
Abstract
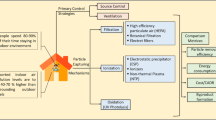
Indoor Air Quality (IAQ) is now well recognized as impacting employee work efficiency. Poor indoor air quality can lead to productivity problems and absence from work. To examine IAQ conditions inside offices in an academic institute, IIT Kanpur, real-time monitoring of particulate matter (PM) was conducted during office hours (10 am to 5 pm). Particulate levels inside five offices on different floors of a multi-storeyed building were monitored over three consecutive days. All offices are on the same side of the building and have 3–6 permanent staff each. Office occupants were given a questionnaire survey to obtain feedback on health-related discomfort indoors (sleepiness, headache, and eye irritation). Only one location (Office A on the first floor) marginally met the current WHO guidelines for PM10 (45 μg/m3), and all others far exceeded it. At least one-fifth of the staff in the four offices that do not meet the WHO guidelines complained about health-related discomfort. Mass (due to PM10) retained in the trachea-bronchi (TB) of the lungs of office (these four) occupants (using the Multiple-Path Particle Dosimetry (MPPD) model) was 50% (average) higher than that in the case of staff in office A. The office with the highest number of printing appliances shows the highest concentration of fine-particulate matter (PM1) and confirms the influence of indoor sources on IAQ. Air purifiers are low-cost interventions that can improve IAQ. Achieving the WHO guidelines inside offices will reduce particle mass retained on the TB up to a staggering 56%. Meeting guidelines may increase the efficiency of workers in these offices by 12–45%.
Shubham Rathi—Presenting author
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others
Keywords
1 Introduction
Years of research have shed significant light on the relationship between indoor air quality (IAQ) and ventilation in offices worldwide. The link of good IAQ to occupant productivity, health, and well-being is now well-accepted [2, 5, 11]. Offices with poor indoor air quality have been linked to sick building syndrome symptoms (SBS). In such cases, employee discomfort, dissatisfaction with the perceived air quality, and reduced performance [1, 10, 12] have been recorded. Most studies have examined the IAQ inside schools, and information about the situation inside offices in academic institutions in India is limited. This preliminary study was conducted on the academic campus of IIT Kanpur in India to gain knowledge of particle distribution indoors and estimate health benefits by meeting the required guidelines. Indoor locations frequented by staff and students were selected. This study’s findings will be expanded to implement suggested interventions at identified indoor hotspots, which will be followed by monitoring the effectiveness of mitigation measures.
2 Methodology
The six-story Faculty Building (FB), which has the maximum number of offices inside the academic area of the IIT Kanpur campus, was selected for our study. In April 2019, a questionnaire survey in offices and real-time air quality monitoring was conducted. Data collected on particulate matter levels indoors was analyzed for particle deposition fraction inside the lungs using the MPPD model. This section provides information with the details, data analysis, and modelling parameters.
2.1 Sampling Site Description
In the current study, five offices in the FB spread across four floors represent today’s common office types and have been numbered alphabetically (Office A on the 1st Floor to Office E on the 6th floor). Office types vary from small (faculty offices) to large (departmental and Sectional offices). All the selected offices are located on the same side of FB and were selected based on occupant agreement for the study. Permanent occupancy and floor area are also listed in Table 1. Sampling details are noted in the next section.
The movement of people inside departmental offices, mainly students, faculty, and staff, is continuous throughout the sampling period and varies over 40–60 people per day apart from permanent staff. The only faculty room in this study, Office C, with the least floor area, had minimal visitors during the sampling period (around 5–10 people). Commercial printers and photocopiers were placed inside all the offices and were used regularly except Office C, which had a small personal printer. Windows were closed in all offices during the sampling period. However, departmental offices had a higher frequency of opening and closing doors.
2.1.1 Instrumentation for Measurement of Indoor Air Quality Parameters
Real-time measurements of size-segregated particle mass concentration (PM10, PM3, and PM1) in the selected offices using an Optical Particle Sizer (OPS, Maker: TSI, Model: 3330). The sampling inside offices was done in April 2019 for 7 h (10 am to 5 pm) over three days in each case.
2.2 Questionnaire Survey to Assess Occupants’ Perception of Their Environment
The questionnaire survey (QS) is an effective and efficient method of learning how the occupants perceive indoor conditions, including thermal comfort and IAQ [6, 11]. The QS focused on how people experienced offices and asked about symptoms people generally experience inside a “sick building” (headaches, eye irritation and sneezing) [8]. The QS was distributed to employees and visitors during the study period.
2.3 MPPD Modelling for Particle Deposition in TB Region of Lungs
The Eulerian Multiple Path Particle Dosimetry or MPPD model (version 3.04) was used to calculate the percent change in the mass of coarse particulates deposited in the human respiratory system’s Trachea Bronchi (TB). The Chemical Industry Institute of Toxicology and the Dutch National Institute for Public Health and the Environment developed this model.
We adopted the human age-specific symmetric lung model to calculate particle deposition in the TB region. The exposure scenario for an employee sitting in an office for 7 h (10 am to 5 pm) for one day was considered. The model was applied to respirable particulates with a density of 1.4 g/cm3, and a geometric standard deviation (GSD) of 3.00 was assumed. The default parameters selected for the model of an adult at rest [i.e., upright body orientation, respiratory frequency of 12 breaths min−1, functional reserve capacity (FRC) of 3300 mL, upper respiratory tract (URT) volume of 50 mL at a fixed tidal volume of 625 mL, the inspiratory fraction of 0.5, and nasal route breathing].
3 Results and Discussion
3.1 Trends in Particle Mass Distribution Inside Offices (PM10, PM3, and PM1)
Table 2 displays the typical particle mass concentration inside each office. The average concentration for PM10, PM3 and PM1 particles exhibits the following trend:
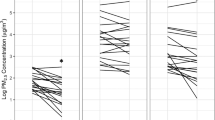
PM10 concentration only in Office A was within the acceptable range. It was below (marginally) the (World Health Organisation) WHO-recommended indoor limit of 45 μg/m3. Office D, where the PM levels were twice as high as Office A, had the highest PM10 concentration. For the two locations on the same floor (third), the smaller faculty office with the least number of visitors, Office C, had average PM10 levels higher than those in Office B, the departmntal office. However, in Office B, a higher peak concentration was seen. In Offices B and C, the observations for PM3 and PM1 were similar. The lowest average fine particle PM1 levels were in Departmental Office D on the fourth floor, with the fewest permanent employees. This office also had the highest levels of respirable and coarser particles.
Dominant particle size bin. Particles in size bin 5.5–7 μm contribute more inside Offices A, C, and D, while the next size bin, 7–10 μm, is dominant inside Offices B and E.
The lower particle ratios of PM3/PM10 and PM1/PM10 in offices on upper floors D and E, relative to other offices, are likely due to this trend in coarser particle levels. These ratios indicate that the mass concentration in all the offices was significantly influenced (66–73%) by the quasi-coarser particles (PM3−10) [9]. In all the offices, the contributions to PM10 by respirable (PM3) was <15% (range: 2.5–15%), and by fine (PM1) particle, it was <35% (26–34%).
Influence of occupant activity on particle levels. Other than fines, the concentration of particles is susceptible to resuspension by occupant movement or activity, leading to peaks in particle levels. In contrast, the occupants’ activity does not impact the concentration of submicron particles. These particles enter the building from the outside or are released from office equipment.
Our findings are consistent with the study, which found that the submicron particle (PM1) is less likely than PM1-3 and PM3-10 to be resuspended by occupant activity [7]. The authors looked at how the walking patterns of staff affected the resuspension of particulate matter (0.5–5 μm) inside an experiment chamber. Compared to particles with a diameter larger than one μm, the resuspension of particles in the size range of 0.5–1.0 μm was minimal [7].
3.2 Deposition of Coarse Particles in Lungs (TB) Attributable to Particle Exposure Inside Offices
Table 3 shows the particle mass (mg) retained in employees’ lungs due to exposure to PM10. The mass retained correlated with PM10 values and was highest for Office D and least for Office A. The four offices (B–E) that do not meet WHO guidelines have an average of 50% more particle deposition in lungs (TB) compared to office A, which marginally met the guidelines. The level of coarse particle mass in the lungs directly correlates with cases of headache reported in the questionnaire response by office occupants. It was the least for Office B, one in five employees (20%) to the maximum in Office D, three in four employees (75%).
3.3 Meeting WHO Guidelines, Change in Coarse Particle Deposition in Lungs (TB), and Employees’ Efficiency
Table 4 shows that if indoor air quality is maintained at WHO guidelines levels, then coarse particle mass (PM10) retained on the TB region of the lungs could be reduced by a staggering 56% (Office D) to 18% (Office B). Researchers have examined the influence of improved indoor air quality and suggest that healthy air quality directly contributes to staff performance. In this study, removing headache issues experienced by employees within the offices will improve work productivity. The employee working in a better (headache-free) environment can perform around 60% better in cognitive tasks [4], which may improve the efficiency of the offices by 12% (Office B) to 45% (Office D).
We suggest using simple air purifiers to reduce air pollution and maintain the WHO guideline levels indoors. Air purifier costs average around 6000–14,500 INR in the local market [3].
4 Conclusions
Particle levels inside most offices in this study are higher than indoor guidelines set by WHO. The departmental offices observed frequent quasi-RSPM (Respirable Suspended Particulate Matter) and coarser PM peaks. Personnel movement indoors is the likely cause which does not seem to affect fine particle concentration, which remained almost steady. Particle deposition inside the lungs can be drastically reduced by meeting the IAQ guidelines marginally. Using air filters is low-cost and a viable intervention that can be implemented quickly. Spending little money (air filters) on improving the office’s indoor air quality can drastically improve work efficiency. Furthermore, It is crucial to assess the ventilation condition inside offices on campus to understand better factors impacting IAQ.
During the QS, it was noted that few respondents were familiar with IAQ concepts or were aware of Sick Building Syndrome, which was a significant finding. IAQ significantly negatively impacts people’s health and productivity at work. Efforts should be made to inform and raise public awareness of the causes and dangers of SBS and poor air quality.
References
al Horr Y, Arif M, Katafygiotou M, Mazroei A, Kaushik A, Elsarrag E (2016) Impact of indoor environmental quality on occupant well-being and comfort: a review of the literature. Int J Sustain Built Environ 5(1):1–11. https://doi.org/10.1016/J.IJSBE.2016.03.006
Allen JG, MacNaughton P, Laurent JGC, Flanigan SS, Eitland ES, Spengler JD (2015) Green buildings and health. Curr Environ Health Rep 2(3):250–258. https://doi.org/10.1007/S40572-015-0063-Y/FIGURES/1
Amazon.in: air purifier (2023) Amazon Website. https://www.amazon.in/s?k=air+purifier&crid=1YZF7BOL1LA41&sprefix=air+purifie%2Caps%2C238&ref=nb_sb_noss_2
Camfil Website (2023) How to improve indoor air quality and productivity|Camfil. Cafil Website. https://www.camfil.com/en-in/insights/air-quality/how-to-improve-indoor-air-quality-and-productivity
Chan WR, Parthasarathy S, Fisk WJ, Mckone TE (2016) Estimated effect of ventilation and filtration on chronic health risks in U.S. offices, schools, and retail stores. Indoor Air 26(2):331–343. https://doi.org/10.1111/INA.12189
Jafari MJ, Khajevandi AA, Najarkola SAM, Yekaninejad MS, Pourhoseingholi MA, Omidi L, Kalantary S (2015) Association of sick building syndrome with indoor air parameters. Tanaffos 14(1):55. /pmc/articles/PMC4515331/
Lv Y, Wang H, Zhou Y, Yoshino H, Yonekura H, Takaki R, Kurihara G (2019) The influence of ventilation mode and personnel walking behavior on distribution characteristics of indoor particles. Build Environ 149:582–591. https://doi.org/10.1016/J.BUILDENV.2018.12.057
Mølhave L (2019) Sick building syndrome. Encycl Environ Health, 663–669. https://doi.org/10.1016/B978-0-444-63951-6.00271-0
Rohra H, Tiwari R, Khare P, Taneja A (2018) Indoor-outdoor association of particulate matter and bounded elemental composition within coarse, quasi-accumulation and quasi-ultrafine ranges in residential areas of northern India. Sci Total Environ 631–632:1383–1397. https://doi.org/10.1016/J.SCITOTENV.2018.03.095
Wargocki P, Wyon DP (2017) Ten questions concerning thermal and indoor air quality effects on the performance of office work and schoolwork. Build Environ 112:359–366. https://doi.org/10.1016/J.BUILDENV.2016.11.020
Wargocki P, Wyon DP, Sundell J, Clausen G, Fanger PO (2000) The effects of outdoor air supply rate in an office on perceived air quality, sick building syndrome (SBS) symptoms and productivity. Indoor Air 10(4):222–236. https://doi.org/10.1034/J.1600-0668.2000.010004222.X
Weng J, Zhang Y, Chen Z, Ying X, Zhu W, Sun Y (2022) Field measurements and analysis of indoor environment, occupant satisfaction, and sick building syndrome in university buildings in hot summer and cold winter regions in China. Int J Environ Res Pub Health 20:554. https://doi.org/10.3390/IJERPH20010554
Acknowledgements
The authors appreciate the office staff’s cooperation, assistance in answering the questionnaire survey, and patience during sampling. We also want to thank Mr Krishnkant Gupta (SURGE-2019, IITK) for his help gathering real-time data.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2024 The Author(s), under exclusive license to Springer Nature Singapore Pte Ltd.
About this paper

Cite this paper
Rathi, S., Goel, A., Ola, D. (2024). Low-Cost Interventions that Reduce Particle Levels Indoors Are Viable Options to Enhance the Operating Efficiency of Occupants. In: Kulshreshtha, P., Chinthala, S., Kumar, P., Aggarwal, B. (eds) Indoor Environmental Quality. ACIEQ 2022 2023. Lecture Notes in Civil Engineering, vol 380. Springer, Singapore. https://doi.org/10.1007/978-981-99-4681-5_10
Download citation
DOI: https://doi.org/10.1007/978-981-99-4681-5_10
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-99-4680-8
Online ISBN: 978-981-99-4681-5
eBook Packages: EngineeringEngineering (R0)