.
-
(5)
Naso-orbital branch. Small branches to the anterior-inferior orbit and side of the nose that anastamose with the ophthalmic artery.
-
(6)
Zygomatic branches. Lateral branch (or branches) supplying the cheek and connecting to the transverse facial artery and jugal trunk of the facial artery.
-
(1)
-
iii)
Territories
-
(1)
The infraorbital artery supplies the adjacent infraorbital (maxillary) nerve, mucosa, and bony margin of the maxillary sinus.67 Distal branches contribute to the lower eyelid and pre-maxillary cheek soft tissue.7 Both the orbital branch and the distal infraorbital branch (palpebral branch) anastamose with the ophthalmic artery, putting vision at risk when anything toxic is injected in the infraorbital artery.68 The infraorbital artery connects to the posterior superior alveolar, sphenopalatine, and facial arteries.
-
(1)
-
iv)
Variants
-
(1)
May be hypoplastic or hypertrophic, depending on the size of the facial artery.
-
(2)
Can arise in a common trunk with the posterior superior alveolar artery.
-
(1)
-
i)
-
m)
Pterygovaginal artery
-
i)
This is a small branch running posteriorly from the IMA into the pterygoid canal. It anastamoses with the accessory meningeal artery and ascending pharyngeal artery branches to the Eustachian tube region, and may connect with the petrous ICA.
-
i)
-
n)
Vidian artery (aka artery of the pterygoid canal)69,70
-
i)
This artery may arise from the pterygovaginal artery, or separately from the IMA. It enters the Vidian canal and may anastamose with a Vidian branch of the petrous ICA.
-
i)
-
o)
Artery of foramen rotundum
-
i)
Small, posteriorly directed branch with a characteristic wavy appearance as it passes through the foramen rotundum. Supplies the maxillary nerve and adjacent skull base. It is an important collateral to the anterolateral branch of the inferolateral trunk of the cavernous ICA.
-
i)
-
p)
Descending palatine artery
-
i)
This large artery descends obliquely from its origin, travels in the pterygopalatine (aka greater palatine) canal, turns abruptly forward horizontally and travels medial to the maxillary teeth to supply the palate. When it emerges from the greater palatine foramen, it then becomes the Greater palatine artery.
-
ii)
Branches
-
(1)
Lesser palatine artery. Smaller branch or branches running parallel to the greater palatine artery in a separate bony canal, usually without a distal horizontal segment. May arise independently from the IMA.27
-
(2)
Palatine branch. It is a small branch turning posteriorly to supply the soft palate and anastamoses with the middle pharyngeal and/or the ascending palatine.
-
(3)
Septal branch. It is the terminal branch of the greater palatine at the incisive canal. It supplies the nasal septum and anastamoses with sphenopalatine and ethmoidal arteries.
-
(1)
-
iii)
Territories
-
(1)
A major contributor to the blood supply of the hard palate, it also contributes to the mucosa, gingiva, soft palate, and tonsils.7 Anastamotic connections exist with the contralateral greater palatine artery, ipsilateral middle pharyngeal artery, ascending palatine artery, sphenopalatine artery, and ethmoidal branches of the ophthalmic.19
-
(1)
-
iv)
Variants
-
(1)
The greater palatine artery may be hypoplastic or absent on one or both sides.
-
(2)
Bilateral hypolasia of the greater palatine artery is seen in cleft palate syndrome.71
-
(1)
-
i)
-
q)
Sphenopalatine artery
-
i)
This is a major branch of the terminal IMA that enters the sphenopalatine foramen to supply the nasal cavity. This artery can be a major source of bleeding in epistaxis cases. The sphenopalatine artery can also supply vascular lesions in the nasal cavity such as juvenile nasopharyngeal angiofibromas.
-
ii)
Branches
-
(1)
Septal branch
-
(2)
This is a small branch that first goes straight medially, takes a right angle cephalad and another right angle medially before spreading out into the nasal septum. It also supplies the superior turbinate in 72% of cases.72
-
(3)
Lateral nasal branch (aka posterior lateral nasal branch).
-
(4)
This branch travels inferiorly before ramifying along the nasal turbinates to supply the nasal cavity mucosa.
-
(1)
-
iii)
Territories
-
(1)
Sphenopalatine arteries supply the mucosa of nasal cavity and are a very common source of bleeding in idiopathic epistaxis. They anastamose with ethmoidal branches of the ophthalmic artery, the greater palatine artery, and the septal branch of the superior labial artery.7
-
(1)
-
iv)
Variants
-
(1)
None described.
-
(1)
-
i)
-
a)
-
2)
Territories (IMA)
-
(a)
The IMA supplies bones in the mid and lower face, muscles of mastication mucosa in the nasal cavity, the palate, numerous cranial nerves (III–VII) and large areas of dura.7 There are multiple potential anastamoses with the internal carotid directly, the ophthalmic and numerous other vessels in the face and head.
-
(a)
-
3)
Variants (IMA)
-
(a)
Superficial-type versus deep-type IMA (see beginning of IMA section, above).
-
(b)
Rarely, the IMA shares a common origin with the facial artery.73
-
(a)

3.9 Other ECA Branches
Variable unnamed branches of the ECA are present. They are usually small and not well seen on angiography unless they are involved with a vascular malformation or neoplasm. The named branches that occasionally arise from the ECA usually arise from one of its major branches:
-
(a)
Tiny carotid body branches arise from the proximal ECA itself or from the proximal branches of the ECA.
-
(b)
The sternocleidomastoid branch (or branches) can arise from the ECA, but usually arises from the superior thyroid, occipital, or posterior auricular artery.
-
(c)
The superior laryngeal artery usually originates from the superior thyroid artery, but can arise separately from the ECA.
-
(d)
A recurrent pharyngeal branch to the upper oropharynx and palate can arise directly from the ECA.27
-
(e)
A small branch to the stylomastoid muscle arises from the distal ECA.
-
(f)
A small masseteric branch originates from the distal ECA.
-
(g)
The ascending palatine artery usually arises from the facial artery, but may originate directly from the proximal ECA.
-
(h)
The transverse facial artery frequently arises separately from the distal ECA, although it is more often a branch of the superficial temporal artery.
4 Internal Carotid Artery
Several classification schemes exist for the segments of the ICA, including various numbering systems (Fig. 1.14). The numbering systems can be confusing and needlessly arcane for the purposes of everyday clinical work. The authors of this handbook favor the following simple system (corresponding to the description by Gibo and colleagues):74

-
1.
Cervical
-
2.
Petrous
-
3.
Cavernous
-
4.
Supraclinoid
The segmental nomenclature used by Bouthillier and coworkers will be used in this chapter for the purpose of anatomic description.75
The system established by Fischer in 1938 was intended to describe angiographic patterns of arterial displacement by intracranial tumors, numbered the ICA segments against the flow of blood, and excluded the extracranial ICA.76 Subsequent systems have included the cervical segment and have numbered the segments with the flow of blood.

4.2 Cervical Segment (C1)
This segment begins at the carotid bifurcation and ends at the skull base and usually has no branches. The carotid bifurcation is usually at the level of C3. The ICA receives approximately 80% of the flow from the CCA. The ICA is encircled by sympathetic fibers, and travels in the carotid sheath, which also contains the internal jugular vein and the vagus nerve. The uppermost portion of the carotid sheath (superior to the nasopharynx) also contains cranial nerves IX, XI, and XII.
-
1)
Divisions
-
(a)
Carotid bulb. Focal dilation of the ICA at the origin, measuring 7.4 mm in diameter on average, compared to 7.0 mm for the CCA and 4.7 mm for the ICA distal to the carotid bulb.77
-
(b)
Ascending cervical segment. The diameter remains relatively constant throughout its course. Coiling or complete looping of the vessel is seen in up to 15% of angiograms.1
-
(a)
-
2)
Branches: None.
-
3)
Variants
-
(a)
Position of origin. The carotid bifurcation can be found as low as T2 or as high as C1.1 Rarely, the ICA may arise directly from the aortic arch; in these cases the non-bifurcating carotid artery gives rise to all of the branches normally supplied by the ECA and then continues as the ICA.78
-
(b)
Agenesis and hypoplasia
-
i.
Congenital absence or hypoplasia of the ICA may occur sporadically in a association with other congenital anomalies, such as anencephaly or basal telangectasia.79 Intracranial aneurysms are associated in 67% of cases.80
-
ii.
Agenesis of the ICA has a prevalence of 0.01%81 and can be distinguished from ICA occlusion by imaging of the skull base; in patients with agenesis, the carotid canal is absent.82 Agenesis is more frequent on the left.83
-
iii.
Bilateral ICA agenesis is seen in <10% of ICA agenesis cases83 and is associated with intracranial aneurysms in some 25% of cases.84
-
iv.
ICA Hypoplasia has an incidence of 0.079%,83 and should not be confused with diffuse narrowing of the ICA, which is most commonly seen with fibromuscular dysplasia, dissection, or secondary to high-grade atherosclerotic stenosis. Congenital hypoplasia can be distinguished from acquired stenosis by the presence of a small petrous carotid canal.82
-
i.
-
(c)
Anomalous branches are rare but can include:85
-
i.
Ascending pharyngeal artery
-
ii.
Superior thyroid artery
-
iii.
Occipital artery
-
iv.
Posterior meningeal artery
-
v.
Persistent stapedial artery
-
vi.
Vidian artery
-
i.
-
(d)
Duplication and fenestration of the cervical ICA has been reported.86,87
-
(e)
Carotid-vertebrobasilar anastamoses.
-
(a)
4.3 Carotid–Vertebrobasilar Anastomoses
Transient connections appear during development between the carotid and hindbrain circulations. These anastomoses usually disappear as the posterior communicating arteries develop and rarely persist into adulthood. The most common of these is the persistent fetal origin of the posterior cerebral artery, which has a prevalence of some 18–22% in the general population (see below).88 Three of the four other embryonic arteries are named for the cranial nerves they parallel. From superior to inferior, these persistent fetal vessels (excepting the fetal PCA) include: trigeminal, otic, hypoglossal, and proatlantal intersegmental arteries (Fig. 1.16). A mnemonic for this uses the acronym TO(h)P: The primitive anastomotic vessels appear near the TO(h)P of the craniospinal axis.

Carotid–vertebrobasilar anastomoses. The most common configuration of each type of persistent embryologic connection between the carotid and vertebrobasilar system are shown. The persistent fetal origin of the PCA is illustrated in Fig. 1.20. (a) Persistent trigeminal artery; (b) persistent otic artery; (c) persistent hypoglossal artery; (d) Proatlantal intersegmental artery, Type I (solid) and Type II (dashed)
-
1.
Persistent trigeminal artery
-
(a)
Most common carotid-basilar anastomosis, seen in some 0.1–0.2% of angiograms.33,85
-
(b)
Extends from the cavernous ICA to the upper part of the basilar artery and often perforates the dorsum sella.
-
i.
The vertebrobasilar system proximal to the upper basilar artery may be hypoplastic, with the primitive trigeminal artery supplying most of the flow to the PCAs and the SCAs.
-
i.
-
(c)
Two main variants.89 The relative prevalence of the two types is almost equal.90
-
i.
Saltzman Type I. The persistent trigeminal artery supplies the PCA and SCA territories. The posterior communicating arteries and the basilar artery proximal to the anastomosis are hypoplastic.
-
ii.
Salzman Type II. The PCAs are supplied by the posterior communicating arteries and the persistent trigeminal artery joins the basilar artery at the level of the SCAs.
-
i.
-
(d)
A less common trigeminal artery variant consists of the superior cerebellar artery arising from the internal carotid.91
-
(e)
Associated with intracranial aneurysms.
-
(f)
May have an intrasellar component and should not be mistaken for a pituitary mass.92
-
(a)
-
2.
Persistent otic artery
-
3.
Persistent hypoglossal artery
-
(a)
Second most common carotid-basilar anastomosis, seen in 0.03–0.26% of angiograms.96
-
(b)
Extends from the cervical ICA to the basilar artery via the hypoglossal canal.
-
i.
Arises from the ICA between the carotid bifurcation and C1.
-
ii.
The posterior communicating arteries may be absent.97
-
iii.
The ipsilateral vertebral artery is usually hypoplastic.
-
i.
-
(c)
May be associated with an aneurysm.98
-
(a)
-
4.
Proatlantal intersegmental artery
-
(a)
Extends from the cervical ICA or ECA to the vertebrobasilar system via the foramen magnum. Extremely rare.
-
(b)
Associated with aplasia or hypoplasia of the vertebral arteries in 50% of cases.99
-
(c)
Type I
-
i.
Arises from the ICA at C2-3, courses horizontally above the atlas, and gives rise to the ipsilateral vertebral artery.
-
ii.
More common than Type II.
-
i.
-
(d)
Type II
-
i.
Arises from ICA and joins the vertebral artery at C1.
-
ii.
May have a common origin with the occipital artery.100
-
i.
-
(a)
4.4 Petrous Segment (C2)
The petrous segment extends from the opening of the carotid canal in the skull base to the posterior edge of the foramen lacerum. The vertical subsegment transitions into the horizontal subsegment via the genu of the petrous ICA, which is a 90° bend in the vessel. At the entrance into the carotid canal, the carotid sheath splits into two layers; the inner layer continues as the periosteum of the carotid canal, and the outer layer is continuous with the periosteum of the inferior surface of the skull base. Post-ganglionic sympathetic fibers (internal carotid nerve) continue to travel with the ICA. A venous plexus (internal carotid artery plexus of Rektorzik) also surrounds the petrous ICA;101 the existence of this venous plexus has been proposed to effectively dampen the pulsation of the carotid, making it less perceptible by the adjacent hearing apparatus.102 In fact, anatomic specimens have shown that the venous plexus seems to be most prominent on the side of the vessel facing the cochlea, a finding that lends support to the theory (Fig. 1.17).

Relationship between the pericarotid venous plexus and the cochlea. Drawing of a histological section through the temporal bone showing that the pericarotid venous plexus (VP) is most developed on the side of the ICA facing the cochlea (C) IAC, internal auditory canal
-
1)
Subsegments
-
(a)
Vertical
-
i.
Average length is 10.5 mm.103
-
i.
-
(b)
Horizontal
-
i.
Approximately twice the length of the vertical subsegment; average length is 20.5 mm.103
-
ii.
A 1-cm length of this segment may be exposed in the floor of the middle fossa lateral to the trigeminal nerve, and covered by dura only or a thin layer of cartilage.
-
i.
-
(a)
-
2)
Branches
-
(a)
Normal petrous ICA branches are visible on angiography in only 23% of cases.104 In a cadaver dissection series, the petrous ICA was found to have branches in only 38% of the specimens (a Vidian branch in was found in 30%, and a periosteal branch was present in 8%); the “caroticotympanic artery,” was not found in single case.103
-
(b)
Periosteal branch
-
i.
Arises at the entrance of the ICA into the carotid canal. Found in 8% of the dissections.103
-
i.
-
(c)
Caroticotympanic artery
-
i.
Commonly described branch of the petrous ICA, although its existence has been disputed by some authors.103
-
ii.
Arises from the petrous ICA near the genu and travels superiorly and posteriorly to the middle ear cavity.
-
iii.
Anastomoses with the ascending pharyngeal artery via the inferior tympanic artery.104
-
i.
-
(d)
Vidian artery (aka artery of the pterygoid canal)
-
i.
Small branch that may arise from the horizontal petrous ICA and travels anteriorly within the Vidian (pterygoid) canal to the pterygo-palatine fossa. The Vidian canal is in the floor of the sphenoid sinus and also contains the Vidian nerve.
-
The Vidian nerve is formed by the combination of the deep petrosal nerve (containing sympathetic fibers from the plexus surrounding the ICA) and the greater superficial petrosal nerve (containing parasympathetic and sensory fibers).
-
-
ii.
The Vidian artery anastomoses with branches of the IMA.
-
i.
-
(a)
-
3)
Variants
-
(a)
Aberrant ICA.
-
i.
The ICA enters the temporal bone posterior to the external auditory meatus, ascends between the facial canal and the jugular bulb and passes within the middle ear cavity.
-
May present as a pulsatile mass within the middle ear or with hearing loss; this variant must be kept in mind to avoid a potentially disastrous biopsy procedure.
-
Predilection for woman (67% of patients are female); 15% are bilateral.105
-
As discussed above, the so-called “aberrant ICA” is more appropriately termed ascending pharyngeal artery, and supplies collateral flow to a segmentally atretic internal carotid.18
-
-
i.
-
(b)
Persistent stapedial artery
-
i.
A rare, persistent embryonic vessel that appears as a branch of the vertical segment of the petrous ICA, travels through the middle ear, and gives rise to the middle meningeal artery.106
-
i.
-
(c)
Persistent otic artery (described with the other carotid-vertebrobasilar anastomoses, above).
-
(a)
4.5 Lacerum Segment (C3)
The lacerum segment is a short part of the artery that extends from the petrous ICA to the cavernous segment, over the foramen lacerum. The foramen lacerum is approximately 1 cm long and is filled with fibrocartilage, amounting to a “closed floor” over which the ICA passes.103 The foramen lacerum is not a true foramen, as no significant structures (other than the Vidian nerve) travel through it. The lacerum segment is separated from the cavernous segment by the petrolingual ligament. The petrolingual ligament is a small fold of periosteum that extends from the lingula of the sphenoid bone to the petrous apex,107 and represents a continuation of the periosteum of the carotid canal.75 The lacerum segment lies inferior to the trigeminal ganglion, and has thus been termed the “trigeminal segment” by some authors.108 The foramen lacerum is vulnerable to wayward placement of needles or electrodes during percutaneous procedures, such as foramen ovale instrumentation for trigeminal neuralgia.109 Among patients with basilar skull fractures, the junction between the lacerum and cavernous segments is the most frequently fractured segment of the carotid canal (62% of all carotid canal fractures occur at that site).110
-
1.
Subsegments: None.
-
2.
Branches: None.
-
3.
Variants: None.
4.6 Cavernous Segment (C4)
The cavernous segment is S-shaped and extends from the superior margin of the petrolingual ligament, through the cavernous sinus, to the proximal dural ring (Fig. 1.18). This portion of the ICA is surrounded by areolar tissue, fat, postganglionic sympathetic fibers, and the interconnecting venous chambers of the cavernous sinus. The ICA rests directly against the lateral surface of the body of the sphenoid bone in a groove called the carotid suclus, which defines the course of the cavernous segment of the ICA.111 The cavernous ICA also travels directly adjacent to the wall of the sphenoid sinus; a layer of bone less than 0.5-mm thick separates the artery from the sinus in almost 90% of cases, and a complete absence of bone between the artery and the sinus is present in nearly 10%.111 In some cases, the ICA may actually extend into the sphenoid sinus, an anatomic variant that should be kept in mind during surgery of the sphenoid sinus. The cavernous segment of the ICA forms the greater part of the carotid siphon (Fig. 1.19).

Cavernous internal carotid artery. Lateral view of the cavernous segment of the ICA. Major branches: Posterior trunk: (a) Tentorial artery (1), (b) Inferior hypophyseal artery (2), and (c) Dorsal meningeal artery (3). Lateral trunk: (a) Anteromedial branch (4), (b) Anterolateral branch (5), and (c) Posterior branch (6). Medial branch group is not shown here because they arise from the opposite side of the ICA from that shown

Carotid siphon. The carotid siphon is an S-shaped part to the ICA; it begins at the posterior bend of the cavernous ICA and ends at the ICA bifurcation. It can have an open configuration (a) or a closed one (b), with obvious implications for the ease of endovascular navigation in this region. A closed siphon anatomy can be attributed in some cases to exaggerated tortuosity of the ICA, as can be seen in patients with advanced age or fibromuscular dysplasia122. A CTA image of a closed siphon in a patient with an ophthalmic segment aneurysm (below)
-
1.
Subsegments:112
-
(a)
Posterior vertical
-
(b)
Posterior bend
-
(c)
Horizontal
-
i.
Longest part of the cavernous ICA.
-
i.
-
(d)
Anterior bend
-
(e)
Anterior vertical
-
(a)
-
2.
Branches:
-
(a)
The most prominent branches of the cavernous ICA can be divided into three groups.113 These branches are highly variable; the most consistent branches are the posterior and lateral trunks.112
-
i.
Posterior trunk (meningohypophyseal artery) arises from the posterior bend of the cavernous ICA approximately 10 mm distal to the foramen lacerum.112 All three of the following branches are found in some 70% of dissections:112
-
Tentorial artery. This vessel is the most consistent branch of the posterior trunk, being present in 100% of dissections.114 It has two branches:
-
(a)
Marginal artery of the tentorium (aka artery of Bernasconi and Cassinari).115 Travels posteriorly along the medial edge of the tentorium. This artery may arise directly from the ICA.
-
(b)
Basal tentorial artery. Travels laterally along the border between the tentorium and the petrous ridge. Anastomoses with the middle meningeal artery and the dural arteries of the posterior fossa.6
-
(a)
-
Inferior hypophyseal artery
-
(a)
Travels in a superior and medial direction to supply the posterior lobe of the pituitary gland.116 It anastomoses with the superior hypophyseal artery, the medial branch group, and the contralateral inferior hypophyseal artery.
-
(a)
-
Dorsal meningeal artery. Found traversing Dorello’s canal in 75% of dissections.117 Two branches that supply dura of the skull base:
-
(a)
Lateral clival artery: supplies dura around Durello’s canal and abducens nerve.
-
(b)
Dorsal (aka medial) clival artery: supplies superior clival dura.
-
(a)
-
Recurrent artery of foramen lacerum: Tiny vessel that may anastamose with the carotid branch of the ascending pharyngeal.19
-
-
ii.
Lateral trunk (aka the inferolateral trunk, artery of the inferior cavernous sinus, or lateral main stem) arises from the lateral aspect of the horizontal segment and travels superior to the abducens nerve to supply cranial nerves within the cavernous sinus. It is found in about 66% of dissections.113
-
Anteromedial branch. May anastomose with the ophthalmic artery via its recurrent meningeal branch.
-
Anterolateral branch. May anastomose with the artery of the foramen rotundum.
-
Posterior branch. May anastomose with the cavernous branches of the middle and accessory meningeal arteries.
-
Superior branch. Very small vessel that may anastamose with ophthalmic.19
-
-
iii.
Medial branch group (aka capsular arteries of McConnell) arises from the most superior portion of the cavernous segment, and supplies the pituitary gland. They are found in only about 28% of dissections.113
-
iv.
Other cavernous ICA branches:
-
Ophthalmic artery (found to arise from the cavernous segment, instead of the ophthalmic segment), in about 8% of cases.118
-
Recurrent artery of the foramen lacerum.
-
Artery of the Gasserian ganglion.
-
-
i.
-
(a)
-
3.
Variants:
-
(a)
Kissing intrasellar ICAs
-
(b)
Intercavernous ICA anastomoses
-
(c)
Persistent trigeminal artery (described with the other carotid–vertebro-basilar anastomoses, above).
-
(a)
4.6.1 Angio-Anatomic Correlate! Lateral Trunk Collaterals (Fig. 1.20)

The lateral trunk provides potential collateral flow between the cavernous segment of the internal carotid artery and external carotid artery branches. Carotid artery injection (a) in this patient with prior external carotid artery branches. Carotid artery injection (a) in this patient with prior external carotid ligation shows filling of anterolateral and posterior branches of the lateral trunk (arrows). Later phase of arteriogram (b) shows these branches reconstitute multiple external carotid branches (arrows).
The lateral trunk provides potential collateral flow between the cavernous segment of the internal carotid artery and external carotid artery branches. Carotid artery injection (a) in this patient with prior external carotid ligation shows filling of anterolateral and posterior branches of the lateral trunk (arrows). Later phase of arteriogram (b) shows these branches reconstitute multiple external carotid branches (arrows).
4.7 Clinoidal Segment (C5)
The clinoidal segment comprises a tiny wedge-shaped part of the ICA between the proximal and distal dural rings (Fig. 1.21). The anterior clinoid process lies superior and lateral to the clinoidal ICA, over the part of widest separation between the dural rings. Although this segment is described as “interdural,” the ICA is surrounded in this region by a dural collar that contains venous tributaries of the cavernous sinus, known as the clinoid venous plexus.114 These venous channels extend to the distal dural ring and have implications for surgery in this region.

Clinoidal segment. The clinoidal segment is defined by the proximal (P) and distal (D) dural rings, which are related to one another at an angle, like two dinner plates nearly touching on one edge. The space between the dural rings is wide on the lateral aspect of the ICA and small on the medial aspect, where the dural rings come closest together. The medial part of the distal dural ring is incomplete; this region, which includes the proximal portion of the ophthalmic segment, is known as the “carotid cave” and is a site for aneurysm formation.108,289 The anterior clinoid process (AC) extends like a thumb over the clinoidal segment; the relationships between the dural rings and the anterior clinoid are variable. OA ophthalmic artery, OS optic strut, M medial, L lateral
-
1.
Subsegments: None
-
2.
Branches: The ophthalmic artery may arise from the clinoidal segment in rare cases.1
-
3.
Variants: None.
4.8 Ophthalmic Segment (C6)
The ophthalmic segment is the most proximal intradural part of the ICA and extends from the distal dural ring to the origin of the posterior communicating artery. The average length is 9.6 mm.74 The optic nerve travels superior and medial to the ICA in this region, and the sphenoid sinus is anterior and inferior. The optic strut is a bony process that extends between the base of the anterior clinoid to the body of the sphenoid bone. The optic strut separates the optic canal from the superior orbital fissure, and the identification of the optic strut on CT can help distinguish cavernous segment aneurysms from ophthalmic segment aneurysms.123
-
1.
Subsegments: None.
-
2.
Branches:
-
(a)
Ophthalmic artery (Fig. 1.22)
-
i.
The ophthalmic artery arises from the anterior aspect of the ICA medial to the anterior clinoid process. The vessel originates distal to or at the distal dural ring in ≥90% of cases; in about 8% of cases, the vessel arises from the cavernous segment.118 The artery then usually travels inferior and lateral to the optic nerve in the optic canal. Within the orbit, the ophthalmic artery loops inferior and lateral to the optic nerve in 83% of cases, and then approaches the globe along its medial aspect. In 17% of cases, the ophthalmic artery stays medial and inferior to the optic nerve throughout its course.118
-
ii.
The diameter of the ophthalmic artery at the origin averages 1.4 mm (range, 0.9–2.1 mm).124
-
iii.
Ophthalmic artery branches. The ophthalmic artery branches are highly variable, and anastomoses with the branches of the external carotid artery are extensive. Ophthalmic artery branches can be divided into three groups:
-
1.
Ocular group
-
(a)
Central retinal artery
-
i.
Arises from the ophthalmic artery as a single trunk or in common with a posterior ciliary artery, then penetrates the optic nerve sheath to supply the retina.124 The central retinal artery is a terminal branch of the ophthalmic artery and a true end-artery, with no appreciable collateral circulation. Occlusion of the central retinal artery usually results in loss of vision.
-
ii.
The inner diameter averages 400 μm (range, 300–600 μm).124
-
i.
-
(b)
Ciliary arteries
-
i.
Divided into posterior and anterior ciliary arteries, these vessels produce the choroidal blush seen on lateral angiography.
-
i.
-
(a)
-
2.
Orbital group
-
(a)
Lacrimal artery
-
i.
The lacrimal artery arises from the ophthalmic artery adjacent to the optic nerve and passes along the lateral rectus muscle to irrigate the lacrimal gland and conjunctiva. It anastomoses anteriorly with branches of the superficial temporal artery and with multiple branches of the internal maxillary artery.125
-
ii.
A significant branch of the lacrimal artery is the recurrent meningeal artery, which travels back and out of the orbit through the superior orbital fissure, and anastomoses with the middle meningeal artery.126
-
iii.
Zygomaticofacial branches anastamose with deep temporal and transverse facial branches.126
-
i.
-
(b)
Muscular branches
-
i.
Arteries that irrigate the extraocular muscles and periosteum of the orbit; each branch is named for the structure it irrigates (e.g., muscular branch to the medial rectus).
-
i.
-
(a)
-
3.
Extraorbital group
-
(a)
Ethmoidal arteries
-
i.
These vessels supply the upper nasal mucosa and anastomose with branches of the sphenopalatine branches of the internal maxillary artery. They also perforate the cribriform plate to irrigate the dura of the anterior fossa.
-
ii.
Anterior ethmoidal artery
-
1.
Gives rise to the anterior falx artery, which enters the intracranial space via the foramen caecum.
-
1.
-
iii.
Posterior ethmoidal artery
-
1.
Anastomoses with branches of the sphenopalatine artery.
-
1.
-
i.
-
(b)
Palpebral artery
-
i.
Divides into medial, inferior medial, and superior medial palpebral branches.118 These branches anastomose with the frontal branch of the superficial temporal artery and the infraorbital branch of the internal maxillary artery.
-
i.
-
(c)
Terminal portion of the ophthalmic artery
-
i.
The ophthalmic artery terminates by dividing into the
-
1.
Supratrochlear branch
-
a.
Anastomoses with branches of the superficial temporal artery.
-
a.
-
2.
Dorsal nasal branch
-
a.
Anastomoses with branches of the facial artery.
-
a.
-
1.
-
i.
-
(a)
-
1.
-
iv.
Ophthalmic artery variants
Several anomalous origins of the ophthalmic artery have been described. The most common is a middle meningeal artery origin, seen in nearly 16% of cases in a dissection series127 (conversely, an ophthalmic origin of the middle meningeal artery is seen in about 0.5% of the angiograms.).46 Other reported anomalous origins include the cavernous ICA, the MCA, ACA, PCA, and the basilar artery.118
-
i.
-
(b)
Superior hypophyseal artery
-
i.
There is an average of 1.8 superior hypophyseal arteries arising from the ICA, and most originate within 5 mm of the ophthalmic artery origin.128 Superior hypophyseal arteries appear in two forms: in 42% of cases, a single large artery branches like a candelabra into smaller branches, and in the remaining cases, two or three hypophyseal arteries are present.128 The vessels then travel toward the origin of the pituitary stalk and connect with the branches of the contralateral superior hypophyseal artery and the posterior communicating arteries to form a circuminfundibular anastomosis.128 The superior hypophyseal arteries and the circuminfundibular plexus are distributed to the pituitary stalk and the anterior lobe of the pituitary (the inferior hypophyseal branch of the meningohypophyseal artery irrigates the posterior lobe).74
-
i.
-
(c)
Perforating branches
-
i.
Several perforating branches arising from the ophthalmic segment are not properly included with the superior hypophyseal arteries. They arise from the posterior or medial aspect of the ICA and primarily irrigate the optic chiasm, the optic nerve, the floor of the third ventricle, and the optic tract.74
-
i.
-
(a)
-
3.
Variants: Most anatomic variants of the ophthalmic segment of the ICA amount to anomalous origins of the ophthalmic artery (see above). A fenestration of the ophthalmic segment of the ICA has been reported.129

Ophthalmic artery. Lateral view of a selective ophthalmic artery angiogram (above) and superior views of the ophthalmic artery (OA, a). On the angiogram, note the typical upward course of the OA as it crosses over the optic nerve (arrow) and the choroidal blush (arrowheads). In 83% of cases, the OA passes around the lateral aspect of the optic nerve (b, left); in the remaining cases the OA stays medial to the optic nerve (b, right). Significant branches include: (1) Recurrent meningeal arteries, (2) posterior ethmoidal artery, (3) muscular branches, (4) central retinal artery, (5) ciliary arteries (anterior and posterior), (6) lacrimal artery, and (7) anterior falx artery. The OA can be divided into three segments:290 (1) Segment 1. Extends from the entrance of the OA into the orbit to the point where the vessel changes direction to cross over or under the optic nerve. (2) Segment 2. Short part of the vessel as it passes over or under the nerve. (3) Segment 3. Extends from the bend in the vessel on the medial aspect of the optic nerve, to the edge of the orbit. The safety point, beyond which embolization can be done with minimal risk of embolization of the retina, is generally thought to be anywhere beyond Segment 2291
4.9 Communicating Segment (C7)
The communicating segment begins just proximal to the origin of the posterior communicating artery and ends with the bifurcation of the ICA into the ACA and the MCA. The average length is 10.6 mm.74
-
1.
Branches
-
(a)
Posterior communicating artery
-
i.
The posterior communicating artery arises from the ICA an average of 9.6 mm distal to the ophthalmic artery and 9.7 mm proximal to the ICA bifurcation.74 It travels posteromedially an average distance of 12 mm to join the PCA at the junction between the P1 and P2 segments.
-
ii.
Branches. The number of perforating arteries ranges from four to 14, with an average of 7.8.74 These branches terminate in the floor of the third ventricle, the posterior perforated substance, optic tract, pituitary stalk, and optic chiasm.130 These perforators reach the thalamus, hypothalamus, and internal capsule. These arteries are called anterior thalamoperforators to distinguish them from the thalamoperforators that arise from the P1 segment. The largest and the most constant of these is the premamillary artery.88
-
iii.
Variants
-
1.
Persistent fetal origin. A “fetal configuration” is defined as a prominent P-comm artery that gives rise to, and has the same diameter of, the P2 segment of the PCA (Fig. 1.23). This anatomy is present in 18–22% of cases.88 The ipsilateral P1 segment is usually hypoplastic.
Fig. 1.23 
Persistent fetal configuration of the posterior communicating artery. A posterior communicating artery is a “fetal” variant (arrow) when the diameter of the vessel is equal to the diameter of the P2 segment it connects to
-
2.
Infundibulum. A funnel-shaped origin of the P-comm artery (see below).
-
3.
Hypoplasia. Although a “hypoplastic” P-comm artery is present in up to 34% of the dissections, the complete absence of the vessel is very rare.88
-
4.
Absence. Complete absence of the P-comm artery is found in 0.6% of the dissections.131
-
5.
Fenestration of the P-comm artery has been reported.132
-
1.
-
i.
-
(b)
Anterior choroidal artery
-
i.
The anterior choroidal artery (Fig. 1.24) arises from the posterolateral aspect of the ICA, 2–4 mm distal to the posterior communicating artery, and an average of 5.6 mm proximal to the ICA bifurcation.74 The diameter of the vessel averages 1.0 mm,74 and is duplicated in 4% of cases.133 The anterior choroidal artery has two segments:
Fig. 1.24 
Anterior choroidal artery. On a lateral angiogram, the cisternal segment of the anterior choroidal artery has a characteristic gentle, undulating appearance as it passes around the cerebral peduncle. A kink appears in the vessel (the plexal point, (black arrow)) where it enters the temporal horn. The posterior communicating artery (white arrow) travels inferior and parallel to the anterior choroidal artery
-
1.
Cisternal segment. From the ICA, the vessel travels in a posterior direction, sweeping first medially, then laterally to pass around the cerebral peduncle. The anterior choroidal artery then angles upward as it passes through the choroidal fissure to enter the temporal horn of the lateral ventricle. The cisternal segment averages 24 mm in length and gives rise to an average of eight perforating branches;133 these are the branches of the anterior choroidal artery that irrigate most of the vital structures that are vulnerable to ischemic injury with anterior choroidal artery occlusion.
-
2.
Intraventricular segment. Within the ventricle, the anterior choroidal artery travels with the choroid plexus, anastomosing with branches of the lateral posterior choroidal artery in this region. The artery then arcs up and around the thalamus, and in some cases it reaches as far as the Foramen of Monro and anastomoses with branches of the medial posterior choroidal artery (from the posterior cerebral). Branches from the intraventricular segment supply to the optic tract, lateral geniculate body and thalamus.134
-
1.
-
ii.
Territories
-
1.
The anterior choroidal artery sends branches, in decreasing order of frequency, to the optic tract, cerebral peduncle, lateral geniculate body, uncus, and temporal lobe.74 The brain structures irrigated by these branches include the optic radiation, globus pallidus, midbrain, thalamus, and posterior limb of the internal capsule. Occlusion of the anterior choroidal artery can produce contralateral hemiplegia, hemianesthesia, hemianopia, memory loss, and somnolence. Regions of the brain affected by the anterior choroidal artery occlusion on CT include the posterior limb of the internal capsule, the retrolenticular portion of the internal capsule, the internal portion of the globus pallidus, and the lateral thalamus.135 The severity of neurologic change after occlusion of the vessel is highly variable, however, presumably because of varying anastomoses with the posterior choroidal arteries as well as the PCA (and less commonly, the ACA and MCA). Irving S. Cooper, M.D., a functional neurosurgeon, demonstrated this variability.136 During a subtemporal approach for a cerebral pedunculotomy to treat a patient with Parkinson’s disease, Cooper occluded the anterior choroidal artery because of an inadvertent injury to the vessel. The patient awoke after surgery with complete resolution of his tremor and rigidity and without any persistent hemiparesis. Deliberate occlusion of the anterior choroidal artery was done for the treatment of Parkinson’s disease in the 1950s.137
-
1.
-
iii.
Variants
-
1.
Ectopic origin. Seen in 4% of the dissections.134
-
(a)
The anterior choroidal artery may originate from the MCA or PCA.
-
(b)
Rarely, the anterior choroidal artery may originate from the ICA proximal to the posterior communicating artery.138
-
(a)
-
2.
Absence of the anterior choroidal artery is seen in 3% of angiograms.139
-
3.
Hyperplasia, in which the anterior choroidal artery supplies part of the PCA territory, is seen in 2.3% of angiograms.139
-
1.
-
i.
-
(c)
Perforating branches
-
i.
Perforators arising from the communicating segment extend to the optic tract, floor of the third ventricle, and the anterior perforated substance.74
-
i.
-
(a)


4.10 The Infundibulum: A Normal Variant
An infundibulum is a conical, triangular, or funnel-shaped dilatation at the origin of an artery, and is found most commonly at the junction of the posterior communication artery and ICA (Fig. 1.25). At this location, an infundibulum is defined as a symmetric bulge at the origin of the P-comm, with a maximum diameter of 3 mm.140,141 The authors of this handbook have also found infundibula at the P-comm-PCA junction, the P2 segment, in the anterior communicating artery complex, the ophthalmic artery origin, and at the origin of the anterior choroidal artery. The reported prevalence of infundibula on otherwise normal angiograms is 7–15%.142–144 Bilateral P-comm infundibula are present in 25% of cases. Angiographic criteria for infundibular dilation include round or conical in shape, ≤3 mm in the maximum diameter, without aneurysmal neck, and with a posterior communicating artery arising from its apex.140

Posterior communicating artery infundibulum
5 Circle of Willis
The circle of Willis is the ring of interconnecting vessels encircling the pituitary infundibulum providing important collateral circulation between the carotid territories and the vertebrobasilar system (Fig. 1.26). It is actually a nonagon, a nine-sided structure, rather than a circle. Although it bears the name of Thomas Willis (named in honor of Willis by his student Lower), who described the structure in 1664 in a publication illustrated by Sir Christopher Wren,145 earlier anatomists had recognized an arterial circle at the base of the brain.146 Although a complete circle of Willis is present in some 90% of individuals, a well-developed and symmetric circle is found in ≤50% of cases.147 In some 60% of cases, at least one component of the circle is relatively hypoplastic and diminished in its capacity to provide collateral flow.1 Asymmetry of the circle of Willis results in significant asymmetric flow148 and is an important factor in the development of intracranial aneurysms and in ischemic stroke. Patients with aneurysms are more likely to have asymmetry or an anomaly of the circle.149 The presence of a nonfunctional anterior collateral pathway in the circle of Willis in patients with ICA occlusive disease is strongly associated with ischemic stroke.150 The individual components of the circle are discussed separately in this handbook. Anatomic variations causing asymmetry of the circle are listed in Table 1.6.

Circle of Willis
5.1 Anterior Cerebral Artery
Several classification schemes for the ACA have been described. The simplest and most common system includes three segments (Fig. 1.27):

Anterior cerebral artery. Left lateral oblique view of the left ACA
-
1.
A1. From ICA to anterior communicating artery
-
2.
A2. From anterior communicating artery to the origins of the pericallosal and supramarginal arteries
-
3.
A3. Distal branches
5.2 A1 Segment and Anterior Communicating Artery Complex
The A1 segment (aka the precommunicating segment)1 extends from the ICA bifurcation in a medial and superior direction to its junction with the anterior communicating artery within or just inferior to the interhemispheric fissure. It travels superior to the optic chiasm or optic nerves and inferior to the anterior perforated substance. The A-comm complex is highly variable and may take one of the four main patterns (Fig. 1.28). The A-comm artery averages 4.0 mm in length and 1.7 mm in diameter.151

Anterior communicating artery complex. In most cases, the A-comm complex assumes one of the four configurations151. (a) A single or duplicated A-comm forms a bridge between the ACAs. (b) A single large branch arises from the A-comm. (c) The A-comm vessel is not present, and the two ACAs join together directly. (d) Azygos ACA
-
1.
Branches
-
(a)
A1 perforating branches can be divided into superior and inferior branches
-
i.
Some 2–15 superior branches are medial lenticulostriate arteries that travel superiorly and posteriorly into the anterior perforated substance and supply the anterior hypothalamus, septum pellucidum, anterior commissure, fornix, and the anterior striatum.152
-
ii.
Inferior branches supply the optic chiasm and optic nerves.
-
i.
-
(b)
A-comm artery branches
-
i.
Perforating branches of the A-comm artery can be divided into subcallosal, hypothalamic, and chiasmatic branches, according to their vascular territories.151 The subcallosal branch is usually single and the largest branch of the A-comm artery; it supplies the septum pellucidum, columns of the fornix, corpus callosum and lamina terminalis.153 The hypothalamic branches are smaller and multiple. A chiasmatic branch is present in only 20% of cases.151
-
i.
-
(c)
The recurrent artery of Heubner, most often an A2 branch, may arise from the A1 segment in up to 17% of cases and from the ACA-A-comm junction in 35% of cases.154,155 (See below for further discussion of Heubner).
-
(a)
-
2.
Variants
-
(a)
A1 variants
-
i.
Asymmetry. The left and right A1 segments are asymmetric in size in up to 80% of cases.6 Right A1 segments tend to be longer, more tortuous, deviated and narrow than left A1 segments.156 About 10% of the A1 vessels are hypoplastic (defined as having a diameter of ≤1.5 mm).152
-
ii.
Absence. Absence of one A1 segment is seen in 1–2% of cases.1
-
iii.
Persistent olfactory artery. Rare anomaly in which a persistent primitive olfactory artery travels from the ICA, along the olfactory tract, to supply the distal ACA territory.157 May be associated with an aneurysm.158
-
iv.
Infraoptic ACA. In rare cases the A1 segment may travel inferior to or through the optic nerve.159–161 Associated with aneurysms (Fig. 1.29).
Fig. 1.29 
Infraoptic anterior cerebral artery. The infraoptic ACA originates in an unusually proximal location from the ICA (arrow)
-
v.
Fenestration of the A1 segment is rare and is associated with aneurysms.162–164
-
vi.
Accessory ACA. An atypical branch of the ICA courses under the optic nerve and ACA to give rise to the orbitofrontal and frontopolar arteries.165
-
vii.
Anomalous origins of the A1 from the cavernous ICA,166 from the ICA at or proximal to the ophthalmic artery,167 and from the contralateral ICA168 have been reported.
-
i.
-
(b)
A-comm artery variants. Some 227 A-comm artery complex variations have been described.169 A “normal” A-comm artery, in which single vessel forms a link between two non-anomalous ACAs, is present in only about 40% of cases.151,154,169,170 Anomalous A-comm anatomy is present in the remaining 60% of cases. These patterns included the plexiform (i.e., multiple complex vascular channels, 33%), dimple (i.e., incomplete fenestration, 33%), fenestration (21%), duplication (18%), string (18%), fusion (12%), median artery of the corpus callosum (6%), and azygos ACA (3%).151 The A-comm artery is absent in some 5% of cases.171
-
(a)

5.3 A2 Segment
The A2 segment travels in a vertical direction from the A-comm artery to its division into the pericallosal and callosomarginal arteries, adjacent to the genu of the corpus callosum. Defined in this way, the A2 segment is analogous to the M1 segment of the MCA, which is defined in this handbook as ending with its bifurcation into the superior and inferior divisions. Although the authors of this handbook prefer this definition of the A2 segment, it is somewhat problematic, as some 18% of the hemispheres do not have a definite callosomarginal branch.172 Other authors have defined the A2–A3 junction as the part of the ACA immediately anterior to the corpus callosum genu1 or at the junction between the rostrum and genu of the corpus callosum.6
The length of the A2 segment averages 43 mm when it is defined as extending from the A-comm to the origin of the callosomarginal artery.172 The left and right A2 segments usually travel together in the interhemispheric fissure, although the right A2 is more often (72% of cases) anterior to the left A2 in the sagittal plane.172
-
1.
Branches
-
(a)
Perforators. Perforating branches of the A2 segment are located along the first 5 mm of the segment, and penetrate the brain at the gyrus rectus and olfactory sulcus.154
-
(b)
Recurrent artery of Heubner. This artery, which is a large lenticulostriate artery, arises from the A2 segment in most (57–78%) cases.152,154 It doubles back and runs in the opposite direction to the A1 segment to enter the lateral anterior perforated substance lateral to the ICA bifurcation.155 The artery supplies the head of the caudate nucleus, anterior limb of the internal capsule, and the anterior third of the putamen.173 Although it is often not large enough to be seen on angiography (Fig. 1.30), it is regularly identified during surgery of the A-comm complex; inadvertent occlusion of the vessel can occur by pinching the vessel during retraction of the frontal lobe. Isolated infarction of the territory of this vessel can be clinically silent, or produce a hemiparesis that is most prominent in the face and upper extremity.6
Fig. 1.30 
Recurrent artery of Heubner. Left carotid injection with filling of contralateral A2 segment via the A-comm artery. The recurrent artery of Heubner is visible (arrow) because it is not obscured by other arteries. Clipping of the aneurysm could put the recurrent artery of Heubner at risk
-
(c)
Orbitofrontal artery. This artery is the first cortical branch of the A2 segment, and may appear as two or three vessels rather than single branch.172 The artery runs close to the midline in an anterior direction to the gyrus rectus, olfactory bulb, and medial aspect of the inferior frontal lobe.
-
(d)
Frontopolar artery. This artery may also appear as a group of vessels and usually arises from the distal A2 segment, below the corpus callosum. It travels anteriorly and superiorly towards the frontal pole.
-
(a)
-
2.
Variants
-
(a)
Bihemispheric ACA. In this variant, one A2 segment is hypoplastic and the other A2 vessel irrigates both the hemispheres. Present in up to 7% of cases.172
-
(b)
Azygos ACA. This is defined as a single unpaired A2 segment that arises from the junction of the A1s (Fig. 1.31). It is present in ≤1% of the general population;174 as many as 41% of patients with an azygos ACA have a terminal aneurysm.175,176 This anomaly is also associated with holoprosencephaly.177
Fig. 1.31 
Azygos anterior cerebral artery. In an azygos anterior cerebral artery, both A1 segments join to form single A2 segment
-
(c)
Duplicated A2. More than one A2 segment has been reported in up to 13% of cases.1 In some cases, this may represent persistence of the primitive median artery of the corpus callosum,1 which is found in 6% of cases.151
-
(d)
Superior anterior communicating artery. An anomalous communicating vessel between the ACAs near the corpus callosum has been described and is associated with aneurysms.178
-
(a)


5.4 A3 Branches
The “A3 branches” include all the ACA branches distal to the origin of the pericallosal and callosomarginal arteries (Fig. 1.32). The distal ACA may be further subdivided into A4 and A5 segments;76,172 the A3 segment is defined as the part of the ACA that extends around the genu of the corpus callosum, and the A4 and A5 segments comprise the part of the ACA that travels posteriorly over the corpus callosum. The A4 and A5 segments are separated by the coronal suture.172 The distal ACA branches have extensive anastomoses with distal branches of the MCA and PCA. These connecting arteries, in the furthest reaches of the intracranial circulation, comprise the watershed zones; the corresponding territories of the brain are the most vulnerable to ischemia during hemodynamic failure.

Distal ACA branches. (1) Orbitofrontal artery; (2) frontopolar artery; (3) anterior internal frontal artery; (4) middle internal frontal artery; (5) posterior internal frontal artery; (6) paracentral artery; (7) superior parietal artery; (8) inferior parietal artery; (9) callosomarginal artery; (10) pericallosal artery
-
1.
Branches
-
(a)
Pericallosal artery. The pericallosal artery is the main trunk of the ACA as it passes posteriorly over the corpus callosum. It gives off multiple small branches (“short callosal arteries”)172 that travel laterally along the corpus callosum (Fig. 1.33) and anastomose with the splenial artery (the “posterior pericallosal branch”), a branch of the PCA. Infrequently, a “long callosal artery” may be present, which is a branch of and runs parallel to the pericallosal artery.172
Fig. 1.33 
The smile and the mustache. During the late arterial phase of an AP angiogram (high magnification, inset), the branches of the pericallosal artery curve upward along the surface of the corpus callosum, forming a smile (a, black arrows). Branches of the callosomarginal artery curve downward, forming a mustache (b, white arrows). This pattern is nicely demonstrated in a photograph of someone looking quite a bit like the senior author of this handbook (b). Black bars have been placed across his eyes to protect his privacy and to comply with HIPAA regulations
-
(b)
Callosomarginal artery. The callosomarginal artery is the second largest distal branch of the ACA, after the pericallosal artery. It travels superiorly over the cingulate gyrus to run in a posterior direction within the cingulate sulcus. It is absent in 18% of hemispheres.172
-
(c)
Internal frontal branches. These branches are identified according to which part of the superior frontal gyrus they supply. They may arise from the pericallosal or the callosomarginal artery.
-
i.
Anterior internal frontal arteries
-
ii.
Middle internal frontal arteries
-
iii.
Posterior internal frontal arteries
-
i.
-
(d)
Paracentral artery. This vessel arises from the pericallosal or callosomarginal artery midway between the genu and splenium of the corpus callosum, to supply the paracentral lobule.
-
(e)
Parietal arteries. These are the final and most distal branches of the ACA. They supply the medial aspect of the hemisphere above the corpus callosum and most of the precuneus.179 They anastomose with the parieto-occipital branch of the PCA. They can be divided into:
-
i.
Superior parietal artery
-
ii.
Inferior parietal artery
-
i.
-
(a)
-
2.
Variants

Mnemonic for the cortical ACA branches |
|---|
On Frontal Imaging, Find Peace and Prosperity |
Orbitofrontal artery |
Frontopolar artery |
Internal Frontal Branches (anterior, middle, and posterior) |
Paracentral artery |
Parietal arteries (superior and inferior) |
The two Ps at the end of the mnemonic also serve to remind the reader of the Posterior Pericallosal artery, which anastomose with the distal end of the ACA. |
6 Middle Cerebral Artery
Most classification schemes divide the MCA into four segments. The authors of this handbook favor the following system (Fig. 1.34):

Middle cerebral artery
-
1.
M1 From ICA to the bifurcation (or trifurcation)
-
2.
M2 From the MCA bifurcation to the circular sulcus of the insula
-
3.
M3 From the circular sulcus to the superficial aspect of the sylvian fissure
-
4.
M4 Cortical branches
6.1 M1 Segment
The M1 segment (aka horizontal segment or sphenoidal segment)180 arises from the ICA and travels in a lateral direction, parallel to the sphenoid wing, and terminates by dividing into the M2 segments. The M1 origin is usually twice the size of the A1 origin.1 Although most anatomic studies define the M1 segment as the ending where the MCA branches take a 90° turn within the sylvian fissure76,180 (and thus having both prebifurcation and postbifurcation subsegments), the division point of the main MCA trunk is considered by most clinicians to be the M1/M2 junction.6 The MCA bifurcates in 71% of cases, trifurcates in 20% of cases, and divides into four branches in 9% of cases.181 The M1 segment averages about 16 mm in length.181
-
1.
Branches
-
(a)
Lateral lenticulostriate branches. Approximately 80% of the lenticulostriates that arise from the MCA arise from the M1 segment. These branches average 10 in number,181,182 and most arise from the superior aspect of the M1 segment. They enter the anterior perforated substance to supply the anterior commissure, internal capsule, caudate nucleus, putamen, globus pallidus, and substantia innominata.
-
(b)
Anterior temporal artery. The anterior temporal artery typically arises near the midpoint of the M1 segment. Less commonly, it arises from the inferior division (an M2 segment) or as part of an M1 trifurcation. It travels in an anterior and inferior direction over the temporal tip and does not usually enter the sylvian fissure itself.1 It supplies the anterior temporal lobe.
-
(a)
-
2.
Variants
-
(a)
MCA duplication. This anomaly consists of a large MCA branch arising from the ICA proximal to the ICA bifurcation, and has a frequency of 0.2–2.9%.183 This vessel travels parallel and inferior to the main M1 segment and primarily supplies the anterior temporal lobe.183,184 It is associated with aneurysms.185,186
-
(b)
Accessory MCA. An accessory MCA arises from the ACA and runs parallel to the M1 segment, and has a prevalance of 0.3–4.0%.183,187 There is a classification scheme for accessory MCAs:188 Type 1 arises from the ICA (i.e., MCA duplication), type 2 from the A1 segment, and type 3 from the A2 segment. The accessory MCA primarily supplies the orbitofrontal area,189 and is also associated with aneurysms.185,190 This anomaly should be not be confused with a large recurrent artery of Heubner.191
-
(c)
Aplasia. Aplasia of the MCA is rare and is associated with aneurysms.192
-
(d)
Fenestration. Fenestration of the M1 segment has been reported.184
-
(a)
6.2 M2 Segments
The M2 segments (aka insular segments) extend from the main division point of the M1 segment, over the insula within the sylvian fissure, and terminate at the circular sulcus of the insula. The MCA divisions are equal in diameter and size in 18% of the hemispheres; the superior division is larger (dominant) in 28% of the hemispheres and the inferior division is larger in 32% of the hemispheres.180 The cortical area supplied by the superior division extends from the orbitofrontal area to the posterior parietal area. The cortical area supplied by the inferior division extends from the temporal pole to the angular area. The M2 segments number from six to eight arteries at the point of transition into the M3 segments.
6.3 M3 Segments
The M3 segments (opercular segments) begin at the circular sulcus of the insula and end at the surface of the sylvian fissure. These vessels travel over the surface of the frontal and temporal opercula to reach the external surface of the sylvian fissure. The M3 branches, together with the M2 vessels, give rise to the stem arteries, which in turn give off the cortical branches. There are usually eight stem arteries per hemisphere, and each one typically gives rise to one to five cortical branches.180
6.4 M4 Branches
The M4 branches (aka cortical branches) begin at the surface of the sylvian fissure and extend over the surface of the cerebral hemisphere (Figs. 1.35 and 1.36). The smallest cortical branches arise from the anterior sylvian fissure and the largest ones emerge from the posterior sylvian fissure.180 The cortical branches can be grouped according to the region of the cortex that they supply; any given region may have a single artery or several arteries supplying it. The following 12-subdivision system is in common usage.1,180,193 Although each branch is discussed as a single artery, any given cortical artery may actually exist as several branches (up to five) from a single stem artery.

MCA cortical branches. The most common branching pattern of the MCA is shown: (1) anterior parietal artery, (2) posterior parietal artery, (3) angular artery, (4) temporo-occipital artery, (5) posterior temporal artery, (6) middle temporal artery, (7) anterior temporal artery, (8) temporopolar artery, (9) orbitofrontal artery, (10) prefrontal artery, (11) precentral artery, and (12) Central artery

Mnemonic for the cortical MCA branches. Because of the astonishing coincidence that there are 12 cortical branches and 12 h on the clock, the cortical branches can be remembered by assigning each one to an hour of the day. The central artery occupies the central position on the clock, that of high noon. The position of the angular artery at 3 o’clock, reflects the importance of that vital artery, because, as we all know, 3 o’clock was the time that school let out when we were kids. The middle temporal artery is at 6 o’clock, which is in the middle position at the bottom of the clock. The orbitofrontal artery is at the extreme left position, at 9 o’clock, which is appropriate because the orbitofrontal artery is the most extreme anterior branch of the MCA
-
1.
Orbitofrontal artery May arise from the M1 or M2 segment, and may share a common origin with the prefrontal artery. Travels within the anterior horizontal ramus of the sylvian fissure to supply orbital surface of the frontal lobe.
-
2.
Prefrontal artery May share a common origin with the orbitofrontal artery. Supplies the opercular part of the inferior frontal gyrus and most of the middle frontal gyrus.
-
3.
Precentral artery Travels in the precentral sulcus. Supplies part of the inferior frontal gyrus and the inferior part of the precentral gyrus.
-
4.
Central artery (aka Rolandic artery) Travels within the central sulcus. May share a common origin with the anterior parietal artery. Largest MCA branch to the frontal lobe.180 Supplies the superior part of the precentral gyrus and the inferior half of the postcentral gyrus.
-
5.
Anterior parietal artery May arise with the central artery or the posterior parietal artery. Travels in the postcentral sulcus. Supplies the superior part of the postcentral gyrus, the upper part of the central sulcus, the anterior part of the inferior parietal lobule, and the anteroinferior part of the superior parietal lobule.
-
6.
Posterior parietal artery The most posterior ascending branch of the MCA. May share a common trunk with the anterior parietal artery or the angular artery. Supplies the posterior part of the superior and inferior parietal lobules, including the supramarginal gyrus.
-
7.
Angular artery The terminal and largest branch of the MCA. It emerges from the posterior end of the sylvian fissure to travel over the superior temporal gyrus and terminate over the superior half of the occipital lobe. Supplies the posterior part of the superior temporal gyrus, and parts of the supramarginal and angular gyri, and superior parts of the lateral occipital lobe.
-
8.
Temporo-occipital artery May share an origin with the angular artery. Supplies the posterior half of the superior temporal gyrus, the posterior extent of the middle and inferior gyri, and the inferior parts of the lateral occipital lobe.
-
9.
Posterior temporal artery Leaves the posterior sylvian fissure and crosses over the superior and middle temporal gyri. Supplies the middle and posterior parts of the superior temporal gyrus, the posterior third of the middle temporal gyrus, and the posterior extent of the inferior temporal gyrus.
-
10.
Middle temporal artery Emerges from the middle of the sylvian fissure. Supplies the middle parts of the temporal gyri.
-
11.
Anterior temporal artery Passes inferiorly and posteriorly over the temporal lobe, and terminates in the middle temporal sulcus. Supplies the anterior parts of the superior, middle, and inferior temporal gyri.
-
12.
Temporopolar artery Supplies the anterior pole of the temporal lobe.
The cortical branches can be grouped according to which lobe they supply:193
-
1.
Frontal lobe Orbitofrontal, prefrontal, precentral, and central arteries
-
2.
Parietal lobe Anterior and posterior parietal arteries and angular artery
-
3.
Temporal lobe Temporopolar, anterior, middle and posterior temporal arteries, and temporo-occipital artery
-
4.
Occipital lobe Temporo-occipital artery
The cortical branches can also be grouped according to which M2 segment they arise from:180
-
1.
Superior division Orbitofrontal, prefrontal, precentral, and central arteries.
-
2.
Inferior division Temporopolar, temporo-occipital, angular, and anterior, middle, and posterior temporal arteries.
-
3.
Dominant division (these branches may arise from either division, and usually come off of the larger of the MCA divisions). Anterior and posterior parietal arteries.
Leptomeningeal collaterals |
|---|
These are a network of anastamotic channels up to 1 mm in diameter connecting distal cortical arterial branches.194 Otto Heubner first described their existence in 1874.195 Since then there has been increasing recognition of their importance in cases of ischemic stroke.196 They are quite variable in size and distribution197 and this may explain variable outcomes in situations of arterial occlusions. These collaterals may also be the target of therapeutic maneuvers such as blood pressure modification in cases of cerebral vasospasm or other causes of ischemia. |
|

7 Posterior Cerebral Artery
Most classification schemes for the PCA include three or four segments. The following system is the most common (Fig. 1.38):

Posterior cerebral artery. The most common PCA configuration is on the left, and the persistent fetal origin of the PCA is on the right
-
1.
P1 From the basilar artery bifurcation to the junction with the P-comm artery.
-
2.
P2 From the P-comm artery to the posterior aspect of the midbrain.
-
3.
P3 From the posterior aspect of the midbrain to the calcarine fissure.
-
4.
P4 The terminal branches of the PCA distal to the anterior limit of the calcarine fissure.
7.1 PCA Branches
The PCA branches (Fig. 1.39) can be divided into three categories:

Major branches of the posterior cerebral artery. (1) Posterior communicating artery; (2) hippocampal artery; (3) posteromedial choroidal artery; (4) anterior temporal artery; (5) middle temporal artery; (6) posterior temporal artery; (7) posterolateral choroidal artery; (8) splenial artery; (9) parieto-occipital artery; (10) Calcarine artery
-
1.
Perforating branches, to the brainstem and thalamus
-
2.
Ventricular branches
-
3.
Cortical branches
Perforating branches arise from the P1 and P2 segments. Ventricular branches originate mostly from the P2 segment. Cortical branches arise from the P2, P3, and P4 segments. Perforating arteries are divided into direct branches, which pass directly into the brain, and circumflex vessels, which travel around the brainstem for various distances before entering the brain.
7.2 P1 Segment
The P1 segment (aka precommunicating, mesencephalic or horizontal segment) lies immediately superior to the oculomotor and trochlear nerves. The average length is 6.6 mm; when a fetal PCA is present, the vessel averages 8.6 mm in length.198
-
1.
Branches
-
(a)
Perforators
-
i.
Direct perforating branches (posterior thalamoperforating arteries) from the P1 segment pass directly into the brainstem. These are termed the posterior thalamoperforators to distinguish them from the anterior thalamoperforators, which arise from the P-comm artery. These arteries average 2.7 in number,198 and arise from the posterior and superior aspects of the P1 segment, although, rarely, they may arise from the anterior aspect of the vessel.130 The direct perforators enter the brain medial cerebral peduncles and posterior perforated substance to supply parts of the thalamus, brainstem, and posterior internal capsule.
-
ii.
Circumflex arteries. The circumflex arteries (aka peduncular, mesencephalic, or tegmental thalamoperforating arteries) arise from the P1 and P2 segments and encircle the midbrain parallel and medial to the PCA. They are subdivided into short and long circumflex arteries. The short and long circumflex arteries number 0.8 and 1.3 per hemisphere, respectively.198
-
1.
Short circumflex arteries One or more short circumflex arteries travel a short distance around the brainstem before entering the brain, and reach only as far as the geniculate bodies. Most short circumflex arteries arising from P1 terminate at the posterolateral border of the peduncle.198
-
2.
Long circumflex arteries Up to three long circumflex arteries (aka quadrigeminal arteries) pass around the brainstem, to supply the geniculate bodies and superior colliculi. They arise from the PCA distal to the origin of the short circumflex arteries; in 80% of cases they arise from P1 and in the remaining cases they arise from P2.198 The long circumflex artery anastomoses with the branches of the superior cerebellar arteries.
-
1.
-
i.
-
(b)
Posteromedial choroidal artery This vessel usually arises from the P2 segment (see below), but arises from the P1 segment in 12% of cases.198
-
(c)
Meningeal branch (aka artery of Davidoff and Schecter). A small branch from the P1 segment to supply a midline strip of the inferior surface of the tentorium may be enlarged by pathological processes.199
-
(a)
-
2.
Variants
-
(a)
Side-to-side asymmetry of the P1 segments common is present in 52% of angiograms.200 When a fetal P-comm artery is present, the ipsilateral P1 is typically hypoplastic, and may not fill noticeably on angiography, making it appear to be absent or occluded.
-
(b)
In some persistent carotid–vertebrobasilar anastomoses, the PCA may be supplied by branches from the carotid system (see above).
-
(c)
True anomalies of the P1 segment are uncommon, accounting for 3% of cases in an autopsy series.201 These include duplication, fenestration, and a bilateral shared origin of the PCA and SCA.
-
(d)
Congenital absence of the P1 is rare.130
-
(e)
There may be a prominent perforating branch that supplies portions of both the ipsilateral and contralateral thalamus and potentially mid-brain.202 This perforator has been called the artery of Percheron.203,204
-
(a)
7.3 P2 Segment
The P2 segment (aka ambient segment) is relatively long, averaging 50 mm in length.198 It is subdivided by some authors into an anterior half and a posterior half for discussion of surgical approaches.198 The P2 segment begins at the P-comm artery junction and travels around the lateral aspect of the midbrain within the ambient cistern, parallel and inferior to the basal vein of Rosenthal. Other adjacent structures are the trochlear nerve, the free edge of the tentorium, and the superior cerebellar artery.
-
1.
Branches
-
(a)
Perforators
-
i.
Direct perforators
-
1.
Thalamogeniculate arteries originate from the midportion of the P2 segment, and arise in a superior and lateral direction to perforate the inferior surface of the geniculate bodies. They number 1–3 per hemisphere,198,205 and supply the posterior half of the lateral thalamus, the posterior limb of the internal capsule, and the optic tract.
-
2.
Peduncular perforating arteries pass directly into the cerebral peduncle and supply multiple structures within the brainstem as well as parts of the oculomotor nerve. They average 2.8 per hemisphere.198
-
1.
-
ii.
Circumflex arteries. The circumflex arteries usually arise from the P1 segment. In 20% of cases the long circumflex artery arises from the P2 segment.198
-
i.
-
(b)
Posteromedial choroidal artery (Fig. 1.40). This artery (aka medial posterior choroidal artery) is single in 54% of the hemispheres and may be duplicated or triplicated.198 The vessel arises from the P2 segment in most cases. Other sites of origin of the posteromedial choroidal artery are the P1 segment (12%), P3 %pent (4%), parieto-occipital artery (10%), and calcarine artery (3%),198 or, rarely, the basilar artery.206 The posteromedial choroidal artery has two segments:
Fig. 1.40 
Posteromedial choroidal artery. The undulating course of the posteromedial choroidal artery as it passes over the quadrigeminal plate, gives it a characteristic undulating “3” pattern (arrows)
-
i.
Cisternal segment. This segment averages 42 mm in length.207 From its origin, the vessel curves around the brainstem medial to the main trunk of the PCA and gives off small tegmental branches before it turns forward adjacent to the pineal gland to enter the roof of the third ventricle. The tegmental branches irrigate portions of the midbrain, tectal plate, pineal gland, thalamus, and medial geniculate body.
-
ii.
Plexal segment. This segment travels anteriorly within the velum interpositum between the thalami, adjacent to the internal cerebral vein and the contralateral medical posterior choroidal artery. It travels through the foramen of Monro to enter the choroid plexus of the lateral ventricle and anastomose with the terminal branches of the lateral posterior choroidal artery. Branches from the plexal segment irrigate the choroid plexus of the third ventricle, as well as the thalamus and the stria medullaris.207
-
i.
-
(c)
Posterolateral choroidal arteries. Unlike the posteromedial choroidal artery, the posterolateral choroidal arteries are multiple in the majority (84%) of cases207 and number up to nine (average: 4).198 They arise from the P2 segment in 51% of cases; other sites of origin include the parieto-occipital (13%), anterior temporal (10%), hippocampal (8%), posterior temporal (9%), posteromedial choroidal (4%), calcarine (2%), or middle temporal artery (2%).198 The sizes of these arteries are inversely proportional to the size of the anterior choroidal artery.208 The posterolateral choroidal arteries travel laterally to enter the choroidal fissure, and have two segments:
-
i.
Cisternal segment. The cisternal segment averages 23 mm in length and sends branches to the thalamus, geniculate bodies, fornix, cerebral peduncle, pineal body, corpus callosum, tegmentum, and temporal occipital cortex.207
-
ii.
Plexal segment. This segment begins with the passage of the lateral posterior choroidal arteries through the choroidal fissure lateral to the ambient cistern at the level of the temporal horn or atrium. They travel along the medial border of the choroid plexus in the lateral ventricle, eventually intermingling with branches of the medial posterior choroidal artery in the body of the ventricle and at the foramen of Monro.207 Branches from plexal segment vessels irrigate the choroid plexus and penetrate the ventricular surfaces of the thalamus and fornix.
-
i.
-
(d)
Hippocampal artery. A hippocampal artery arises from the P2 segment in 64% of cases; when present, it is the first cortical branch of the PCA.198 This artery supplies the uncus, hippocampal gyrus, hippocampal formation, and dentate gyrus. Some authors include the hippocampal artery with the inferior temporal arteries.198
-
(e)
Inferior temporal arteries. The inferior temporal arteries are distinguished from the temporal arteries, which are branches of the MCA. The inferior temporal arteries are variable and may appear as a single initial branch of the P2 segment, called a common temporal artery (aka lateral division of the PCA or lateral occipital artery), which is seen in 16% of cases.198
-
i.
Anterior inferior temporal artery. The anterior temporal artery is usually the second cortical branch of the PCA. It may be duplicated. It travels anteriorly and laterally inferior to the hippocampal gyrus, and anastomoses with anterior temporal branches of the MCA.200
-
ii.
Middle inferior temporal artery. A middle temporal artery is present in 38% of hemispheres and supplies the inferior surface of the temporal lobe.198
-
iii.
Posterior inferior temporal artery (Fig. 1.41). The posterior temporal artery is a prominent branch of the PCA and usually arises from the inferior and lateral aspect of the P2 segment and travels obliquely toward the occipital pole. It supplies the inferior temporal and occipital surfaces. This vessel arises from the P3 segment in 6% of cases.
Fig. 1.41 
The PCA pitchhfork. A distinctive identifying landmark of the PCA on a lateral view is the “pitchhfork” appearance of the take-off of the posterior temporal artery from the main trunk of the PCA. Visualization of this feature can help distinguish the PCA from other arteries on a cluttered angiogram
-
i.
-
(f)
Parieto-occipital artery. The parieto-occipital artery arises as a single trunk from the P2 segment slightly more often than from the P3 segment.198 It travels posteriorly and laterally within the parieto-occipital fissure, which separates the parietal lobe from the occipital lobe, to supply the posterior parasagittal region, cuneus, precuneus, and lateral occipital gyrus. In 24% of cases it sends branches through the choroidal fissure into the lateral ventricle.
-
(g)
Calcarine artery. The calcarine artery arises from the P2 segment slightly less commonly than from the P3 segment (see below).
-
(h)
Splenial artery. The splenial artery originates from the P2 segment in 4% of cases (see below).198
-
(i)
Artery of Davidoff and Schechter (dural branch). Generally only seen in pathological conditions, this artery supplies the apex of the tentorium, walls of the vein of Galen, and then curves forward along the free edge of the falx cerebri.209 It can also provide some collateral supply to the superior vermis and inferior colliculi.210 The artery of Davidoff and Schechter is often difficult to see angiographically, even when enlarged, due to superimposition with other PCA branches. It is more commonly found on the left.211
-
(a)
-
2.
Variants
-
(a)
Anomalous origin of cortical branches. In rare cases, the parieto-occipital, posterior temporal, or calcarine artery may arise directly from the ICA.1,212 Similarly, anomalous anterior choroidal artery supply to temporal, parietal and occipital cortical regions normally supplied by branches of the PCA has been reported.213
-
(a)



7.4 P3 Segment
The P3 segment (aka quadrigeminal segment) extends in a medial and posterior direction from the quadrigeminal plate to the anterior limit of the calcarine fissure, and averages 20 mm in length. The P3 segments from each side approach each other. The point where the two PCAs are nearest to each other is referred to as the collicular, or quadrigeminal point; this separation averages 8.9 mm.198 The PCA often divides into its two terminal branches (the calcarine and parieto-occipital arteries) between the quadrigeminal plate and the calcarine fissure.
-
1.
Branches
-
(a)
Parieto-occipital artery. The parieto-occipital artery arises from the P3 segment in 46% of the hemispheres (see above).
-
(b)
Posterolateral choroidal artery. This artery arises from the P3 segment in 11% of cases (see above).207
-
(a)
7.5 P4 Segment
The P4 segment begins at the anterior limit of the calcarine fissure, and includes one of the two main terminal branches of the PCA, the calcarine artery. The other main terminal branch of the PCA, the parieto-occipital artery, frequently arises from the P2 or P3 segment.
-
1.
Branches
-
(a)
Calcarine artery. The calcarine artery travels posteriorly and medially within the calcarine fissure to reach the occipital pole. It is duplicated in 10% of cases and arises from the parieto-occipital artery in 10% of cases.198 The calcarine artery sends branches to the lingual gyrus and inferior cuneus; it primarily supplies the visual cortex.
-
(b)
Splenial artery. The splenial artery (aka posterior pericallosal artery) arises from the parieto-occipital artery in 62% of cases, but may arise from the calcarine artery (12%), posteromedial choroidal artery (8%), posterior temporal artery (6%), P2 or P3 segments (4% each) or the posterolateral choroidal artery (4%).198 The splenial artery is relatively constant and travels superiorly around the splenium of the corpus callosum to anastomose with the pericallosal artery.
-
(a)
8 Vertebral Artery
The vertebral artery has four segments (Fig. 1.43):

Vertebral artery
-
1.
V1 From the subclavian artery to the foramen transversarium of C6.
-
2.
V2 From C6 to the foramen transversarium of C1.
-
3.
V3 From the C1 to the dura.
-
4.
V4 Intradural part of the vertebral artery.
8.1 V1 Segment
The V1 segment (extraosseous segment) arises from the posterosuperior wall of the subclavian artery (Fig. 1.44) and travels in a superior and posterior direction. It passes posterior to the anterior scalene muscles and enters the transverse foramen of the C6 (90% of most cases), C5 (7%) or C7 (3%). Supplies the stellate ganglion.214

Vertebral artery origin. Anterolateral view of a cervical spine CT angiogram showing the right vertebral artery (arrow) arising from the posterior wall of the subclavian artery. The optimal angiographic projection is usually an AP view with 20–30° of Townes
-
1.
Variants
-
(a)
Anomalous origin. The left vertebral artery arises directly from the aortic arch in about 0.5% of cases.1 Anomalous origins of the right vertebral artery from the arch,215 of both vertebral arteries from the arch,216 and of the right vertebral artery from the right common carotid artery217 have been reported.
-
(b)
Duplication and fenestration. Duplication218 or fenestration of the vertebral artery is found in ≤1% of dissections.113
-
(a)
8.2 V2 Segment
The V2 segment (foramenal segment) travels in a vertical direction within the foramen transversaria, usually from C6 to C2. It is surrounded by sympathetic fibers (although this is now debatable)219 from the stellate ganglion and by a venous plexus that covers the entire V2 segment and drains through the vertebral vein into the subclavian or internal jugular veins.220 The vertebral vein (or veins) is usually large and is directly anterior to the vertebral artery.221
-
1.
Branches
-
(a)
Spinal branches. These branches (aka radiculomedullary branches) arise from the vertebral artery from C1 to C5 and may vary in the number and side of origin.220,221 They supply the spinal cord as well as the periosteum and bone of the vertebrae.
-
(b)
Muscular branches. Multiple small muscular branches arise from the V2 segment to supply the cervical muscles.
Artery of the cervical enlargement. The artery of the cervical enlargement usually arises from both vertebral arteries in the region of C4 to C6 and anastomoses with the anterior spinal artery to supply the ventral spinal cord. This artery may also arise from the thyrocervical trunk (see General Principles of Spinal Arterial Anatomy, below).6
-
(c)
Anterior meningeal artery. Originates from the distal V2 segment and supplies the dura around the foramen magnum and extends up the clivus. Forms collaterals with the ascending pharyngeal artery via the odontoid arcade and the dural branches of the ascending pharyngeal artery, and with the ICA via the meningohypophyseal trunk branches.
-
(d)
Posterior meningeal artery. Arises near the foramen magnum and supplies the medial occipital dura and the falx cerebelli (Fig. 1.45).
Fig. 1.45 
Posterior meningeal artery. Posterior meningeal artery (arrows) arises from the vertebral artery at C1 and supplies the falx cerebelli. The posterior meningeal artery in this particular case is enlarged due to the presence of a dural arteriovenous fistula
-
(e)
PICA. Occasionally the PICA originates at the C1 level.222
-
(a)

8.3 V3 Segment
The V3 segment (aka extraspinal segment) begins as the vertebral artery exits the transverse foramen of C1 on the medial side of the lateral rectus muscle of the head. It then travels in a horizontal and medial direction superior to the posterior arch of C1 and runs inferior to the posterior atlanto-occipital membrane before turning superiorly and anteriorly to penetrate the dura.
-
1.
Branches
-
(a)
PICA. In some 5–20% of cases, the PICA has an extradural origin, usually from the V3 segment.222 In these cases the PICA may originate at any point along the V3 segment.
-
(b)
Suboccipital artery of Salmon. One, or up to three muscular branches supplying the suboccipital muscles is seen in 67% of cases.223
-
(a)
8.4 V4 Segment
The V4 segment is the intradural part of the vertebral artery and extends from its entrance through the dura to the junction with the opposite vertebral artery. The dura is thickened and it forms a fibrous dural ring around the vertebral artery.224 The length of the V4 segment averages 22 mm.225 The left and right V4 segments usually come together at the level of the pontomedullary junction. The branches of the intradural vertebral artery can be separated into medial branches (including the anterior spinal artery and branches of the foramen caecum) and lateral branches, the most prominent of which is the PICA.225 A wide anastomotic net usually interconnects the branches of V4.225
-
1.
Branches
-
(a)
Posterior inferior cerebellar artery (PICA). The PICA is the largest and most complex of the cerebellar arteries (Fig. 1.46). It originates approximately 16–17 mm proximal to the vertebrobasilar junction, an average of 8.6 mm superior to the foramen magnum.226 The territory supplied by the PICA includes the lower medulla and inferior aspects of the fourth ventricle, cerebellar tonsils, vermis, and inferolateral cerebellar hemisphere. The PICA arises from the vertebral artery and travels posterolaterally around the medulla. Over the dorsal aspect of the brainstem, the vessel travels inferiorly for a variable distance – sometimes as far south as C2 – then forms a loop (the caudal loop) and turns 180° to travel superiorly adjacent to the cerebellar tonsil. The vessel then reaches its superior extent and forms another loop (the cranial loop) and then travels inferiorly and laterally to emerge over the cerebellar hemisphere (Fig. 1.47). The PICA can be divided into five segments, detailed below. The first four segments can be remembered by using the acronym, ALPS.
Fig. 1.46 
Posterior inferior cerebellar artery. Lateral view of the brainstem and cerebellum. The segments of the PICA include the anterior medullary (A), lateral medullary (L), posterior medullary (P), supratonsillar (S), and cortical (C) segments. Arrow indicates the choroidal point. The artist was inspired to depict the Swiss Alps in the background
Fig. 1.47 
The choroidal point. The single most important anatomical fact about the PICA for neurointerventionalists has to do with the cranial loop (arrow), aka the choroidal point. The choroidal point is the superior-most point of the PICA. The PICA gives off branches to the brainstem proximal to the choroidal point but not distal to it. Occlusion of the PICA at or distal to the choroidal point does not usually result in a functionally significant ischemic injury, because of anastomotic connections with AICA and SCA292,293
-
i.
Anterior medullary segment. Extends from the origin to the inferior olivary prominence. In some 40% of cases, there is no anterior medullary segment, because the PICA arises lateral, rather than anterior to the medulla.226 This segment averages one perforator.226
-
ii.
Lateral medullary segment. Extends from the inferior olivary prominence to the origins of the ninth, tenth, and eleventh cranial nerves, and averages 1.8 perforators.226
-
iii.
Posterior medullary segment. This segment (aka tonsillomedullary segment) begins where the PICA passes posterior to the lower cranial nerves and ends where the ascending vessel reaches the midlevel of the medial surface of the tonsil. It passes immediately posterior to the roof of the lower half of the fourth ventricle, and averages 3.3 perforators.226
-
iv.
Supratonsillar segment. This segment, the telovelotonsillar segment, begins midway up the tonsil, includes the cranial loop, and ends where the PICA exits the fissures between the vermis, tonsil, and cerebellar hemisphere to reach the cortical surface. On a lateral angiogram, the supratonsillar segment outlines the tonsil along its anterior, superior, and posterior aspects.6
-
v.
Cortical segments. These segments are also known as hemispheric branches. The PICA often bifurcates into medial and lateral trunks where the vessel emerges onto the inferior cortical surface. The medial trunk gives rise to the vermian and tonsillar branches, and the lateral trunk produces the hemispheric branches.
-
vi.
PICA branches
-
1.
Perforators
-
(a)
Direct perforators. These branches travel directly into the brainstem, and are found in all three medullary segments.
-
(b)
Circumflex perforators. These perforators travel around the brainstem for some distance before entering it. These vessels arise mostly from the lateral and posterior medullary segments.
-
(a)
-
2.
Choroidal arteries. Branches to the choroid plexus of the fourth ventricle arise from the posterior and supratonsillar segments.
-
3.
Cortical arteries
-
(a)
Vermian branches
-
(b)
Tonsillar branches
-
(c)
Hemispheric branches
-
(a)
-
4.
Meningeal branches. The posterior meningeal artery and the artery of the falx cerebelli may arise from the PICA.
-
1.
-
vii.
PICA variants
-
1.
Anomalous origin. Extradural origin of the PICA is found in 5–20% of cases (see above). Origination of the PICA from the ICA,227 the posterior meningeal artery,228 a hypoglossal artery,229 and a proatlantal artery229 have been reported.
-
2.
Duplication. The PICA is duplicated in some 2.5–6% of cases.226
-
3.
Hypoplasia. The PICA is hypoplastic in 5–16% of the hemispheres.229,230
-
4.
Absence. The PICA is absent on one side in 15–26% of cases and on both sides in 2% of cases.3,229,230
-
5.
A shared AICA-PICA trunk is a normal variant.1
-
6.
The vertebral artery terminates in PICA in 0.2% of cases.1
-
1.
-
i.
-
(b)
Perforators. An average of 4.2 perforators arise directly from each vertebral artery and supply lateral medulla, inferior cerebellar peduncle, and the medullary surface of the cerebellum.225
-
(c)
Anterior spinal artery. The anterior spinal artery arises from the vertebral artery 6.5 mm proximal to the vertebrobasilar junction225 and travels in an inferior direction to supply the anterior surface of the medulla and spinal cord. In about 50% of cases a small communicating artery (the anterior spinal communicating artery) connects the left and right anterior spinal arteries on the anterior surface of the medulla.225
-
(d)
Branches of the foramen caecum. In about one third of cases branches of the vertebral artery travel superiorly to supply the foramen caecum at the base of the pons.225
-
(e)
Lateral spinal artery. The lateral spinal artery may arise from the V4 segment or from the PICA,231 and may be difficult to see on angiography.6 It originates lateral to the medulla and travels in a caudal direction, anterior to the posterior spinal nerve roots and posterior to the dentate ligament. It supplies the eleventh cranial nerve and the lateral and posterior surfaces of the cord via branches to the C1–C4 spinal nerves.
-
(f)
Meningeal branches. The posterior meningeal artery and the artery of the falx cerebelli may arise from the PICA.
-
(a)


9 Basilar Artery
The basilar artery originates at the pontomedullary junction, travels anterior to the pons, and terminates near pontomesencephalic junction. The artery averages 32 mm in length130 and travels in the midline, or at least medial to the lateral margins of the clivus, in 98% of cases.232 The course of the artery is straight in 45% of cases, curved in 35%, and tortuous in 20%.233 The outer diameter is typically constant, averaging 4.1 mm in adults,234 except for a widening at the basilar bifurcation, giving it a “cobra-like appearance,” in 16% of cases.130
-
1.
Branches
-
(a)
Anterior inferior cerebellar artery (AICA). The AICA arises from the basilar artery an average of 9.6 mm distal to the vertebrobasilar junction.233 It travels in a posterior, inferior and lateral direction across the pons toward the cerebellopontine angle. It terminates by passing over and sending branches to the anterolateral surface of the cerebellar hemisphere.235 Usually the smallest of the three cerebellar arteries, the AICA has reciprocal relationships and extensive anastomoses with the SCA and the PICA. It also has anastomoses with the SCA. The sixth cranial nerve crosses the AICA 6–7 mm distal to the origin of the artery,234 and the vessel lies adjacent to the seventh and eighth cranial nerves in the cerebellopontine angle.236 The AICA has three segments:
-
i.
Premeatal segment. Extends from the origin of the vessel to the seventh and eighth cranial nerves.
-
ii.
Meatal segment. The part of the AICA that is related to the internal auditory canal.
-
iii.
Postmeatal segments. The AICA typically divides into rostral and caudal trunks in the cerebellopontine angle.237,238 After crossing the seventh and eighth cranial nerves, the rostral trunk travels laterally over the flocculus to reach the middle cerebellar peduncle and the superior part of the anterolateral (petrosal) surface of the cerebellar hemisphere. The caudal trunk supplies the inferior part of the anterolateral surface.
-
iv.
AICA branches
-
1.
Perforators. The brainstem receives small perforating branches from the premeatal segment and recurrent perforating branches from the meatal segment.
-
2.
Internal auditory artery (labyrinthine artery). This vessel arises from the AICA in 45% of cases.1 The vessel may arise from the premeatal or meatal segment, or from the lateral branch of the postmeatal segment. The internal auditory artery travels with the seventh and eighth cranial nerves into the internal auditory meatus and is distributed to the inner ear.239
-
3.
Subarcuate artery. The subarcuate artery arises from the AICA medial to the internal auditory meatus and penetrates the dura covering the subarcuate fossa on the posterior surface of the temporal bone and supplies the bone in the region of the semicircular canals.240
-
4.
Cerebellar cortical branches.
-
1.
-
v.
AICA variants
-
i.
-
(b)
Basilar artery perforators. An average of 17 perforators arises from the basilar artery from its origin to the SCAs.233 In addition, on average, another 2.5 average small horizontal brainstem perforators arise from the posterior surface of the basilar artery distal to the origin of the SCAs.242 Significantly, no perforators arise directly from the tip of the basilar artery.242,243 Basilar perforators supply the posterior perforated substance and brainstem structures such as the corticospinal and corticobulbar tracts, pontine nuclei, and the lemnisci, fasciculi, and motor nuclei of the midbrain and pons.
-
i.
Medial perforators. Medial perforators average 5.8 mm in length and enter the pons in the basilar suclus or within a few mm of it.233
-
ii.
Circumflex perforators. Circumflex perforators average 16 mm in length and travel around the brainstem for various distances before entering.
-
i.
-
(c)
Superior cerebellar artery (SCA). The SCA is the most constant cerebellar artery and arises from the basilar artery immediately prior to the basilar bifurcation. The SCA travels posterolaterally around the brainstem, inferior to the third and fourth cranial nerves and superior to the fifth cranial nerve. The SCA comes into contact with the fifth cranial nerve in 50% of cases,244 and is usually the target of surgical microvascular decompression for trigeminal neuralgia (the AICA and adjacent veins may also come into contact with the fifth nerve). At an average distance of 18.5 mm from the origin, the SCA bifurcates into a rostral and a caudal trunk.245 The rostral trunk continues around the brainstem, gives off direct and circumflex perforators, sends branches to the inferior colliculi, and supplies the superior surface of the vermis and the paramedian aspect of the cerebellar hemisphere. The caudal trunk supplies the superior lateral surface of the cerebellar hemisphere, the superior cerebellar peduncle and dentate nucleus, and part of the brachium pontis. The SCA can be divided into four segments:245
-
i.
Anterior pontomesencephalic segment. This segment (aka anterior pontine segment) extends from the SCA origin to the anterolateral margin of the brainstem.
-
ii.
Lateral pontomesencephalic segment. This segment (aka ambient segment) extends from the anterolateral margin of the brainstem to the anterior margin of the cerebellomesencephalic groove. This segment is parallel to the PCA and basal vein of Rosenthal. The fourth cranial nerve crosses the midportion of this segment.
-
iii.
Cerebellomesencephalic segment. This segment (aka quadrigeminal segment) travels within a groove between the cerebellum, the midbrain, and the superior cerebellar peduncles.
-
iv.
Cortical segments. The cortical segments include branches to the vermis and superior cerebellar hemisphere cortical surface.
-
v.
SCA branches
-
1.
Perforators. An average of two perforators arises from the main SCA trunk, five from the rostral trunk, and two from the caudal trunk.245 Direct perforators from the SCA are less common than circumflex perforators.
-
2.
Precerebellar arteries. The precerebellar arteries arise from the hemispheric branches (average: four) and the vermian branches (average: two), and supply the deep cerebellar nuclei, the inferior colliculi, and the superior medullary velum.245
-
3.
Cortical arteries.
-
(a)
Hemispheric branches
-
(b)
Vermian branches
-
(c)
Marginal artery
-
(a)
-
4.
Internal auditory artery. This vessel is most often a branch of the AICA (see above) but arises from the SCA in 25% of cases.1
-
1.
-
vi.
SCA variants
-
i.
-
(d)
Internal auditory artery. This vessel is most often a branch of the AICA (see above) but arises directly from the basilar artery in 16% of cases.1
-
(a)
-
2.
Variants
-
(a)
Fenestration of the basilar artery is found in 1.33% of dissection and 0.12% of angiograms.1,247
-
i.
Fenestration or segmental duplication is a rare congenital anomaly. In a review of 5,190 cerebral- angiograms, arterial fenestration was observed in 37 (0.7%).248 Considering all fenestrations, the prevalence of an associated aneurysm is 7%.248 Table 1.7 is an inventory of reported intracranial fenestrations.
Table 1.7 Intracranial arterial fenestrations
-
i.
-
(a)
10 Venous System
The most important facts about the craniocervical venous system are:
-
1.
Venous anatomy is highly variable.
-
2.
The venous structures of the head and neck are widely interconnected.
-
3.
Valves are not present in the intracranial venous system.
-
4.
Valves are typically present at several predictable locations in the cervical region.
Two other useful generalizations can be made:
-
1.
Many veins have reciprocal relationships with other veins. For instance, if the vein of Labbé is large, the vein of Trolard is usually small.
-
2.
In addition to anatomical variation, the size and flow direction of any given vein can vary greatly with the patient’s head and neck position and in the presence of pathology.
As the venous system is so variable, the following discussion details the most common venous anatomic patterns and selected clinically relevant variants. An exhaustive inventory of known variations would be mind-numbingly tedious to read and not particularly useful.
10.1 Extracranial Veins
10.1.1 Scalp Veins
The scalp veins have extensive connections with the emissary veins of the skull, although these connections are not normally seen on angiography.
-
1.
Frontal vein. Drains the anterior part of the skull and forehead and communicates with the supratrochlear and supraorbital veins.
-
2.
Supratrochlear vein. Drains the frontal scalp and forehead and descends over the forehead medial to the supraorbital vein.
-
3.
Supraorbital vein. Drains the frontal scalp and forehead and travels over the superior orbital rim lateral to the supratrochlear vein to anastomose with the orbital veins and the angular vein.
-
4.
Medial temporal vein. Drains the anterior temporal region and joins the superficial temporal vein.
-
5.
Superficial temporal vein. Usually runs together with the corresponding superficial temporal artery. It descends in front of the ear and penetrates the parotid glands, where it is joined by the maxillary vein to form the retromandibular vein, which drains into the internal jugular (IJ) or external jugular (EJ) vein.
-
6.
Posterior auricular vein. Drains the retroauricular area and connects to the IJ or EJ.
-
7.
Occipital vein. Drains the occipital and posterior cervical areas and anastomoses with the deep cervical and vertebral veins and the transverse sinus via the mastoid emissary vein. It drains into the IJ or EJ (Fig. 1.48).
Fig. 1.48 
Superficial extracranial veins. (1) frontal vein; (2) supratrochlear vein; (3) supraorbital vein; (4) medial temporal vein; (5) superficial temporal vein; (6) posterior auricular vein; (7) occipital vein; (8) angular vein; (9) facial vein; (10) labial veins; (11) submental vein; (12) retromandibular vein; (13) thyroid veins; (14) internal jugular vein; (15) external jugular vein

10.1.2 Orbital Veins
The orbital veins comprise an important anastomoses between the intracranial and extracranial venous systems, and are typically enlarged in the presence of a carotid-cavernous fistula.
-
1.
Superior ophthalmic vein (SOV). The largest and the most constant orbital vein.249 It originates near the trochlea below the medial orbital roof and travels posteriorly and medially to enter the cavernous sinus. The common direction of flow in the ophthalmic veins is from extracranial to intracranial;250 reversal of flow in the SOV should raise suspicion of intracranial venous hypertension. The SOV anastomoses with the supraorbital vein and the angular vein.
-
2.
Inferior ophthalmic vein. Much smaller than the SOV, it is connected to the SOV via several anastomotic vessels (anterior, medial, and posterior anastomosing veins), and drains into the cavernous sinus or directly into the superior ophthalmic vein.
-
3.
Medial ophthalmic vein. Present in some cases.
10.1.3 Facial Veins (Figs. 1.48 and 1.49)

Deep extracranial veins. (1) superior orbital vein; (2) inferior orbital vein; (3) angular vein; (4) facial vein; (5) pterygoid plexus; (6) deep facial veins; (7) maxillary vein; (8) common facial vein; (9) suboccipital veins; (10) pharyngeal vein
-
1.
Angular vein. The angular vein is formed by the junction of the supratrochlear and supraorbital veins. It travels in an inferior direction at an angle next to the nose (thus the name) and medial to the orbit. The angular vein communicates with orbital veins and continues inferiorly as the facial vein.
-
2.
Facial vein. The facial vein (aka anterior facial vein) is the continuation of the angular vein, and it begins at the medial palpebral angle. The facial vein descends obliquely across the face and curves around the inferior edge of the mandible to merge with the submental and retromandibular veins to drain into the IJ. Along its course, the facial vein receives tributaries from the orbit, facial muscles, and submental region.1 It has extensive connections with deep facial vein, pterygoid plexus, and cavernous sinus.250
-
3.
Pterygoid plexus. The pterygoid plexus is a network of venous channels that is nestled between the temporalis and lateral pterygoid muscles. It is connected to the facial vein via the deep facial vein, and it receives a wide array of tributaries from deep facial and oropharyngeal structures. It connects to the cavernous sinus via emissary veins that travel through the foramen ovale and spinosum, and to the IJ via the maxillary vein.
-
4.
Deep facial vein. Connection between the facial vein and the pterygoid plexus.
-
5.
Maxillary vein. This vein connects to the pterygoid plexus and travels posteriorly to join the superficial temporal vein to form the retromandibular vein.
-
6.
Labial veins. The superior and inferior labial veins drain the upper and lower lips, respectively, and drain into the facial vein.
-
7.
Retromandibular vein. This vein (aka temporo-maxillary vein) is formed by the confluence of the maxillary and superficial temporal veins, and passes within the parotid gland to join the facial vein.
-
8.
Common facial vein. Formed by the junction of the facial, lingual anterior division of the retromandibular and communicating veins. It receives submental, lingual and thyroid tributaries, and drains into the IJ.1
-
9.
Submental vein. Drains the floor of the mouth and runs under the mandible. It drains into the facial vein.
10.1.4 Cervical Veins
-
1.
Internal jugular vein (IJ). The IJ begins in the jugular fossa and is the continuation of the sigmoid sinus. The jugular bulb is the enlargement of the IJ at its origin. The IJ travels within the carotid sheath posterior and lateral to the common carotid artery, and connects with the subclavian vein on each side to form the branchiocephalic vein. A valve is usually present where the IJ meets the subclavian vein. The right IJ is usually dominant.
-
2.
External jugular vein (EJ). The EJ is formed by the junction of the posterior division of the retromandibular and posterior auricular veins. It originates inferior to the angle of the mandible and travels across the sternocleidomastoid muscle to drain into the subclavian vein. A valve may be present where the EJ meets the subclavian vein.
-
3.
Suboccipital veins. These veins drain the suboccipital region and communicate with the vertebral venous plexus.
-
4.
Thyroid veins. Superior and inferior thyroid veins drain the thyroid gland and connect to IJ.
-
5.
Pharyngeal vein. Drains the posterior pharyngeal region and connects to the IJ.
-
6.
Anterior condylar confluence (of Trolard). Present in essentially 100% of cases, it is possibly the dominant outflow of the venous drainage of the brain in the upright position.101 It lies adjacent to the hypoglossal canal and connects the jugular bulb to the anterior, posterior, and lateral condylar veins.
-
7.
Anterior condylar vein. The anterior condylar vein travels through the hypoglossal canal and connects the inferior petrosal sinus with the vertebral venous plexus and suboccipital veins. It is the rostral equivalent of a spinal radicular vein.251
-
8.
Posterior condylar vein (aka condylar emissary vein). Connection between the sigmoid sinus and vertebral venous plexus.1
-
9.
Lateral condylar vein. Also drains to the vertebral venous plexus. Seen on 76% of sides of cadaveric specimens.101
-
10.
Spinal radicular veins. Each spinal radicular vein corresponds to a spinal artery. These veins travel within the neural foramena and connect the epidural venous plexus to the vertebral venous plexus.
-
11.
Vertebral venous plexus. The vertebral venous plexus begins in the suboccipital region and extends inferiorly along the vertebral column to drain into the brachiocephalic vein. It surrounds the V2 segment of the vertebral artery and has numerous connections with the occipital veins, epidural venous plexus, and other cervical and facial veins.
-
12.
Vertebral vein. The vertebral vein (aka anterior vertebral vein)252 is anterior to the vertebral artery221 and drains into the vertebral venous plexus.
10.2 Venous Structures of the Skull
A rich network of veins connects the intracranial venous system to the extracranial venous system.
-
1.
Diploic veins. The cancellous bone between the inner and outer tables of the skull contains an extensive network of veins that do not cross suture lines and are not normally seen on angiography.6 They communicate widely with meningeal and pericranial veins, and with the dural sinuses.
-
2.
Emissary veins. These veins connect the extracranial veins to the intracranial venous sinuses.
-
(a)
Parietal emissary veins. Communicate between the scalp veins and the superior sagittal sinus.
-
(b)
Mastoid emissary veins. Communicate between the occipital and posterior auricular veins and the sigmoid sinus.
-
(a)
10.3 Meningeal Veins
Meningeal veins lie on the outer surface of the dura and each corresponds to its respective meningeal artery.6 The anterior meningeal vein joins the superficial Sylvian vein to form the sphenoparietal sinus.
10.4 Intracranial Venous Sinuses
The dural sinuses are venous channels that are located between the meningeal and endosteal layers of dura. They are rigid and do not have valves. They may be trabeculated and contain bands, chords, and bridges.126 They also contain arachnoid granulations; Pacchionian granulations are macroscopic arachnoid granulations that project directly into the venous sinuses. Pacchionian granulations may measure up to 1 cm in diameter253 and should not be mistaken on angiography for intraluminal thrombus (Fig. 1.50). Dural sinuses are also present within the falx cerebri and tentorium. There are two main groups of dural venous sinuses: the superior group and the inferior group.253

Arachnoid granulation. Venogram of the inferior venous sinuses, showing an arachnoid granulation in the transverse sinus (arrow). Arachnoid granulations can have a “punched out” appearance on angiography that can mimic a flow void due to intraluminal thrombus
10.4.1 Superior Group
The superior group primarily drains the majority of the brain and skull (Fig. 1.51).

Superior group of dural venous sinuses. (1) Superior sagittal sinus; (2) inferior sagittal sinus; (3) straight sinus; (4) occipital sinus; (5) transverse sinus; (6) sigmoid sinus
-
1.
Superior sagittal sinus (SSS). The SSS lies in a shallow midsagittal groove at the junction of the falx cerebri and the dura lining the inner table of the calvaria. It originates near the crista galli and terminates in the torcular Herophili. The transverse diameter of the SSS ranges from 4 mm in the frontal area to 10 mm in the occipital region.126 The “1/3rd Rule” states that it is generally safe to therapeutically occlude the SSS in the anterior third of the structure, without a significant risk of venous infarction.254 Cortical venous tributaries are most prominent in the middle third of the SSS, and relatively few in number and caliber in the posterior third.
-
(a)
Venous connections
-
i.
Facial and nasal veins: Although there have been denials of its existence,255,256 there can be a vein of the foramen caecum draining the nasal veins to the superior sagittal sinus, more commonly seen in infants257
-
ii.
Scalp veins
-
iii.
Cortical veins
-
iv.
“Intermediate veins”:253 Diploic, meningeal, and emissary veins. These structures provide important collateral pathways in the event of venous sinus occlusion
-
i.
-
(a)
-
2.
Inferior sagittal sinus. The inferior sagittal sinus is relatively small and travels in or slightly superior to the falx. It begins at the junction of the anterior and middle thirds of the falx, runs above the corpus callosum, and terminates at the falcotentorial apex by connecting with the vein of Galen to form the straight sinus. It is more prominent in infants and young children, than adults.253
-
(a)
Venous connections
-
i.
Tributaries from the falx, corpus callosum, medial cerebral hemispheres, and SSS via falcine veins.
-
i.
-
(a)
-
3.
Straight sinus. The straight sinus is formed by the confluence of the inferior sagittal sinus and vein of Galen. It travels posteriorly and inferiorly beneath the splenium of the corpus callosum toward the internal occipital protuberance. The straight sinus averages 5 cm in length258 and drains into the confluence of the sinuses, or predominantly into one transverse sinus, usually the left.253 The straight sinus is single channel in most cases, but is doubled or tripled in some 15% of cases.259
-
(a)
Venous connections
-
i.
Vermian veins
-
ii.
Tentorial sinuses
-
iii.
Cerebellar hemispheric veins
-
i.
-
(a)
-
4.
Occipital sinus. The occipital sinus is present in 65% of cases, and travels in the midline, within the attached margin of the falx cerebelli, between the confluence of the sinuses and the marginal sinus.260
-
5.
Torcular Herophili. The confluence of the sinuses (Fig. 1.52) is formed by the junction of the SSS, straight sinus, transverse sinuses, and occipital sinus. The torcular Herophili is typically asymmetric and widely variable in its configuration. In 10–15% of cases, the superior sagittal sinus drains into one transverse sinus and there is no direct connection between the left and right transverse sinuses.261
Fig. 1.52 
Torcular herophili. The confluence of the sinuses carries the eponym, Torcular Herophili, after the anatomist, Herophilus of Chalcedon. The term “torcular” is commonly thought to be translated from the ancient Greek as “wine press,” as the four-limbed confluence (left) bears some resemblance to a wine press (right)294. An alternative school of thought holds that this is a mistranslation, and that Torcular Herophili actually refers to the concavity on the interior of the occipital bone that houses the confluence295
-
6.
Transverse sinus. The transverse sinuses (aka lateral sinus) travel within the peripheral margins of the tentorium and extend from the internal occipital protuberances to the bases of the petrous temporal bones. The right and left transverse sinuses are asymmetric in about half of cases, and the right transverse sinus is usually larger.261 In some 20% of cases, there is partial or total agenesis of one of the transverse sinuses, usually the left, and in these cases the sigmoid sinus may fill via the vein of Labbé.261
-
(a)
Venous connections
-
i.
SSS and contralateral transverse sinus
-
ii.
Veins from the inferior and lateral surfaces of the temporal and occipital lobes, including the vein of Labbé.
-
iii.
Cerebellar veins.
-
iv.
Veins of the scalp via mastoid emissary veins.
-
v.
Superior petrosal sinus
-
i.
-
(a)
-
7.
Sigmoid sinus. The sigmoid sinus originates where the transverse sinus leaves the tentorial margin. It forms a gentle S-shape and terminates at jugular bulb, where the internal jugular vein begins.
-
(a)
Venous connections
-
i.
Transverse sinus and internal jugular vein.
-
ii.
Suboccipital muscular and scalp veins and the vertebral venous plexus via the mastoid and condylar emissary veins.
-
i.
-
(a)

10.4.2 Inferior Group
The inferior group primarily drains the sylvian veins, the inferior surface of the brain, and the orbits (Fig. 1.53).

Inferior group of dural venous sinuses. (1) Cavernous sinus. (2) Superior petrosal sinus. (3) Inferior petrosal sinus. (4) Basilar venous plexus. (5) Sphenoparietal sinus. (6) Marginal sinus
-
1.
Cavernous sinus. Each cavernous sinus lies lateral to the body of the sphenoid bone and extends from the superior orbital fissure to the petrous apex. The anterior and posterior part of the cavernous sinuses are connected to each other via the intercavernous sinus (aka “circular sinus”) around the sella turcica and the basilar venous plexus. This consists of an anterior intercavernous sinus in front of the sella, a posterior intercavernous sinus behind the sella, and in some cases an inferior intercavernous sinus as well.262 Cranial nerves III, IV, V1, and V2 travel in the lateral wall of the cavernous sinus, and the ICA, sympathetic plexus, and cranial nerve VI are suspended by fibrous trabeculae within the lumen of the cavernous sinus.253
-
(a)
Venous connections
-
i.
Superior and inferior ophthalmic veins
-
ii.
Sphenoparietal sinus
-
iii.
Superior petrosal vein
-
iv.
Inferior petrosal sinus
-
v.
Pterygoid plexus via emissary veins of the foramen ovale, foramen lacerum, and foramen Vesalius.
-
i.
-
(a)
-
2.
Inferior petrosal sinus. The inferior petrosal sinus travels in groove between the petrous apex and the clivus (Dorello’s canal), extending from the posterior part of the cavernous sinus to the anterior superior aspect of the jugular bulb. In 39% of cases the left and right inferior petrosal sinuses are markedly asymmetric, and in 8% of cases the sinus is absent on at least one side.263
-
(a)
Venous connections
-
i.
Cavernous sinus
-
ii.
Basilar venous plexus
-
iii.
Internal auditory veins
-
iv.
Cerebellar and brainstem veins
-
v.
Internal jugular vein
-
i.
-
(a)
-
3.
Superior petrosal sinus. The superior petrosal sinus extends from the transverse sinus to the cavernous sinus, and travels along the attachment of the tentorium to the superior margin of the petrous temporal bone. The direction of flow is presumably from posterior to anterior.264
-
(a)
Venous connections
-
i.
Transverse sinus
-
ii.
Petrosal vein
-
iii.
Lateral mesencephalic vein
-
iv.
Cerebellar veins
-
v.
Veins draining the tympanic cavity
-
vi.
Cavernous sinus
-
i.
-
(a)
-
4.
Sphenoparietal sinus. The sphenoparietal sinus (aka sinus of Breschet) is the medial extension of the Sylvian veins.253 It travels beneath the lesser wing of the sphenoid bone and drains into the cavernous sinus, pterygoid plexus, or into the inferior petrosal sinus or transverse sinus.264 A “true” sphenoparietal sinus exists when the structure anastomoses with other venous structures at both ends.249
-
5.
Basilar venous plexus. The basilar venous plexus (aka clival venous plexus) is a network of dural veins that extends over the dorsal surface of the clivus.
-
(a)
Venous connections
-
i.
Cavernous sinus
-
ii.
Inferior petrosal sinus
-
iii.
Marginal sinus
-
i.
-
(a)
-
6.
Marginal sinus. The marginal sinus lies in the margin of the foramen magnum and drains into the jugular bulbs. It anastomoses with the occipital sinus and vertebral venous plexuses.
-
7.
Vertebral venous plexus. The venous plexus is the extensive network of veins associated with the spine. It can be subdivided into internal and external components.
10.5 Supratentorial Cortical Veins
The cortical veins drain the outer 1–2 cm of the cortex and the subcortical white matter, and travel centrifugally (Fig. 1.54). They have no valves. They exhibit reciprocal prominence, i.e., when one vein is large on a given side, others are usually small.253 Cerebral cortical drainage occurs via three principle routes:

Superficial cortical veins. (1) Sylvian vein; (2) vein of Labbé; (3) superior convexity veins; (4) vein of Trolard
-
3.
Sylvian veins. The Sylvian veins (aka superficial middle cerebral veins) originate in the posterior third of the lateral Sylvian fissure and travel through the lateral aspect of the sylvian fissure and drain parts of the frontal and temporal lobes into the cavernous sinus and pterygoid plexus.253,265
-
4.
Temporo-occipital veins. These veins drain temporal, occipital and parts of the parietal cortex into the transverse sinus.
-
(a)
Vein of Labbé (aka occipito-temporal vein) is defined as the largest cortical vein crossing the temporal lobe convexity from the Sylvian vein to the transverse sinus.6 It can be identified on one or both hemispheres in 75% of dissections,266 and is most commonly larger in the dominant hemisphere.267 It travels in the occipitotemporal sulcus and may have important anastomotic connections with tentorial dural sinuses.
-
(a)
-
5.
Superior convexity veins. These veins, which average 14 per hemisphere,126 drain the superolateral and superomedial cortex into the superior sagittal sinus. The veins enter the superior sagittal sinus perpendicularly in the anterior frontal region; the angle becomes progressively more acute (i.e., opposite to the direction of flow in the superior sagittal sinus) in the parietal and occipital regions. Occipital region veins may pass for a considerable distance before connecting to the superior sagittal sinus, and may be confused with venous anomalies.253 The vein of Rolando travels in the central sulcus.
10.6 Deep Venous System
The deep venous system drains the periventricular white matter, basal ganglia, and thalamic regions (Fig. 1.55). In contrast to the cortical venous system, which runs centrifugally, the deep venous system runs centripetally. The deep veins can be divided into a ventricular group (which includes the subependymal veins and internal cerebral vein) and a cisternal group (primarily consisting of the basal vein of Rosenthal and its tributaries).

Deep venous system. (1) Medullary veins; (2) subependymal veins; (3) septal vein; (4) anterior caudate vein; (5) thalamostriate vein; (6) internal cerebral vein; (7) basal vein of Rosenthal; (8) vein of Galen (aka great cerebral vein)
-
1.
Medullary veins. The medullary veins are an array of veins that drain the cerebral white matter. They originate 1–2-cm deep to the cortical mantle and join the subependymal veins. They are typically straight and perpendicular to the subependymal veins.
-
2.
Subependymal veins
-
(a)
Septal veins. The septal veins originate at the lateral aspect of the frontal horns and travel posteriorly and medially to run along the septum pelucidum. In the majority of cases, the septal veins join the thalamostriate veins to form the internal cerebral vein. The venous angle is the junction of the septal vein with the thalamostriate vein. Although the venous angle is generally considered to approximate the location of the foramen of Monro on angiography, in 47.5% of hemispheres the septal vein joins the internal cerebral vein an average of 6 mm posterior to the foramen of Monro.268 The septal veins drain the deep frontal white matter and anterior corpus callosum.
-
(b)
Anterior caudate veins. The anterior caudate veins (aka longitudinal caudate veins or anteroinferior caudate veins) are a group of tributaries from the medial surface of the caudate nucleus that drain into the thalamostriate vein.
-
(c)
Thalamostriate vein. The thalamostriate vein arises from tributaries that converge on the sulcus between the caudate nucleus and the thalamus, and travels in a medial direction towards the Foramen of Monro to join the septal veins and form the internal cerebral vein. It drains the posterior frontal lobe, anterior parietal lobe, caudate nucleus, and internal capsule. Despite its name, the thalamostriate vein does not receive significant tributaries from the thalamus.
-
(d)
Medial and lateral atrial veins. These veins drain the walls of the atrium, and may drain directly into the internal cerebral vein, basal vein of Rosenthal, or the vein of Galen.269
-
(a)
-
3.
Internal cerebral vein. The internal cerebral vein is formed by the junction of the septal veins and the thalamostriate vein posterior to the foramen of Monro. It travels posteriorly to join the contralateral internal cerebral vein to form the vein of Galen. The internal cerebral vein receives subependymal tributaries and, just anterior to the vein of Galen, the ipsilateral basal vein of Rosenthal. It averages 30.2 mm in length269 and drains the posterior frontal lobe, anterior parietal lobe, caudate nucleus, lentiform nucleus, and internal capsule.
-
4.
Basal vein of Rosenthal. The basal vein of Rosenthal (aka basal vein) is the most prominent cisternal vein and is formed below the anterior perforated substance by the junction of the anterior cerebral and deep middle cerebral veins. The anterior cerebral vein originates near the optic chiasm and is connected to its contralateral counterpart by the anterior communicating vein. The deep middle cerebral vein is formed near the limen insula by the confluence of the insular veins. The basal vein of Rosenthal travels posteriorly between the midbrain and the temporal lobe and terminates by joining the internal cerebral vein or the vein of Galen. It receives extensive tributaries from the temporal lobe, thalamus, and midbrain.
-
5.
Vein of Galen. The vein of Galen (aka great cerebral vein) originates in the quadrigeminal cistern by the union of the internal cerebral veins. It curves in a posterosuperior direction towards the apex of the tentorium, where it joins the straight sinus. It is 5–20 mm in length6 and its tributaries include the posterior pericallosal, superior cerebellar, and precentral cerebellar veins.
10.7 Infratentorial Venous System
The veins of the posterior fossa can be grouped according to the principle route of drainage (Fig. 1.56).

Infratentorial venous system. (1) Vein of Galen; (2) straight sinus; (3) precentral cerebellar vein; (4) superior vermian vein; (5) basal vein of Rosenthal; (6) anterior pontomesencephalic vein; (7) anterior medullary vein; (8) petrosal vein; (9) lateral mesencephalic vein; (10) inferior vermian vein; (11) posterior mesencephalic vein; (12) brachial vein; (13) superior retrotonsillar vein; (14) inferior retrotonsillar vein
-
1.
Superior (vein of Galen) group. These veins drain the upper part of the cerebellar hemispheres, vermis, and midbrain.
-
(a)
Precentral cerebellar vein. The unpaired midline precentral cerebellar vein receives the superior hemispheric and vermian tributaries, and travels superiorly and posteriorly parallel to the roof of the forth ventricle. It enters the vein of Galen posterior to the inferior colliculi.
-
(b)
Superior vermian vein. The paired superior vermian veins originate from tributaries in the culman, posterior to the precentral cerebellar vein. They travel superiorly to drain into the vein of Galen, with or anterior to the precentral cerebellar vein.
-
(c)
Posterior mesencephalic vein. This vein originates in the interpeduncular fossa and curves around the midbrain to enter the vein of Galen or internal cerebral vein.249
-
(a)
-
2.
Anterior (petrosal vein) group. These veins drain the anterior part of the brainstem and cerebellum, and empty primarily into the superior and inferior petrosal sinuses.
-
(a)
Anterior pontomesencephalic vein. The unpaired midline pontomesencephalic vein travels along the anterior belly of the pons, connecting the midline anterior medullary vein inferiorly (which, in turn, connects to the anterior spinal vein) to the peduncular vein, in the interpeduncular cistern. It may also communicate with the petrosal vein and the basal vein of Rosenthal.
-
(b)
Petrosal vein (aka Dandy’s vein). The petrosal vein is formed by numerous tributaries from the pons, medulla, and cerebellum. It is 2–2.5 cm long,249 and travels anterior and lateral to the trigeminal nerve to enter the superior petrosal sinus above the internal auditory meatus.
-
(c)
Lateral mesencephalic vein. This vein runs in the lateral mesencephalic sulcus and anastomoses with the posterior mesencephalic and petrosal veins.
-
(a)
-
3.
Posterior (tentorial) group. These veins drain toward the tentorium.
-
(a)
Inferior vermian veins. The paired inferior vermian veins are formed by the superior and inferior retrotonsillar veins. The inferior vermian veins receive tributaries from the vermis and cerebellar hemispheres, and travel posteriorly and superiorly along the inferior vermis to drain into the tentorial, straight, or transverse sinus.
-
(a)
10.8 Intracranial Venous System Variants
The intracranial venous system is widely variable. Selected variants and anomalies are detailed below:
-
1.
Developmenta venous anomaly (DVA). A DVA (aka venous angioma or cerebral venous malformation) is a normal variant in which a network of small medullary veins converges into single large central venous channel (see also Chap. 16). They are found in some 2% of autopsies.270 They have a characteristic stellate appearance on imaging, and have been hypothesized to occur when medullary veins become hypertrophic to compensate for the occlusion or absence of some other adjacent venous structure. They are frequently found adjacent to cavernous malformations; among patients with cavernous malformations, and up to 29% have an associated developmental venous anomaly.271,272 In fact, focal venous congestion within developmental venous anomalies are thought to contribute to the formation of cavernous malformations.273
-
2.
Vein of Galen malformation. This anomaly consists of a dramatically enlarged persistent median vein of the prosencephalon, which is the embryonic precursor to the vein of Galen (see also Chap. 14).274 Multiple feeding arteries typically flow directly into the varix and usually arise from the anterior and posterior choroidal arteries and the anterior cerebral artery. The malformation develops prior to the formation of the vein of Galen and the straight sinus, and the venous pouch drains via the falcine sinus to the superior sagittal sinus. The straight sinus may be hypoplastic or absent. The deep venous system, as a rule, does not appear to communicate with the malformation, although there is a well-documented case of visualization of a communication to normal deep veins after treatment of a vein of Galen malformation.275
-
3.
Chiari II malformation. In the Chiari II malformation (Fig. 1.57), the posterior fossa is very small and the straight sinus is angled sharply downward. The confluence of sinuses may be at or below the level of the foramen magnum.
Fig. 1.57 
Chiari II malformation. The Chiari II malformation is characterized by an abnormally small posterior fossa, with downward angulation of the straight sinus and low-lying transverse sinuses
-
4.
Dandy–Walker complex. The Dandy-Walker complex is a congenital syndrome that includes cystic dilatation of the forth ventricle and enlargement of the posterior fossa (Fig. 1.58). The straight sinus and torcular Herophili are often elevated and the transverse sinuses angle inferiorly.
Fig. 1.58 
Dandy–walker complex. The tentorium, straight sinus, and torcular Herophili are displaced superiorly by cystic dilatation of the fourth ventricle and enlargement of the posterior fossa


11 Spinal Neurovascular Anatomy
The spine, and in particular, the spinal cord, is supplied by a number of relatively small and variable arteries with similarly small and variable veins. There is a general organization of spinal blood supply that is constant: Segmental arteries contribute to the segmental levels of the spine and may contribute to the extrinsic arteries of the spinal cord, which then contribute to the intrinsic arteries within the substance of the cord. Similarly, the intrinsic veins of the spinal cord drain into the extrinsic veins on the surface of the cord, which then drains to epidural and paraspinal venous structures.
These vessels should be considered when evaluating vascular lesions in the spine (Table 1.8).
11.1 Spinal Cord Blood Supply: General Principles
-
Segmental arteries are the source of blood flow to longitudinal arteries within the spine.
-
Longitudinal intraspinal veins drain via segmental veins into the longitudinal epidural and paraspinal venous systems.
-
Inter-segmental and side-to-side anastamoses are common (Table 1.9).
Table 1.9 Spinal vascular anastomoses -
Variability of segmental connections to longitudinal arterial and venous systems is very common.
11.2 General Principles of Spinal Arterial Anatomy
-
1.
Vertebral artery contributions to the spine (Fig. 1.59)
Fig. 1.59 
Normal spinal arterial anatomy. (a) Anterior view. Radicular artery (1), radiculomedullary artery (2), pial arterial plexus (3), anterior spinal artery (4); (b) Posterior view. Radicular artery (1), radiculopial artery (5), posterolateral arteries (6)
-
(a)
Anterior spinal artery
The anterior spinal artery has two, very short paired branches from the extreme distal vertebral arteries creating a V-like configuration that merges to a single midline artery that descends from the vertebrobasilar junction inferiorly in the ventral sulcus of the cord. Sometimes one limb of the V is hypoplastic and the anterior spinal arises from only one of the distal vertebral arteries.
-
(b)
Posterolateral spinal artery
The posterolateral spinal artery arises from the distal vertebral artery or proximal posterior inferior cerebellar artery (PICA), and travels inferiorly along the posterior cord. There is one on each side. There are two major variants of this artery. Each is associated with variations in the size and course of the distal vertebral artery and level of origin of the PICA.231,276
-
i.
Posterior spinal artery
This artery arises from either the distal extracranial portion of the vertebral or commonly also from the proximal part of an extracranial origin of PICA. Each posterior spinal artery then travels inferiorly along the posterior cord dorsal to the posterior spinal nerve roots.276
-
ii.
Lateral spinal artery
This artery arises from the distal vertebral artery or proximal PICA. However, the lateral spinal artery travels along the posterolateral cord ventral to the posterior roots of C1 through C4.231 The lateral spinal artery joins the ipsilateral posterior spinal artery at the C4 or C5 level.276
-
i.
-
(c)
Segmental branches
These small paired arteries provide muscular and osseous blood flow in the cervical region. They are variable and can supply anterior and posterior radicular branches that follow the spinal nerve roots. These radicular branches can connect to either the anterior spinal artery or to the posterolateral spinal artery to provide segmental input to these longitudinal spinal arteries, usually below C3.277
-
(d)
A particularly large radicular input into the cervical anterior spinal artery is sometimes termed the artery of the cervical enlargement. This artery often is a branch of the vertebral artery, although it may arise from the costocervical trunk (Fig. 1.60) or even directly from the subclavian artery.
Fig. 1.60 
Artery of cervical enlargement. A dominant branch to the cervical portion of the anterior spinal artery often arises from the segmental branches of the vertebral artery, but in this case can be seen to fill on an injection of the costocervical trunk. This is a frontal view with injection into the left thyrocervical trunk Note the hair-pin turn of the vessel as it enters the anterior spinal artery (arrow)
-
(a)
-
2.
Deep cervical artery
The deep cervical artery arises from the costocervical trunk or directly from the second part of the subclavian artery. The left and right deep cervical arteries paired longitudinal arterial systems that are posterior to the transverse processes. They have considerable muscular territories, anastamose with the vertebral arteries, and can provide flow to the radicular arteries along the C7 and C8 roots.277 They variably contribute to the lower cervical cord.
-
3.
Ascending cervical artery
The ascending cervical artery is a branch of the thyrocervical trunk and ascends in the neck anterior to the transverse processes. This artery supplies cervical muscles, anastamoses with the vertebral artery, and can provide radicular branches.
-
4.
Supreme intercostal artery
This artery arises from the costocervical trunk or directly from the subclavian artery and descends to supply several spinal levels, generally providing radicular arteries to the C7 and C8 levels277 and sometimes one or two levels below. Branches contribute to bone, connective tissue and muscle at the cervicothoracic junction usually at T1 and T2 and collateralizing to T3. The supreme intercostal arteries occasionally arise directly from the aorta.7
-
5.
Intercostal (aka posterior intercostal) artery
Usually nine pairs of intercostal arteries arise from the aorta. Occasionally, adjacent intercostal arteries arise as a common trunk. Intercostal arteries provide branches to the spine and paraspinal tissues before traveling laterally under the rib in the costal groove. Adjacent intercostal arteries share numerous collaterals. The intercostal arteries have several branches:7
-
(a)
Dorsal branch
The dorsal branch divides into a spinal branch that supplies bone and dura, which in turn provides a radicular branch that supplies the nerves and possibly the spinal cord. The dorsal branch also has medial and lateral musculocutaneous branches that supply posterior muscles and overlying skin.
-
(b)
Collateral intercostal branch
This branch anastamoses to adjacent intercostal arteries.
-
(c)
Muscular branches
This branch supplies lateral and anterior chest wall muscles and anastamose with lateral thoracic branches of the axillary artery.
-
(d)
Lateral cutaneous
This branch supplies intercostal nerves and lateral chest wall skin.
-
(e)
Multiple small branches to ribs and deep chest wall tissues.
-
(a)
-
6.
Lumbar arteries
Usually four pairs of lumbar arteries arise from the aorta. There are collaterals between ipsilateral lumbar arteries and from side-to-side. The lumbar arteries have branches that are similar to the intercostal arteries:7
-
(a)
Dorsal branch
The dorsal branch gives osseous branches to the vertebral body, and then provides a spinal branch that supplies bone and dura via a post-central branch in the anterior region of the spinal canal, and a prelaminar branch to the posterior region of the canal. In between those two branches, the spinal artery provides a radicular branch to supply the nerves and the spinal cord. The dorsal branch also has medial and lateral musculocutaneous branches that supply the posterior muscles and the overlying skin of the lumbar region.
-
(b)
Collateral lumbar branches
These branches anastamose with adjacent lumbar arteries.
-
(c)
Muscular branches
These branches supply lateral and posterior muscles and anastamose with lower intercostal arteries, adjacent lumbar, iliolumbar, inferior epigastric, and deep circumflex iliac arteries.7
-
(a)
-
7.
Iliolumbar artery
This branch of the posterior division of the internal iliac artery has branches to the psoas muscle, collaterals to the fourth lumbar artery, an L5 radicular artery, and supplies the gluteal and abdominal wall muscles.7
-
8.
Lateral sacral artery
The paired lateral sacral arteries are branches of the internal iliac arteries. They supply upper sacral radicular arteries and can anastamose with median sacral artery branches.
-
9.
Median sacral artery
A single descending median sacral artery arises at the aortic bifurcation and supplies multiple levels of the sacrum. It anastamoses with the lateral sacral and ileolumbar arteries.7 This artery is the remnant of the caudal aorta prior to the development of the limb buds.


11.3 Segmental Contributions to Neural Territories
11.3.1 Radicular Arteries (Anterior and Posterior)
The radicular arteries enter the spine along the spinal nerves and include an anterior radicular artery along the ventral root and a posterior radicular artery along the dorsal root. They may or may not be present at each level and do not necessarily contribute to the spinal cord at every level. In the cervical spine there is an average of 2–3 radicular artery connections to the spinal cord, including 2–3 anteriorly and 1 or 2 posteriorly.277 In the thoracolumbar region, 80% of spinal cord blood flow comes from two radicular contributions.278 Throughout the cord, anterior radicular contributions to the cord number 3–15, and posterior radicular artery contributions number 14–25.279 There are two commonly mentioned types of radicular artery contributions to the spinal cord: the radiculomedullary and radiculopial arteries.
-
1)
Radiculomedullary arteries. These radicular branches connect the anterior radicular artery to the anterior spinal artery.
-
a)
The artery of Adamkiewicz (aka “arteria radicularis magna” or “artery of the lumbar enlargement”) is the dominant radiculomedullary contribution to anterior spinal artery in thoracolumbar spine. It supplies an average of 68% of blood flow to the lower cord, with an average diameter of 0.7 mm.278 It has a classic “hairpin turn” appearance. It travels sharply cephalad from a radicular artery, and then takes a sharp caudal turn as it joins the anterior spinal artery.
-
b)
The origin of the artery of Adamkiewicz is variable. In nearly all cases it arises from the intercostal and lumbar arteries from T8–L2 and is on the left in 80% of cases.33 In 70% of cases the artery of Adamkiewicz arises from a lumbar artery.280 A dominant radiculomedullary artery below L3 was found in only 3 of 4,000 spine angiograms.281 When it arises from above T8 or below L2 there may be a second dominant radiculomedullary contributor above or below.
-
a)
-
2)
Radiculopial arteries. These radicular branches connect the posterior radicular branches to a pial network and the posterolateral spinal arteries.282 In 63% of cases a radiculomedullary feeder also has a posterior radiculopial contribution to posterior spinal artery.95
11.3.2 Strange, but True
Albert Wojciek Adamkiewicz’s study of the vascular anatomy of the spinal cord was the result of his interest in syphilis. He wanted to determine how the bacteria responsible for syphilis made their way to the spinal cord. This originated with his idea that tabes dorsalis was a blood-borne disease.277,283,284 The rest is history.
11.4 Extrinsic Spinal Cord Arteries
These intradural arteries run along the surface of the spinal cord (Fig. 1.59).
-
1)
Anterior spinal artery
-
a)
The anterior spinal artery is a longitudinal artery that originates from the distal vertebral arteries and runs continuously down the cord in the anterior median sulcus with variable contributions from radiculomedullary inputs.280 Occasionally, it may split into two channels, but almost never below C5–6.277
-
a)
-
2)
Posterolateral spinal arteries
-
a)
These paired longitudinal arteries originate from the vertebral arteries proximal to the PICA origins (or from the PICA itself) and run more or less discontinuously along the posterolateral cord, with sporadic contributions from radiculopial arteries. In the cervical region there may be two pairs of longitudinal vessels posteriorly, including the lateral spinal ventral to the dorsal root and posterior spinal dorsal to that dorsal root; these two systems merge at C4 or C5.276 A single pair of posterior longitudinal arteries exist throughout the majority of the extent of the cord.
-
a)
-
3)
Pial network
-
a)
This is a variable network of longitudinal and interconnecting axial vessels, that primarily anastamose to the posterior spinal arteries with only very small connections to anterior spinal artery.279
-
a)
-
4)
Conus basket
-
a)
The anterior spinal artery and posterior spinal arteries join together in a “basket” of arteries around the lower part of the conus medularis.
-
b)
An important arterial source for the conus is the artery of Deproges–Gotteron (aka the cone artery).285 This artery is inconstant and may arise from the internal iliac artery or its branches. It courses along the L-5 or S-1 nerve roots to anastomos with the conus basket.
-
a)
11.5 Intrinsic Cord Arteries
-
1)
Sulcal commissural arteries
-
a)
These arteries arise from ASA, dive into the median sulcus, and feed the grey matter structures.
-
a)
-
2)
Radial perforating arteries
-
a)
These arteries originate from the pial network, penetrate deeply, and primarily supply white matter tracts.
-
a)
-
3)
Intrinsic anastamoses
-
a)
Axial and longitudinal precapillary connections interconnect the intrinsic arteries in all planes from one to another at the same axial level, and to the vessels cranial and caudal to that level.282
-
a)
11.6 Spinal Venous System
Spinal venous anatomy is many ways similar to and in other ways different from the corresponding arterial organization. They are “the same, but different.” Lasjaunias provided an exhaustive description of spinal venous anatomy.282
-
1)
Intrinsic spinal cord veins
-
a)
Intrinsic cord veins are radially oriented venules with axial and longitudinal anastomoses. They are uniformly distributed throughout the cord. They drain into ventral and dorsal sulcal veins.
-
a)
-
2)
Extrinsic spinal cord veins
-
a)
Ventromedial and dorsomedial veins
-
i)
These are continuous longitudinal craniocaudal channels of more or less equal size. Unlike spinal cord arteries, ventral and dorsal veins do not differ significantly in size.282 Transmedullary anastomoses are present between ventral and dorsal sulcal veins.
-
i)
-
b)
Ventral and dorsal pial network
-
i)
Small interconnected veins connecting radial intrinsic veins with longitudinal veins.
-
i)
-
c)
Dorsal and ventral radicular veins
-
i)
Variable veins connecting cord veins to epidural veins. Levels without a patent radicular vein may have a fibrotic remnant. Transdural portion of the vein has a relative narrowing.
-
i)
-
d)
In thoracic region: Longitudinal ventromedial and dorsomedial veins often split up into three channels. Many more patent radicular veins are usually present, compared to the cervical and lumbar regions. The upper thoracic cord drains cephalad, and the lower thoracic cord drains in a caudal direction, producing a potential “watershed zone” at variable levels in the thoracic spinal cord.282
-
a)
-
3)
Epidural and extra-spinal veins
-
a)
Epidural venous plexus
-
i)
Dense, multichannel network from skull-base to sacrum. There are lateral longitudinal channels and side-to-side connections without valves at each vertebral level. The ventral channels are more prominent.
-
i)
-
b)
Dorsal and ventral emissary radicular veins
-
i)
These veins connect the epidural plexus to the longitudinal spinal veins (vertebral, azygos/hemiazygos, lumbar, and sacral veins).
-
i)
-
c)
Cervical region: Vertebral veins connect with the suboccipital plexus above and the jugular veins and deep cervical veins below.
-
d)
Thoracic region: On the right drainage is into the azygos vein; on the left drainage is into the superior (aka accessory) and inferior hemiazygos veins.
-
e)
Lumbar region: Drainage is into the azygos vein and directly into the inferior vena cava and left renal vein.
-
f)
Sacrum: Drainage is into the internal iliac veins.
-
a)
References
Osborn AG. Diagnostic cerebral angiography. 2nd ed. Philadelphia: Lippincott Williams & Wilkins; 1999.
De Garis CF, Black IB, Riemenschnedider EA. Patterns of the aortic arch in American white and Negro stocks, with comparative notes on certain other mammals. J Anat. 1933; 67:599–618.
Tsutsumi M, Ueno Y, Kazekawa K, Tanaka A, Nomoto Y. Aberrant right subclavian artery – three case reports. Neurol Med Chir (Tokyo). 2002;42:396–8.
La Barbera G, La Marca G, Martino A, et al. Kinking, coiling, and tortuosity of extracranial internal carotid artery: is it the effect of a metaplasia? Surg Radiol Anat. 2006;28:573–80.
Reiner A, Kasser R. Relative frequency of a subclavian vs. a transverse cervical origin for the dorsal scapular artery in humans. Anat Rec. 1996;244:265–8.
Morris P. Practical neuroangiography. Baltimore: Williams & Wilkins; 1997.
Standring S. Gray’s anatomy. 39th ed. New York: Elsevier; 2005.
Handa J, Matsuda M, Handa H. Lateral position of the external carotid artery. Report of a case. Radiology. 1972;102:361–2.
Teal JS, Rumbaugh CL, Bergeron RT, Segall HD. Lateral position of the external carotid artery: a rare anomaly? Radiology. 1973;108:77–81.
Dahn MS, Kaurich JD, Brown FR. Independent origins of the internal and external carotid arteries – a case report. Angiology. 1999;50:755–60.
Aggarwal NR, Krishnamoorthy T, Devasia B, Menon G, Chandrasekhar K. Variant origin of superior thyroid artery, occipital artery and ascending pharyngeal artery from a common trunk from the cervical segment of internal carotid artery. Surg Radiol Anat. 2006;28:650–3.
Kaneko K, Akita M, Murata E, Imai M, Sowa K. Unilateral anomalous left common carotid artery; a case report. Ann Anat. 1996;178:477–80.
Zumre O, Salbacak A, Cicekcibasi AE, Tuncer I, Seker M. Investigation of the bifurcation level of the common carotid artery and variations of the branches of the external carotid artery in human fetuses. Ann Anat. 2005;187:361–9.
Silbergleit R, Quint DJ, Mehta BA, Patel SC, Metes JJ, Noujaim SE. The persistent stapedial artery. AJNR Am J Neuroradiol. 2000;21:572–7.
Rodesch G, Choi IS, Lasjaunias P. Complete persistence of the hyoido-stapedial artery in man. Case report. Intra-petrous origin of the maxillary artery from ICA. Surg Radiol Anat. 1991;13:63–5.
Moreano EH, Paparella MM, Zelterman D, Goycoolea MV. Prevalence of facial canal dehiscence and of persistent stapedial artery in the human middle ear: a report of 1000 temporal bones. Laryngoscope. 1994;104:309–20.
Lasjaunias P, Moret J. Normal and non-pathological variations in the angiographic aspects of the arteries of the middle ear. Neuroradiology. 1978;15:213–9.
Lasjaunias P, Santoyo-Vazquez A. Segmental agenesis of the internal carotid artery: angiographic aspects with embryological discussion. Anat Clin. 1984;6:133–41.
Lasjaunias P, Berenstein A. Functional anatomy of craniofacial arteries. New York: Springer; 1987.
Monfared A, Kim D, Jaikumar S, Gorti G, Kam A. Microsurgical anatomy of the superior and recurrent laryngeal nerves. Neurosurgery. 2001;49:925–32; discussion 32–3.
Liu JL, Liang CY, Xiang T, et al. Aberrant branch of the superior laryngeal artery passing through the thyroid foramen. Clin Anat. 2007;20:256–9.
Delattre JF, Flament JB, Palot JP, Pluot M. Variations in the parathyroid glands. Number, situation and arterial vascularization. Anatomical study and surgical application. J Chir (Paris). 1982;119:633–41.
Lo A, Oehley M, Bartlett A, Adams D, Blyth P, Al-Ali S. Anatomical variations of the common carotid artery bifurcation. ANZ J Surg. 2006;76:970–2.
Hacein-Bey L, Daniels DL, Ulmer JL, et al. The ascending pharyngeal artery: branches, anastomoses, and clinical significance. AJNR Am J Neuroradiol. 2002;23:1246–56.
Haffajee MR. A contribution by the ascending pharyngeal artery to the arterial supply of the odontoid process of the axis vertebra. Clin Anat. 1997;10:14–8.
Mercer NS, MacCarthy P. The arterial supply of the palate: implications for closure of cleft palates. Plast Reconstr Surg. 1995;96:1038–44.
Huang MH, Lee ST, Rajendran K. Clinical implications of the velopharyngeal blood supply: a fresh cadaveric study. Plast Reconstr Surg. 1998;102:655–67.
Lasjaunias P, Berenstein A, Doyon D. Normal functional anatomy of the facial artery. Radiology. 1979;133:631–8.
Djindjian R, Merland J. Superselective arteriography of the external carotid artery. New York: Springer; 1978.
Niranjan NS. An anatomical study of the facial artery. Ann Plast Surg. 1988;21:14–22.
Moreau S, Bourdon N, Salame E, et al. Facial nerve: vascular-related anatomy at the stylomastoid foramen. Ann Otol Rhinol Laryngol. 2000;109:849–52.
Tubbs RS, Salter G, Oakes WJ. Continuation of the ascending cervical artery as the occipital artery in man. Anat Sci Int. 2004;79:43–5.
Lasjaunias P, Berenstein A, ter Brugge KG. Surgical neuroangiography, volume 1: clinical vascular anatomy and variations. Berlin: Springer; 2001.
McKinnon BJ, Wall MP, Karakla DW. The vascular anatomy and angiosome of the posterior auricular artery. A cadaver study. Arch Facial Plast Surg. 1999;1:101–4.
Pinar YA, Ikiz ZA, Bilge O. Arterial anatomy of the auricle: its importance for reconstructive surgery. Surg Radiol Anat. 2003;25:175–9.
Imanishi N, Nakajima H, Aiso S. Arterial anatomy of the ear. Okajimas Folia Anat Jpn. 1997;73:313–23.
Burggasser G, Happak W, Gruber H, Freilinger G. The temporalis: blood supply and innervation. Plast Reconstr Surg. 2002;109:1862–9.
Lauber H. Ueber einige varietaeten im verlaufe der arteria maxillaris interna. Anat Anz. 1901;19:444–8.
Lurje A. On the topographical anatomy of the internal maxillary artery. Acta Anat. 1947;2:219–31.
Wasicky R, Pretterklieber ML. The human anterior tympanic artery. A nutrient artery of the middle ear with highly variable origin. Cells Tissues Organs. 2000;166:388–94.
Diamond MK. Homologies of the meningeal-orbital arteries of humans: a reappraisal. J Anat. 1991;178:223–41.
Erturk M, Kayalioglu G, Govsa F, Varol T, Ozgur T. The cranio-orbital foramen, the groove on the lateral wall of the human orbit, and the orbital branch of the middle meningeal artery. Clin Anat. 2005;18:10–4.
Yoshioka N, Rhoton Jr AL, Abe H. Scalp to meningeal arterial anastomosis in the parietal foramen. Neurosurgery. 2006;58:ONS123–6; discussion ONS-6.
Tolosa E. Collateral circulation in occlusive vascular lesions of the brain. The role of the middle meningeal artery in the collateral circulation in compensating for occlusions of the internal carotid artery or its branches. Prog Brain Res. 1968;30:247–54.
Dilenge D, Ascherl Jr GF. Variations of the ophthalmic and middle meningeal arteries: relation to the embryonic stapedial artery. AJNR Am J Neuroradiol. 1980;1:45–54.
Gabriele OF, Bell D. Ophthalmic origin of the middle meningeal artery. Radiology. 1967;89:841–4.
McLennan JE, Rosenbaum AE, Haughton VM. Internal carotid origins of the middle meningeal artery. The ophthalmic-middle meningeal and stapedial-middle meningeal arteries. Neuroradiology. 1974;7:265–75.
Kawai K, Yoshinaga K, Koizumi M, Honma S, Tokiyoshi A, Kodama K. A middle meningeal artery which arises from the internal carotid artery in which the first branchial artery participates. Ann Anat. 2006;188:33–8.
Brucher J. Origin of the ophthalmic artery from the middle meningeal artery. Radiology. 1969;93:51–2.
Hiura A. An anomalous ophthalmic artery arising from the middle meningeal artery. Anat Anz. 1980;147:473–6.
Watanabe A, Hirano K, Ishii R. Dural caroticocavernous fistula with both ophthalmic arteries arising from middle meningeal arteries. Neuroradiology. 1996;38:806–8.
Liu Q, Rhoton Jr AL. Middle meningeal origin of the ophthalmic artery. Neurosurgery. 2001;49:401–6; discussion 6–7.
Anderson RJ. A palatine branch from the middle meningeal artery. J Anat Physiol. 1880;15:136–8.
Kresimir Lukic I, Gluncic V, Marusic A. Extracranial branches of the middle meningeal artery. Clin Anat. 2001;14:292–4.
Silvela J, Zamarron MA. Tentorial arteries arising from the external carotid artery. Neuroradiology. 1978;14:267–9.
Seeger JF, Hemmer JF. Persistent basilar/middle meningeal artery anastomosis. Radiology. 1976;118:367–70.
Lasjaunias P, Moret J, Manelfe C, Theron J, Hasso T, Seeger J. Arterial anomalies at the base of the skull. Neuroradiology. 1977;13:267–72.
Waga S, Okada M, Yamamoto Y. Basilar-middle meningeal arterial anastomosis. Case report. J Neurosurg. 1978;49:450–2.
Hofmeijer J, Klijn CJ, Kappelle LJ, Van Huffelen AC, Van Gijn J. Collateral circulation via the ophthalmic artery or leptomeningeal vessels is associated with impaired cerebral vasoreactivity in patients with symptomatic carotid artery occlusion. Cerebrovasc Dis. 2002;14:22–6.
Baumel JJ, Beard DY. The accessory meningeal artery of man. J Anat. 1961;95:386–402.
Vitek JJ. Accessory meningeal artery: an anatomic misnomer. AJNR Am J Neuroradiol. 1989;10:569–73.
Duncan IC, Dos Santos C. Accessory meningeal arterial supply to the posterior nasal cavity: another reason for failed endovascular treatment of epistaxis. Cardiovasc Intervent Radiol. 2003;26:488–91.
Lasjaunias P, Theron J. Radiographic anatomy of the accessory meningeal artery. Radiology. 1976;121:99–104.
Komiyama M, Kitano S, Sakamoto H, Shiomi M. An additional variant of the persistent primitive trigeminal artery: accessory meningeal artery–antero-superior cerebellar artery anastomosis associated with moyamoya disease. Acta Neurochir (Wien). 1998;140:1037–42.
Khaki AA, Tubbs RS, Shoja MM, Shokouhi G, Farahani RM. A rare variation of the inferior alveolar artery with potential clinical consequences. Folia Morphol (Warsz). 2005;64:345–6.
Chien HF, Wu CH, Wen CY, Shieh JY. Cadaveric study of blood supply to the lower intraorbital fat: etiologic relevance to the complication of anaerobic cellulitis in orbital floor fracture. J Formos Med Assoc. 2001;100:192–7.
Traxler H, Windisch A, Geyerhofer U, Surd R, Solar P, Firbas W. Arterial blood supply of the maxillary sinus. Clin Anat. 1999;12:417–21.
Markham JW. Sudden loss of vision following alcohol block of the infraorbital nerve. Case report. J Neurosurg. 1973;38:655–7.
Osborn AG. The vidian artery: normal and pathologic anatomy. Radiology. 1980;136:373–8.
Tubbs RS, Salter EG. Vidius vidius (guido guidi): 1509–1569. Neurosurgery. 2006;59:201–3; discussion 201–3.
Amin N, Ohashi Y, Chiba J, Yoshida S, Takano Y. Alterations in vascular pattern of the developing palate in normal and spontaneous cleft palate mouse embryos. Cleft Palate Craniofac J. 1994;31:332–44.
Lee HY, Kim HU, Kim SS, et al. Surgical anatomy of the sphenopalatine artery in lateral nasal wall. Laryngoscope. 2002;112:1813–8.
Pretterklieber ML, Krammer EB, Mayr R. A bilateral maxillofacial trunk in man: an extraordinary anomaly of the carotid system of arteries. Acta Anat (Basel). 1991;141:206–11.
Gibo H, Lenkey C, Rhoton Jr AL. Microsurgical anatomy of the supraclinoid portion of the internal carotid artery. J Neurosurg. 1981;55:560–74.
Bouthillier A, van Loveren HR, Keller JT. Segments of the internal carotid artery: a new classification. Neurosurgery. 1996;38:425–32; discussion 32–3.
Fischer E. Die Lageabweichungen der vorderen Hirnarterie im Gefässbild. Zentralbl Neurochir. 1938;3:300–13.
Kerber CW, Know K, Hecht ST, Buxton RB. Flow dynamics in the human carotid bulb. Int J Neuroradiol. 1996;2:422–9.
Morimoto T, Nitta K, Kazekawa K, Hashizume K. The anomaly of a non-bifurcating cervical carotid artery. Case report. J Neurosurg. 1990;72:130–2.
Pascual-Castroviejo I, Viano J, Pascual-Pascual SI, Martinez V. Facial haemangioma, agenesis of the internal carotid artery and dysplasia of cerebral cortex: case report. Neuroradiology. 1995;37:692–5.
Lee JH, Oh CW, Lee SH, Han DH. Aplasia of the internal carotid artery. Acta Neurochir (Wien). 2003;145:117–25; discussion 25.
Chen CJ, Chen ST, Hsieh FY, Wang LJ, Wong YC. Hypoplasia of the internal carotid artery with intercavernous anastomosis. Neuroradiology. 1998;40:252–4.
Quint DJ, Boulos RS, Spera TD. Congenital absence of the cervical and petrous internal carotid artery with intercavernous anastomosis. AJNR Am J Neuroradiol. 1989;10:435–9.
Tasar M, Yetiser S, Tasar A, Ugurel S, Gonul E, Saglam M. Congenital absence or hypoplasia of the carotid artery: radioclinical issues. Am J Otolaryngol. 2004;25:339–49.
Cali RL, Berg R, Rama K. Bilateral internal carotid artery agenesis: a case study and review of the literature. Surgery. 1993;113:227–33.
Teal JS, Rumbaugh CL, Segall HD, Bergeron RT. Anomalous branches of the internal cartoid artery. Radiology. 1973;106: 567–73.
Glasscock 3rd ME, Seshul M, Seshul Sr MB. Bilateral aberrant internal carotid artery case presentation. Arch Otolaryngol Head Neck Surg. 1993;119:335–9.
Chess MA, Barsotti JB, Chang JK, Ketonen LM, Westesson PL. Duplication of the extracranial internal carotid artery. AJNR Am J Neuroradiol. 1995;16:1545–7.
Pedroza A, Dujovny M, Artero JC, et al. Microanatomy of the posterior communicating artery. Neurosurgery. 1987;20:228–35.
Saltzman GF. Patent primitive trigeminal artery studied by cerebral angiography. Acta Radiol. 1959;51:329–36.
McKenzie JD, Dean BL, Flom RA. Trigeminal-cavernous fistula: Saltzman anatomy revisited. AJNR Am J Neuroradiol. 1996;17:280–2.
Uchino A, Sawada A, Takase Y, Kudo S. MR angiography of anomalous branches of the internal carotid artery. AJR Am J Roentgenol. 2003;181:1409–14.
Richardson DN, Elster AD, Ball MR. Intrasellar trigeminal artery. AJNR Am J Neuroradiol. 1989;10:205.
Lie AA. Congenital anomolies of the carotid arteries. Amsterdam: Excerpta Medica Foundation; 1968.
Patel AB, Gandhi CD, Bederson JB. Angiographic documentation of a persistent otic artery. AJNR Am J Neuroradiol. 2003;24:124–6.
Lasjaunias PL, Berenstein A. Surgical neuroangiography: functional vascular anatomy of brain, spinal cord and spine. New York: Springer; 1991.
De Caro R, Parenti A, Munari PF. The persistent primitive hypoglossal artery: a rare anatomic variation with frequent clinical implications. Ann Anat. 1995;177:193–8.
Brismar J. Persistent hypoglossal artery, diagnostic criteria. Report of a case. Acta Radiol Diagn (Stockh). 1976;17:160–6.
Kanai H, Nagai H, Wakabayashi S, Hashimoto N. A large aneurysm of the persistent primitive hypoglossal artery. Neurosurgery. 1992;30:794–7.
Kolbinger R, Heindel W, Pawlik G, Erasmi-Korber H. Right proatlantal artery type I, right internal carotid occlusion, and left internal carotid stenosis: case report and review of the literature. J Neurol Sci. 1993;117:232–9.
Suzuki S, Nobechi T, Itoh I, Yakura M, Iwashita K. Persistent proatlantal intersegmental artery and occipital artery originating from internal carotid artery. Neuroradiology. 1979;17:105–9.
San Millan Ruiz D, Gailloud P, Rufenacht DA, Delavelle J, Henry F, Fasel JH. The craniocervical venous system in relation to cerebral venous drainage. AJNR Am J Neuroradiol. 2002;23:1500–8.
De Ridder D, De Ridder L, Nowe V, Thierens H, Van de Heyning P, Moller A. Pulsatile tinnitus and the intrameatal vascular loop: why do we not hear our carotids? Neurosurgery. 2005;57:1213–7.
Paullus WS, Pait TG, Rhoton Jr AI. Microsurgical exposure of the petrous portion of the carotid artery. J Neurosurg. 1977;47:713–26.
Quisling RG, Rhoton Jr AL. Intrapetrous carotid artery branches: radioanatomic analysis. Radiology. 1979;131:133–6.
Windfuhr JP. Aberrant internal carotid artery in the middle ear. Ann Otol Rhinol Laryngol Suppl. 2004;192:1–16.
Pahor AL, Hussain SS. Persistent stapedial artery. J Laryngol Otol. 1992;106:254–7.
Tauber M, van Loveren HR, Jallo G, Romano A, Keller JT. The enigmatic foramen lacerum. Neurosurgery. 1999;44: 386–91; discussion 91–3.
Ziyal IM, Salas E, Wright DC, Sekhar LN. The petrolingual ligament: the anatomy and surgical exposure of the posterolateral landmark of the cavernous sinus. Acta Neurochir (Wien). 1998;140:201–4; discussion 4–5.
Ziyal IM, Ozgen T, Sekhar LN, Ozcan OE, Cekirge S. Proposed classification of segments of the internal carotid artery: anatomical study with angiographical interpretation. Neurol Med Chir (Tokyo). 2005;45:184–90; discussion 90–1.
Marshman LA, Connor S, Polkey CE. Internal carotid-inferior petrosal sinus fistula complicating foramen ovale telemetry: successful treatment with detachable coils: case report and review. Neurosurgery. 2002;50:209–12.
Resnick DK, Subach BR, Marion DW. The significance of carotid canal involvement in basilar cranial fracture. Neurosurgery. 1997;40:1177–81.
Rhoton Jr AL. The sellar region. Neurosurgery. 2002;51: S335–74.
Inoue T, Rhoton Jr AL, Theele D, Barry ME. Surgical approaches to the cavernous sinus: a microsurgical study. Neurosurgery. 1990;26:903–32.
Tran-Dinh H. Cavernous branches of the internal carotid artery: anatomy and nomenclature. Neurosurgery. 1987;20:205–10.
Rhoton Jr AL. The cavernous sinus, the cavernous venous plexus, and the carotid collar. Neurosurgery. 2002;51: S375–410.
Bernasconi V, Cassinari V. Angiographical characteristics of meningiomas of tentorium. Radiol Med (Torino). 1957;43:1015–26.
Tsitsopoulos PD, Tsonidis CA, Petsas GP, Hadjiioannou PN, Njau SN, Anagnostopoulos IV. Microsurgical study of the Dorello’s canal. Skull Base Surg. 1996;6:181–5.
Parkinson D. Collateral circulation of cavernous carotid artery: anatomy. Can J Surg. 1964;7:251–68.
Hayreh SS. Orbital vascular anatomy. Eye. 2006;20: 1130–44.
Renn WH, Rhoton Jr AL. Microsurgical anatomy of the sellar region. J Neurosurg. 1975;43:288–98.
Sacher M, Som PM, Shugar JM, Leeds NE. Kissing intrasellar carotid arteries in acromegaly: CT demonstration. J Comput Assist Tomogr. 1986;10:1033–5.
Midkiff RB, Boykin MW, McFarland DR, Bauman JA. Agenesis of the internal carotid artery with intercavernous anastomosis. AJNR Am J Neuroradiol. 1995;16:1356–9.
Kobayashi S, Kyoshima K, Gibo H, Hegde SA, Takemae T, Sugita K. Carotid cave aneurysms of the internal carotid artery. J Neurosurg. 1989;70:216–21.
Gonzalez LF, Walker MT, Zabramski JM, Partovi S, Wallace RC, Spetzler RF. Distinction between paraclinoid and cavernous sinus aneurysms with computed tomographic angiography. Neurosurgery. 2003;52:1131–7; discussion 8–9.
Tsutsumi S, Rhoton Jr AL. Microsurgical anatomy of the central retinal artery. Neurosurgery. 2006;59:870–8; discussion 8–9.
Gray H. Gray’s anatomy. 1901st ed. Philadelphia: Running Press; 1901.
Hayreh SS. Arteries of the orbit in the human being. Br J Surg. 1963;50:938–53.
Lang J, Kageyama I. The ophthalmic artery and its branches, measurements and clinical importance. Surg Radiol Anat. 1990;12:83–90.
Krisht AF, Barrow DL, Barnett DW, Bonner GD, Shengalaia G. The microsurgical anatomy of the superior hypophyseal artery. Neurosurgery. 1994;35:899–903; discussion 903.
Alvarez H, Rodesch G, Garcia-Monaco R, Lasjaunias P. Embolisation of the ophthalmic artery branches distal to its visual supply. Surg Radiol Anat. 1990;12:293–7.
Saeki N, Rhoton Jr AL. Microsurgical anatomy of the upper basilar artery and the posterior circle of Willis. J Neurosurg. 1977;46:563–78.
Alpers BJ, Berry RG, Paddison RM. Anatomical studies of the circle of Willis in normal brain. AMA Arch Neurol Psychiatry. 1959;81:409–18.
Tripathi M, Goel V, Padma MV, et al. Fenestration of the posterior communicating artery. Neurol India. 2003;51: 75–6.
Rhoton Jr AL, Fujii K, Fradd B. Microsurgical anatomy of the anterior choroidal artery. Surg Neurol. 1979;12:171–87.
Morandi X, Brassier G, Darnault P, Mercier P, Scarabin JM, Duval JM. Microsurgical anatomy of the anterior choroidal artery. Surg Radiol Anat. 1996;18:275–80.
Paroni Sterbini GL, Agatiello LM, Stocchi A, Solivetti FM. CT of ischemic infarctions in the territory of the anterior choroidal artery: a review of 28 cases. AJNR Am J Neuroradiol. 1987;8:229–32.
Das K, Benzil DL, Rovit RL, Murali R, Couldwell WT. Irving S. Cooper (1922–1985): a pioneer in functional neurosurgery. J Neurosurg. 1998;89:865–73.
Cooper IS. Surgical occlusion of the anterior choroidal artery in parkinsonism. Surg Gynecol Obstet. 1954;92:207–19.
Moyer DJ, Flamm ES. Anomalous arrangement of the origins of the anterior choroidal and posterior communicating arteries. Case report. J Neurosurg. 1992;76:1017–8.
Takahashi S, Suga T, Kawata Y, Sakamoto K. Anterior choroidal artery: angiographic analysis of variations and anomalies. AJNR Am J Neuroradiol. 1990;11:719–29.
Taveras JM, Wood EH. Diagnostic neuroradiology. 2nd ed. Baltimore: Williams & Wilkins; 1976. p. 584–7.
Waga S, Morikawa A. Aneurysm developing on the infundibular widening of the posterior communicating artery. Surg Neurol. 1979;11:125–7.
Ohyama T, Ohara S, Momma F. Fatal subarachnoid hemorrhage due to ruptured infundibular widening of the posterior communicating artery–case report. Neurol Med Chir (Tokyo). 1994;34:172–5.
Saltzman GF. Infundibular widening of the posterior communicating artery studied by carotid angiography. Acta Radiol. 1959;51:415–21.
Wollschlaeger G, Wollschlaeger PB, Lucas FV, Lopez VF. Experience and result with postmortem cerebral angiography performed as routine procedure of the autopsy. Am J Roentgenol Radium Ther Nucl Med. 1967;101:68–87.
Willis T. Cerebri anatome; cui accessit nervorum descriptio et usus. London: J. Flesher; 1664.
Wolpert SM. The circle of Willis. AJNR Am J Neuroradiol. 1997;18:1033–4.
Krabbe-Hartkamp MJ, van der Grond J, de Leeuw FE, et al. Circle of Willis: morphologic variation on three-dimensional time-of-flight MR angiograms. Radiology. 1998;207:103–11.
Hendrikse J, van Raamt AF, van der Graaf Y, Mali WPTM, van der Grond J. Distribution of cerebral blood flow in the circle of Willis. Radiology. 2005;235:184–9.
Alpers BJ, Berry RG. Circle of Willis in cerebral vascular disorders. The anatomical structure. Arch Neurol. 1963;8: 398–402.
Rhoton Jr AL, Saeki N, Perlmutter D, Zeal A. Microsurgical anatomy of common aneurysm sites. Clin Neurosurg. 1979;26:248–306.
Hoksbergen AW, Legemate DA, Csiba L, Csati G, Siro P, Fulesdi B. Absent collateral function of the circle of Willis as risk factor for ischemic stroke. Cerebrovasc Dis. 2003;16: 191–8.
Serizawa T, Saeki N, Yamaura A. Microsurgical anatomy and clinical significance of the anterior communicating artery and its perforating branches. Neurosurgery. 1997; 40:1211–6; discussion 6–8.
Dunker RO, Harris AB. Surgical anatomy of the proximal anterior cerebral artery. J Neurosurg. 1976;44:359–67.
Gomes FB, Dujovny M, Umansky F, et al. Microanatomy of the anterior cerebral artery. Surg Neurol. 1986;26:129–41.
Zurada A, St Gielecki J, Tubbs RS, et al. Three-dimensional morphometry of the A1 segment of the anterior cerebral artery with neurosurgical relevance. Neurosurgery. 2010;67:1768–82.
Marinkovic S, Milisavljevic M, Kovacevic M. Anatomical bases for surgical approach to the initial segment of the anterior cerebral artery. Microanatomy of Heubner’s artery and perforating branches of the anterior cerebral artery. Surg Radiol Anat. 1986;8:7–18.
Moffat DB. A case of peristence of the primitive olfactory artery. Anat Anz. 1967;121:477–9.
Nozaki K, Taki W, Kawakami O, Hashimoto N. Cerebral aneurysm associated with persistent primitive olfactory artery aneurysm. Acta Neurochir (Wien). 1998;140:397–401; discussion 401–2.
Bollar A, Martinez R, Gelabert M, Garcia A. Anomalous origin of the anterior cerebral artery associated with aneurysm–embryological considerations. Neuroradiology. 1988; 30:86.
Maurer J, Maurer E, Perneczky A. Surgically verified variations in the A1 segment of the anterior cerebral artery. Report of two cases. J Neurosurg. 1991;75:950–3.
Given 2nd CA, Morris PP. Recognition and importance of an infraoptic anterior cerebral artery: case report. AJNR Am J Neuroradiol. 2002;23:452–4.
Minakawa T, Kawamata M, Hayano M, Kawakami K. Aneurysms associated with fenestrated anterior cerebral arteries. Report of four cases and review of the literature. Surg Neurol. 1985;24:284–8.
Suzuki M, Onuma T, Sakurai Y, Mizoi K, Ogawa A, Yoshimoto T. Aneurysms arising from the proximal (A1) segment of the anterior cerebral artery. A study of 38 cases. J Neurosurg. 1992;76:455–8.
Choudhari KA. Fenestrated anterior cerebral artery. Br J Neurosurg. 2002;16:525–9.
Ladzinski P, Maliszewski M, Majchrzak H. The accessory anterior cerebral artery: case report and anatomic analysis of vascular anomaly. Surg Neurol. 1997;48:171–4.
Singer RJ, Abe T, Taylor WH, Marks MP, Norbash AM. Intracavernous anterior cerebral artery origin with associated arteriovenous malformations: a developmental analysis: case report. Neurosurgery. 1997;40:829–31; discussion 31.
Spinnato S, Pasqualin A, Chioffi F, Da Pian R. Infraoptic course of the anterior cerebral artery associated with an anterior communicating artery aneurysm: anatomic case report and embryological considerations. Neurosurgery. 1999;44:1315–9.
Burbank NS, Morris PP. Unique anomalous origin of the left anterior cerebral artery. AJNR Am J Neuroradiol. 2005; 26:2533–5.
Busse O. Aneurysmen und Bildungsfehler der A. Communicans Anterior. Virchows Arch Pathol Anat. 1927;229:178–89.
Perlmutter D, Rhoton Jr AL. Microsurgical anatomy of the anterior cerebral-anterior communicating-recurrent artery complex. J Neurosurg. 1976;45:259–72.
Marinkovic S, Milisavljevic M, Marinkovic Z. Branches of the anterior communicating artery. Microsurgical anatomy. Acta Neurochir (Wien). 1990;106:78–85.
Perlmutter D, Rhoton Jr AL. Microsurgical anatomy of the distal anterior cerebral artery. J Neurosurg. 1978;49:204–28.
Ostrowski AZ, Webster JE, Gurdjian ES. The proximal anterior cerebral artery: an anatomic study. Arch Neurol. 1960;3:661–4.
Baptista AG. Studies on the arteries of the brain. Ii. The anterior cerebral artery: some anatomic features and their clinical implications. Neurology. 1963;13:825–35.
Huber P, Braun J, Hirschmann D, Agyeman JF. Incidence of berry aneurysms of the unpaired pericallosal artery: angiographic study. Neuroradiology. 1980;19:143–7.
Cinnamon J, Zito J, Chalif DJ, et al. Aneurysm of the azygos pericallosal artery: diagnosis by MR imaging and MR angiography. AJNR Am J Neuroradiol. 1992;13:280–2.
Osaka K, Matsumoto S. Holoprosencephaly in neurosurgical practice. J Neurosurg. 1978;48:787–803.
Yasargil MG, Carter LP. Saccular aneurysms of the distal anterior cerebral artery. J Neurosurg. 1974;40:218–23.
Gloger S, Gloger A, Vogt H, Kretschmann HJ. Computer-assisted 3D reconstruction of the terminal branches of the cerebral arteries. I. Anterior cerebral artery. Neuroradiology. 1994;36:173–80.
Gibo H, Carver CC, Rhoton Jr AL, Lenkey C, Mitchell RJ. Microsurgical anatomy of the middle cerebral artery. J Neurosurg. 1981;54:151–69.
Umansky F, Gomes FB, Dujovny M, et al. The perforating branches of the middle cerebral artery. A microanatomical study. J Neurosurg. 1985;62:261–8.
Grand W. Microsurgical anatomy of the proximal middle cerebral artery and the internal carotid artery bifurcation. Neurosurgery. 1980;7:215–8.
Komiyama M, Nakajima H, Nishikawa M, Yasui T. Middle cerebral artery variations: duplicated and accessory arteries. AJNR Am J Neuroradiol. 1998;19:45–9.
Umansky F, Dujovny M, Ausman JI, Diaz FG, Mirchandani HG. Anomalies and variations of the middle cerebral artery: a microanatomical study. Neurosurgery. 1988;22:1023–7.
Uchino M, Kitajima S, Sakata Y, Honda M, Shibata I. Ruptured aneurysm at a duplicated middle cerebral artery with accessory middle cerebral artery. Acta Neurochir (Wien). 2004;146:1373–4; discussion 5.
Takahashi T, Suzuki S, Ohkuma H, Iwabuchi T. Aneurysm at a duplication of the middle cerebral artery. AJNR Am J Neuroradiol. 1994;15:1166–8.
Jain KK. Some observations on the anatomy of the middle cerebral artery. Can J Surg. 1964;7:134–9.
Gloger S, Gloger A, Vogt H, Kretschmann HJ. Computer-assisted 3D reconstruction of the terminal branches of the cerebral arteries. II. Middle cerebral artery. Neuroradiology. 1994;36:181–7.
Abanou A, Lasjaunias P, Manelfe C, Lopez-Ibor L. The accessory middle cerebral artery (AMCA). Diagnostic and therapeutic consequences. Anat Clin. 1984;6:305–9.
Morioka M, Fujioka S, Itoyama Y, Ushio Y. Ruptured distal accessory anterior cerebral artery aneurysm: case report. Neurosurgery. 1997;40:399–401; discussion 401–2.
Takahashi S, Hoshino F, Uemura K, Takahashi A, Sakamoto K. Accessory middle cerebral artery: is it a variant form of the recurrent artery of Heubner? AJNR Am J Neuroradiol. 1989;10:563–8.
Han DH, Gwak HS, Chung CK. Aneurysm at the origin of accessory middle cerebral artery associated with middle cerebral artery aplasia: case report. Surg Neurol. 1994;42:388–91.
Van Der Zwan A, Hillen B. Araldite F as injection material for quantitative morphology of cerebral vascularization. Anat Rec. 1990;228:230–6.
Heubner O. Die luetischen Erkrankungen der Hirnarterien. Leipzig: FC Vogel; 1874. p. 170–214.
Vander Eecken HM, Adams RD. The anatomy and functional significance of the meningeal arterial anastomoses of the human brain. J Neuropathol Exp Neurol. 1953;12:132–57.
Brozici M, van der Zwan A, Hillen B. Anatomy and functionality of leptomeningeal anastomoses: a review. Stroke. 2003;34:2750–62.
Michotey P, Moscow NP, Salamon G. Anatomy of the cortical branches of the middle cerebral artery. In: Newton TH, Potts DG, editors. Radiology of the skull and brain. St. Louis: C.V. Mosby; 1974. p. 1471–8.
Hart JL, Davagnanam I, Chandrashekar HS, Brew S. Angiography and selective microcatheter embolization of a falcine meningioma supplied by the artery of Davidoff and Schechter. J Neurosurg. 2011;114:710–3.
Margolis MT, Newton TH, Hoyt WF. Gross and roentgenologic anatomy of the posterior cerebral artery. In: Newton TH, Potts PC, editors. Radiology of the skull and brain. St. Louis: C.V. Mosby; 1974. p. 1551–76.
Margolis MT, Newton TH, Hoyt WF. Cortical branches of the posterior cerebral artery. Anatomic-radiologic correlation. Neuroradiology. 1971;2:127–35.
Caruso G, Vincentelli F, Rabehanta P, Giudicelli G, Grisoli F. Anomalies of the P1 segment of the posterior cerebral artery: early bifurcation or duplication, fenestration, common trunk with the superior cerebellar artery. Acta Neurochir (Wien). 1991;109:66–71.
Percheron G. Arteries of the human thalamus. II. Arteries and paramedian thalamic territory of the communicating basilar artery. Rev Neurol (Paris). 1976;132:309–24.
Raphaeli G, Liberman A, Gomori JM, Steiner I. Acute bilateral paramedian thalamic infarcts after occlusion of the artery of Percheron. Neurology. 2006;66:E7.
Matheus MG, Castillo M. Imaging of acute bilateral paramedian thalamic and mesencephalic infarcts. AJNR Am J Neuroradiol. 2003;24:2005–8.
Milisavljevic MM, Marinkovic SV, Gibo H, Puskas LF. The thalamogeniculate perforators of the posterior cerebral artery: the microsurgical anatomy. Neurosurgery. 1991;28: 523–9; discussion 9–30.
Berland LL, Haughton VM. Anomalous origin of posterior choroidal artery from basilar artery. AJR Am J Roentgenol. 1979;132:674–5.
Fujii K, Lenkey C, Rhoton Jr AL. Microsurgical anatomy of the choroidal arteries: lateral and third ventricles. J Neurosurg. 1980;52:165–88.
Galloway JR, Greitz T. The medial and lateral choroid arteries. An anatomic and roentgenographic study. Acta Radiol. 1960;53:353–66.
Wollschlaeger PB, Wollschlaeger G. An infratentorial meningeal artery. Radiologe. 1965;5:451–2.
Ono M, Ono M, Rhoton Jr AL, Barry M. Microsurgical anatomy of the region of the tentorial incisura. J Neurosurg. 1984;60:365–99.
Bojanowski WM, Rigamonti D, Spetzler RF, Flom R. Angiographic demonstration of the meningeal branch of the posterior cerebral artery. AJNR Am J Neuroradiol. 1988;9:808.
Furuno M, Yamakawa N, Okada M, Waga S. Anomalous origin of the calcarine artery. Neuroradiology. 1995; 37:658.
Abrahams JM, Hurst RW, Bagley LJ, Zager EL. Anterior choroidal artery supply to the posterior cerebral artery distribution: embryological basis and clinical implications. Neurosurgery. 1999;44:1308–14.
Tubbs RS, Salter G, Wellons 3rd JC, Oakes WJ. Blood supply of the human cervical sympathetic chain and ganglia. Eur J Morphol. 2002;40:283–8.
Lemke AJ, Benndorf G, Liebig T, Felix R. Anomalous origin of the right vertebral artery: review of the literature and case report of right vertebral artery origin distal to the left subclavian artery. AJNR Am J Neuroradiol. 1999;20:1318–21.
Goray VB, Joshi AR, Garg A, Merchant S, Yadav B, Maheshwari P. Aortic arch variation: a unique case with anomalous origin of both vertebral arteries as additional branches of the aortic arch distal to left subclavian artery. AJNR Am J Neuroradiol. 2005;26:93–5.
Palmer FJ. Origin of the right vertebral artery from the right common carotid artery: angiographic demonstration of three cases. Br J Radiol. 1977;50:185–7.
Goddard AJ, Annesley-Williams D, Guthrie JA, Weston M. Duplication of the vertebral artery: report of two cases and review of the literature. Neuroradiology. 2001;43:477–80.
Tubbs RS, Loukas M, Remy AC, Shoja MM, Salter EG, Oakes WJ. The vertebral nerve revisited. Clin Anat. 2007; 20:644–7.
Brink B. Approaches to the second segment of the vertebral artery. In: Berguer R, Bauer R, editors. Vertebrobasilar arterial occlusive disease. New York: Raven; 1984. p. 257–64.
Diaz FG, Ausman JI, Shrontz C, et al. Surgical correction of lesions affecting the second portion of the vertebral artery. Neurosurgery. 1986;19:93–100.
D’Antoni AV, Battaglia F, Dilandro AC, Moore GD. Anatomic study of the suboccipital artery of Salmon with surgical significance. Clin Anat. 2010;23(7):798–802.
Fine AD, Cardoso A, Rhoton Jr AL. Microsurgical anatomy of the extracranial-extradural origin of the posterior inferior cerebellar artery. J Neurosurg. 1999;91:645–52.
de Oliveira E, Rhoton Jr AL, Peace D. Microsurgical anatomy of the region of the foramen magnum. Surg Neurol. 1985;24:293–352.
Akar ZC, Dujovny M, Slavin KV, Gomez-Tortosa E, Ausman JI. Microsurgical anatomy of the intracranial part of the vertebral artery. Neurol Res. 1994;16:171–80.
Lister JR, Rhoton Jr AL, Matsushima T, Peace DA. Microsurgical anatomy of the posterior inferior cerebellar artery. Neurosurgery. 1982;10:170–99.
Ahuja A, Graves VB, Crosby DL, Strother CM. Anomalous origin of the posterior inferior cerebellar artery from the internal carotid artery. AJNR Am J Neuroradiol. 1992;13:1625–6.
Ogawa T, Fujita H, Inugami A, Shishido F, Higano S, Uemura K. Anomalous origin of the posterior inferior cerebellar artery from the posterior meningeal artery. AJNR Am J Neuroradiol. 1991;12:186.
Margolis MT, Newton TH. The posterior inferior cerebellar artery. In: Newton TH, Potts DG, editors. Radiology of the skull and brain. St. Louis: C.V. Mosby; 1974. p. 1710–74.
Salamon G, Huang YP. Radiologic anatomy of the brain. Berlin: Springer; 1976. p. 305–6.
Lewis SB, Chang DJ, Peace DA, Lafrentz PJ, Day AL. Distal posterior inferior cerebellar artery aneurysms: clinical features and management. J Neurosurg. 2002;97:756–66.
Smoker WR, Price MJ, Keyes WD, Corbett JJ, Gentry LR. High-resolution computed tomography of the basilar artery: 1. Normal size and position. AJNR Am J Neuroradiol. 1986;7:55–60.
Torche M, Mahmood A, Araujo R, Dujovny M, Dragovic L, Ausman JI. Microsurgical anatomy of the lower basilar artery. Neurol Res. 1992;14:259–62.
Shrontz C, Dujovny M, Ausman JI, et al. Surgical anatomy of the arteries of the posterior fossa. J Neurosurg. 1986;65:540–4.
Amarenco P, Rosengart A, DeWitt LD, Pessin MS, Caplan LR. Anterior inferior cerebellar artery territory infarcts. Mechanisms and clinical features. Arch Neurol. 1993;50: 154–61.
Naidich TP, Kricheff II, George AE, Lin JP. The normal anterior inferior cerebellar artery. Anatomic-radiographic correlation with emphasis on the lateral projection. Radiology. 1976;119:355–73.
Atkinson WJ. The anterior inferior cerebellar artery: it’s variation, pontine distribution and significance in surgery of cerebello-pontine angle tumors. J Neurol Neurosurg Psychiatry. 1949;12:137–51.
Rhoton Jr AL. Microsurgery of the internal acoustic meatus. Surg Neurol. 1974;2:311–8.
Brunsteins DB, Ferreri AJ. Microsurgical anatomy of VII and VIII cranial nerves and related arteries in the cerebellopontine angle. Surg Radiol Anat. 1990;12:259–65.
Martin RG, Grant JL, Peace D, Theiss C, Rhoton Jr AL. Microsurgical relationships of the anterior inferior cerebellar artery and the facial-vestibulocochlear nerve complex. Neurosurgery. 1980;6:483–507.
Ito J, Takeda N, Suzuki Y, Tekeuchi S, Osugi S, Yoshida Y. Anomalous origin of the anterior inferior cerebellar arteries from the internal carotid artery. Neuroradiology. 1980;19: 105–9.
Caruso G, Vincentelli F, Giudicelli G, Grisoli F, Xu T, Gouaze A. Perforating branches of the basilar bifurcation. J Neurosurg. 1990;73:259–65.
Pedroza A, Dujovny M, Ausman JI, et al. Microvascular anatomy of the interpeduncular fossa. J Neurosurg. 1986; 64:484–93.
Hardy DG, Rhoton Jr AL. Microsurgical relationships of the superior cerebellar artery and the trigeminal nerve. J Neurosurg. 1978;49:669–78.
Hardy DG, Peace DA, Rhoton Jr AL. Microsurgical anatomy of the superior cerebellar artery. Neurosurgery. 1980;6: 10–28.
Stopford JSB. The arteries of the pons and medulla oblongata. J Anat. 1916;50:131–64.
De Caro R, Serafini MT, Galli S, Parenti A, Guidolin D, Munari PF. Anatomy of segmental duplication in the human basilar artery. Possible site of aneurysm formation. Clin Neuropathol. 1995;14:303–9.
Sanders WP, Sorek PA, Mehta BA. Fenestration of intracranial arteries with special attention to associated aneurysms and other anomalies. AJNR Am J Neuroradiol. 1993;14:675–80.
Huber P. Cerebral angiography. 2nd ed. New York: Thieme; 1982.
Osborn AG. Craniofacial venous plexuses: angiographic study. AJR Am J Roentgenol. 1981;136:139–43.
Braun JP, Tournade A. Venous drainage in the craniocervical region. Neuroradiology. 1977;13:155–8.
Andrews BT, Dujovny M, Mirchandani HG, Ausman JI. Microsurgical anatomy of the venous drainage into the superior sagittal sinus. Neurosurgery. 1989;24:514–20.
Curé JK, Van Tassel P, Smith MT. Normal and variant anatomy of the dural venous sinuses. Semin Ultrasound CT MR. 1994;15:499–519.
Boyd GI. The emissary foramina of the cranium in man and the anthropoids. J Anat. 1930;65:108–21.
Thewissen JG. Mammalian frontal diploic vein and the human foramen caecum. Anat Rec. 1989;223:242–4.
San Millan Ruiz D, Gailloud P, Rufenacht DA, Yilmaz H, Fasel JH. Anomalous intracranial drainage of the nasal mucosa: a vein of the foramen caecum? AJNR Am J Neuroradiol. 2006;27:129–31.
Jaeger R. Observations on resection of the superior longitudinal sinus at and posterior to the rolandic venous inflow. J Neurosurg. 1951;8:103–9.
Hasegawa M, Yamashita J, Yamashima T. Anatomical variations of the straight sinus on magnetic resonance imaging in the infratentorial supracerebellar approach to pineal region tumors. Surg Neurol. 1991;36:354–9.
Browder J, Kaplan HA, Krieger AJ. Anatomical features of the straight sinus and its tributaries. J Neurosurg. 1976;44: 55–61.
Das AC, Hasan M. The occipital sinus. J Neurosurg. 1970;33:307–11.
Green HT. The venous drainage of the human hypophysis cerebri. Am J Anat. 1957;100:435–69.
Tubbs RS. Herophilus of Chalcedon: a pioneer in neuroscience. Neurosurgery. 2006;58:E590; discussion E.
Gebarski SS, Gebarski KS. Inferior petrosal sinus: imaging-anatomic correlation. Radiology. 1995;194:239–47.
Hacker H. Superficial supratentorial veins and dural sinues. In: Newton TH, Potts DG, editors. Radiology of the skull and brain: veins. St. Louis: C.V. Mosby; 1974. p. 1851–902.
Galligioni F, Bernardi R, Pellone M, Iraci G. The superficial sylvian vein in normal and pathologic cerebral angiography. Am J Roentgenol Radium Ther Nucl Med. 1969;107: 565–78.
Sener RN. The occipitotemporal vein: a cadaver, MRI and CT study. Neuroradiology. 1994;36:117–20.
Di Chiro G. Angiographic patterns of cerebral convexity veins and superficial dural sinuses. Am J Roentgenol Radium Ther Nucl Med. 1962;87:308–21.
Ture U, Yasargil MG, Al-Mefty O. The transcallosal-transforaminal approach to the third ventricle with regard to the venous variations in this region. J Neurosurg. 1997;87:706–15.
Ono M, Rhoton Jr AL, Peace D, Rodriguez RJ. Microsurgical anatomy of the deep venous system of the brain. Neurosurgery. 1984;15:621–57.
Garner TB, Del Curling Jr O, Kelly Jr DL, Laster DW. The natural history of intracranial venous angiomas. J Neurosurg. 1991;75:715–22.
Wilms G, Bleus E, Demaerel P, et al. Simultaneous occurrence of developmental venous anomalies and cavernous angiomas. AJNR Am J Neuroradiol. 1994;15:1247–54; discussion 55–7.
Abe T, Singer RJ, Marks MP, Norbash AM, Crowley RS, Steinberg GK. Coexistence of occult vascular malformations and developmental venous anomalies in the central nervous system: MR evaluation. AJNR Am J Neuroradiol. 1998;19:51–7.
Mullan S, Mojtahedi S, Johnson DL, Macdonald RL. Embryological basis of some aspects of cerebral vascular fistulas and malformations. J Neurosurg. 1996;85:1–8.
Raybaud CA, Strother CM, Hald JK. Aneurysms of the vein of Galen: embryonic considerations and anatomical features relating to the pathogenesis of the malformation. Neuroradiology. 1989;31:109–28.
Gailloud P, O’Riordan DP, Burger I, Lehmann CU. Confirmation of communication between deep venous drainage and the vein of galen after treatment of a vein of Galen aneurysmal malformation in an infant presenting with severe pulmonary hypertension. AJNR Am J Neuroradiol. 2006;27:317–20.
Siclari F, Burger IM, Fasel JH, Gailloud P. Developmental anatomy of the distal vertebral artery in relationship to variants of the posterior and lateral spinal arterial systems. AJNR Am J Neuroradiol. 2007;28:1185–90.
Chakravorty BG. Arterial supply of the cervical spinal cord (with special reference to the radicular arteries). Anat Rec. 1971;170:311–29.
Schalow G. Feeder arteries, longitudinal arterial trunks and arterial anastomoses of the lower human spinal cord. Zentralbl Neurochir. 1990;51:181–4.
Rodriguez-Baeza A, Muset-Lara A, Rodriguez-Pazos M, Domenech-Mateu JM. The arterial supply of the human spinal cord: a new approach to the arteria radicularis magna of Adamkiewicz. Acta Neurochir (Wien). 1991;109:57–62.
Biglioli P, Roberto M, Cannata A, et al. Upper and lower spinal cord blood supply: the continuity of the anterior spinal artery and the relevance of the lumbar arteries. J Thorac Cardiovasc Surg. 2004;127:1188–92.
Tveten L. Spinal cord vascularity. III. The spinal cord arteries in man. Acta Radiol Diagn (Stockh). 1976;17:257–73.
Lo D, Vallee JN, Spelle L, et al. Unusual origin of the artery of Adamkiewicz from the fourth lumbar artery. Neuroradiology. 2002;44:153–7.
Adamkiewicz A. Die Blutgefasse desmenschlichen Ruckenmarkes. I. Theil. Die Gefasse der Ruckenmarkssubstanz. Sitzungsberichte der Kaiserlichen Akademie der Wissenschaften, mathematisch-naturwissenschaftliche Classe. 1881;84:469–502.
Desproges-Gotteron R. Contribution á l’étude de la sciatque paralysante (thése). Paris; 1955.
Habel RE, Budras KD. Bovine anatomy: an illustrated text. Hanover: Schlütersche GmbH & Co.; 2003.
Layton KF, Kallmes DF, Cloft HJ, Lindell EP, Cox VS. Bovine aortic arch variant in humans: clarification of a common misnomer. AJNR Am J Neuroradiol. 2006;27:1541–2.
Pickhardt PJ, Siegel MJ, Gutierrez FR. Vascular rings in symptomatic children: frequency of chest radiographic findings. Radiology. 1997;203:423–6.
Gottfried ON, Soleau SW, Couldwell WT. Suprasellar displacement of intracavernous internal carotid artery: case report. Neurosurgery. 2003;53:1433–4; discussion 4–5.
Fujimura M, Seki H, Sugawara T, Tomichi N, Oku T, Higuchi H. Anomalous internal carotid artery-anterior cerebral artery anastomosis associated with fenestration and cerebral aneurysm. Neurol Med Chir (Tokyo). 1996;36: 229–33.
Hayreh SS, Dass R. The ophthalmic artery. II. Origin and intracranial and intra-canalicular course. Br J Ophthalmol. 1962;46:165–85.
Lasjaunias P, Vallee B, Person H, Ter Brugge K, Chiu M. The lateral spinal artery of the upper cervical spinal cord. Anatomy, normal variations, and angiographic aspects. J Neurosurg. 1985;63:235–41.
Barr JD, Lemley TJ. Endovascular arterial occlusion accomplished using microcoils deployed with and without proximal flow arrest: results in 19 patients. AJNR Am J Neuroradiol. 1999;20:1452–6.
Zouaoui A, Hidden G. Cerebral venous sinuses: anatomical variants or thrombosis? Acta Anat (Basel). 1988;133: 318–24.
Acar F, Naderi S, Guvencer M, Ture U, Arda MN. Herophilus of Chalcedon: a pioneer in neuroscience. Neurosurgery. 2005;56:861–7; discussion 861–7.
Author information
Authors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media New York
About this chapter
Cite this chapter
Harrigan, M.R., Deveikis, J.P. (2013). Essential Neurovascular Anatomy. In: Handbook of Cerebrovascular Disease and Neurointerventional Technique. Contemporary Medical Imaging, vol 1. Humana Press, Totowa, NJ. https://doi.org/10.1007/978-1-61779-946-4_1
Download citation
DOI: https://doi.org/10.1007/978-1-61779-946-4_1
Published:
Publisher Name: Humana Press, Totowa, NJ
Print ISBN: 978-1-61779-945-7
Online ISBN: 978-1-61779-946-4
eBook Packages: MedicineMedicine (R0)