
Abstract
India is one the world’s fastest-growing economies, but it struggles with high levels of poverty, malnutrition, and infant and maternal mortality rates. While the country has made strides in providing for a rights-based approach towards food, work and education, with much visible impacts on their developmental outcomes, two key fundamental rights—social insurance and health—have not received adequate policy attention. This chapter discusses the role of civil society mobilization and political support in ensuring entitlements with respect to work (albeit in rural areas), education and food and argues for a similar approach for ensuring universal health coverage, welcoming the Draft National Health Policy 2015, which advocates for health as a fundamental right. The chapter suggests immediate policy interventions, including the very critical aspect of sanitation, to address key health sector issues, particularly in India’s rural areas.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Gross Domestic Product
- Universal Health Coverage
- Maternal Mortality Ratio
- National Family Health Survey
- National Rural Health Mission
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
India’s economy has grown at an impressive rate in recent years, yet the incidence of income (or consumption) poverty remains large, with 269 million persons (or 22 percent of its population) living below the national poverty line.Footnote 1 Since 2004–2005, the absolute number of poor has been declining for the first time in India’s history, but the proportion of the population that suffers from capability deprivation is still high. This is demonstrated by the fact that one-third of adults suffer from malnutrition, around 30 percent of children below five years of age were considered malnourished in 2013 (Ministry of Women and Child Development 2015), 310 million persons (or 26 percent of the population) were illiterate and life expectancy at birth, although having risen, remained around 65 years in 2011 (IAMR 2011).
India remains an outlier among emerging market economies in terms of the share of workers in informal employment (93 percent) (Mehrotra et al. 2013). It is expected that social insurance will be available for the unorganized sector workers, in addition to universal coverage of preventive and even public health care. However, both a social insurance system and the public health system are limited in coverage and fragmented in character; lacunas which will be addressed in this chapter.
The progression of India’s welfare system from treating citizens as mere beneficiaries of state-provided welfare to a rights-based approach is a relatively recent one. The implementation of the right to work (albeit in rural areas), the right to education and the right to food demonstrate major achievements towards an entitlements-based approach. However, in a country where a large proportion of the population lives below the poverty line and a huge proportion of the workforce is in informal employment, it is imperative that all persons have access to universal preventive and public health services. Furthermore, full coverage of social insurance (old age pension, death and disability insurance, maternity benefits) should be available at least to the poor among those who work in the informal sector. In the absence of publicly provided health care, such insurance might allow access to a preventive and basic curative care package.
In light of these goals, this chapter examines the strengths and weaknesses of India’s health care system. It discusses the factors leading to the enactment of fundamental rights—to work, education and food—then presents health outcome indicators and an overview of India’s health sector before making a case for universal health coverage.
Right to Employment, Right to Education and Right to Food
Human rights and human development are interrelated (Alston and Bhuta 2005). Moreover, rights or entitlements, by their very definition, impose claims on other people or institutions to help or collaborate in ensuring access to some freedom (UNDP 2000).
In India, Article 21 of the Constitution guarantees a fundamental right to life and personal liberty and Article 47 of the Constitution makes it one of the primary duties of the State to raise the standard of nutrition and the standard of living and to improve the public health of its people. In addition, the provision of social protection is enshrined in Articles 38 (securing a social order for the promotion of welfare of the people), 39 (certain principles of policy), 41 (right to work, education, and public assistance in certain cases), 42 (just and human conditions of work and maternity relief) and 43 (living wage, etc.) of the Constitution as part of the Directive Principles of State Policy. In this context, civil society mobilization and political support have resulted in a focus on universalization and entitlements in respect of education, employment and food.
In the legal context, an important development has been the decision of the highest appellate court—the Supreme Court of India in the early 1980s—to waive off traditional doctrines of standing and pleadings to permit concerned citizens, public interest advocates and non-governmental organizations to petition it on behalf of individuals or communities suffering violations of constitutionally protected rights (Alston and Bhuta 2005). By way of development of its Public Interest Litigation jurisdiction, the Supreme Court of India has come to act as a “combination of constitutional ombudsman and inquisitorial examining magistrate, vested with responsibility to do justice to the poor litigant before it by aggressively searching out the facts and the law, and by taking responsibility for fully implementing its decisions” (Neuborne 2003: 503).
Furthermore, the National Advisory Council (NAC), created in 2004, provided support to the idea that the state has a key role to play in the provision of minimum levels of employment, education and food as basic entitlements to every needy citizen in the country.
The NAC, along with the civil society movement, was instrumental in the enactment of the National Rural Employment Guarantee Act in 2005. The NAC also played a key role in providing impetus to the government’s flagship programmes in rural health, nutrition, education, infrastructure and urban renewal. For the purpose of this chapter, it is important to note that the NAC was a creation of the central government, led by the Congress Party (2004–2014), and was disbanded by the new government (led by the Bhartiya Janata Party) in May 2014. The new government announced in early 2015 a new National Policy Framework for Health.
Before turning to a further discussion of health, we present below some landmark legislation of recent times—the right to employment, right to education and right to food.
Right to Employment
In India, a major focus for rural development has been the productive absorption of the underemployed and surplus labour by the provision of direct supplementary wage employment to the rural poor through public works (Second Administrative Reforms Commission 2006). The Mahatma Gandhi National Rural Employment Guarantee Act (MGNREGA) of 2005 represented a paradigm shift towards fulfilling the long-standing demands of the Right to Food Campaign and the labour movement in India. The Act stipulated that any adult willing to undertake casual labour at the minimum wage is entitled to employment on local public works within 15 days, subject to a limit of 100 days per household per year (Gazette of India 2005).
Under the MGNREGA, an employment scheme was launched, implemented during the period 2006–09 to cover all the 600-odd rural districts in the country. The scheme sought to enhance the income of the poor by providing employment, and through the process of employment helped to create durable assets leading to much-needed productive infrastructure for sustainable poverty alleviation. Moreover, it has been suggested that the worker’s organizations would lead to linking the employment guarantee with social security schemes, and the greater bargaining power would also help rural workers in the realization of other social and economic rights (Drèze and Khera 2009).
It is argued that the challenges for successful implementation of the MGNREGA stem from five factors: the focus on universalization and entitlements; the funding by the union government and execution by the state governments; the centrality of local governments; administrative and institutional arrangements; and the problems in less developed areas (Second Administrative Reforms Commission 2006). Furthermore, for the success of any entitlements-based programme, close attention should be paid to the circumstances that shape people’s perceptions of their rights as well as their ability to enforce them (Drèze 2004).
It is worth mentioning that as a result of the MGNREGA, rural open market wages have risen from Indian Rupee (INR) 65 in 2006–07 to INR 128 in 2012–13, partly because the wages provided under the programme were higher than the prevailing rural market wages (The Hindu 2014). The MGNREGA made work available locally, giving landless labourers an alternative to migrating to urban or other rural areas in search of work, or working on the landlord’s farm (Mehrotra 2008). An impact evaluation of the MGNREGA using the capability approach finds a significant expansion in the capability set of the individuals interviewed (Dasgupta 2013).
Right to Education
The right to education was first recognized as a fundamental right by the Supreme Court of India in the judgement of Mohini Jain v. Union of India (1992) 3 SCC 666. A strong civil society demand for the right to education was responsible for its enactment. In December 2002, the Indian Parliament passed the 86th Amendment to the Indian Constitution, which mandated the provision of free and compulsory education. After a participatory process of inviting comments from members of the public, the Right of Children to Free and Compulsory Education Act or Right to Education (RTE) Act was passed by the Indian Parliament in August 2009 and came into force in April 2010.
The RTE Act guarantees free and compulsory education to all children aged 6–14 years, stipulates a pupil–teacher ratio of 30:1 at the primary level and 35:1 at the upper primary level, and has provisions for improvements in school infrastructure (IAMR 2011). Schooling is provided free-of-cost (including indirect costs such as uniforms, books and transportation) until a child’s elementary education is completed.
The Sarva Shiksha Abhiya n (SSA), a programme working towards the universalization of elementary education which pre-dated the RTE Act, is now implemented in partnership with state governments to cover the entire country. SSA seeks to open new schools where facilities are lacking and to strengthen existing school infrastructures through the provision of additional classrooms, toilets, drinking water, maintenance grants and school improvement grants.Footnote 2
The impact of the RTE remains questionable, however. The Annual Status of Education Report (Pratham 2012) found that India is very close to achieving universal enrolment, with levels for children aged 6–14 years at 96 percent enrolment or more for the previous four years. However, though pupil–teacher ratios have shown improvement in rural areas, learning levels have dropped in many states since the RTE Act came into effect. This may be attributed to the absence of exams and assessments in the new regime, leading to the relaxation of teaching and productivity.
Right to Food
The Right to Food Campaign is an informal network of organizations and individuals campaigning for the realization of the right to food, through the state guarantee of entitlements relating to livelihood security, such as the right to work, land reform and social security. The campaign began with a writ petition submitted to the Supreme Court in April 2001 by the People's Union for Civil Liberties, Rajasthan. This was followed by a larger public campaign resulting in the Supreme Court of India appointing Commissioners on the right to food.
As a result of civil society mobilization and political support, the government approved the National Food Security Act (NFSA) in 2013. The entitlements under the NFSA include an assured quota of subsidized food grains (rice, wheat and millets) from the Public Distribution System (PDS), maternity benefits for all pregnant women and nutritious meals for children through local Anganwadis or primary schools. The NFSA aims to cover 75 percent of rural and 50 percent of urban populations (Department of Food and Public Distribution).Footnote 3
It has been argued that for the NFSA to have an impact on hunger in India there needs to be improvement in the governance, productivity and accountability of the public sector. Major food-related programmes, such as the PDS of wheat and rice and Integrated Child Development Services, are plagued by corruption, leakages, errors in selection, procedural delays, poor allocations and little accountability. Moreover, they discriminate against and exclude those who need them the most (Saxena 2012; Mander 2012). It has also been argued that the magnitude of the subsidy under NFSA is huge and thus imprudent (Bhalla 2013). Unless the PDS is radically reformed, it has been suggested that a cash transfer equivalent to the value of the cereals entitlement would be more appropriate (at least in cities).
Despite a plethora of demands for a comprehensive “Food Entitlements Act” from the Right to Food Campaign, state governments have failed to reform PDS and the NFSA has been implemented in only 11 of India’s 29 states.
The India Human Development Report (IAMR 2011) highlighted a conceptual framework regarding the feedback loops that run through human development inputs and outcomes. Thus, nutrition, education and income (employment) are all important inputs that feed into better health outcomes. The above narrative suggests that these entitlements-based public programmes can play a crucial role in improving overall human development outcomes, including indirectly health outcomes, provided they are timely and adequately monitored and evaluated.
The Two Missing Rights: Social Insurance and Health
While progress has been made towards the three fundamental rights in India—education, food and work—there are two that are completely absent: social insurance and health.
It is argued that social security consists of two categories of support to workers: first, social assistance and second, social insurance (Mehrotra 2015). Social assistance (assistance in kind or cash) is intended for those who are unable to work (for example, the old and indigent, disabled and poor widows) or those who are unable to earn enough from work to guarantee a basic income or consumption level. Social insurance is intended for those able to work but with limited access to a safety net that is normally available in the organized sector as a form of health coverage (old age pension, maternity benefit and death or disability benefit). It is argued that the Indian state has so far failed to provide effective social insurance for its people (Mehrotra 2015).
Social security interventions remain fragmentary in India. Government-sponsored and -administered programmes dominate pension and health insurance provision in India. However, in distributional terms, social security coverage is concentrated in the upper part of the income distribution and fails to reach the vast majority of the population. One of the reasons for this low coverage of social security is the extent of the informal work sector (World Bank 2011b). While 93 percent of the Indian labour force is in informal employment, less than 1 percent of workers in the unorganized sector have any formal pension coverage through public schemes. The coverage through commercial schemes is only 1.2 percent for personal accident insurance, 0.5 percent for private health insurance and 23 percent for life insurance (O’Keefe 2005).
A social insurance programme, it is argued, should be comprised of three components—old age pension, death and disability benefit (or life insurance) and maternity benefit in line with the internationally recognized minimal requirements by the International Labour Organization’s 2012 Social Protection Floors Recommendation (ILO 2012). These safety nets provide crucial support in times of health hazards which can potentially hurt poor families and push them further into the shackles of poverty. In line with the needs of the unorganized sector as highlighted in the NCEUS report (NCEUS 2008), we argue that social insurance should also include a national health insurance mechanism for those in the unorganized sector. Thus, providing for social insurance and universal preventive health care systems are important concerns to be addressed in developing country frameworks to improve the overall productivity and capabilities of their population.
Health Outcome Indicators
Health is an important facet of human development and well-being. Health inputs as well as health outcomes have important implications for nutritional and learning outcomes. Ensuring universal coverage of health services is an important component in universalizing social protection. An assessment of health outcome, process and input indicators reveals that despite the National Rural Health Mission (NRHM),Footnote 4 progress in terms of these indicators has been slow to be able to achieve the Millennium Development Goals (MDGs) (IAMR 2011).
The development goal to eradicate extreme poverty and hunger required halving the proportion of those suffering from hunger between 1990 and 2015. The estimate of underweight children (an indicator of food insecurity) has shown some improvement in the past decades. While the proportion of underweight children aged 0–3 years was 53.5 percent in 1990, it was estimated to be 47 percent in 1998–99 according to the second National Family Health Survey (NFHS), and 46 percent in 2005–06 as per the third NFHS. A 2013 survey by the central government (supported by UNICEF) provided the latest available estimates and found that the level of malnutrition had fallen to around 30 percent (Ministry of Women and Child Development 2015). The MDGs, however, required this proportion to be reduced to 27 percent by 2015—a goal which was ultimately not met.
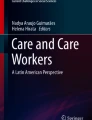
The development goal to reduce child mortality required reducing the under-five mortality rate (UFMR) by two-thirds between 1990 and 2015, as well as reducing the infant mortality rate (IMR) to 26.7 per 1000 live births by 2015. There has indeed been progress in reducing child mortality rates in the last two decades, although much remains to be achieved (see Fig. 11.1). While IMR declined from 80 per 1000 live births in 1990 to 68 in 2000, the pace of decline slowed during the next decade, when IMR fell by only 24 points to reach 40 per 1000 live births in 2013 (Registrar General 2014). In order to achieve the MDG target, IMR would have needed to decline by another 13 points in the remaining two years.

Infant mortality rate (IMR), under-five mortality rate (UFMR) and total fertility rate (TFR) in India (Source: Author based on data from World Development Indicators)
The inter-state differences in IMR are more worrisome (see Fig. 11.2). While the national average in 2013 was 40 per 1000 live births, and the lowest was in Kerala (12), the relatively poorer states recorded an IMR much higher than the national average—Assam (54), Madhya Pradesh (54), Odisha (51) and Uttar Pradesh (50) (Registrar General 2014).

Infant mortality rate in selected Indian states, 2013 (Source: Author based on data from Registrar General, Government of India (various years))
The UFMR, or the probability of a child not surviving to his/her fifth birthday, stood at 125 per 1000 live births in India in 1990. The MDG target was to reduce UFMR to 42 per 1000 live births by 2015. It declined to 85 per 1000 live births in 2000, to 55 in 2011, to 52 in 2012, and further to 49 in 2013 (Registrar General various years). However, for the poorer states of Assam (73), Madhya Pradesh (69), Odisha (66) and Uttar Pradesh (64), high levels of child mortality rates reflect the inefficiency of the public health institutions as well as a lack of entitlements for healthy living. These also implicate gaps in child immunization practices.
According to the third NFHS, 44 percent of children received all vaccinationsFootnote 5 in 2005–06. This proportion was lower in rural areas where it was 39 percent, and even lower for rural areas of Assam and Madhya Pradesh (32 percent), Bihar (31 percent), Jharkhand (30 percent), Rajasthan (22 percent) and Uttar Pradesh (21 percent). In 2007–08, as per the District Level Household and Facility Survey estimates, 54 percent of all children received all vaccinations. However, in Madhya Pradesh, only about one-third of children received all vaccinations, a number that was even lower in Uttar Pradesh (IAMR 2011).
The health and nutritional status of the child is critically dependent on the mother’s health and care taken during pregnancy and delivery. The maternal mortality ratio (MMR) measures the number of women of reproductive age dying per 100,000 live births due to maternal causes. MMR was as high as 560 in India in 1990–91 and the MDG target was set at 140 by 2015. MMR declined dramatically to 301 per 100,000 live births in 2001–03 and declined by 89 points to reach 212 per 100,000 in 2007–09. The MMR stood at 178 in 2010–12, falling to 167 in 2011–13 (Registrar General various years), but still far from the MDG target of 140.
At the state level, it is seen that Kerala (66), Tamil Nadu (90), Maharashtra (87) and Andhra Pradesh (110) have realized the MDG target of 140 per 100,000 live births. The most significant decline in average MMR, from 308 to 257, was seen in those states participating in the Empowered Action GroupFootnote 6 and in Assam. However, Assam remained a major drag on the MMR with 328 deaths per 100,000 live births, along with Odisha (235), Rajasthan (255) and Uttar Pradesh/Uttarakhand (292). The suboptimal performance in terms of these indicators (child mortality and MMR) reflect the gaps in antenatal care, skilled birth attendance and emergency obstetrical care in these relatively poorer states (Planning Commission 2013).
High MMRs can be attributed to the high incidence of non-institutional deliveries. Continued high rates of child and maternal mortality suggest that the public health system has been ineffective in promoting reproductive and child health programmes and healthy practices such as breastfeeding, the use of oral rehydration salts, and preventive and care-seeking behaviours (Planning Commission 2013). Indian women suffer, in particular, due to their limited access to health care services during pregnancy. According to the third NFHS estimates for 2005–06, only 52 percent women had three or more antenatal care check-ups.
On average, only 39 percent of deliveries took place in an institution in India, according to NFHS data for 2005–06. In rural areas, the figure was even lower at 29 percent. According to the District Level Health Survey data, 47 percent of women aged 15–49 years had an institutional delivery in 2007–08. The Sample Registration System (SRS) of the Registrar General of India estimates of 2011, however, show that there has been a sharp rise in institutional deliveries, which can be attributed to the success of NRHM and the Janani Suraksha Yojana.Footnote 7 The percentage distribution of births by type of medical attention at delivery shows that about 13 percent of live births occurred in the presence of untrained functionaries or others. Government and private hospitals respectively accounted for 50 percent and 24.4 percent of deliveries, the remainder being accounted for by other qualified professionals (like female health workers or auxiliary nurse midwives) (Registrar General SRS Statistical Report 2013).
Health Sector Overview
The performance illustrated by the health outcome indicators indicates gaps in the health system of the country. Improving the health conditions of the population requires investment in health infrastructure and human resources (IAMR 2011). The expenditure (public and private) on health has been abysmally low in India, hovering at around 4 percent of gross domestic product (GDP) in 2010 with the share of public expenditure in total health expenditure at 28 percent. The higher proportion of private expenditure on health results from the high out-of-pocket costs incurred by private households (86 percent of total private expenditure) (DGHS 2013). High out-of-pocket expenditure on health, especially by those belonging to the poorer sections of the society, often pushes them below the poverty line, particularly in the case of certain unforeseen circumstances.
In 2011–12, the combined public expenditure on health reached 1.04 percent of GDP. With additional spending on drinking water and sanitation, as well as the Integrated Child Development Scheme and Mid Day Meal Scheme, public expenditure on health rose to 1.97 percent of GDP in the period 2007–12. From 2012 to 2017, it is expected to rise to 2.5 percent of GDP (Planning Commission 2013; IAMR 2011).
Low public expenditure on health also reflects gaps in health infrastructure for both physical as well as human resources. Health infrastructure indicates the quality of health care delivery and, in turn, affects health outcomes. Despite the NRHM and increases in public expenditure in health, National Health Profiles for 2005 and 2013 (DGHS 2005, 2013) present an insubstantial increase in the number of subcentres (142,655 in 2004 to 151,684 in 2013), primary health centres (23,109 in 2004 to 24,448 in 2013) and community health centres (3222 in 2004 to 5187 in 2013). According to the World Development Indicators of the World Bank, compared to the figure of 36 hospital beds per 10,000 people in China, India has just nine hospital beds per 10,000. The severe shortage of public health infrastructure can be illustrated by the fact that the average population served per government hospital is 98,970. The situation is much more severe in certain other states, however: it is as high as 451,325 in the case of Bihar, 229,118 in Uttar Pradesh, 194,863 in Assam, 178,243 in Andhra Pradesh, 159,721 in Haryana, 155,470 in Madhya Pradesh and 139,676 in West Bengal. The average population served per government hospital bed is 1,512, but is more than 5,000 in the cases of Bihar and Jharkhand and over 3,500 in Uttar Pradesh and Assam (DGHS 2011).
The availability of skilled human resources is an important prerequisite for effective health service delivery. The number of allopathic doctors possessing recognized medical qualifications (under the Medical Council of India Act) and registered with state medical councils increased from 656,111 in 2005 to 921,877 in 2011 (an increase of around 40 percent). There has also been an improvement in the average population served per government allopathic doctor from 15,980 in 2005 to 12,005 in 2011. However, the increase in doctors in primary health centres in rural areas was only 20 percent over this period. It is noteworthy, however, that there was an almost 50 percent increase in female health workers or auxiliary nurse midwives between 2005 and 2011 (see Table 11.1).
In 2008, the government launched its flagship health insurance scheme for the poor: the Rashtriya Swasthya Bima Yojana (RSBY).Footnote 8 This combines technology with incentives to provide inpatient insurance coverage up to an annual sum of INR 30,000 for eligible enrolled households. The RSBY is implemented through insurance companies with premiums subsidized by union and state governments to the extent of 75 percent and 25 percent respectively.
The population coverage under various publicly financed health insurance schemes increased from almost 55 million people in 2003–04 to about 370 million in 2014 (or almost one-quarter of the population) (Ministry of Health and Family Welfare 2014). However, this coverage is low given that 50–60 percent of the country’s population is vulnerable to poverty. It is argued that insurance schemes that cover only hospital expenses, such as those being rolled out nationally in India, will fail to adequately protect the poor against impoverishment due to the extent of many other health care costs beyond hospitalization (Shahrawat and Rao 2012).
Another study finds that the impact of RSBY on financial risk protection in India’s health care is questionable (Selvaraj and Karan 2012). An examination of the poorer households in intervention districts of the RSBY, Rajiv Aarogyasri of Andhra Pradesh and Tamil Nadu Health Insurance schemes finds a rise in real per capita health care expenditure, particularly with regard to hospitalization, and an increase in catastrophic headcount, defined as the “number of households making out-of-pocket payment expenditure greater than 10 percent of their total household expenditure” (Selvaraj and Karan 2012: 62). This is “a conclusive proof that RSBY and other state government-based interventions failed to provide financial risk protection” (Selvaraj and Karan 2012: 60).
Towards Universal Health Coverage
In India, inequalities in health care by socioeconomic status, geography and gender persist, and three-quarters of health spending is private. Moreover, health expenditures are responsible for pushing around 39 million Indians into poverty each year. Consequently, India’s health care system is posed with the challenge of responding to the needs of the most disadvantaged members of the Indian society (Balarajan et al. 2011).
While the civil society movements for the rights to education and work are long-standing and were largely responsible for the enactment of those rights, the historical civil society momentum for the right to health is missing. Health, both as the state subject and later as the concurrent subject, continued to be neglected until the 1990s. Economic reforms to dismantle the ‘licence-quota raj’ in the economy were characterized by liberalization and deregulation since 1991. For the health sector, this reform period was characterized by a mindset that favoured the introduction of user charges in public hospitals, private sector development and the growth of private health care. Also, public health issues as safe sanitation were recognized as important only in the last decade—according to the Census of India 2011 estimates, 69 percent of all households in rural India did not have a toilet—though the mindset started to change after the economic growth picked up in 2003–04. These developments have set the stage for a demand for universal health care in India.
More recently, the draft National Health Policy (Ministry of Health and Family Welfare 2014) proposes to make the right to health justiciable:
The Center shall enact, after due discussion and on the request of three or more States (using the same legal clause as used for the Clinical Establishments Bill), a National Health Rights Act, which will ensure health as a fundamental right, whose denial will be justiciable. States would voluntarily opt to adopt this by a resolution of their Legislative Assembly. States which have achieved a per capita public health expenditure rate of over INR 3800 per capita (at current prices) should be in a position to deliver on this—and though many States are some distance away—there are states which are approaching or have even reached this target. (Ministry of Health and Family Welfare 2014: 56)
It is argued that such a policy formulation/resolution would be the right signal to give a push for increased public health expenditure, as well as for the recognition of health as a basic human right and its realization as a goal that the nation must set for itself. The draft policy aims at increasing the government expenditure on health to 2.5 percent of GDP from the currently abysmal rate of 1 percent, ensuring universal access to free drugs and diagnostics at government hospitals. The proposal for a National Health Rights Act, along similar lines to those covered in the Act, is indeed a very welcome step in ensuring an individual’s fundamental right to universal access to affordable health care services. However, the existing apparatus poses dire challenges in achieving a public health care system that enacts health as a fundamental right, whose denial can be “justiciable”.
A high-level expert group (HLEG) on universal health coverage (UHC) was earlier constituted in 2010 by the Planning Commission of India. It was entrusted with the mandate of developing a framework for providing easily accessible and affordable health care to all. In its report the HLEG recognized that it is possible for India, even with the financial resources available to it, to devise an effective architecture for health financing and financial protection that can offer UHC to every citizen. The HLEG made recommendations regarding a number of different areas: health financing and financial protection; access to medicines; vaccines and technology; human resources for health; health service norms; management and institutional reforms; community participation and citizen engagement; and gender and health (Planning Commission 2011).
The recommendations of the HLEG are wide-ranging and lack prioritization. We argue that India needs to focus on five key areas given the scarcity of resources and especially human resources for health.
First, all doctors should be required to serve in rural areas regardless of the requirement for a postgraduate seat (Rao et al. 2012).Footnote 9 Several states in India—Assam, Arunachal Pradesh, Chhattisgarh, Gujarat, Kerala, Manipur, Meghalaya, Nagaland, Orissa, Tamil Nadu and West Bengal—have made it compulsory for all the medical graduates to serve in rural areas (Gupta et al. 2010).We argue that this policy should be extended to all states on account of the huge public subsidy on doctors’ education, and cite the experience of Sri Lanka, where the compulsory rural posting of doctors in the 1950s enabled substantial reduction in mortality in all areas and in every population group (Rannan-Eliya and Sikurajapathy 2008; Alailama and Sanderatne 1997).
Second, there is a strong case for the introduction of a three-year course for rural practice in all states in line with the experience of rural medical assistants in the state of Chhattisgarh (Rao et al. 2010). In many states of India, AYUSH (Ayurveda, Yoga, Unani, Siddha and Homeopathy) physicians are posted at primary health centres in an attempt to mainstream the Indian systems of medicine. Often they are the sole clinician present and practice both allopathic and their own system of medicine (Rao and Ramani 2013). Clinicians with three years’ training in allopathic medicine operate in two states. In the state of Chhattisgarh, rural medical assistants are posted at primary health centres, and in the state of Assam, rural health practitioners are posted at subcentres. In a recent initiative, the Central Health Ministry proposed the introduction of a national three-year clinician course, the Bachelor’s degree in Rural Health Care, with the intention of stationing these graduates at rural subcentres (Rao and Ramani 2013). A study on non-physician clinicians in the state of Chhattisgarh found that physicians and clinicians with shorter duration clinical training (that is, rural medical assistants) were equally competent in managing conditions commonly seen in primary care settings (Rao et al. 2010).
Third, more regular staff or paramedics are needed to manage services and as frontline providers of services. The nurse to doctor ratio in India (1.5:1 instead of the desirable 3:1) is poor in comparison with other countries (Reddy 2012). This is because nursing training institutions have been left to wither, despite a great need for nursing skills.
The availability of competent and committed health workers requires that attention be paid to both the numbers and the quality of these workers. There is a huge need to establish new medical and nursing colleges. In addition, priority should be given to locating these new colleges in states which have very few training facilities, and they should preferably have linkages with the district hospitals. The training of health professionals has to emphasize health system connectivity, problem-solving skills, team functioning and partnership with the community (Reddy 2012).
Fourth, the essential drug procurement system needs to be revamped. Essential drugs should be available at affordable prices in the public health system. To strengthen the logistics and management system of health care, Tamil Nadu Medical Services Corporation was established in January 1995, which is the apex body for purchase and distribution of generic essential drugs for government medical centres in the state.
Fifth, sanitation is important in terms of both nutrition and securing improvements in health status. For example, India accounts for nearly 60 percent of the 626 million people in the world who defecate in the open (and also 90 percent of the total in South Asia). This number is more than double that of the next 18 countries combined where open defecation is prevalent (UNICEF and WHO 2012). As per National Statistical Survey Organization data, the percentage of the population who have no access of any type of toilet facility was approximately 60 percent in 2002 and had improved only very little, to 49 percent, by 2009 (IAMR 2011). The approximate economic loss due to lack of adequate sanitation could be as huge as INR 2.4 trillion in a year, constituting approximately 6.4 percent of India’s GDP in 2006 (Water and Sanitation Program 2011). These costs are associated with death, disease, accessing and treating water, as well as losses in education, productivity, time and tourism.
Improved sanitation has a direct impact on health, leading to other positive externalities. First, improved sanitation impacts directly on nutrition by reducing the probability of water-borne diseases resulting in conditions such as diarrhoea, which significantly affects the nutrient-absorbing capacity in individuals. Constant exposure to such diseases results in lower nutritional status and poor health outcomes. Since malnutrition accounts for half of all child deaths, sanitation also impacts health and nutrition outcomes such as mortality rates, height for age, etc. Second, improved sanitation in schools improves the enrolment rates of girls. Moreover, the effects of improved sanitation in schools go well beyond enrolment, and extend to actual learning and better cognitive skills (Mehrotra and Ghosh 2013).
Concluding Remarks
In this chapter, we have discussed the key role of civil society mobilization and political support through the NAC in India, resulting in a focus on universalization and entitlements with regards to work (albeit in rural areas), education and food. However, two rights are only available to a very limited share of the population: social insurance and health. The health system in India remains weak due to limited coverage and low public expenditure on health, leaving the poorest people vulnerable to poverty. Furthermore, this chapter finds that the government’s flagship health insurance scheme for the poor, the RSBY, remains ineffective in terms of providing financial risk protection for India’s health care, with inadequate coverage which does not include consultations outside of hospitalization. Last but not least, it argues for universal health coverage in India and suggests areas for immediate policy intervention in the health sector.
Notes
- 1.
This poverty line is quite close to the international poverty line of USD 1.25 per person per day.
- 2.
See http://ssa.nic.in/ (accessed September 2015).
- 3.
Department of Food and Public Distribution website, accessed 13 March 2016. http://dfpd.nic.in/nfsa-act.htm.
- 4.
The NRHM was launched in April 2005, to provide accessible, affordable and quality health care to the rural population, especially the vulnerable groups.
- 5.
One BCG injection to protect against tuberculosis, three doses each of DPT (diphtheria, pertussis, tetanus) and polio vaccines, and one measles vaccine.
- 6.
The Empowered Action Group was set up to facilitate preparation of area-specific programmes in eight states, namely Bihar, Jharkhand, Madhya Pradesh, Chhattisgarh, Orissa, Rajasthan, Uttar Pradesh and Uttaranchal, which have lagged behind in containing population growth to manageable levels.
- 7.
Janani Suraksha Yojana is a safe motherhood intervention under the NRHM. It is being implemented with the objective of reducing maternal and neonatal mortality by promoting institutional delivery among poor pregnant women. The scheme is under implementation in all states and union territories, with a special focus on “low performing states”.
- 8.
A well-designed and implemented health insurance may both increase access to health care and may even improve its quality over time. The RSBY provides the participating below-poverty line household with freedom of choice between public and private hospitals and makes them a potential client worth attracting on account of the significant revenues that hospitals stand to earn through the scheme. The coverage extends to five members of the family, which includes the head of the household, a spouse and up to three dependents. Beneficiaries need to pay only INR 30 or lower as a registration fee while central and state government pays the premium to the insurer selected on the basis of a competitive bidding. The budgetary allocation for RSBY was INR 264.51 crore in 2009–10, INR 445.89 crore in 2010–11, and INR 279.94 crore in 2011–12 (Source: http://www.rsby.gov.in/, accessed 13 March 2016).
- 9.
From the experience of two Indian states, Uttarakhand and Andhra Pradesh, it is argued that linking postgraduate programmes to rural service appears to be an influential incentive for attracting doctors to rural posts. There is a strong desire for specialization among doctors after medical qualification (MBBS), which, coupled with few available postgraduate seats compared to the number of medical graduates, makes for intense competition in obtaining admission to postgraduate programmes (Rao et al. 2012).
Bibliography
Alailama, P., and N. Sanderatne. 1997. Social development in a slowly growing economy: Sri Lanka. In Development with a human face: Experiences in social achievement and economic growth, ed. Santosh Mehrotra and Richard Jolly, 235–263. Oxford: Oxford University Press.
Alston, Philip, and Nehal Bhuta. 2005. Human rights and public goods: Education as a fundamental right in India, Center for Human Rights and Global Justice. Working Paper No. 6, Economic, social and cultural rights series, NYU School of Law.
Balarajan, Yarlini, S. Selvaraj, and S.V. Subramanian. 2011. Health care and equity in India. The Lancet 377(9764): 505–515.
Bhalla, Surjit. 2013. Manmonia’s FSB: 3% of GDP. The Financial Express, July 6.
Dasgupta, Poulomi. 2013. Employment guarantee schemes and long-term development: A case study of the NREGA in India. In Employment guarantee schemes: Job creation and policy in developing countries and emerging markets, ed. Michael J. Murray and Mathew Forstater, 103–125. Basingstoke: Palgrave Macmillan.
DGHS (Directorate General of Health Services), Government of India. 2005 National health profile. New Delhi: Central Bureau of Health Intelligence.
———. Government of India. 2011, National health profile. New Delhi: Central Bureau of Health Intelligence.
———. Government of India. 2013, National health profile. New Delhi: Central Bureau of Health Intelligence.
Drèze, Jean. 2004. Democracy and right to food. Economic and Political Weekly 39(17): 1723–1731; Gazette of India. 2005. The National Rural Employment Guarantee Act. No. 42 of 2005. http://nrega.nic.in/rajaswa.pdf. Accessed Sept 2015.
Drèze, Jean, and Reetika Khera. 2009. The battle for employment guarantee. Frontline 26(1): 3–16.
Gazette of India. 2005. The National Rural Employment Guarantee Act. No. 42 of 2005. http://nrega.nic.in/rajaswa.pdf. Accessed September 2015.
Gupta, G., T. Sundararaman, and K. Rao. 2010. Human resources for health in India: Strategies for increasing the availability of qualified health workers in underserved areas. www.nhsrcindia.org. Accessed June 2010.
IAMR (Institute of Applied Manpower Research, India). 2011. India human development report 2011: Towards social inclusion. New Delhi: Oxford University Press.
ILO (International Labour Organization). 2012. R202—Social protection floors recommendation. Geneva: ILO. http://www.ilo.org/dyn/normlex/en/f?p=NORMLEXPUB:12100:0::NO::P12100_INSTRUMENT_ID:3065524. Accessed 13 Mar 2016.
Mander, Harsh. 2012. Ending indifference: A law to exile hunger? Journal of the National Human Rights Commission India 11: 39–52.
Mehrotra, Santosh. 2008. NREG two years on: Where do we go from here? Economic and Political Weekly 43(31): 27–35.
———. 2015. Realising the demographic dividend: Policies to achieve inclusive growth in India. New Delhi: Cambridge University Press.
Mehrotra, Santosh, and Deboshree Ghosh. 2013. Addressing the world’s worst sanitation problem: A programme re-design to use not just build toilets. IAMR Occasional Paper 2/2013. New Delhi: Institute of Applied Manpower Research.
Mehrotra, Santosh, Ankita Gandhi, Partha Saha, and Bimal K. Sahoo. 2013. Turnaround in India’s employment story: Silver lining amidst joblessness and informalization? Economic and Political Weekly 48(35): 87–96.
Ministry of Health and Family Welfare, Government of India. 2014. National health policy 2015: Draft. http://www.mohfw.nic.in/showfile.php?lid=3014. Accessed Sept 2015.
Ministry of Women and Child Development, Government of India. 2015. Rapid survey on children 2013–14: India Fact Sheet. Provisional results, July 2015. http://wcd.nic.in/issnip/National_Fact%20sheet_RSOC%20_02-07-2015.pdf. Accessed Mar 2016.
NCEUS (National Commission on Enterprises in the Unorganized Sector). 2008. Conditions of work in the unorganized sector. New Delhi: Government of India.
Neuborne, B. 2003. The supreme court of India. International Journal of Constitutional Law 1(3): 476–510.
O’Keefe, P. 2005. Strengthening employment and social security for unorganized sector workers in India. World Bank. Mimeo.
Planning Commission, Government of India. 2011. High level expert group report on universal health coverage for India. New Delhi: Government of India. http://planningcommission.nic.in/reports/genrep/rep_uhc0812.pdf. Accessed Mar 2016.
———. 2013. Twelfth five year plan (2012–2017). New Delhi: Government of India.
Pratham. 2012. Annual status of education report. New Delhi: ASER Centre. img.asercentre.org/docs/Publications/ASER%20Reports/ASER_2012/fullaser2012report.pdf. Accessed Mar 2016.
Rannan-Eliya, Ravi P., and Lankani Sikurajapathy. 2008. Sri Lanka: ‘Good Practice’ in expanding health care coverage. Washington, DC: The International Bank for Reconstruction and Development.
Rao, K.D., and S. Ramani. 2013. What works, where, and how well? Lessons from a comparative assessment of current rural retention strategies for doctors in India. Human Resources Technical Paper II. Public Health Foundation of India. http://uhc-india.org/downloadpdf.php?link=Ruralretentionstrategies-LessonsfordoctorsinIndia-E.pdf. Accessed August 2013.
Rao, K.D., G. Gupta, K. Jain, A. Bhatnagar, T. Sundararaman, P. Kokho, et al. 2010. Which doctor for primary health care? An assessment of primary health care providers in Chhattisgarh, India. New Delhi: Public Health Foundation.
Rao, K., Z. Shroff, S. Ramani, S. Murthy, I. Hazarika, N. Khandpur, and M. Chokshi. 2012. How to attract health workers to rural areas in India? Findings from a discrete choice experiment. Washington, DC: World Bank.
Reddy, K. Srinath. 2012. Universal health coverage in India: The time has come. The National Medical Journal of India 25(2): 65–67.
Registrar General, Government of India. 2014. Sample Registration System (SRS) Bulletin, September 2014. New Delhi: Office of the Registrar General and Census Commissioner.
______ . Various years. Sample Registration System (SRS) Statistical Reports. New Delhi: Office of the Registrar General and Census Commissioner.
Saxena, N.C. 2012. Food security and hunger in India. Journal of the National Human Rights Commission India 11: 53–64.
Second Administrative Reforms Commission. 2006. Unlocking human capital: Entitlements and governance, a case study. New Delhi: Government of India.
Selvaraj, Sakthivel, and Anup K. Karan. 2012. Why publicly financed health insurance schemes are ineffective in providing financial risk protection. Economic and Political Weekly47(11): 60–68.
Shahrawat, Renu, and Krishna D. Rao. 2012. Insured yet vulnerable: Out-of-pocket payments and India’s poor. Health Policy and Planning 27: 213–221.
The Hindu. 2014. Now, 150 workdays for Tribals under MGNREGA. The Hindu, 28 February 2014. http://www.thehindu.com/news/national/now-150-workdays-for-tribals-under-mgnrega/article5736740.ece. Accessed Sept 2015.
UNDP (United Nations Development Programme). 2000. Human development report 2000: Human rights and human development. New York: Oxford University Press.
UNICEF and WHO. 2012. Progress on drinking water and sanitation: 2012 update. New York: UNICEF. http://www.unicef.org/media/files/JMPreport2012.pdf. Accessed 14 Mar 2016.
Water and Sanitation Program. 2011. Flagship report: Economic impacts of inadequate sanitation in India. New Delhi: Water and Sanitation Program.
World Bank. 2011b. Social protection for a changing India: Volume 2. Washington, DC: International Bank for Reconstruction and Development. http://www-wds.worldbank.org/external/default/WDSContentServer/WDSP/IB/2011/04/20/000333037_20110420235739/Rendered/PDF/612750v20ESW0P11SP0Report0Volume0II.pdf. Accessed Mar 2016.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Copyright information
© 2017 United Nations Research Institute for Social Development
About this chapter
Cite this chapter
Mehrotra, S., Kumra, N., Gandhi, A. (2017). The Fragmented Social Protection System in India: Five Key Rights but Two Missing. In: Yi, I. (eds) Towards Universal Health Care in Emerging Economies. Social Policy in a Development Context. Palgrave Macmillan, London. https://doi.org/10.1057/978-1-137-53377-7_11
Download citation
DOI: https://doi.org/10.1057/978-1-137-53377-7_11
Published:
Publisher Name: Palgrave Macmillan, London
Print ISBN: 978-1-137-53376-0
Online ISBN: 978-1-137-53377-7
eBook Packages: Economics and FinanceEconomics and Finance (R0)