
Abstract
Posttraumatic stress disorder (PTSD) is associated with changes in specific brain regions. These brain regions, which include the amygdala, hippocampus, and prefrontal cortex, are involved in memory as well as the stress response. Brain studies in patients with posttraumatic stress disorder (PTSD) have replicated findings in animal studies by finding alterations in these brain areas. Brain areas implicated in PTSD play an important role in the stress response as well as memory, highlighting the important interplay between memory and the traumatic stress response. Abnormalities in these brain areas are hypothesized to underlie symptoms of PTSD.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Single Photon Emission Compute Tomography
- Conditioned Stimulus
- Ptsd Symptom
- Hippocampal Volume
- Medial Prefrontal Cortex
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Lasting Effects of Posttraumatic Stress Disorder
Posttraumatic stress disorder (PTSD) affects about 8% of Americans at some time in their lives (Kessler et al. 1995). For many trauma victims, PTSD can be a life-long problem (Saigh and Bremner 1999). The development of effective treatments is limited by gaps in knowledge about the underlying neurobiological mechanisms that mediate symptoms of PTSD. Until 12 years ago, no brain imaging studies had ever been performed in patients with PTSD or other stress related psychiatric disorders. The past decade has seen an explosion of research using brain imaging to assess changes in the brain in PTSD (Bremner 2005). These studies have implicated the amygdala, hippocampus, and the medial prefrontal cortex (including the anterior cingulate) in PTSD and other stress related psychiatric disorders. This chapter reviews brain imaging studies in the field of PTSD, and integrates them with the basic science findings on the neuroscience of stress.
Neural Circuits of PTSD
PTSD is characterized by specific symptoms, including intrusive thoughts, hyperarousal, flashbacks, nightmares, and sleep disturbances, changes in memory and concentration, and startle responses. Symptoms of PTSD are hypothesized to represent the behavioral manifestation of stress-induced changes in brain structure and function. Stress results in acute and chronic changes in the neurochemical systems and specific brain regions, which result in long-term changes in brain “circuits,” involved in the stress response (Vermetten and Bremner 2002a, b; Bremner 2002a; Pitman 2001). The brain regions that are felt to play an important role in PTSD include the hippocampus, the amygdala, and the medial prefrontal cortex.
Preclinical and clinical studies have shown alterations in memory function in PTSD patients (Elzinga and Bremner 2002), as well as changes in a circuit of brain areas, including the hippocampus, the amygdala, and the medial prefrontal cortex, that mediate alterations in memory (Bremner 2003). The hippocampus, a brain area involved in verbal declarative memory, is very sensitive to the effects of stress. Stress in animals was associated with damage to the neurons in the CA3 region of the hippocampus (which may be mediated by hypercortisolemia, decreased brain derived neurotrophic factor, and/or elevated glutamate levels) and inhibition of neurogenesis (Gould et al. 1998; Magarinos et al. 1996; McEwen et al. 1992; Nibuya et al. 1995; Sapolsky et al. 1990, 1996).
Antidepressant treatments were shown to block the effects of stress and/or promote neurogenesis (Nibuya et al. 1995; Malberg et al. 2000; Czeh et al. 2001; Santarelli et al. 2003; Lucassen et al. 2004). Animal studies have demonstrated several agents with potentially beneficial effects on stress-induced hippocampal damage. It has been found that phenytoin blocks the effects of stress on the hippocampus, probably through modulation of excitatory amino acid induced neurotoxicity.(Watanabe et al. 1992a) Other agents, including tianeptine, dihydroepiandosterone (DHEA), and fluoxetine have similar effects (Malberg et al. 2000; Czeh et al. 2001; Lucassen et al. 2004; Garcia 2002; D’Sa and Duman 2002; Duman et al. 1997, 2001; Duman 2004; McEwen and Chattarji 2004). These medications may share a common mechanism of action through upregulation of the cAMP response element binding protein (CREB) that leads to regulation of the expression of specific target genes involved in structural modeling of the hippocampus. Such treatment effects on BDNF and trkB mRNA, can have long-term effects on brain structure and function. There is new evidence that neurogenesis is necessary for the behavioral effects of antidepressants (Santarelli et al. 2003; Watanabe et al. 1992b) although this continues to be a source of debate (Duman 2004; Henn and Vollmayr 2004).
In addition to the hippocampus, other brain structures including the amygdale and prefrontal cortex have been implicated in a neural circuitry of stress. The amygdala is involved in memory for the emotional valence of events, and plays a critical role in the acquisition of fear responses (Davis 1992). The medial prefrontal cortex includes the anterior cingulate gyrus (Brodmann’s area 32) and the subcallosal gyrus (area 25), as well as orbitofrontal cortex. Lesion studies have demonstrated that the medial prefrontal cortex modulates emotional responsiveness through the inhibition of amygdala function (Morgan et al. 1993). Studies show that the neurons of the medial prefrontal cortex play an active role in the inhibition of fear responses that are mediated by the amygdala (Milad and Quirk 2002; Milad et al. 2006). Conditioned fear responses are extinguished following repeated exposure to the conditioned stimulus in the absence of the unconditioned (aversive, e.g., electric shock) stimulus. This inhibition appears to be mediated by the medial prefrontal cortical inhibition of amygdala responsiveness. Animal studies also show that early stress is associated with a decrease in the branching of neurons in the medial prefrontal cortex (Radley et al. 2004).
Changes in Brain Structure in PTSD
Studies in PTSD are consistent in the changes in cognition and brain structure. Multiple studies have demonstrated verbal declarative memory deficits in PTSD (Elzinga and Bremner 2002; Buckley et al. 2000; Brewin 2001; Golier and Yehuda 1998). Patients with PTSD secondary to combat (Vasterling et al. 1998; Bremner et al. 1993; Golier et al. 1997; Yehuda et al. 1995; Uddo et al. 1993) and childhood abuse (Bremner et al. 1995a, 2004a) were found to have deficits in verbal declarative memory function based on neuropsychological testing. Studies using a variety of measures (including the Wechsler Memory Scale, the visual and verbal components of the Selective Reminding Test, the Auditory Verbal Learning Test, Paired Associate Recall, the California Verbal New Learning Test, and the Rivermead Behavioral Memory Test), found specific deficits in verbal declarative memory function, with a relative sparing of visual memory and IQ (Vasterling et al. 1998, 2002; Bremner et al. 1993, 1995a; Golier et al. 1997; Yehuda et al. 1995; Uddo et al. 1993; Gilbertson et al. 2001; Jenkins et al. 1998; Moradi et al. 1999; Roca and Freeman 2001; Barrett et al. 1996; Gil et al. 1990; Sachinvala et al. 2000). These studies have been conducted both in patients with PTSD related to Vietnam combat (Vasterling et al. 1998, 2002; Bremner et al. 1993; Golier et al. 1997; Yehuda et al. 1995; Uddo et al. 1993; Gilbertson et al. 2001; Roca and Freeman 2001; Barrett et al. 1996; Sachinvala et al. 2000), rape (Jenkins et al. 1998) the Holocaust (Golier et al. 2002, Yehuda et al. 2005a, b) adults with early childhood abuse (Bremner et al. 1995a), and traumatized children (Moradi et al. 1999). Returning Iraq soldiers were shown to have decreases in verbal memory performance compared to their pre-deployment baselines, with greater verbal memory deficits in veterans with high levels of PTSD symptoms (Vasterling et al. 2006). These studies suggest that traumas such as early abuse with associated PTSD result in deficits in the verbal declarative memory.
Studies have also shown changes in hippocampal volume. Vietnam veterans with PTSD were originally shown to have 8% smaller right hippocampal volume based on MRI relative to controls matched for a variety of factors such as alcohol abuse and education (p < 0.05); smaller volume was correlated with deficits in verbal declarative memory function as measured with the WMS (Bremner et al. 1995b). A second study from our group showed a 12% reduction in the left hippocampal volume in 17 patients with childhood abuse-related PTSD compared to 17 case-matched controls; this was significant after controlling for confounding factors (Bremner et al. 1997a). Smaller hippocampal volume was shown to be specific to PTSD within the anxiety disorders, and was not seen in panic disorder (Narayan et al. 1999). Gurvits et al. 1996 showed bilateral hippocampal volume reductions in combat-related PTSD compared to combat veterans without PTSD and normal controls. Combat severity was correlated with volume reduction. Stein et al. 1997 found a 5% reduction in the left hippocampal volume. Other studies in PTSD have found smaller hippocampal volume and/or reductions in NAA, a marker of neuronal integrity (Lindauer et al. 2005, 2006, 2004a; Bremner et al. 2003a; Freeman et al. 1998; Gilbertson et al. 2002; Schuff et al. 2001; Villarreal et al. 2002; Shin et al. 2004a; Emdad et al. 2006; Mahmutyazicioglu et al. 2005; Irle et al. 2005; Li et al. 2006; Hedges et al. 2003). Some studies have found smaller hippocampal volume in PTSD subjects compared to trauma exposed non PTSD subjects (Bremner et al. 2003a) while others have not, finding reductions in both trauma exposed non PTSD and trauma exposed PTSD relative to non trauma exposed non PTSD subjects (Winter and Irle 2004). Studies in childhood (De Bellis et al. 1999, 20001; Carrion et al. 2001) PTSD did not find hippocampal volume reduction, although reduced NAA (indicating loss of neuronal integrity) was found in the medial prefrontal cortex in childhood PTSD (De Bellis et al. 2000). Some studies of new onset or recent PTSD did not find changes in hippocampal volume (Bonne et al. 2001; Notestine et al. 2002), while others showed a reduction (Wignall et al. 2004). In a recent meta-analysis, we pooled data from all of the published studies and found smaller hippocampal volume for both the left and the right sides, equally in adult men and women with chronic PTSD, and no change in children (Kitayama et al. 2005). Another recent meta-analysis had similar findings (Smith 2005). More recent studies of holocaust survivors with PTSD did not find a reduction in hippocampal volume (Golier et al. 2005) although PTSD patients who developed PTSD in response to an initial trauma had smaller hippocampal volume compared to those who developed PTSD after repeated trauma, suggesting a possible vulnerability of smaller hippocampal volume (Yehuda et al. 2007). Several studies have shown that PTSD patients have deficits in hippocampal activation while performing a verbal declarative memory task (Bremner et al. 2003a; Shin et al. 2004a) or a virtual water maze task (Astur et al. 2006). Both hippocampal atrophy and hippocampal-based memory deficits reversed with treatment with the SSRI, paroxetine, which has been shown to promote neurogenesis (the growth of neurons) in the hippocampus, in preclinical studies (Vermetten et al. 2003). We hypothesize that stress-induced hippocampal dysfunction may mediate many of the symptoms of PTSD which are related to memory dysregulation, including both explicit memory deficits as well as fragmentation of memory in abuse survivors. It is unclear at the current time whether these changes are specific to PTSD, whether certain common environmental events (e.g., stress) in different disorders lead to similar brain changes, or whether common genetic traits lead to similar outcomes.
In addition to the hippocampus, other brain structures have been implicated in a neural circuitry of stress, including the amygdala and the prefrontal cortex. The amygdala is involved in memory for the emotional valence of events, and plays a critical role in the acquisition of fear responses. The medial prefrontal cortex includes the anterior cingulate gyrus (Brodmann’s area 32) and the subcallosal gyrus (area 25), as well as the orbitofrontal cortex. Lesion studies have demonstrated that the medial prefrontal cortex modulates emotional responsiveness through the inhibition of amygdala function. Conditioned fear responses are extinguished following repeated exposure to the conditioned stimulus (in the absence of the unconditioned (aversive, e.g., electric shock) stimulus. This inhibition appears to be mediated by the medial prefrontal cortical inhibition of amygdala responsiveness. The insula plays a critical role in integrating the physiological stress response.
Animal studies also show that early stress is associated with a decrease in the branching of neurons in the medial prefrontal cortex (Radley et al. 2004). Several studies have found smaller anterior cingulate volume based on MRI measurements in PTSD (Rauch et al. 2003; Yamasue et al. 2003; Woodward et al. 2006), including women with abuse and PTSD (Kitayama et al. 2005). One study found a reduction in NAA/Cr measured with MRS (Mahmutyazicioglu et al. 2005), while another found a decrease in gray matter density (Corbo et al. 2005). An important question is whether these effects are reversible with treatment. Other findings related to volumetrics include smaller volumes of the corpus callosum in neglected children (Teicher et al. 2004) and adults with PTSD (Villarreal et al. 2004). One study showed a smaller volume of the insula with voxel based morphometry (Chen et al. 2006). A study in twins found smaller volume of the cavum septum pellucidum (May et al. 2004).
Functional Neuroimaging Studies in PTSD
Imaging studies of brain function in PTSD are consistent with dysfunction of the medial prefrontal cortex, the amygdala, and the hippocampus (Pitman 2001; Liberzon and Phan 2003; Liberzon and Martis 2006; Liberzon et al. 2003; Bremner 1998; Bremner 2002b; Rauch et al. 2006; Cannistraro and Rauch 2003). The methodology of imaging studies in PTSD is outlined in Table 1 and a summary of findings by the author, and brain region in Table 2. Studies of resting blood flow or metabolism with PET and SPECT showed alterations at rest in the medial prefrontal, temporal, and dorsolateral prefrontal cortex, the cerebellum, and the amygdala (Bonne et al. 2003; Chung et al. 2006; Bremner et al. 1997b). Stimulation of the noradrenergic system with yohimbine resulted in a failure of activation in the dorsolateral prefrontal, temporal, parietal and orbitofrontal cortex, and decreased function in the hippocampus (Bremner et al. 1997b). Exposure to traumatic reminders in the form of traumatic slides and/or sounds or traumatic scripts was associated with an increase in PTSD symptoms, decreased blood flow and/or failure of activation in the medial prefrontal cortex/anterior cingulate, including Brodmann’s area 25, or subcallosal gyrus, area 32 and 24, as measured with PET, SPECT or fMRI (Britton et al. 2005; Yang et al. 2004; Bremner et al. 1999a, b; Lanius et al. 2001, 2003; Liberzon et al. 1999; Shin et al. 1999, 1997, 2001, 2004b, 2005; Semple et al. 2000; Lindauer et al. 2004b; Phan et al. 2006) (Fig. 1). Other findings in studies of traumatic reminder exposure include decreased function in the hippocampus (Bremner et al. 1999b), the thalamus (Lanius et al. 2001, 2003), the visual association cortex (Lanius et al. 2003; Bremner et al. 1999b; Shin et al. 1997, 2004b), the parietal cortex (Bremner et al. 1999b; Shin et al. 1997, 1999; Rauch et al. 1996; Sakamoto et al. 2005), and the inferior frontal gyrus (Lanius et al. 2003; Bremner et al. 1999b; Shin et al. 1997, 1999, 2001; Rauch et al. 1996; Sakamoto et al. 2005), and increased function in the amygdala (Liberzon et al. 1999; Shin et al. 2004b; wv2001; Shin et al. 1997), and the parahippocampal gyrus (Bremner et al. 1999a, b; Liberzon et al. 1999). Shin et al. 2004b found a correlation between the increased amygdala function and the decreased medial prefrontal function with traumatic reminders, indicating that a failure of inhibition of the amygdala by the medial prefrontal cortex could account for increased PTSD symptoms with traumatic reminders. Other studies found increased amygdala and parahippocampal function and decreased medial prefrontal function during performance of an attention task (Semple et al. 2000), and increased amygdala function at rest (Chung et al. 2006), during a working memory task (Bryant et al. 2005), during recall of traumatic words (Protopopescu et al. 2005), with exposure to masked fearful faces (Rauch et al. 2000; Armony et al. 2005), overt fearful faces (Shin et al. 2005), traumatic sounds (Liberzon et al. 1999; Pissiota et al. 2002), and traumatic scripts (Rauch et al. 1996).

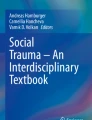
Hippocampal volume on MRI in PTSD. There was smaller hippocampal volume in a representative patient with PTSD (right) relative to a non PTSD subject (left)
Several studies have examined neural correlates of cognitive tasks in PTSD. During working memory tasks, patients showed decreased inferior frontal (Clark et al. 2003) and parietal function (Bryant et al. 2005; Clark et al. 2003). Retrieval of emotionally valenced words (Bremner et al. 2001) (e.g., “rape-mutilate”) in women with PTSD from early abuse resulted in decreases in blood flow in an extensive area which included the orbitofrontal cortex, the anterior cingulate, and the medial prefrontal cortex (Brodmann’s areas 25, 32, 9), the left hippocampus, and the fusiform gyrus/inferior temporal gyrus, with increased activation in the posterior cingulate, the left inferior parietal cortex, the left middle frontal gyrus, and the visual association and motor cortex (Bremner et al. 2003b). Another study found a failure of the medial prefrontal cortical/anterior cingulate activation, and decreased visual association and parietal cortex function in women with abuse and PTSD, relative to women with abuse without PTSD, during performance of the emotional Stroop task (i.e., naming the color of a word such as “rape”) (Bremner et al. 2004b). Shin et al. 2001 showed an increased posterior cingulate and parahippocampal gyrus and a decreased medial prefrontal and dorsolateral prefrontal during an emotional “counting” Stroop paradigm with fMRI.
Studies have also used declarative memory tasks as specific probes of hippocampal function. We measured brain activation with a paragraph encoding task in conjunction with PET O-15 water measurement of brain blood flow. Women with abuse and PTSD showed a failure of hippocampal activation during the memory task, relative to controls (Bremner et al. 2003a). Women with abuse and PTSD in this study also had smaller hippocampal volume measured with MRI, relative to both women with abuse without PTSD and non-abused non-PTSD women. The failure of hippocampal activation was significant after controlling differences in hippocampal volume as well as accuracy of encoding. Shin et al. 2004a also found a failure of hippocampal activation with a memory stem completion task in PTSD.
Although multiple studies have used symptom provocation with traumatic scripts or similar designs, little has been done in the area of fear conditioning in PTSD. To that end, we studied women with a history of severe childhood sexual abuse and the diagnosis of current PTSD (N = 8), and women without childhood abuse or PTSD (N = 11). All the subjects underwent positron emission tomographic (PET) measurement of cerebral blood flow and psychophysiology measurement of heart rate and skin conductance during habituation, acquisition and extinction conditions on a single day, with scanning during a control condition on another day separated by 1 week from the active condition. During habituation the subjects were repeatedly exposed to a blue square on a screen (conditioned stimulus (CS)); during active fear acquisition, exposure to the blue square (CS) was paired with an electric shock to the forearm (unconditioned stimulus (UCS)); and during extinction, subjects were again exposed to the blue squares (CS) without shock (“active” extinction). On the second day, the subjects went through the same procedure with electric shocks delivered randomly when the blue square was not present (unpaired CS–UCS). Acquisition of fear was associated with increased skin conductance (SC) responses to CS exposure during the active versus the control conditions in all the subjects. There was increased SC for PTSD during the first CS–UCS presentation. Extinction of fear was associated with increased skin conductance (SC) responses to CS exposure during the active versus the control conditions, in all the subjects. When PTSD and non-PTSD subjects were examined separately, the SC levels were significantly elevated in non-PTSD subjects undergoing extinction of fear following the active compared to the control condition during session one. PTSD subjects showed activation of the bilateral amygdala during fear acquisition compared to the control condition (Fig. 2). Non-PTSD subjects showed an area of activation in the region of the left amygdala. When PTSD subjects and control subjects were directly compared, PTSD subjects showed a greater activation of the left amygdala during the fear conditioning condition (pairing of US and CS) relative to the random shock control than healthy women. Other areas that showed increased activation with fear acquisition in PTSD included the bilateral superior temporal gyrus (Brodmann’s Area (BA) 22), cerebellum, bilateral inferior frontal gyrus (BA 44, 45) and the posterior cingulate (BA) 24). Fear acquisition was associated with decreased function in the medial prefrontal cortex, the visual association cortex, and the medial temporal cortex, the inferior parietal lobule function, and other areas. Extinction of fear responses was associated with decreased function in the orbitofrontal and medial prefrontal cortex (including subcallosal gyrus, BA 25, and anterior cingulate BA 32), the visual association cortex, and other areas in the PTSD subjects, but not in the controls. Amygdala blood flow with fear acquisition was negatively correlated with medial prefrontal blood flow with fear extinction (increased blood flow in the amygdala correlated with decreased blood flow in the medial prefrontal cortex) in all the subjects (r = −0.48; p < 0.05). Increased amygdala blood flow with fear acquisition was positively correlated with PTSD (r = 0.45), anxiety (r = 0.44) and dissociative (r = 0.80) symptom levels in PTSD (but not non-PTSD) subjects. There was a negative correlation between the medial prefrontal blood flow during extinction and anxiety as measured with the PASS during extinction in the PTSD group only which was significant after correction for multiple comparisons (r = −0.90; p = 0.006) (Bremner et al. 2005a). This study was consistent with increased amygdala function with fear acquisition, and decreased medial prefrontal (anterior cingulate) function during extinction in PTSD. This is consistent with the model of an over active amygdala and a failure of medial prefrontal cortex to extinguish, or shut off, the amygdala, when the acute threat is no longer present.

Medial prefrontal dysfunction in PTSD. There was a failure of medial prefrontal activation in a group of combat veterans with PTSD compared to combat veterans without PTSD during exposure to traumatic combat related slides and sounds (yellow area in prefrontal cortex)
Few studies have involved imaging of receptors in the brain in PTSD. One study used single photon emission computed tomography (SPECT) to show a decrease in benzodiazepine receptor binding in the frontal cortex in Vietnam combat-related PTSD (Bremner et al. 2000). Another study of Gulf War-related PTSD showed a negative correlation between childhood trauma and right superior temporal gyrus benzodiazepine receptor binding (Fujita et al. 2004).
In summary, these studies are consistent with dysfunction of a circuit involving the medial prefrontal cortex, the dorsolateral prefrontal cortex, and the hippocampus and the amygdala, in PTSD patients that we hypothesize underlie symptoms of PTSD.
Effects of Pharmacotherapy on Brain Function and Structure in PTSD
We have begun to assess the effects of pharmacotherapy on brain structure and function in PTSD (Bremner and Vermetten 2004). We recently assessed the effects of phenytoin on brain structure and function. Studies in animals show that phenytoin, which is used in the treatment of epilepsy and is known to modulate glutamatergic function, blocks the effects of stress on the hippocampus (Watanabe et al. 1992a). We studied nine patients with PTSD in an open label function before and after treatment with phenytoin. Phenytoin resulted in a significant improvement in PTSD symptoms (Bremner et al. 2004c). Phenytoin also resulted in increases in both right hippocampal volume and right hemisphere volume (Bremner et al. 2005b). These findings indicate that phenytoin has an effect on PTSD symptoms as well as brain structure in PTSD patients. In a second study, patients with PTSD were shown to have an increase in hippocampal volume and memory function with paroxetine (Vermetten et al. 2003), and a decrease in cortisol responsiveness to a stressful cognitive challenge (Vermetten et al. 2006). One case report showed decreased inferior frontal, prefrontal, and insula blood flow measured with PET in response to war related sounds. These changes normalized with successful treatment with the SSRI fluoxetine (Fernandez et al. 2001). Another study assessed resting brain blood flow with SPECT Tc-99m HMPAO before and after 8 weeks of open label treatment with the SSRI citalopram in 11 adult patients with PTSD. The treatment resulted in a decrease in the left medial temporal cortex blood flow; decreased PTSD symptoms as measured with the CAPS were correlated with increased function in the medial prefrontal cortex (Seedat et al. 2003).
Summary and Conclusions
Brain imaging studies have shown that PTSD is associated with changes in brain function and structure. Brain areas implicated in the stress response include the amygdala, the hippocampus, and the prefrontal cortex. These brain areas also play a critical role in memory, highlighting the important interplay between memory and the traumatic stress response. Preclinical studies show that stress affects these brain areas. Furthermore, antidepressants have effects on the hippocampus that counteract the effects of stress. In fact, promotion of nerve growth (neurogenesis) in the hippocampus may be central to the efficacy of the antidepressants. Studies in patients with posttraumatic stress disorder (PTSD) show alterations in brain areas implicated in animal studies, including the amygdala, the hippocampus, and the prefrontal cortex. Increased amygdala activation with acquisition of fear responses, and a failure of the medial prefrontal cortex to properly mediate extinction are hypothesized to underlie symptoms of PTSD. Treatments that are efficacious for PTSD show a promotion of neurogenesis in animal studies as well as a promotion of memory and increased hippocampal volume in PTSD. Future studies are needed to assess neural mechanisms in treatment response in PTSD. In addition, studies need to move beyond assessments of brain function and to examine areas such as neuroreceptor binding and changes in brain chemicals (e.g., with MRS).
References
Armony JL, Corbo V, Clement MH, Brunet A (2005) Amygdala response in patients with acute PTSD to masked and unmasked emotional facial expressions. Am J Psychiatry 162(10):1961–1963
Astur RS, St Germain SA, Tolin D et al (2006) Hippocampus function predicts severity of post-traumatic stress disorder. Cyberpsychol Behav 9(2):234–240
Barrett DH, Green ML, Morris R, Giles WH, Croft JB (1996) Cognitive functioning and posttraumatic stress disorder. Am J Psychiatry 153(11):1492–1494
Bonne O, Brandes D, Gilboa A et al (2001) Longitudinal MRI study of hippocampal volume in trauma survivors with PTSD. Am J Psychiatry 158:1248–1251
Bonne O, Gilboa A, Louzoun Y et al (2003) Resting regional cerebral perfusion in recent posttraumatic stress disorder. Biol Psychiatry 54(10):1077–1086
Bremner JD (1998) Neuroimaging of posttraumatic stress disorder. Psychiatr Ann 28:445–450
Bremner JD (2002a) Does stress damage the brain? Understanding trauma-related disorders from a mind-body perspective. W.W. Norton, New York, NY
Bremner JD (2002b) Neuroimaging of childhood trauma. Semin Clin Neuropsychiatry 7:104–112
Bremner JD (2003) Functional neuroanatomical correlates of traumatic stress revisited 7 years later, this time with data. Psychopharmacol Bull 37(2):6–25
Bremner JD (2005) Brain imaging handbook. W.W. Norton, New York, NY
Bremner JD, Vermetten E (2004) Neuroanatomical changes associated with pharmacotherapy in posttraumatic stress disorder (PTSD). Ann N Y Acad Sci 1032:154–157
Bremner JD, Scott TM, Delaney RC et al (1993) Deficits in short-term memory in post-traumatic stress disorder. Am J Psychiatry 150:1015–1019
Bremner JD, Randall PR, Capelli S et al (1995a) Deficits in short-term memory in adult survivors of childhood abuse. Psychiatry Res 59:97–107
Bremner JD, Randall PR, Scott TM et al (1995b) MRI-based measurement of hippocampal volume in patients with combat-related posttraumatic stress disorder. Am J Psychiatry 152:973–981
Bremner JD, Randall PR, Vermetten E et al (1997a) MRI-based measurement of hippocampal volume in posttraumatic stress disorder related to childhood physical and sexual abuse: a preliminary report. Biol Psychiatry 41:23–32
Bremner JD, Innis RB, Ng CK et al (1997b) PET measurement of cerebral metabolic correlates of yohimbine administration in posttraumatic stress disorder. Arch Gen Psychiatry 54:246–256
Bremner JD, Staib L, Kaloupek D et al (1999a) Neural correlates of exposure to traumatic pictures and sound in Vietnam combat veterans with and without posttraumatic stress disorder: a positron emission tomography study. Biol Psychiatry 45:806–816
Bremner JD, Narayan M, Staib LH et al (1999b) Neural correlates of memories of childhood sexual abuse in women with and without posttraumatic stress disorder. Am J Psychiatry 156:1787–1795
Bremner JD, Innis RB, Southwick SM et al (2000) Decreased benzodiazepine receptor binding in frontal cortex in combat-related posttraumatic stress disorder. Am J Psychiatry 157:1120–1126
Bremner JD, Soufer R, McCarthy G et al (2001) Gender differences in cognitive and neural correlates of remembrance of emotional words. Psychopharmacol Bull 35:55–87
Bremner JD, Vythilingam M, Vermetten E et al (2003a) MRI and PET study of deficits in hippocampal structure and function in women with childhood sexual abuse and posttraumatic stress disorder (PTSD). Am J Psychiatry 160:924–932
Bremner JD, Vythilingam M, Vermetten E et al (2003b) Neural correlates of declarative memory for emotionally valenced words in women with posttraumatic stress disorder (PTSD) related to early childhood sexual abuse. Biol Psychiatry 53:289–299
Bremner JD, Vermetten E, Nafzal N, Vythilingam M (2004a) Deficits in verbal declarative memory function in women with childhood sexual abuse-related posttraumatic stress disorder (PTSD). J Nerv Ment Dis 192(10):643–649
Bremner JD, Vermetten E, Vythilingam M et al (2004b) Neural correlates of the classical color and emotional Stroop in women with abuse-related posttraumatic stress disorder. Biol Psychiatry 55(6):612–620
Bremner JD, Mletzko T, Welter S et al (2004c) Treatment of posttraumatic stress disorder with phenytoin: an open label pilot study. J Clin Psychiatry 65(11):1559–1564
Bremner JD, Vermetten E, Schmahl C et al (2005a) Positron emission tomographic imaging of neural correlates of a fear acquisition and extinction paradigm in women with childhood sexual abuse-related posttraumatic stress disorder. Psychol Med 35(6):791–806
Bremner JD, Mletzko T, Welter S et al (2005b) Effects of phenytoin on memory, cognition and brain structure in posttraumatic stress disorder: a pilot study. J Psychopharmacol 19(2):159–165
Brewin CR (2001) A cognitive neuroscience account of post-traumatic stress disorder and its treatment. Behav Res Ther 39:373–393
Britton JC, Phan KL, Taylor SF, Fig LM, Liberzon I (2005) Corticolimbic blood flow in posttraumatic stress disorder during script-driven imagery. Biol Psychiatry 57(8):832–840
Bryant RA, Felmingham KL, Kemp AH et al (2005) Neural networks of information processing in posttraumatic stress disorder: a functional magnetic resonance imaging study. Biol Psychiatry 58(2):111–118
Buckley TC, Blanchard EB, Neill WT (2000) Information processing and PTSD: a review of the empirical literature. Clin Psychol Rev 28(8):1041–1065
Cannistraro PA, Rauch SL (2003) Neural circuitry of anxiety: evidence from structural and functional neuroimaging studies. Psychopharmacol Bull 37(4):8–25
Carrion VG, Weems CF, Eliez S et al (2001) Attenuation of frontal asymmetry in pediatric posttraumatic stress disorder. Biol Psychiatry 50:943–951
Chen S, Xia W, Li L et al (2006) Gray matter density reduction in the insula in fire survivors with posttraumatic stress disorder: a voxel-based morphometric study. Psychiatry Res 146(1):65–72
Chung YA, Kim SH, Chung SK et al (2006) Alterations in cerebral perfusion in posttraumatic stress disorder patients without re-exposure to accident-related stimuli. Clin Neurophysiol 117(3):637–642
Clark CR, McFarlane AC, Morris P et al (2003) Cerebral function in posttraumatic stress disorder during verbal working memory updating: a positron emission tomography study. Biol Psychiatry 53:474–481
Corbo V, Clement MH, Armony JL, Pruessner JC, Brunet A (2005) Size versus shape differences: contrasting voxel-based and volumetric analyses of the anterior cingulate cortex in individuals with acute posttraumatic stress disorder. Biol Psychiatry 58(2):119–124
Czeh B, Michaelis T, Watanabe T et al (2001) Stress-induced changes in cerebral metabolites, hippocampal volume, and cell proliferation are prevented by antidepressant treatment with tianeptine. Proc Natl Acad Sci USA 98:12796–12801
Davis M (1992) The role of the amygdala in fear and anxiety. Annu Rev Neurosci 15:353–375
De Bellis MD, Keshavan MS, Clark DB et al (1999) A.E. Bennett Research Award: Developmental traumatology: Part II. Brain development. Biol Psychiatry 45:1271–1284
De Bellis MD, Keshavan MS, Spencer S, Hall J (2000) N-acetylaspartate concentration in the anterior cingulate of maltreated children and adolescents with PTSD. Am J Psychiatry 157:1175–1177
De Bellis MD, Hall J, Boring AM, Frustaci K, Moritz G (2001) A pilot longitudinal study of hippocampal volumes in pediatric maltreatment-related posttraumatic stress disorder. Biol Psychiatry 50:305–309
D’Sa C, Duman RS (2002) Antidepressants and neuroplasticity. Bipolar Disord 4:183–194
Duman RS (2004) Depression: a case of neuronal life and death? Biol Psychiatry 56:140–145
Duman RS, Heninger GR, Nestler EJ (1997) A molecular and cellular theory of depression. Arch Gen Psychiatry 54:597–606
Duman RS, Malberg JE, Nakagawa S (2001) Regulation of adult neurogenesis by psychotropic drugs and stress. J Pharmacol Exp Ther 299:401–407
Elzinga BM, Bremner JD (2002) Are the neural substrates of memory the final common pathway in PTSD? J Affect Disord 70:1–17
Emdad R, Bonekamp D, Sondergaard HP et al (2006) Morphometric and psychometric comparisons between non-substance-abusing patients with posttraumatic stress disorder and normal controls. Psychother Psychosom 75(2):122–132
Fernandez M, Pissiota A, Frans O et al (2001) Brain function in a patient with torture related post-traumatic stress disorder before and after fluoxetine treatment: a positron emission tomography provocation study. Neurosci Lett 297:101–104
Freeman TW, Cardwell D, Karson CN, Komoroski RA (1998) In vivo proton magnetic resonance spectroscopy of the medial temporal lobes of subjects with combat-related posttraumatic stress disorder. Magn Reson Med 40:66–71
Fujita M, Southwick SM, Denucci CC et al (2004) Central type benzodiazepine receptors in Gulf War veterans with posttraumatic stress disorder. Biol Psychiatry 56(2):95–100
Garcia R (2002) Stress, metaplasticity, and antidepressants. Curr Mol Med 2:629–638
Gil T, Calev A, Greenberg D, Kugelmas S, Lerer B (1990) Cognitive functioning in posttraumatic stress disorder. J Trauma Stress 3:29–45
Gilbertson MW, Gurvits TV, Lasko NB, Orr SP, Pitman RK (2001) Multivariate assessment of explicit memory function in combat veterans with posttraumatic stress disorder. J Trauma Stress 14:413–420
Gilbertson MW, Shenton ME, Ciszewski A et al (2002) Smaller hippocampal volume predicts pathologic vulnerability to psychological trauma. Nat Neurosci 5(11):1242–1247
Golier J, Yehuda R (1998) Neuroendocrine activity and memory-related impairments in posttraumatic stress disorder. Dev Psychopathol 10(4):857–869
Golier J, Yehuda R, Cornblatt B et al (1997) Sustained attention in combat-related posttraumatic stress disorder. Integr Physiol Behav Sci 32(1):52–61
Golier JA, Yehuda R, Lupien SJ et al (2002) Memory performance in Holocaust survivors with posttraumatic stress disorder. Am J Psychiatry 159(10):1682–1688
Golier JA, Yehuda R, De Santi S et al (2005) Absence of hippocampal volume differences in survivors of the Nazi Holocaust with and without posttraumatic stress disorder. Psychiatry Res 139(1):53–64
Gould E, Tanapat P, McEwen BS, Flugge G, Fuchs E (1998) Proliferation of granule cell precursors in the dentate gyrus of adult monkeys is diminished by stress. Proc Natl Acad Sci USA 95:3168–3171
Gurvits TG, Shenton MR, Hokama H et al (1996) Magnetic resonance imaging study of hippocampal volume in chronic combat-related posttraumatic stress disorder. Biol Psychiatry 40:192–199
Hedges DW, Allen S, Tate DF et al (2003) Reduced hippocampal volume in alcohol and substance naive Vietnam combat veterans with posttraumatic stress disorder. Cogn Behav Neurol. 16(4):219–224
Henn FA, Vollmayr B (2004) Neurogenesis and depression: etiology or epiphenomenon? Biol Psychiatry 56:146–150
Irle E, Lange C, Sachsse U (2005) Reduced size and abnormal asymmetry of parietal cortex in women with borderline personality disorder. Biol Psychiatry 57(2):173–182
Jenkins MA, Langlais PJ, Delis D, Cohen R (1998) Learning and memory in rape victims with posttraumatic stress disorder. Am J Psychiatry 155:278–279
Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson CB (1995) Posttraumatic stress disorder in the national comorbidity survey. Arch Gen Psychiatry 52:1048–1060
Kitayama N, Vaccarino V, Kutner M, Weiss P, Bremner JD (2005) Magnetic resonance imaging (MRI) measurement of hippocampal volume in posttraumatic stress disorder: a meta-analysis. J Affect Disord 88(1):79–86
Lanius RA, Williamson PC, Densmore M et al (2001) Neural correlates of traumatic memories in posttraumatic stress disorder: a functional MRI investigation. Am J Psychiatry 158:1920–1922
Lanius RA, Williamson PC, Hopper J et al (2003) Recall of emotional states in posttraumatic stress disorder: an fMRI investigation. Biol Psychiatry 53(3):204–210
Li L, Chen S, Liu J et al (2006) Magnetic resonance imaging and magnetic resonance spectroscopy study of deficits in hippocampal structure in fire victims with recent-onset posttraumatic stress disorder. Can J Psychiatry 51(7):431–437
Liberzon I, Martis B (2006) Neuroimaging studies of emotional responses in PTSD. Ann N Y Acad Sci 1071:87–109
Liberzon I, Phan KL (2003) Brain-imaging studies of posttraumatic stress disorder. CNS Spectr 8(9):641–650
Liberzon I, Taylor SF, Amdur R et al (1999) Brain activation in PTSD in response to trauma-related stimuli. Biol Psychiatry 45:817–826
Liberzon I, Britton JC, Phan KL (2003) Neural correlates of traumatic recall in posttraumatic stress disorder. Stress 6(3):151–156
Lindauer RJ, Vlieger EJ, Jalink M et al (2004a) Smaller hippocampal volume in Dutch police officers with posttraumatic stress disorder. Biol Psychiatry 56(5):356–363
Lindauer RJ, Booij J, Habraken JB et al (2004b) Cerebral blood flow changes during script-driven imagery in police officers with posttraumatic stress disorder. Biol Psychiatry 56(11):853–861
Lindauer RJ, Vlieger EJ, Jalink M et al (2005) Effects of psychotherapy on hippocampal volume in out-patients with post-traumatic stress disorder: a MRI investigation. Psychol Med 35(10):1421–1431
Lindauer RJ, Olff M, van Meijel EP, Carlier IV, Gersons BP (2006) Cortisol, learning, memory, and attention in relation to smaller hippocampal volume in police officers with posttraumatic stress disorder. Biol Psychiatry 59(2):171–177
Lucassen PJ, Fuchs E, Czeh B (2004) Antidepressant treatment with tianeptine reduces apoptosis in the hippocampal dentate gyrus and temporal cortex. Eur J Neurosci 14:161–166
Magarinos AM, McEwen BS, Flugge G, Fluchs E (1996) Chronic psychosocial stress causes apical dendritic atrophy of hippocampal CA3 pyramidal neurons in subordinate tree shrews. J Neurosci 16:3534–3540
Mahmutyazicioglu K, Konuk N, Ozdemir H et al (2005) Evaluation of the hippocampus and the anterior cingulate gyrus by proton MR spectroscopy in patients with post-traumatic stress disorder. Diagn Interv Radiol 11(3):125–129
Malberg JE, Eisch AJ, Nestler EJ, Duman RS (2000) Chronic antidepressant treatment increases neurogenesis in adult rat hippocampus. J Neurosci 20:9104–9110
May FS, Chen QC, Gilbertson MW, Shenton ME, Pitman RK (2004) Cavum septum pellucidum in monozygotic twins discordant for combat exposure: relationship to posttraumatic stress disorder. Biol Psychiatry 55(6):656–658
McEwen BS, Chattarji S (2004) Molecular mechanisms of neuroplasticity and pharmacological implications: the example of tianeptine. Eur Neuropsychopharmacol 14(Suppl 5):S497–S502
McEwen BS, Angulo J, Cameron H et al (1992) Paradoxical effects of adrenal steroids on the brain: protection versus degeneration. Biol Psychiatry 31:177–199
Milad MR, Quirk GJ (2002) Neurons in medial prefrontal cortex signal memory for fear extinction. Nature 420:70–73
Milad MR, Rauch SL, Pitman RK, Quirk GJ (2006) Fear extinction in rats: implications for human brain imaging and anxiety disorders. Biol Psychol 73(1):61–71
Moradi AR, Doost HT, Taghavi MR, Yule W, Dalgleish T (1999) Everyday memory deficits in children and adolescents with PTSD: performance on the Rivermead Behavioural Memory Test. J Child Psychol Psychiatr 40:357–361
Morgan CA, Romanski LM, LeDoux JE (1993) Extinction of emotional learning: contribution of medial prefrontal cortex. Neurosci Lett 163:109–113
Narayan M, Bremner JD, Kumar A (1999) Neuroanatomical substrates of late-life mental disorders. J Geriatr Psychiatry Neurol 12:95–106
Nibuya M, Morinobu S, Duman RS (1995) Regulation of BDNF and trkB mRNA in rat brain by chronic electroconvulsive seizure and antidepressant drug treatments. J Neurosci 15:7539–7547
Notestine CF, Stein MB, Kennedy CM, Archibald SL, Jernigan TL (2002) Brain morphometry in female victims of intimate partner violence with and without posttraumatic stress disorder. Biol Psychiatry 51:1089–1101
Phan KL, Britton JC, Taylor SF, Fig LM, Liberzon I (2006) Corticolimbic blood flow during nontraumatic emotional processing in posttraumatic stress disorder. Arch Gen Psychiatry 63(2):184–192
Pissiota A, Frans O, Fernandez M et al (2002) Neurofunctional correlates of posttraumatic stress disorder: a PET symptom provocation study. Eur Arch Psychiatry Clin Neurosci 252:68–75
Pitman RK (2001) Investigating the pathogenesis of posttraumatic stress disorder with neuroimaging. J Clin Psychiatry 62:47–54
Protopopescu X, Pan H, Tuescher O et al (2005) Differential time courses and specificity of amygdala activity in posttraumatic stress disorder subjects and normal control subjects. Biol Psychiatry 57(5):464–473
Radley JJ, Sisti HM, Hao J et al (2004) Chronic behavioral stress induces apical dendritic reorganization in pyramidal neurons of the medial prefrontal cortex. Neuroscience 125(1):1–6
Rauch SL, van der Kolk BA, Fisler RE et al (1996) A symptom provocation study of posttraumatic stress disorder using positron emission tomography and script driven imagery. Arch Gen Psychiatry 53:380–387
Rauch SL, Whalen PJ, Shin LM et al (2000) Exaggerated amygdala response to masked facial stimuli in posttraumatic stress disorder: a functional MRI study. Biol Psychiatry 47(9):769–776
Rauch SL, Shin LM, Segal E et al (2003) Selectively reduced regional cortical volumes in post-traumatic stress disorder. Neuroreport 14(7):913–916
Rauch SL, Shin LM, Phelps EA (2006) Neurocircuitry models of posttraumatic stress disorder and extinction: human neuroimaging research – past, present, and future. Biol Psychiatry 60(4):376–382
Roca V, Freeman TW (2001) Complaints of impaired memory in veterans with PTSD. Am J Psychiatry 158:1738
Sachinvala N, vonScotti H, McGuire M et al (2000) Memory, attention, function, and mood among patients with chronic posttraumatic stress disorder. J Nerv Ment Dis 188:818–823
Saigh PA, Bremner JD (1999) Posttraumatic stress disorder: a comprehensive text. Allyn & Bacon, Needham Heights, MA
Sakamoto H, Fukuda R, Okuaki T et al (2005) Parahippocampal activation evoked by masked traumatic images in posttraumatic stress disorder: a functional MRI study. Neuroimage 26(3):813–821
Santarelli L, Saxe M, Gross C et al (2003) Requirement of hippocampal neurogenesis for the behavioral effects of antidepressants. Science 301(5634):805–809
Sapolsky RM (1996) Why stress is bad for your brain. Science 273:749–750
Sapolsky RM, Uno H, Rebert CS, Finch CE (1990) Hippocampal damage associated with prolonged glucocorticoid exposure in primates. J Neurosci 10:2897–2902
Schuff N, Neylan TC, Lenoci MA et al (2001) Decreased hippocampal N-acetylaspartate in the absence of atrophy in posttraumatic stress disorder. Biol Psychiatry 50:952–959
Seedat S, Warwick J, van Heerden B et al (2003) Single photon emission computed tomography in posttraumatic stress disorder before and after treatment with a selective serotonin reuptake inhibitor. J Affect Disord 80:45–53
Semple WE, Goyer PF, McCormick R, Compton-Toth B, Morris E, Donovan B, et al. (1996) Attention and regional cerebral blood flow in posttraumatic stress disorder patients with substance abuse histories. Psychiatry Research: Neuroimaging 67:17–28
Semple WE, Goyer P, McCormick R et al (2000) Higher brain blood flow at amygdala and lower frontal cortex blood flow in PTSD patients with comorbid cocaine and alcohol abuse compared to controls. Psychiatry 63:65–74
Shin LM, Kosslyn SM, McNally RJ et al (1997) Visual imagery and perception in posttraumatic stress disorder: a positron emission tomographic investigation. Arch Gen Psychiatry 54:233–237
Shin LM, McNally RJ, Kosslyn SM et al (1999) Regional cerebral blood flow during script-driven imagery in childhood sexual abuse-related PTSD: a PET investigation. Am J Psychiatry 156:575–584
Shin LM, Whalen PJ, Pitman RK et al (2001) An fMRI study of anterior cingulate function in posttraumatic stress disorder. Biol Psychiatry 50:932–942
Shin LM, Shin PS, Heckers S et al (2004a) Hippocampal function in posttraumatic stress disorder. Hippocampus 14(3):292–300
Shin LM, Orr SP, Carson MA et al (2004b) Regional cerebral blood flow in the amygdala and medial prefrontal cortex during traumatic imagery in male and female Vietnam veterans with PTSD. Arch Gen Psychiatry 61(2):168–176
Shin LM, Wright CI, Cannistraro PA et al (2005) A functional magnetic resonance imaging study of amygdala and medial prefrontal cortex responses to overtly presented fearful faces in posttraumatic stress disorder. Arch Gen Psychiatry 62(3):273–281
Smith ME (2005) Bilateral hippocampal volume reduction in adults with post-traumatic stress disorder: a meta-analysis of structural MRI studies. Hippocampus 15(6):798–807
Stein MB, Koverola C, Hanna C, Torchia MG, McClarty B (1997) Hippocampal volume in women victimized by childhood sexual abuse. Psychol Med 27:951–959
Teicher MH, Dumont NL, Ito Y et al (2004) Childhood neglect is associated with reduced corpus callosum area. Biol Psychiatry 56:80–85
Uddo M, Vasterling JJ, Braily K, Sutker PB (1993) Memory and attention in posttraumatic stress disorder. J Psychopathol Behav Assess 15:43–52
Vasterling JJ, Brailey K, Constans JI, Sutker PB (1998) Attention and memory dysfunction in posttraumatic stress disorder. Neuropsychology 12:125–133
Vasterling JJ, Duke LM, Brailey K et al (2002) Attention, learning, and memory performance and intellectual resources in Vietnam veterans: PTSD and no disorder comparisons. Neuropsychology 16:5–14
Vasterling JJ, Proctor SP, Amoroso P et al (2006) Neuropsychological outcomes of Army personnel following deployment to the Iraq War. JAMA 296:519–529
Vermetten E, Bremner JD (2002a) Circuits and systems in stress. II. Applications to neurobiology and treatment of PTSD. Depress Anxiety 16:14–38
Vermetten E, Bremner JD (2002b) Circuits and systems in stress. I. Preclinical studies. Depress Anxiety 15:126–147
Vermetten E, Vythilingam M, Southwick SM, Charney DS, Bremner JD (2003) Long-term treatment with paroxetine increases verbal declarative memory and hippocampal volume in posttraumatic stress disorder. Biol Psychiatry 54(7):693–702
Vermetten E, Vythilingam M, Schmahl C et al (2006) Alterations in stress reactivity after long-term treatment with paroxetine in women with posttraumatic stress disorder. Ann N Y Acad Sci 1071:184–202
Villarreal G, Hamilton DA, Petropoulos H et al (2002) Reduced hippocampal volume and total white matter in posttraumatic stress disorder. Biol Psychiatry 52:119–125
Villarreal G, Hamilton DA, Graham DP et al (2004) Reduced area of the corpus callosum in posttraumatic stress disorder. Psychiatry Res 131:227–235
Watanabe YE, Gould H, Cameron D, Daniels D, McEwen BS (1992a) Phenytoin prevents stress and corticosterone induced atrophy of CA3 pyramidal neurons. Hippocampus 2:431–436
Watanabe Y, Gould E, Daniels DC, Cameron H, McEwen BS (1992b) Tianeptine attenuates stress-induced morphological changes in the hippocampus. Eur J Pharmacol 222:157–162
Wignall EL, Dickson JM, Vaughan P et al (2004) Smaller hippocampal volume in patients with recent-onset posttraumatic stress disorder. Biol Psychiatry 56(11):832–836
Winter H, Irle E (2004) Hippocampal volume in adult burn patients with and without posttraumatic stress disorder. Am J Psychiatry 161(12):2194–2200
Woodward SH, Kaloupek DG, Streeter CC et al (2006) Decreased anterior cingulate volume in combat-related PTSD. Biol Psychiatry 59(7):582–587
Yamasue H, Kasai K, Iwanami A et al (2003) Voxel-based analysis of MRI reveals anterior cingulate gray-matter volume reduction in posttraumatic stress disorder due to terrorism. Proc Natl Acad Sci USA 100(15):9039–9043
Yang P, Wu MT, Hsu CC, Ker JH (2004) Evidence of early neurobiological alternations in adolescents with posttraumatic stress disorder: a functional MRI study. Neurosci Lett 370(1):13–18
Yehuda R, Keefe RS, Harvey PD et al (1995) Learning and memory in combat veterans with posttraumatic stress disorder. Am J Psychiatry 152:137–139
Yehuda R, Golier JA, Harvey PD et al (2005a) Relationship between cortisol and age-related memory impairments in Holocaust survivors with PTSD. Psychoneuroendocrinology 30(7): 678–687
Yehuda R, Golier JA, Tischler L, Stavitsky K, Harvey PD (2005b) Learning and memory in aging combat veterans with PTSD. J Clin Exp Neuropsychol 27(4):504–515
Yehuda R, Golier JA, Tischler L et al (2007) Hippocampal volume in aging combat veterans with and without post-traumatic stress disorder: relation to risk and resilience factors. J Psychiatr Res 41(5):435–445
Zubieta JK, Chinitz JA, Lombordi U, Fig LM, Cameron OG, Liberzon I (1999) Medical frontal cortex involvement in PTSD symptoms: A SPECT study. Journal of Psychiatry Research 33:259–264
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2010 Springer Science+Business Media, LLC
About this chapter
Cite this chapter
Bremner, J.D. (2010). Imaging in CNS Disease States: PTSD. In: Borsook, D., Beccera, L., Bullmore, E., Hargreaves, R. (eds) Imaging in CNS Drug Discovery and Development. Springer, New York, NY. https://doi.org/10.1007/978-1-4419-0134-7_21
Download citation
DOI: https://doi.org/10.1007/978-1-4419-0134-7_21
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4419-0133-0
Online ISBN: 978-1-4419-0134-7
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)