
Abstract
Individuals with autism spectrum disorders (ASDs) have social deficits which can lead to academic, occupational, and psychiatric difficulties. These individuals face multiple social challenges during the course of their lives which are exacerbated by difficulties understanding, processing, and describing social and emotional content in themselves and others. Self-report of such experiences is challenging for many individuals with ASD. As a result, there has been increasing interest in observing responses to social and nonsocial experiences across multiple levels of analysis, including measurement of psychophysiological systems related to homeostatic regulation. The study of psychophysiological arousal patterns in children and adults with ASDs during social stress provides information about the nature of, and individual differences in, emotional reactivity that is difficult, if not impossible, to achieve via self-report. However, psychophysiological markers of social stress in children and adults with ASDs (including sympathetic, parasympathetic, and hormonal) have yielded inconsistent results. In this chapter, we attempt to disentangle why these inconsistencies have emerged, within the context of the complex relations between these markers.
Access provided by Autonomous University of Puebla. Download reference work entry PDF
Similar content being viewed by others

Keywords
- Autism Spectrum Disorder
- Heart Rate Variability
- Salivary Cortisol
- Social Stress
- Respiratory Sinus Arrhythmia
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
According to the Diagnostic and Statistical Manual of Mental Disorders – 4th Edition, Text Revision (DSM-IV TR) (American Psychiatric Association 2000), autism spectrum disorders (ASDs) are characterized by qualitative impairments in socialization, communication, and circumscribed interests, including stereotypical behavior patterns and behavioral rigidity to changes in routine. Although these symptomatic features are well established, it is unclear whether their origin lies simply in the absence of appropriate social skills and behavioral flexibility or arises from difficulties in psychophysiological arousal and regulation. Psychophysiological factors implicated in ASDs can cause or contribute to significant problems in modulating arousal to social and sensory stimuli that are novel or unpredictable (Dawson 1991; Dawson and Lewy 1989; Kinsbourne 1987; Ornitz and Ritvo 1968; Ornitz 1989), resulting in behavioral and psychophysiological response patterns of either overarousal (Hutt et al. 1964) or under-arousal (DesLauriers and Carlson 1969). According to these arousal modulation theories of ASDs, both anxious and agitated response characteristic of overarousal and passivity and lethargy characteristic of under-arousal interfere with this population’s ability to attend to, process, and interact with the environment. These difficulties result in the failure to develop normative behaviors and skills compared to their typically developing peers (Lord and McGee 2001; Prizant et al. 2003; Siegel 2003).
Psychophysiological markers of arousal are measured as changes in physical systems that relate to emotions and stress in an individual. Measurements of these markers are related to internal mental states that are then associated with specific stimuli. These markers are important tools that aid in our understanding of the nuanced responses to social and nonsocial stress in adults and children with ASDs. A stressor is any stimulus or circumstance that compromises an individual’s physical or psychological well-being or that results in the individual (the organism) adjusting to some other level or state (Lazarus and Folkman 1984). Psychophysiologists have studied physiological responses to attention-demanding, social, and emotional stressors. However, the focus of this chapter will be on social stressors due to the hypothesized relation between deficits in social functioning and difficulties with physiological regulation among adults and children with ASDs. The stress response typically relates to three periods of interaction between the stressor and the individual’s response: (1) the period before the stressful event occurs, (2) the stressor’s occurrence, and (3) after the stressor occurs during which the individual may experience some of the residual effects of the event. Social stressors can involve visual or auditory components with the ultimate result of producing a state of internal unrest with regard to the social presence and/or influence of others.
Along with self-reports of subjective experiences during social events, psychophysiological markers of arousal can elucidate how responses to social stimuli are perceived by those with ASDs compared to those without ASDs. These measurements play a key role in this area as children and adults with ASDs have difficulties processing and identifying emotions (Hill et al. 2004; Losh and Capps 2006; Rieffe et al. 2007), making assessment of response to social events difficult. The ability to identify internal states and psychophysiological arousal may have applied value, helping to tailor interventions and therapies effectively to individuals. Detecting heightened physiological arousal may also constrain the ability of persons with ASDs to benefit from behavioral and social interventions that do not address this psychophysiological reactivity. For example, if an individual with an ASD is identified as being overaroused, stress reduction techniques such as relaxation training (Cautela and Groden 1978) and cognitive picture rehearsal (Groden et al. 1989) might be used as preparatory steps to any further intervention. Thus, understanding of psychophysiological arousal in children and adults with ASDs has significant treatment implications, either in precluding some techniques or investigating others that may have applicability. Psychophysiological studies can also help address the question of whether there are subgroups of individuals with ASD for whom social anxiety causes additional impairment, as opposed to the view that the individuals with ASD may be generally under-responsive to social information. Moreover, because these psychophysiological stress response systems are active from early in development, such studies can elucidate the developmental course of arousal and reactivity in this population.
In this chapter, we focus our attention on commonly studied psychophysiological markers of arousal measured in children and adults with ASDs in response to social stress, which include autonomic and hormonal markers. We will also discuss responses to nonsocial stressors as they are relevant to this discussion. Other measurements of psychophysiology, including neuroimaging and eye movements, are covered in other chapters of this text. We will also discuss how relations between these markers, along with self-reports of arousal, can further enhance our understanding of psychophysiological and emotional reactivity in this population. Studies of these markers may also lead the discovery of mechanisms underlying arousal to social stress in ASDs. In evaluating the utility of each of the psychophysiological measures listed below, we recognize difficulties comparing results across studies due to (1) different methods of measuring each marker, (2) the use of different tasks used to elicit social stress between studies, (3) comparisons across different age groups, (4) the heterogeneity of symptoms and behaviors in ASDs, and (5) the types of comparison group chosen.
Heart Rate Variability
Cardiorespiratory measures, including heart rate (HR), heart rate variability (HRV), and respiratory sinus arrhythmia (RSA), have been widely used in studies of child psychopathology, including some research on ASDs. HRV refers to the beat-to-beat alterations in HR and encompasses both sympathetic and parasympathetic influences on the heart. Reduced HRV has been used as a marker of reduced parasympathetic nervous system (PNS) activity. RSA, a phenomenon defined as periodic variation in HR due to respiratory activity, also reflects central nervous system influences on the heart. RSA is also calculated as beat-to-beat HRV and is mediated by inhibitory signals to the sinoatrial node from brainstem nuclei via the vagus nerve and reflects PNS activity. While RSA and HRV are measuring similar phenomena, RSA measures a specific periodicity or oscillation within the broad range of HRV. Although these are separate terms, due to their similar constructs, and for simplicity, we will use the term RSA to describe both.
Besides its implication in direct cardiovascular regulation, RSA measurements have been associated with emotional regulation and stimulus orientation at multiple developmental levels. Specifically, lower baseline RSA is associated with decreased ability to engage with the environment and is associated with emotional traits such as depression and anxiety (Beauchaine 2001). Higher baseline RSA is thought to indicate a readiness to engage with or respond to environmental demands, including aspects of the social environment. For example, RSA has been notably elevated during synchronous mother-infant interactions and positive affect (Field and Diego 2008), providing support for the Porges “social engagement system” model (Porges 2001). Low baseline RSA has been found in prenatally depressed mothers and their infants, as well as in children with ASDs (Field and Diego 2008; Ming et al. 2005). With regard to RSA reactivity, moderate decreases in RSA in response to a stressor are considered normative and are associated with increased engagement and preparedness to respond. An excessive decrease in RSA, however, is associated with emotional lability and decreased ability to self-regulate in response to stress (Beauchaine 2001). How appropriate versus excessive decreases in RSA are defined is specific to each individual study. We will primarily focus attention on RSA reactivity to social stress as a marker of self-regulation and how this reactivity differs between ASD and non-ASD groups. We will also discuss baseline RSA as it relates to reactivity to social stress when applicable within a particular study.
Studies in non-ASD populations have revealed a consistent decrease in RSA from baseline in adults undergoing paradigms involving worry or social evaluative stress (Bosch et al. 2009; Cervantes Blasquez et al. 2009; Hammel et al. 2010; Pieper et al. 2007; Thayer et al. 1996; Thayer and Brosschot 2005). However, varying protocols used to elicit changes in RSA, whether socially related or not, limit comparison between studies. Few studies have examined measures of RSA at baseline or in response to social events and stimuli in children and adults with ASDs. Bal and colleagues (Bal et al. 2010) found that 7–17-year-old children with ASDs without significant cognitive deficits had lower baseline RSA when compared to controls. They also explored how this lower baseline RSA in the ASD group related to an affective facial recognition task. They found that within the ASD group, those with higher baseline RSA showed more rapid recognition of facial emotions than those with lower baseline RSA, reflecting increased social engagement based due to increased PNS activity in those with ASDs. Vaughan Van Hecke and colleagues (2009) showed similar findings in children with ASDs ages 8–12. They found lower RSA levels at baseline and while watching videos of familiar people, unfamiliar people, and a moving object when compared to typically developing controls. In particular, the ASD group exhibited decreased RSA when watching the video of an unfamiliar person, while the controls maintained baseline RSA levels. Higher baseline RSA in the ASD group was related to higher social skill ratings and fewer problem behaviors. Thus, the social difficulties of children with ASDs may be characterized by specific mobilization to unfamiliar people and support Porges theory that increased baseline PNS activity is associated with increased social engagement.
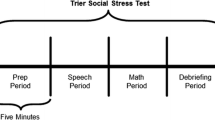
In a study of higher-functioning children with ASDs, Levine and colleagues (2012) found no difference in RSA between a group of 19 school-age (8–12 years old) children with ASDs and a typically developing control group at baseline and during all phases of the Trier Social Stress Test (TSST) (Kirschbaum et al. 1993). The TSST consists of a story completion task and serial subtractions in front of adult evaluators with the goal of inducing evaluative stress. Thus, this paradigm provides a uniquely “real-life” scenario where performance in a task is considered within the context of social evaluation. There were also no differences in RSA following the task, indicating that children with high-functioning ASDs may experience the saliency of social stress in similar ways to those without ASDs and have similar anticipation and recovery from the TSST. As part of their protocol, Levine and colleagues added a third stressor, which involved a task where participants attempted to trace a star through a reflection in a mirror with a buzzer that sounded with errors (Lafayette Instrument Company, Mirror Tracer). Despite a lack of difference in RSA between the groups, both demonstrated significant RSA decreases (Fig. 1) during the storytelling and math sections of the TSST but recovery during the star tracing and debriefing. This pattern may indicate that the story and math sections were emotionally stressful secondary to social evaluation, while the star tracing was not. Previous studies have demonstrated a greater decrease in RSA in non-ASD child samples during the star tracing when compared to listening to an argument (Hinnant and El-Sheikh 2009). However, direct comparison between these studies is difficult since the social stressors in each (story completion/serial subtractions vs. listening to an argument) are quite different. These findings from Levine and colleagues are very similar to a study examining RSA in children with social phobia (SP) and healthy controls who were in the same age range as those in Levine and colleagues and underwent the traditional TSST without the star tracing (Schmitz et al. 2011) (Fig. 2). Thus, across these two studies, children with ASDs, SP, and controls had similar PNS reactivity to a common stress paradigm, indicating the TSST may be a useful paradigm in testing physiological reactivity to social stress in those with ASDs. The lack of difference in RSA reactivity between the ASD group and controls in the Levine and colleagues study is somewhat unexpected as they hypothesized that the ASD group would have a greater decrease in RSA, due to their greater vulnerability to a social stressor, when compared to controls. An alternative hypothesis that the ASD group would show a lessened or no decrease in RSA in response to the TSST could be argued due to their deficits in “Theory of Mind” capabilities or the ability to understand the thoughts and motivations of others (Baron-Cohen et al. 1985). Thus, the ASD group would not be as aware of the social stress induced by the examiners and show less of a psychophysiological stress response. However, this alternative hypothesis is also not supported since there was no difference in RSA between the ASD group and controls. Further studies are required to understand this response better.

RSA in children with ASDs undergoing the TSST. Comparison of RSA between 19 children with ASDs (HFA) versus 11 controls (COMP) undergoing the TSST. Story prep is the preparation of the story, story is the telling of the story, math is serial subtractions, and tracing is the tracing of a star through a mirror. Debrief is a period where examiners tell the participants how well they performed and normalized the experience. Adjust 1 and adjust 2 are baseline and recovery, respectively (Printed with permission from Levine et al. 2012)

RSA in children with social phobia (SP). RSA at baseline, reactivity, and recovery while undergoing the TSST in a group of 30 children with social phobia (SP, n = 30) and healthy controls (HC, n = 26). Prep is preparation for the TSST, TSST1 is the storytelling task, TSST2 is the serial subtraction task, and Rec 1–3 are recovery periods where children watched pictures of landscapes on a computer screen for relaxation and answered questions on their performances (Printed with permission from Schmitz et al. 2011)
There are limited studies of autonomic reactivity and recovery in early childhood. Further understanding of physiological measures to social stress in young children with ASDs could aid in understanding developmental processes in these children and aid in selecting interventions based on psychophysiological reactivity. Corona et al. (1998) reported that 3–5-year-old children with autism failed to show an HR response to the feigned distress of an examiner, a perceived social stressor, as compared to a matched sample of children with developmental delays that showed an overall decrease in HR in response to the examiner’s distress display. In related work, Sigman and colleagues (2003) reported that both young children with ASDs and a matched group of children with developmental delays showed decreased HR when viewing a video of babies laughing or crying. While these studies did not examine measures of HRV such as RSA, they do suggest that experimental design may affect psychophysiological outcomes due to differences in the intensity or salience of the stimuli.
Electrodermal and Sympathetic Nervous System Activity
Electrodermal activity (EDA) is a measure of sympathetic nervous system (SNS) activity that reflects a “fight or flight” response in times of high emotional arousal. It is a measurement of autonomic innervation of eccrine sweat glands which are modulated by postganglionic sympathetic fibers (Sato et al. 1989). Since eccrine sweat glands receive only excitatory sympathetic nerve impulses, EDA constitutes a purely sympathetic response. EDA is noninvasive and can be measured using adhesive leads placed on the fingertips and provides a sensitive and convenient measure for assessing alterations in arousal associated with emotion, cognition, and attention (Critchley 2002). Since EDA can be elicited within 2–4 s of a stimulus with similar recovery time, it can be used to measure the affective intensity of a stimulus.
There is evidence that the SNS is more active during social evaluative stress in adults and children without ASDs (Bosch et al. 2009; Cervantes Blasquez et al. 2009; Hammel et al. 2010; Kudielka et al. 2004; Pieper et al. 2007; Smeets 2010; Yoshie et al. 2009). Similar to RSA and HRV, EDA findings in those with ASDs are inconsistent and utilize different protocols/stimuli to elicit physiological responses. Furthermore, most of these studies do not use social performance paradigms and have led to mixed results. For example, no differences in EDA between children with ASDs and controls were found in response to pleasant, unpleasant, and neutral photographs using the International Affective Picture System (Ben Shalom et al. 2006). Care was taken in this study to exclude images of human faces as the study subjects had difficulties processing facial expressions depicting emotion which could have led to differential responsiveness to pictures of people. In contrast, Hirstein and colleagues found that, compared to controls, children with ASD had increased EDA in multiple real-life environments (sitting quietly, interacting with parent, playing with preferred toys or games), but not in response to looking at a person (Hirstein et al. 2001). This difference in EDA response to a person versus inanimate object suggests a possible lack of social responsiveness to interactions with others. Other studies have found higher baseline EDA in children with ASD, but no differences when compared to controls in response to various auditory stimuli (Palkovitz and Wiesenfeld 1980).
Utilizing more socially relevant paradigms, studies have investigated EDA in response to pictures of people’s faces with varying degrees of eye contact. In their first study, Kylliainen et al. (Kylliainen and Hietanen 2006) compared EDA in children with ASDs to controls while viewing faces with direct gaze (eye contact) and averted gazes. The children with ASDs had a greater EDA response to the faces with direct gaze compared to the averted gaze, but there was no difference between the two conditions in the control group. In a subsequent study (Kylliainen et al. 2012), the stimuli were modified to show varying degrees of eye openness in the pictures (closed to wide open). Children with ASDs had attenuated EDA to faces with closed eyes and increased EDA as a function of the degree of eye openness. The controls once again did not have significant differences in EDA as a result of the eye conditions. In a subsequent study with increased social valence, Kaartinen et al. (2012) measured arousal via EDA in children with ASDs while viewing a live face of another person with varying degrees of eye gaze (direct gaze, averted gaze, and closed eyes conditions). There was a positive correlation between EDA elicited during direct gaze stimuli with impairments in social skills among children with ASD, but not controls. This was not true, however, for the averted gaze and closed eye conditions. There was no evidence from this study that children with or without ASDs exhibited pronounced autonomic responses to direct gaze in relation to averted gaze or to closed eyes. This finding differs from previous results (Kylliainen and Hietanen 2006) showing enhanced autonomic responses to direct gaze in comparison to averted gaze in children with ASD but could be explained by differing experimental protocols.
In the only study of EDA response in children with ASD to date using a standardized social stressor, Levine and colleagues (2012) found no significant difference in EDA between ASD and control groups during the TSST (Fig. 3). This result complements the finding above that RSA was also consistent across the two groups. There is a rise in the EDA, indicating increased SNS activity, and decreased RSA, indicating decreased PNS activity, during the TSST across both groups. This pattern is suggestive of decreased PNS activity relative to SNS activity in response to social stress, a concept that is similar to measures of “autonomic space” described by Berntson et al. (1991). This trend in EDA is also seen in Schmitz et al. (2011) in their study of stress response to the TSST in children with SP and controls (Fig. 4). As with the similarities in RSA trends between the two studies, similarities in EDA generate more interest in the TSST as a useful paradigm to study social stress in those with ASDs.


EDA in children with social phobia (SP). EDA at baseline, reactivity, and recovery while undergoing the TSST in a group of 30 children with social phobia (SP, n = 30) and healthy controls (HC, n = 26) with same format as Fig. 2. EDA is measured as electrodermal sympathetic index (EDI) by combining skin conductance level, number of nonspecific skin conductance fluctuations, and amplitude of nonspecific skin conductance fluctuations (Printed with permission from Schmitz et al. 2011)
Cortisol Reactivity
Cortisol is a hormone secreted from the adrenal glands via the hypothalamic-pituitary-adrenal axis (HPA). Levels have a diurnal pattern (with highest levels in the morning) and also increase or decrease in response to stress. Differential responsiveness of cortisol either in the diurnal pattern or in response to stress, which can be physical or emotional, has implications for how those with ASDs may exhibit arousal differences at baseline and during a stressor. Although the neuronal inputs to the HPA are vast, the limbic system is linked to emotional reactivity in this system and is often a neuroanatomic area of interest when investigating cortisol response to stress. The HPA axis begins with the secretion of corticotropin-releasing factor (CRF) from the hypothalamus which triggers secretion of adrenocorticotropic hormone (ACTH) from the posterior pituitary gland which leads to secretion of cortisol from the adrenal glands. The many positive and negative feedback mechanisms remain complex; thus, cortisol stress reactivity can be influenced at each of these levels. The ability to collect cortisol in saliva, which is highly correlated with plasma levels (Tornhage 2009), has allowed for its measurement without inducing further stress through collection from the serum through phlebotomy. However, salivary cortisol, as measured alone, cannot inform us about alterations in the HPA axis further upstream from the adrenal glands. Furthermore, collection of CRF requires sampling of cerebrospinal fluid and ACTH requires phlebotomy, deterring their collection in children and adults.
Studies with adults and children without ASDs indicate robust associations between social stress and subsequent elevations in salivary cortisol (Bosch et al. 2009; Buske-Kirschbaum et al. 1997; Rimmele et al. 2009; Smeets 2010). Children with ASDs exhibit greater reactivity in salivary cortisol compared to typically developing controls in response to a nonsocial stressor (mock MRI exposure) in some studies (Corbett et al. 2006), but not others (Corbett et al. 2008, 2009). In those studies using social stress protocols, there was no difference in cortisol reactivity from controls in children with ASDs undergoing a public speaking task (Jansen et al. 2003). One study examining children with high-functioning ASDs found significant elevations in cortisol in response to a social interaction with an unfamiliar peer when compared with a previous interaction with a familiar peer, but no difference if the order of the interactions was reversed (Lopata et al. 2008). Another study found that children with autism who engaged in a social playground paradigm had elevated cortisol levels, with consideration for age and behavioral patterns observed in these children, when compared to controls (Corbett et al. 2010). As with measurement of other markers of arousal in ASD groups (RSA and EDA), conclusions across studies about cortisol reactivity are inconclusive due to variability in stress paradigm utilized and other study variables.
Only two studies to date have utilized the same social stress paradigm, the TSST, in examining cortisol reactivity in children with ASDs. Levine and colleagues (2012) found cortisol reactivity to the TSST (measured via salivary cortisol change scores between pre- and post-TSST samples) was decreased in children with ASDs. The control group, however, had the expected overall increase in cortisol in response to the TSST (Fig. 5). In contrast, Lanni and colleagues (2012) did not find significant differences in cortisol reactivity when comparing 15 children with autism ages 8–12 compared to a typically developing control group (Fig. 6). Despite this null result, the authors noted that the cortisol response for the typically developing children differed significantly from zero (increased), whereas the cortisol response for the children with ASDs did not (no response), showing a similar trend as Levine and colleagues. Again, methodological differences in the assessment of cortisol reactivity may have contributed to these inconsistent results. For instance, in contrast to the study by Levine and colleagues, Lanni and colleagues compared the cortisol levels during the experiment to baseline diurnal samples collected at home. Based on their findings, Lanni and colleagues proposed that the TSST may not be a relevant paradigm to elicit social stress in children with ASDs. However, by incorporating measurements of RSA and EDA reactivity, which resemble patterns seen in clinical and nonclinical samples without ASDs, Levine and colleagues proposed that children with ASDs may perceive social stress during the TSST. Furthermore, Levine and colleagues considered multiple explanations for why children with ASDs have an attenuated cortisol response following the TSST. First, children with ASDs may have hypoactivation of the HPA axis secondary to differential functioning in the amygdala (Schultz 2005) and prefrontal cortex (Kennedy and Courchesne 2008) which have connectivity to the HPA axis and may contribute to its activation. Second, children with HFA may have an attenuated cortisol response secondary to chronic stress experienced through a lifetime of difficulty with social interactions and function. This is modeled from similar findings in adults that experienced adverse events in childhood (Carpenter et al. 2007; Elzinga et al. 2008; Klaassens et al. 2009). This decreased activity of the adrenal glands (also known as hypocortisolism) has been reported in some stress-related states (Rohleder et al. 2004). In children, hypocortisolism has been reported in those with chronic stress (Heim et al. 2000; Fries et al. 2005; Raison and Miller 2003), children reared in institutions (Carlson and Earls 1997) or foster care (Fisher et al. 2006, 2007), boys with attention problems (Susman et al. 2007), clinically depressed maltreated school-age children (Kaufman 1991), boys of low-income depressed mothers (Fernald et al. 2008), post-traumatic stress disorder (Goenjian et al. 1996), and children with prenatal cocaine exposure (Lester et al. 2010). However, caution must be used in this interpretation as cortisol reactivity in children tested in similar paradigms can vary by age, gender, pubertal level, availability of coping resources, and the quality of the parent-child relationship (Gunnar et al. 2009a, b; Jessop and Turner-Cobb 2008).

Cortisol changes in children with ASDs undergoing the TSST. Change score comparisons in salivary cortisol levels from pre-TSST to post-TSST between children with ASDs (HFA) and controls (COMP) (Printed with permission from Levine et al. 2012)

Cortisol changes in children with ASDs undergoing the TSST. Cortisol response (log(nmol/L)) in children with autism (n = 15) and controls (typical, n = 15) undergoing the TSST. S1–S2 is a 20-min rest period. S2–S3 is the TSST including speech preparation, speech delivery, serial subtraction, and debriefing, and S3–S6 is a 60-min rest period (Printed with permission from Lanni et al. 2012)
Future Directions
Further exploration of psychophysiological responses to social stress in children and adults with ASDs across studies requires the development of standardized social stressors. In achieving this goal, it will be imperative to incorporate procedures to help participants acclimate to the measurement. This might include a set of pre-observation activities such as familiarizing the participant with the evaluator, providing a measurement rationale appropriate to the participant’s cognitive level, and introducing the participant to the observation setting and measurement apparatus using modeling, desensitization, and direct instruction as needed. The TSST has components of the above, and further modification could be implemented to make it more applicable to ASD populations.
Combining qualitative and quantitative methods of measurement, using repeated assessments, and studying physiological response to stress in a variety of settings can enhance the study of psychophysiological arousal to social stress in ASDs. Concomitant use of direct observation, survey instruments, and psychophysiological measures enable a rich, multilevel description of an individual’s stress response. For those with verbal abilities, the development of more self-report rating scales of stress in individuals with ASDs will help in the rating of subjective feelings during social stressors. Also, collecting multiple psychophysiological measures of arousal (such as RSA, EDA, cortisol reactivity) can address multiple components of arousal and reactivity in individuals with ASDs (Levine et al. 2012) and lead to the exploration of mechanisms of action that could explain differences in stress responsivity from those without ASDs. Other measures of psychophysiological arousal, such as salivary alpha-amylase, could also be utilized as levels rise in response to both physical and psychological stress in salivary samples (Granger et al. 2007). This would be especially useful in experiments already collecting saliva for cortisol measurements.
In addition, in order to collect data in naturalistic settings (home- and school-based activities), technology to produce discrete sensors to collect psychophysiology has been developed to allow for data collection in more “real-life” scenarios where social stress and interactions occur (Fletcher et al. 2010; Poh et al. 2010). The applied potential for these types of measures is at least twofold. First, research on between-subject variability in responses may identify subgroups of individuals who differentially respond to stimuli and therefore may be more or less responsive to different types or styles of treatment. Second, research on within-subject variation in psychophysiological states or responses may yield information that can result in strategic timing of discrete interventions for the purpose of enhancing coping and learning in individuals with ASDs. Both of these potential applied uses of psychophysiology methods can also be expected to improve our understanding of between- and within-subject differences across development.
Key Terms
-
Autism spectrum disorders (ASDs). A group of developmental disorders characterized by qualitative impairments in socialization, communication, and circumscribed interests, including stereotypical behavior patterns and behavioral rigidity to changes in routine. Included in this category are autistic disorder, Asperger’s disorder, and pervasive developmental disorder not otherwise specified.
-
Psychophysiological markers of arousal. Changes in physical states of body systems that relate to emotions and stress in an individual. Measurement of these can be associated with internal mental states that are associated with specific stimuli.
-
Heart rate variability (HRV). Beat-to-beat alterations in heart rate (HR) and encompasses both sympathetic and parasympathetic influences on the heart. HRV changes during a social stressor can indicate stress in an individual.
-
Respiratory sinus arrhythmia (RSA). A phenomenon defined as periodic variation in HR due to respiratory activity, also reflects central nervous system influences on the heart. It is calculated as beat-to-beat HRV and is mediated by inhibitory signals to the sinoatrial node from brainstem nuclei via the vagus and reflects PNS activity. Decrease in RSA can indicate stress during social situations, and increase can represent increased social engagement.
-
Electrodermal activity (EDA). Skin response to stress that indicates a sympathetic nervous system activity increase or “fight or flight” response.
-
Cortisol. A hormone produced by the adrenal glands which is a part of the hypothalamic-pituitary-adrenal axis (HPA). It is often increased in response to stress.
Key Facts
-
RSA is a marker of PNS activity which is associated with emotional regulation and social engagement.
-
EDA is a marker of SNS activity which is associated with a “fight or flight” response.
-
Both EDA and RSA can be noninvasively measured using adhesive leads placed on the hands and/or chest.
-
Cortisol is a hormone produced by the adrenal glands which often increase in response to stress and can be collected in the saliva.
Summary Points
-
Measurements of RSA, EDA, and cortisol reactivity in children and adults with ASDs undergoing social stressors have revealed varying results.
-
These varying results may be secondary to different experimental protocols used in studies examining psychophysiological markers of arousal in children and adults with ASDs.
-
There are some data from RSA and EDA studies supporting the fact that children with ASDs may experience social stress in similar ways to those without ASDs.
-
Cortisol reactivity to social stress in groups with ASDs is attenuated in certain experiments, but not in others.
-
Further studies, utilizing similar experimental protocols, will be helpful in further understanding psychophysiological arousal to social stress in children and adults with ASDs.
References
American Psychiatric Association. Diagnostic and statistical manual of mental disorders. Text revision (DSM-IVTR). 4th ed. Washington, DC: American Psychiatric Publishing; 2000.
Bal E, Harden E, Lamb D, et al. Emotion recognition in children with autism spectrum disorders: relations to eye gaze and autonomic state. J Autism Dev Disord. 2010;40:358–70.
Baron-Cohen S, Leslie AM, Frith U. Does the autistic child have a “theory of mind”? Cognition. 1985;21:37–46.
Beauchaine T. Vagal tone, development, and Gray’s motivational theory: toward an integrated model of autonomic nervous system functioning in psychopathology. Dev Psychopathol. 2001;13:183–214.
Ben Shalom D, Mostofsky SH, Hazlett RL, et al. Normal physiological emotions but differences in expression of conscious feelings in children with high-functioning autism. J Autism Dev Disord. 2006;36:395–400.
Berntson GG, Cacioppo JT, Quigley KS. Autonomic determinism: the modes of autonomic control, the doctrine of autonomic space, and the laws of autonomic constraint. Psychol Rev. 1991;98:459–87.
Bosch JA, de Geus EJ, Carroll D, et al. A general enhancement of autonomic and cortisol responses during social evaluative threat. Psychosom Med. 2009;71:877–85.
Buske-Kirschbaum A, Jobst S, Psych D, et al. Attenuated free cortisol response to psychosocial stress in children with atopic dermatitis. Psychosom Med. 1997;59:419–26.
Carlson M, Earls F. Psychological and neuroendocrinological sequelae of early social deprivation in institutionalized children in Romania. Ann N Y Acad Sci. 1997;807:419–28.
Carpenter LL, Carvalho JP, Tyrka AR, et al. Decreased adrenocorticotropic hormone and cortisol responses to stress in healthy adults reporting significant childhood maltreatment. Biol Psychiatry. 2007;62:1080–7.
Cautela J, Groden J. Relaxation: a comprehensive manual for adults, children and children with special needs. Champaign: Research Press; 1978.
Cervantes Blasquez JC, Rodas Font G, Capdevila Ortis L. Heart-rate variability and precompetitive anxiety in swimmers. Psicothema. 2009;21:531–6.
Corbett BA, Mendoza S, Abdullah M, et al. Cortisol circadian rhythms and response to stress in children with autism. Psychoneuroendocrinology. 2006;31:59–68.
Corbett BA, Mendoza S, Wegelin JA, et al. Variable cortisol circadian rhythms in children with autism and anticipatory stress. J Psychiatry Neurosci. 2008;33:227–34.
Corbett BA, Schupp CW, Levine S, et al. Comparing cortisol, stress, and sensory sensitivity in children with autism. Autism Res. 2009;2:39–49.
Corbett BA, Schupp CW, Simon D, et al. Elevated cortisol during play is associated with age and social engagement in children with autism. Mol Autism. 2010;1:13.
Corona R, Dissanayake C, Arbelle S, et al. Is affect aversive to young children with autism? Behavioral and cardiac responses to experimenter distress. Child Dev. 1998;69:1494–502.
Critchley HD. Electrodermal responses: what happens in the brain. Neuroscientist. 2002;8:132–42.
Dawson G. A psychobiological perspective on the early socio-emotional development of children with autism. In: Cicchetti D, Toth SL, editors. Rochester symposium on developmental psychopathology: vol. 3. Models and integrations. Rochester: University of Rochester Press; 1991. p. 207–34.
Dawson G, Lewy A. Arousal, attention, and the socioemotional impairments of individuals with autism. In: Dawson G, editor. Autism: nature, diagnosis, and treatment. New York: Guilford Press; 1989. p. 49–74.
DesLauriers AM, Carlson CF. Your child is asleep: early infantile autism. Homewood: Dorsey Press; 1969.
Elzinga BM, Roelofs K, Tollenaar MS, et al. Diminished cortisol responses to psychosocial stress associated with lifetime adverse events a study among healthy young subjects. Psychoneuroendocrinology. 2008;33:227–37.
Fernald LC, Burke HM, Gunnar MR. Salivary cortisol levels in children of low-income women with high depressive symptomatology. Dev Psychopathol. 2008;20:423–36.
Field T, Diego M. Vagal activity, early growth and emotional development. Infant Behav Dev. 2008;31:361–73.
Fisher PA, Gunnar MR, Dozier M, et al. Effects of therapeutic interventions for foster children on behavioral problems, caregiver attachment, and stress regulatory neural systems. Ann N Y Acad Sci. 2006;1094:215–25.
Fisher PA, Stoolmiller M, Gunnar MR, et al. Effects of a therapeutic intervention for foster preschoolers on diurnal cortisol activity. Psychoneuroendocrinology. 2007;32:892–905.
Fletcher RR, Dobson K, Goodwin MS, et al. iCalm: wearable sensor and network architecture for wirelessly communicating and logging autonomic activity. IEEE Trans Inf Technol Biomed. 2010;14:215–23.
Fries E, Hesse J, Hellhammer J, et al. A new view on hypocortisolism. Psychoneuroendocrinology. 2005;30:1010–6.
Goenjian AK, Yehuda R, Pynoos RS, et al. Basal cortisol, dexamethasone suppression of cortisol, and MHPG in adolescents after the 1988 earthquake in Armenia. Am J Psychiatry. 1996;153:929–34.
Granger DA, Kivlighan KT, el-Sheikh M, et al. Salivary alpha-amylase in biobehavioral research: recent developments and applications. Ann N Y Acad Sci. 2007;1098:122–44.
Groden J, LeVasseur P, Diller A, Cautela J. Coping with stress through picture rehearsal: a how-to manual for working with individuals with autism and developmental disabilities. Providence: The Groden Center; 1989.
Gunnar MR, Talge NM, Herrera A. Stressor paradigms in developmental studies: what does and does not work to produce mean increases in salivary cortisol. Psychoneuroendocrinology. 2009a;34:953–67.
Gunnar MR, Wewerka S, Frenn K, et al. Developmental changes in hypothalamus-pituitary-adrenal activity over the transition to adolescence: normative changes and associations with puberty. Dev Psychopathol. 2009b;21:69–85.
Hammel JC, Smitherman TA, McGlynn FD, et al. Vagal influence during worry and cognitive challenge. Anxiety Stress Coping. 2010;24:1–16.
Heim C, Ehlert U, Hellhammer DH. The potential role of hypocortisolism in the pathophysiology of stress-related bodily disorders. Psychoneuroendocrinology. 2000;25:1–35.
Hill E, Berthoz S, Frith U. Brief report: cognitive processing of own emotions in individuals with autistic spectrum disorder and in their relatives. J Autism Dev Disord. 2004;34:229–35.
Hinnant JB, El-Sheikh M. Children’s externalizing and internalizing symptoms over time: the role of individual differences in patterns of RSA responding. J Abnorm Child Psychol. 2009;37:1049–61.
Hirstein W, Iversen P, Ramachandran VS. Autonomic responses of autistic children to people and objects. Proc Biol Sci. 2001;268:1883–8.
Hutt C, Hutt SJ, Lee D, et al. Arousal and childhood autism. Nature. 1964;204:908–9.
Jansen LM, Gispen-de Wied CC, van der Gaag RJ, et al. Differentiation between autism and multiple complex developmental disorder in response to psychosocial stress. Neuropsychopharmacology. 2003;28:582–90.
Jessop DS, Turner-Cobb JM. Measurement and meaning of salivary cortisol: a focus on health and disease in children. Stress. 2008;11:1–14.
Kaartinen M, Puura K, Makela T, et al. Autonomic arousal to direct gaze correlates with social impairments among children with ASD. J Autism Dev Disord. 2012;42(9):1917–27.
Kaufman J. Depressive disorders in maltreated children. J Am Acad Child Adolesc Psychiatry. 1991;30:257–65.
Kennedy DP, Courchesne E. The intrinsic functional organization of the brain is altered in autism. Neuroimage. 2008;39:1877–85.
Kinsbourne M. Cerebral brainstem relations in infantile autism. In: Schopler E, Mesibov GB, editors. Neurobiological issues in autism. New York: Plenum Press; 1987. p. 107–25.
Kirschbaum C, Pirke KM, Hellhammer DH. The ‘Trier Social Stress Test’–a tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology. 1993;28:76–81.
Klaassens ER, van Noorden MS, Giltay EJ, et al. Effects of childhood trauma on HPA-axis reactivity in women free of lifetime psychopathology. Prog Neuropsychopharmacol Biol Psychiatry. 2009;33:889–94.
Kudielka BM, Buske-Kirschbaum A, Hellhammer DH, et al. Differential heart rate reactivity and recovery after psychosocial stress (TSST) in healthy children, younger adults, and elderly adults: the impact of age and gender. Int J Behav Med. 2004;11:116–21.
Kylliainen A, Hietanen JK. Skin conductance responses to another person’s gaze in children with autism. J Autism Dev Disord. 2006;36:517–25.
Kylliainen A, Wallace S, Coutanche MN, et al. Affective-motivational brain responses to direct gaze in children with autism spectrum disorder. J Child Psychol Psychiatry. 2012;53:790–7.
Lanni KE, Schupp CW, Simon D, et al. Verbal ability, social stress, and anxiety in children with autistic disorder. Autism. 2012;16:123–38.
Lester BM, Lagasse LL, Shankaran S, et al. Prenatal cocaine exposure related to cortisol stress reactivity in 11-year-old children. J Pediatr. 2010;157:288–95. e281.
Lazarus RS, Folkman S. Stress, appraisal, and coping. New York: Springer; 1984.
Levine TP, Sheinkopf SJ, Pescosolido M, et al. Physiologic arousal to social stress in children with autism spectrum disorders: a pilot study. Res Autism Spectr Disord. 2012;6:177–83.
Lopata C, Volker MA, Putnam SK, et al. Effect of social familiarity on salivary cortisol and self-reports of social anxiety and stress in children with high functioning autism spectrum disorders. J Autism Dev Disord. 2008;38:1866–77.
Lord C, McGee JP. Educating children with autism. Washington, DC: National Academy Press; 2001.
Losh M, Capps L. Understanding of emotional experience in autism: insights from the personal accounts of high-functioning children with autism. Dev Psychol. 2006;42:809–18.
Ming X, Julu PO, Brimacombe M, et al. Reduced cardiac parasympathetic activity in children with autism. Brain Dev. 2005;27:509–16.
Ornitz EM. Autism at the interface between sensory and information processing. In: Dawson G, editor. Autism: nature, diagnosis, and treatment. New York: Guilford Press; 1989. p. 174–297.
Ornitz EM, Ritvo ER. Perceptual inconstancy in early infantile autism. Arch Gen Psychiatry. 1968;18:76–98.
Palkovitz RJ, Wiesenfeld AR. Differential autonomic responses of autistic and normal children. J Autism Dev Disord. 1980;10:347–60.
Pieper S, Brosschot JF, van der Leeden R, et al. Cardiac effects of momentary assessed worry episodes and stressful events. Psychosom Med. 2007;69:901–9.
Poh MZ, Swenson NC, Picard RW. A wearable sensor for unobtrusive, long-term assessment of electrodermal activity. IEEE Trans Biomed Eng. 2010;57:1243–52.
Porges SW. The polyvagal theory: phylogenetic substrates of a social nervous system. Int J Psychophysiol. 2001;42:123–46.
Prizant BM, Wetherby AM, Rubin E, Laurent AC. The SCERTS model: a transactional, family-centered approach to enhancing communication and socioemotional abilities of children with autism spectrum disorder. Infants and Young Children. 2003;16:296–316.
Raison CL, Miller AH. When not enough is too much: the role of insufficient glucocorticoid signaling in the pathophysiology of stress-related disorders. Am J Psychiatry. 2003;160:1554–65.
Rieffe C, Meerum Terwogt M, Kotronopoulou K. Awareness of single and multiple emotions in high-functioning children with autism. J Autism Dev Disord. 2007;37:455–65.
Rimmele U, Seiler R, Marti B, et al. The level of physical activity affects adrenal and cardiovascular reactivity to psychosocial stress. Psychoneuroendocrinology. 2009;34:190–8.
Rohleder N, Joksimovic L, Wolf JM, et al. Hypocortisolism and increased glucocorticoid sensitivity of pro-Inflammatory cytokine production in Bosnian war refugees with posttraumatic stress disorder. Biol Psychiatry. 2004;55:745–51.
Sato K, Kang WH, Saga K, et al. Biology of sweat glands and their disorders. I. Normal sweat gland function. J Am Acad Dermatol. 1989;20:537–63.
Schmitz J, Kramer M, Tuschen-Caffier B, et al. Restricted autonomic flexibility in children with social phobia. J Child Psychol Psychiatry. 2011;52:1203–11.
Schultz RT. Developmental deficits in social perception in autism: the role of the amygdala and fusiform face area. Int J Dev Neurosci. 2005;23:125–41.
Siegel B. When atypical development and typical development cross paths. In: Siegel B, editor. Helping children with autism learn. New York: Oxford University Press; 2003. p. 40–76.
Sigman M, Dissanayake C, Corona R, et al. Social and cardiac responses of young children with autism. Autism. 2003;7:205–16.
Smeets T. Autonomic and hypothalamic-pituitary-adrenal stress resilience: Impact of cardiac vagal tone. Biol Psychol. 2010;84:290–5.
Susman EJ, Dockray S, Schiefelbein VL, et al. Morningness/eveningness, morning-to-afternoon cortisol ratio, and antisocial behavior problems during puberty. Dev Psychol. 2007;43:811–22.
Thayer JF, Friedman BH, Borkovec TD. Autonomic characteristics of generalized anxiety disorder and worry. Biol Psychiatry. 1996;39:255–66.
Thayer JF, Brosschot JF. Psychosomatics and psychopathology: looking up and down from the brain. Psychoneuroendocrinology. 2005;30:1050–8.
Tornhage CJ. Salivary cortisol for assessment of hypothalamic-pituitary-adrenal axis function. Neuroimmunomodulation. 2009;16:284–9.
Van Hecke Vaughan A, Lebow J, Bal E, et al. Electroencephalogram and heart rate regulation to familiar and unfamiliar people in children with autism spectrum disorders. Child Dev. 2009;80:1118–33.
Yoshie M, Kudo K, Murakoshi T, et al. Music performance anxiety in skilled pianists: effects of social-evaluative performance situation on subjective, autonomic, and electromyographic reactions. Exp Brain Res. 2009;199:117–26.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this entry
Cite this entry
Levine, T.P., Conradt, E., Goodwin, M.S., Sheinkopf, S.J., Lester, B. (2014). Psychophysiological Arousal to Social Stress in Autism Spectrum Disorders. In: Patel, V., Preedy, V., Martin, C. (eds) Comprehensive Guide to Autism. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-4788-7_66
Download citation
DOI: https://doi.org/10.1007/978-1-4614-4788-7_66
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-4787-0
Online ISBN: 978-1-4614-4788-7
eBook Packages: Behavioral ScienceReference Module Humanities and Social SciencesReference Module Business, Economics and Social Sciences