
Abstract
Of all the forms of chronic insomnia, perhaps the most insidious is Psychophysiologic insomnia, also called Primary Insomnia in the DSM-IV. This sleep disorder is a final common pathway for many people who initially develop sleeplessness in the context of acute stressors (e.g., pain, job loss), but then acquire a form of “learned” sleeplessness as they become increasingly overconcerned about their unsatisfying sleep patterns. Patients report reduced total sleep time, with increased sleep latency (greater than 30 min), or increased wakeafter sleep onset time, though these findings are not always corroborated on PSG studies. Patients with this form of chronic insomnia are often vexed by its seemingly unpredictable nature from night to night, but to be diagnosed symptoms must be present on three or more nights per week, for more than 1 month (DSM-IV) or 6 months (ICSD-2). The essential feature of this form of insomnia is a pattern of sleep disturbance that evolves over time as a result of psychological distress that triggers unhelpful behaviors and physiological arousal. This chapter will summarize the current understanding of the development of this disorder, and the clinical approaches that may be useful to resolve it.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Psychophysiological insomnia
- Primary insomnia
- Cognitive behavioral therapy
- Sedative-hypnotic medications
- Biofeedback
Introduction
Of all the forms of chronic insomnia, perhaps the most insidious is Psychophysiologic insomnia, also called Primary Insomnia in the DSM-IV. This sleep disorder is a final common pathway for many people who initially develop sleeplessness in the context of acute stressors (e.g., pain, job loss), but then acquire a form of “learned” sleeplessness as they become increasingly overconcerned about their unsatisfying sleep patterns. Patients report reduced total sleep time, with increased sleep latency (greater than 30 min), or increased wake after sleep onset time, though these findings are not always corroborated on PSG studies. Patients with this form of chronic insomnia are often vexed by its seemingly unpredictable nature from night to night, but to be diagnosed symptoms must be present on three or more nights per week, for more than 1 month (DSM-IV) or 6 months (ICSD-2). The essential feature of this form of insomnia is a pattern of sleep disturbance that evolves over time as a result of psychological distress that triggers unhelpful behaviors and physiological arousal. This chapter will summarize the current understanding of the development of this disorder, and the clinical approaches that may be useful to resolve it.
Etiology of Psychophysiologic Insomnia
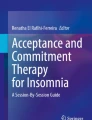
The process of transitioning from wake to sleep involves many steps, most of which we do not usually consider. Given the right circadian timing, and a reasonably accommodating sleep environment, most adults fall asleep within 30 min [1]. For many, the added pressure of chronic sleep deprivation makes sleep onset that much easier and faster. However, when circumstances are unfavorable for sleep, or there is added psychophysiologic tension, falling asleep, or returning to sleep may be delayed. Given several difficult nights of sleep, some people develop conscious as well as unconscious negative associations to their bed and bedroom environment that heighten arousal levels, making it more likely that the trend will continue with successive nights of “failure”. Unfortunately, in frustration and despair, these individuals often make poor choices that may further worsen their sleep disturbance. Using alcohol to facilitate sleep, or going to bed extra early to try to “catch” some sleep may seem like reasonable approaches to the patient, but tend to exacerbate insomnia [2]. Thus the model for this disorder described by Spielman and colleagues (Figure 11.1) rests on the role of perpetuating factors such as these that lead to a chronic, vicious cycle of tension and arousal around sleep in predisposed individuals [3]. This model, “The 3 P’s: Predisposing, Precipitating, and Perpetuating Factors,” works well to account for much of what we see clinically in the development and recovery from Psychophysiologic insomnia.

The evolution of psychophysiologic insomnia. Predisposed individuals enter into a vicious cycle of perpetuating factors that lead to Psychophysiologic insomnia
One concept widely embraced in the insomnia literature is that some people are more likely to develop Psychophysiologic insomnia than others. These “predisposing factors” are still unclear, however. A large majority of patients in treatment for chronic insomnia have increased levels of anxiety and/or depression [4–6], though these symptoms do not often meet the diagnostic criteria for disorders. A distinguishing characteristic of Psychophysiologic insomnia is that anxiety symptoms and dysphoria or hopelessness tends to be nearly exclusively (or disproportionately) about sleep patterns, rather than other life issues.
Current research consistently identifies elevated levels of arousal in adults with chronic insomnia. Insomnia sufferers have been found to have elevated electromyographic activity [7], increased cortisol levels [8] and metabolic rates [9], and higher resting heart rates [10] compared with normal sleepers. Further, the electroencephalographic (EEG) activity of insomniacs during sleep is characteristically too “awake” – beta activity is increased, and delta (slow wave) activity is diminished throughout the night compared with normal sleepers [11]. Recent neuroimaging studies have also added evidence that insomniacs display overactivation of many brain areas that regulate body and emotional tone, and underactivation of executive functioning areas [12]. It is unclear whether these changes are what predispose individuals before their insomnia develops, or arise as a consequence of the disturbed sleep pattern, but the current research suggests that physiologic hyperarousal is a common profile among adults with chronic primary insomnia. Indeed, these altered physiologic patterns may be part of the perpetuating factors that undercut the patient’s ability to get sleep back on track.
Clinically, we see these insomniacs as individuals who are primed to be more physically and emotionally reactive to stress, and sleep disruption tends to be a barometer for how stressed they are feeling. Individuals who are predisposed to this stress-reactivity report that a wide range of life events, physicaland psychological stressors act as triggers that precipitate sleep disruption [13]. Higher subjective stress burden has been shown to be inversely correlated with the delta power of non-REM sleep [14]. In fact, insomniacs differ from other sleepers most clearly in their poor response to stressful events, not the severity or frequency of exposure to stressors [15]. A wide range of physiologic factors may contribute to the vulnerability to sleep disturbance in this population: a hypersensitive HPA axis, dysfunction in the sleep homeostatic system; or dysregulation of emotional control mechanisms [16]. One or more of these specific mechanisms may be involved in the generation of Psychophysiologic insomnia. Ultimately it appears that these insomniacs are biased toward chronicity by their fundamental difficulty in regulating physiologic arousal levels.
Identification of Patients with Psychophysiologic Insomnia
The most important element in the clinical assessment of individuals with insomnia complaints is a thorough sleep and medical history. Insomnia symptoms may be complex, emerging from different sources from night to night, and across time. Medications, substances, medical disorders, sleep environment, or scheduling issues may add to the symptoms of insomnia that patients present. The features of Psychophysiologic insomnia must be discerned between, with and among all the patients’ presenting sleep complaints. A systematic clinical assessment to identify intrinsic or extrinsic conditions that may be contributing to sleeplessness is essential, and insomnia secondary to other conditions should be addressed directly.
A history of escalating overconcern regarding sleep is usually able to be identified outright. Indeed, many patients are desperately aware that their anxiety about sleep is effectively sabotaging their ability to sleep. Occasionally, a patient may be completely unaware that they are anxious or tense, and misattribute sleeplessness to other causes. A fairly typical history for Psychophysiologic insomnia is a patient who has had occasional problems initiating sleep in the past when stressed, but always managed to stay asleep once sleep began. Then, during an extended bout of initial insomnia 2 years ago, the patient became preoccupied with their problem sleeping and began having trouble returning to sleep after waking to urinate. These normal awakenings were perceived as problematic, and as the patient’s focus on sleep intensified, their sleep initiation problem expanded to include sleep maintenance symptoms.
What makes Psychophysiologic insomnia different from the other Insomnia conditions is the essential role of the patient’s psychological and physiological arousal levels in the creation of the symptoms. So in addition to the routine elements of a sleep and medical history, the clinician should develop a longitudinal picture of the patient’s ability to sleep in novel or stressful situations. The patient may recognize themselves as someone who tends to get “revved up” by life events in general, but many observe their trouble unwinding only in relation to their attempt to sleep. Still other patients do not perceive themselves to be anxious or “wound up,” but simply “too awake.” The clinician should explore whether the sleep complaints arise in the context of background of stress-reactivity, and how much insight the patient has about this aspect of themselves. Did this patient have difficulty transitioning to sleep as a child? Was this patient a “light” sleeper, sensitive to variations in their sleep environment? Did this patient feel sleep came easily before the problem of insomnia began, or have they always second-guessed their ability to sleep well? How was their sleep affected on nights before stressful or exciting events? Are they aware of the timing for sleep that really suits them (i.e., morningness vs. eveningness) or do they feel they “never sleep well”?
A comprehensive approach to understanding both the behaviors and the attitudes and beliefs around sleep issues has been demonstrated to be very important to adequately address chronic insomnia symptoms ([17] Morin 2004). Morin and colleagues have developed a variety of assessment tools that identify the cognitive distortions (e.g., “if I don’t sleep 8 hours, I won’t be able to function at all”), and misperceptions related to sleep. Most insomniacs carry dysfunctional patterns of thinking and feeling about sleep that represent a real inner barrier to improved sleep. Informed clinicians can readily identify these patterns, and help patients to change them by using these assessment tools (see Appendix for Dysfunctional Beliefs and Attitudes about Sleep). This type of history takes time, and not all clinicians may feel able or willing to use this approach. However, the investment of time to identify this information will usually allow the clinician to more quickly and precisely correct a patient’s approach to sleep, and develop a more effective treatment plan.
As important element of an insomnia assessment is the use of outpatient self-report forms to document sleep patterns over the 24-h day. Patients may be annoyed by the task, but sleep logs (sleep diaries) are essential to the process of ongoing assessment of their sleep at home, and its response to treatment. There are many formats that can be used; the authors prefer a format that shows blocks of sleep visually, and includes a way to indicate what time a patient got into bed relative to when they first attempted to fall asleep (i.e., would show the time spent reading in bed before “lights out”). It is not necessary to have patients complete an exhaustive diary of meals, activities, and mental states, but patients can include relevant details when they recognize the potential to affect their sleep (e.g., “was very stressed after phone call”). Patients’ subjective reporting on sleep logs is well-supplemented with actigraphy. Wrist-worn actigraphs are inexpensive, durable and lightweight devices that sensitively and continuously record movement activity and rest periods that correspond well to wake and sleep on polysomnography. The patient wears the actigraph on the nondominant wrist like a wrist watch, and objective measurements of activity levels can be collected for up to 4 weeks, allowing an objective assessment of their longitudinal sleep patterns at home [18]. Sleep logs, even without actigraphy, are more accurate and informative than a verbal report of their sleep patterns, particularly because patients tend to overestimate or globalize their lack of sleep (e.g., “It always takes me 3 h to fall asleep”). With consistent use, sleep logs will facilitate collecting data on circadian, sleep hygiene, and sleep-timing patterns that will guide the treatment process. In fact, weekly logs may initially provide the only “proof” to a patient that there are incremental improvements in their sleep patterns.
If the diagnosis of Psychophysiologic insomnia is clear, a nocturnal polysomnogram is not needed. However, one may be needed to rule out other underlying sleep disorders. Patients with chronic insomnia are often surprised when they are able to sleep in the testing environment, and this can be a useful outcome measure as well – to reassure them that their brain can generate effective sleep, even under potentially adverse conditions. This information is useful for the clinician as well – Psychophysiologic insomnia is generally associated with less difficulty sleeping in new environments. Polysomnograms may reveal physiologic clues to the patient’s history of sleeplessness: surges in heart rate with awakenings may correspond with anxiety or pain; shortened REM sleep-onset latency may be seen in patients with residual (or prodromal) major depression; a relative excess of light NREM sleep (N1, N2) and “spindling” will betray exposure to benzodiazepines. Patients may focus upon the findings for clues that their brain is “not broken,” and the clinician should be aware that patients may really benefit from hearing the good news about a relatively normal polysomnogram.
Finally, if a behavioral treatment program has not produced significant improvement after several weeks of patient-compliant therapy then a polysomnogram would be indicated to rule out underlying organic disturbance that may have been missed or underreported by the patient. These studies sometimes reveal significant sleep apnea or other primary sleep disorders whose treatment may fully resolve the subjective sleep complaints or accelerate the patient’s insomnia therapy.
Treatment of Patients with Psychophysiologic Insomnia
Nonpharmacologic Tools
Several longitudinal studies have demonstrated the most effective long-term treatment for Psychophysiological insomnia is Cognitive Behavioral Therapy (CBT) [19]. CBT protocols for insomnia are described in this text (Chap. 22) and comprehensive guides to treatment are also available elsewhere [17, 20]. A summary of the patient instructions and underlying core cognitive and behavioral strategies is outlined in Table 11.1. CBT treatment is used to systematically eliminate the beliefs and behaviors that undermine the patients’ normal sleep process. Because the traditional CBT protocols developed for insomnia take several weeks, and there are a limited number of Behavioral Sleep Medicine clinicians trained in this therapy, clinicians have worked to develop an abbreviated version of CBT that is similarly effective, and can be delivered by primary care clinicians. Edinger and colleagues [21] have demonstrated that even two sessions of CBT delivered by family practitioners may also significantly improve sleep quantity and quality. Patients given this abbreviated version of CBT reported 50% less wake after sleep onset time 3 months after the intervention, a significant improvement over patients given sleep hygiene instructions alone. A more recent study that attempted to define the “dose–response” curve of CBT for insomnia suggests that four individual, biweekly sessions may represent the optimal dosing for the CBT intervention tested [22]. It is clear that even brief courses of CBT can translate into a valuable tool for the long-term recovery from insomnia.
In addition to CBT, many insomnia patients may greatly benefit from practices designed to evoke states of relaxation. Herbert Benson described the “relaxation response” and its benefits for reducing stress on the cardiovascular system many years ago [23]. Similarly, relaxation techniques have been applied in the treatment of insomnia to reduce the somatic and/or cognitive hyperarousal coincident with their sleep disturbance. Some studies have demonstrated that relaxation therapy is moderately effective for sleep maintenance insomnia [24, 25], while other studies have shown more robust benefits for insomniacs [26]. There is little evidence that one method is superior to others, and it is likely that the most critical determinant to success is that no matter what type of method used, the patient must learn to master the technique before applying it to the presleep period. One validated instrument specific to insomnia is the Pre-Sleep Arousal Scale (Table 11.2) which may used to assess a patient initially, and as they begin to apply relaxation tools during the sleep period [27]. Recent research has demonstrated there is value to combining CBT for insomnia with mindfulness-meditation [28] in reducing sleep symptoms, as well as presleep arousal levels. In addition, the overall level of arousal was subjectively reduced with this intervention in these insomniacs.
Another nonpharmacologic tool that may be useful in treatment of insomnia is EEG-Biofeedback, or Neurofeedback (NFB) training [29]. There are several types of NFB training currently available, all of which measure cortical EEG in patients while awake, and provide real-time visual or auditory feedback to the patient about their EEG patterns to facilitate a renormalization of their brain states. For instance, patients can learn to produce more alpha waves in their EEG when their success is coupled to an arrow’s movement toward a target on a graphic display. The majority of NFB systems are modeled after the pioneering work of Barry Sterman [30] who demonstrated that cats can learn to voluntarily enhance their sensorimotor rhythm (SMR, 12–14 Hz activity) in their wake EEG through operant conditioning paradigms. These cats demonstrated significant changes in their sleep EEG (increase in sleep spindles, and in quiet sleep time), suggesting that strengthening the thalamocortical rhythms through NFB training can benefit sleep systems.
To date however, only two studies have evaluated the effect of NFB training on sleep in insomniacs. In 1981, Hauri and colleagues applied three biofeedback methods to a group of 48 insomniacs that he randomized as follows: (1) frontalis muscle EMG feedback, (2) frontalis muscle EMG training followed by theta frequency band EEG NFB; (3) SMR NFB training; or (4) control [31]. Thus, this study intended to evaluate the efficacy of somatic relaxation (frontalis muscle EMG) training, and two types of NFB training or both, on insomniacs. As with Sterman’s cats, the amount of learning in SMR NFB training correlated significantly with sleep improvement. Interestingly, the initial somatic tension levels (frontalis EMG measured 5 min after lights out on NPSG) correlated positively with sleep improvement for the EMG-training groups, but negatively with sleep for the SMR group. Essentially, the authors identified that this group of insomniacs were not uniformly tense, and that the benefits of the biofeedback measures were evident only when patients were randomized to the group appropriate to their specific deficiencies. A replication study conducted by the same group [32] further corroborated that insomniacs who were tense and anxious benefited from theta frequency band EEG-biofeedback (NFB training that facilitates relaxation), while those who were relaxed at intake but still could not sleep benefited only from SMR training (NFB training that strengthens the sleep system). These studies were the first to characterize that insomniacs have distinct pretreatment physiologic profiles, and that selective application of appropriate biofeedback protocols may significantly benefit their sleep.
Recently, we have applied a new type of NFB training in insomnia patients that utilizes a more global approach to EEG training (Zengar, Neurocare system). This NFB system is based on nonlinear dynamical (chaos) control theory that predicts that reducing “turbulence” in EEG will lead to renormalization of brain states. This system measures EEG across the entire range of frequencies (0.5–60 Hz), and provides real-time feedback about the degree of emergent variability (“revving” or “turbulence”) to the patient as brief interruptions in music being played. This NFB system has several advantages, including eliminating the need for a diagnostic quantitative EEG, and there is less potential for side effects than with traditional targeted EEG-biofeedback. We have seen significant clinical improvement in a diverse array of insomnia patients such that the majority of patients’ sleep symptoms are resolved after 16–20 thirty-minute training sessions [33]. Further research is needed to validate this and other more traditional NFB protocols for insomnia treatment, but it is likely these nonpharmacologic tools represent potent technologies that may greatly enhance physiologic recovery from chronic insomnia.
Pharmacologic Treatments
Hypnotic medications may initially be necessary to help a patient begin sleeping regularly again. Anxious patients make poor students, and compliance with CBT and other behavioral regimens will be a challenge for patients desperate to sleep. For these patients, a nightly hypnotic may be the best first step in treatment so that the patient may experience regular, predictable sleep periods again. The choice of hypnotic medications should be made based upon the patient’s pattern of insomnia: short-acting hypnotics for initial insomnia, hypnotics with longer half-lives for problems with sleep maintenance. For a complete discussion of hypnotic medications and their use in insomnia patients, the reader is referred to Chap. 23 of this text. Once the patient is sleeping again, they can successfully participate in CBT protocols, and hypnotics can then be gradually tapered off and discontinued. Of course, there are many patients who have already tried an exhaustive list of hypnotics, but are still not sleeping well. Though these patients may also be desperate to sleep, their despair may actually make them more likely to commit to nonpharmacologic practices if offered in a supportive and systematic way. Ultimately, the challenge for many insomniacs is to rediscover the confidence they have lost that they can sleep, and deal with occasional bouts of sleeplessness on their own. For many chronic insomniacs, successful treatment may be predicated on having access to a suitable hypnotic as a “back-up plan” for the rare night they feel beyond their limit to tolerate sleep issues.
References
Dew MA, Reynolds CF, Monk TH et al (1994) Psychosocial correlates and sequelae of electroencephalographic sleep in healthy elders. J Gerontol 49:8–18
Jefferson CD, Drake CL, Sofield HM et al (2005) Sleep hygiene practices in a population-based sample of insomniacs. Sleep 28(5):611–615
Spielman AJ (1987) A behavioral perspective on insomnia treatment. Psychiatr Clin North Am 10:541–553
Edinger JD, Sullivan RJ, Bastian LA, Hope TV, Young M, Shaw E et al (2000) Insomnia and the eye of the beholder: are there clinical markers of objective sleep disturbances among adults with and without insomnia complaints? J Consult Clin Psychol 68:586–593
Espie CA (1991) The psychological treatment of insomnia. Wiley, Chichester, United Kingdom
Morin CM, Stone J, Trinkle D, Mercer J, Remsberg S (1993) Dysfunctional beliefs and attitudes about sleep among older adults with and without insomnia complaints. Psychol Aging 8:463–467
Haynes SN, Follingstad DR, McGowan WT (1974) Insomnia: sleep patterns and anxiety level. J Psychosom Res 18(2):69–74
Vgontzas AN, Bixler EO, Lin HM et al (2001) Chronic insomnia is associated with nyctohermeral activation of the hypothalamic-pituitary-adrenal axis: clinical implications. J Clin Endocrinol Metab 86(8):3787–3794
Bonnet MH, Arand DL (1995) 24-Hour metabolic rate in insomniacs and matched normal sleepers. Sleep 18(7):581–588
Stepanski E, Zorick F, Roehrs T et al (1988) Daytime alertness in patients with chronic insomnia compared with aympotmatic control subjects. Sleep 11(1):54–60
Perlis ML, Smith MT, Andrew PJ et al (2001) Beta/gamma EEG activity in patients with primary and secondary insomnia and good sleeper controls. Sleep 24(1):110–117
Nofzinger EA, Buysse DJ, Germain A et al (2004) Functional neuroimaging evidence for hyperarousal in insomnia. Am J Psychiatry 161(11):2126
Bonnet MH, Arand DL (2003) Situational Insomnia: consistency, predictors, and outcomes. Sleep 26(8):1029–1036
Hall M, Buysee D, Nowell P, Nofzinger E, Houck P, Reynolds C, Kupfer D (2000) Symptoms of stress and depression as correlates of sleep in primary insomnia. Psychosom Med 62:227–230
Morin CM, Rodrigue S, Ivers H (2003) Role of stress, arousal, and coping skills in primary insomnia. Psychosom Med 65(2):259–267
Drake CL, Roth T (2006) Predisposition in the evolution of insomnia: evidence, potential mechanisms, and future directions. Sleep Med Clin 1(3):333–349
Morin CM, Espie CA (eds) (2004) Insomnia: a clinical guide to assessment and treatment. Springer, New York
Chesson AL, Anderson HK, WM DD, Johnson S, Littner M et al (2000) Practice parameters for the evaluation of chronic insomnia. Sleep 23:237–241
Morin CM (2006) Combined therapeutics for insomnia: should our first approach be behavioral or pharmacological? Sleep Med 7(Suppl 1):S15–S19
Perlis M, Jungquist C, Smith M, Posner D (2005) Cognitive behavioral therapy for insomnia: a session-by-session guide. Springer, New York
Edinger JD, Sampson WS (2003) A primary care ‘friendly’ cognitive behavioral insomnia therapy. Sleep 26:177–182
Edinger JD, Wohlgemuth WK, Radtke RA, Coffman CJ, Carney CE (2007) Dose-response effects of cognitive-behavioral insomnia therapy: a randomized clinical trial. Sleep 30(2):203–212
Benson H, Greenwood MM, Klemchuk H (1975) The relaxation response: psychophysiologic aspects and clinical applications. Int J Psychiatry Med 6(1–2):87–98
Morin CM, Colecchi CS, Stone J, Sood R, Brink D (1999) Behavioral and pharmacological therapies for late-life insomnia: a randomized clinical trial. JAMA 281:991–999
Chesson AL, Anderson WM, Littner M, Davila D, Hartse K, Hurwitz TD et al (1999) Practice parameters for the non-pharmacologic treatment of chronic insomnia. Sleep 22:1128–1133
Jacobs GD, Benson H, Friedman R (1996) Perceived benefits in a behavioral-medicine insomnia program: a clinical report. Am J Med 100(2):212–216
Nicassio PM, Mendlowitz DR, Fussell JJ, Petras L (1985) The phenomenology of the pre-sleep state: the development of the Pre-Sleep Arousal Scale. Behav Res Ther 23:263–271
Ong JC, Shapiro SL, Manber R (2008) Combining mindfulness meditation with cognitive-behavior therapy for insomnia: a treatment-development study. Behav Ther 39(2):171–182
Cortoos A, Verstraeten E, Cluydts R (2006) Neurophysiological aspects of primary insomnia: implications for its treatment. Sleep Med Rev 10(4):255–266
Sterman B, Howe RC, MacDonald LR (1970) Facilitation of spindle-burst sleep by conditioning of electroencephalographic activity while awake. Science 167:1146–1148
Hauri PJ (1981) Treating psychophysiologic insomnia with biofeedback. Arch Gen Psychiatry 38(7):752–758
Hauri PJ, Percy L, Hellekson C, Hartmann E, Russ D (1982) The treatment of psychophysiologic insomnia with biofeedback: a replication study. Biofeedback Self Regul 7(2):223–235
Okunola O, O’Malley E, O’Malley M (2007) Effectiveness of neurofeedback training in chronic insomnia. Sleep 30:A265
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2010 Springer Science+Business Media, LLC
About this chapter
Cite this chapter
O’Malley, M.B., O’Malley, E.B. (2010). Psychophysiological Insomnia. In: Attarian, H., Schuman, C. (eds) Clinical Handbook of Insomnia. Current Clinical Neurology. Humana Press, Totowa, NJ. https://doi.org/10.1007/978-1-60327-042-7_11
Download citation
DOI: https://doi.org/10.1007/978-1-60327-042-7_11
Published:
Publisher Name: Humana Press, Totowa, NJ
Print ISBN: 978-1-60327-033-5
Online ISBN: 978-1-60327-042-7
eBook Packages: MedicineMedicine (R0)