
Abstract
Hereditary gynecological malignancy constitutes a group of women’s cancer syndromes caused by constitutional genetic variants, which carry inherited susceptibility to certain pelvic epithelial malignancies, such as endometrial and ovarian cancers, including primary peritoneum and fallopian tube cancers of synchronous or metachronous onset. The most common inherited gynecological malignancy is Hereditary Breast and Ovarian Cancer syndrome (HBOC), which carries increased lifetime risks of breast and ovarian cancers, including other types of malignancies, such as pancreas, male breast, and prostate cancers. The next leading cause of inherited gynecological malignancy is Lynch syndrome (LS), a hereditary cancer syndrome predisposing individuals to various organ malignancies, including gynecological (endometrium is the most common) and non-gynecological (colonic or extracolonic) cancers, including stomach, urinary tract, brain, small intestine, hepatobiliary, and pancreatic cancers, which harbor impaired DNA mismatch repair due to germline disorders of MLH1, MSH2, MSH6, or PMS2, or the deletion of EPCAM, a gene epithelial cell adhesion molecule. HBOC and LS have communal aspects, which provide effective information for the treatment of symptomatic patients (probands), as well as for at-risk family members or relatives in surveillance and the prevention of malignancies. Cowden syndrome (CS) and Peutz–Jeghers syndrome (PJS), which are inherited hamartoma tumors, or polyposis syndrome are also associated with gynecological malignancies. As CS and PJS are much rarer and have lower malignancy risks, HBOC and LS are discussed as representatives of the hereditary gynecological cancer predisposition syndromes in this chapter.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Hereditary Breast and Ovarian Cancer syndrome (HBOC)
- BRCA1
- BRCA2
- Lynch syndrome (LS)
- DNA mismatch repair (MMR)
- Germline
- Cancer susceptibility
12.1 Epidemiology and Risks of Hereditary Susceptibility to Ovarian Cancers; Hereditary Breast and Ovarian Cancer Syndrome (HBOC)
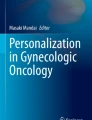
It is conventionally known that ovarian cancer is associated with inherited factors [1, 2]. The strongest risk factor for ovarian cancer is a family history of breast or ovarian cancer, and a quarter of all ovarian cancers are caused by heritable conditions [3]. BRCA1/2 germline pathogenic variants are representative of these heritable factors, leading to an increased lifetime risk of ovarian cancer ranging from 39 to 63% with BRCA1 variants and 16.5–27% with BRCA2 variants, both of which are significantly higher risks of ovarian cancer than that in the general population. The accumulated risk of breast cancer is 38% or more, which is estimated to be over 80% by 70 years of age [4,5,6,7,8] (Table 12.1). The overall prevalence of BRCA1/2 variants is estimated to be 1 out of 400–800, which varies depending on ethnicity; a higher prevalence of 1 in 40 is observed in the Ashkenazi Jewish [7]. A multicentric cohort study showed that the cumulative ovarian cancer risk by 80 years was 44% for BRCA1 and 17% for BRCA2 variant carriers, of which the corresponding relative risks are 35–40 times that of women in the general population [9] (Fig. 12.1). Hirasawa et al. demonstrated that BRCA1/2 is the most frequent germline pathogenic variant in Japanese ovarian cancer patients, with prevalence rates of 8.3% for BRCA1 and 3.5% for BRCA2 [10]. A multicenter study also showed that the overall prevalence of germline BRCA1/2 variants was almost 15%, with germline BRCA1 variants (9.9%) and BRCA2 variants (4.7%) in ovarian cancer patients in Japan [11].

Estimated cumulative risk of breast cancer (left panel) and ovarian cancer (right panel) among BRCA1 and BRCA2 variant carriers. Adapted from Kuchenbaecker et al., JAMA. 2017; 317(23):2402–2416. doi: 10.1001/jama.2017.7112 © 2017, American Medical Association
12.2 Epidemiology and Risks for Hereditary Susceptibility to Endometrial Cancer; Lynch Syndrome (LS)
Lynch syndrome (LS), alternatively termed as hereditary nonpolyposis colorectal cancer (HNPCC), is an autosomal dominant inherited multiple organ malignancy due to a germline variant in one of four DNA mismatch repair (MMR) genes, MSH2, MLH1, MSH6, or PMS2, or the deletion of EPCAM. The estimated prevalence in the population ranges from 1 in 250 to 1 in 3000, depending on the country and ethnicity, or whether the individual carries founder variants or not [13]. Colorectal carcinoma is generally the most common, followed by endometrial carcinoma in women with LS. Three percent of all new cases of colorectal cancer are attributable to LS in the USA [14]. According to various studies, women with LS are estimated to carry higher risks of endometrial cancer than colorectal cancer [15,16,17]. Two to four percent of endometrial cancer before 70 years, and nearly 5% of endometrial cancer onset between 20 and 54 years old, is estimated to be attributed to LS or to those with LS-associated family history [18,19,20]. Loss of function of any of the MMR genes is associated with microsatellite instability, a type of genomic instability, and increased risk of LS-associated cancers. The lifetime risk of endometrial cancer in women with LS is 25–60%, which is comparable to the lifetime risk of colorectal cancer in women with LS [16, 21]. The accumulated penetrance rate of ovarian cancer during the lifetime of women with LS is 6–13%, which is significantly higher than the 1–2% risk of ovarian cancer in the general population [22, 23]. The estimated lifetime endometrial cancer risks in women with LS are dependent on the causative genes. For women with MLH1 or MSH2 variants, the lifetime risk of endometrial cancer is reportedly 34–54% with MLH1 variants and 21–57% with MSH2 variants. The lifetime risks for ovarian cancer are 4–20% with MLH1 variants and 8–38% with MSH2 variants [24,25,26].
According to the International Society for Gastrointestinal Hereditary Tumors (InSiGHT) database, which records variants identified in over 3000 of LS cases, MLH1 and MSH2 are dominantly responsible genes for LS, while the remainder, such as MSH6 and PMS2, are less frequently identified in LS. The proportions of LS attributed to pathogenic variants are 42% in MLH1 and 33% in MSH2, while the smaller population is attributed to MSH6 (18%) and PMS2 (7.5%) [27]. EPCAM deletion is observed in 1–3% of the population with LS [28, 29]. Although MSH6 variants are less commonly observed in LS than MLH1 or MSH2 variants, MSH6 is a dominant causative variant gene in LS-associated endometrial cancer and in an older age onset of LS-associated colorectal cancer [17]. The cumulative risk for endometrial cancer by 80 years in women with MSH6 variants ranges from 17 to 44% [17, 30], while the risks for endometrial carcinoma carrying PMS2 variants or EPCAM deletions are reported to be less than 15 or 12%, respectively [31, 32].
The age of cancer onset in the population with LS is younger than that of the general population; the mean age at the time of diagnosis of endometrial cancer is 48–62 years and the average age for ovarian cancer is 42.5 years in women with LS [8].
According to a cohort study by Win et al., women with a diagnosis of endometrial cancer carrying an MMR variant had significantly higher risks in other cancers, such as colorectal cancer, breast cancer, or urological cancers, such as the ureter, urinary bladder, kidney, and renal pelvis cancers, during the 20-year follow-up visits of endometrial cancer patients [33, 34]. Based on this evidence, endometrial cancer can be termed a “sentinel cancer,” a preceding cancer which is first detected among a series of primary cancers developed in women with LS.
12.3 Molecular Features and Diagnosis of BRCA-Associated Hereditary Gynecologic Malignancy
The germline pathogenic variants of BRCA1/2 account for the majority of hereditary breast and ovarian cancers showing an autosomal dominant predisposition to those diseases [7]. Both BRCA1 and BRCA2 were identified by positional cloning in the early 1990s as genes responsible for susceptibility to breast and ovarian cancers [35, 36]. The locus of BRCA1, which encodes a predicted protein consisting of 1863 amino acids, is at 17q21.31 in the long arm of chromosome 17 (OMIN#113705). BRCA1 is expressed in numerous tissues, including the testis, thymus, breast, and ovary [35]. BRCA2 is located at 13q13.1 in the long arm of chromosome 13 (OMIN#600185) and encodes 3418 amino acids [36]. Although there is no structural homology in BRCA1 and BRCA2, these two genes share communal functions as caretakers in the maintenance of genomic integrity and homologous recombination (HR) during DNA damage repair of double-strand breaks [37]. The loss of function of either BRCA1 or BRCA2 causes serious disruption in the open reading frame of the transcription unit. BRCA1 protein functions by interacting with several proteins. BRCA1-associated RING domain 1 (BARD1) binds to the RING-finger domain near the N-terminus of BRCA1, both of which carry nuclear exporting signal (NES). BRCA1 creates three different types of complexes exclusively with phosphorylated Abraxas (ABRA1), BRCA1-associated C-terminal helicase (BACH1), or CtBP-interacting protein (CtIP) through the BRCT domain near the C-terminus of BRCA1 [38, 39]. As a consequence of interacting with these different proteins, BRCA1 plays distinct roles in DNA damage resistance, ubiquitination, gene transcription, and cell cycle progression, such as G(2)-M checkpoint control [40]. BRCA2 plays a role in genomic integrity maintenance through the DNA repair process and facilitates HR. BRCA2 protein functions to prevent nascent DNA degradation and promote HR-mediated prevention in replication fork stalling by loading RAD51 on DNA breaks and gaps [41, 42]. BRCA2 can form a complex with BRCA1 through PALB2 mediation (Fig. 12.2).

Structures and Functions of BRCA1 and BRCA2 on DNA double-strand breaks. BRCA1 (1863a.a.) contains several recognizable protein motifs, such as a RING-finger domain near the N-terminus for binding with BRAD1 to function as a nuclear exporting signal (NES), coiled-coil domain on exon 11 for interaction with PALB2, and a BRCT domain at the C-terminus. BRCA2 (3418a.a.) contains eight BRC repeats of 30–40 residue motifs found in exon 11, which mediate the binding of BRCA2 to RAD51. RAD51 functions in homologous recombination through interstrand cross-links. Referenced from Sedukhina A et al. Seikagaku 84(7), 529–538, 2012. ©2012, The Japanese Biochemical Society
More than 1600 or 1800 variants have been identified in BRCA1 and BRCA2, which leads to loss of function due to frameshift deletions, insertions, or premature truncation of transcripts, suggesting the significant functions of BRCA1 and BRCA2 as tumor suppressor genes [7, 43, 44]. The loss of function of BRCA1 or BRCA2 increases the sensitivity to poly(ADP-ribose) polymerase (PARP), which is referred to as synthetic lethality, resulting in vulnerability to PARP inhibitors [45, 46]. The locus of variants in BRCA1 and BRCA2 is also known to affect cancer risk. In the analyses of over 400 families carrying a BRCA2 variant with the presence of ovarian cancer and other malignancies, families with ovarian carcinoma or breast cancer were more likely to harbor variants in the ovarian cancer cluster region of exon 11 of BRCA2 than families with variants elsewhere in BRCA2 [47].
12.4 Genetic Testing of BRCA1/2
Genetic testing using blood samples is applicable for clinical diagnosis not only for symptomatic patients (probands) with breast and/or ovarian cancers but also for at-risk relatives as predisposition testing. Distinct testing strategies, for example, targeting analyses, comprehensive analyses, or large genomic rearrangement tests, are provided by Myriad Genetic Laboratories (Salt Lake City, UT, USA). Target analyses may be used for the detection of population-specific founder variants, such as BRCA1 c.68_69delAG (185delAG), BRCA1 c.5266dupC (5382insC), or BRCA2 c.5946delT (6174delT), which are detected at frequencies as high as 1 in 40 individuals of Ashkenazi Jewish heritage [48]. Comprehensive analysis is useful for the evaluation of the predisposition of at-risk individuals through combined methods to detect common BRCA1/2 variants and five specific large genomic rearrangements in BRCA1, which are ethnic-specific or family-specific variants. Further complementary analysis is conducted as a large rearrangement test of the above and beyond the common five rearrangements of BRCA1, such as large genomic rearrangements in BRCA1/2 [7] (Table 12.2).
Clinical BRCA1/2 testing in Japan is covered by the social insurance service as companion diagnostics to determine the indication of PARP inhibitors, as well as for the diagnosis of HBOC only for symptomatic patients (probands) with breast and/or ovarian cancers so far in 2020. Other comprehensive or specific germline cancer panels/analyses including BRCA1/2 are provided by several diagnostic companies, such as LabCorp (Burlington, NC, USA), Ambry Genetics Corporation (Aliso Viejo, CA, USA), and ACT Genomics (Taipei City, Taiwan). These may be used for the investigation of other related disorders of probands as well as for at-risk relatives and for differential diagnosis.
The analysis of genetic testing is reported in three variant categories: a positive, a negative, or an inconclusive, termed as a variant of uncertain significance (VUS), in clinical pathogenicity. It is estimated that up to 20% of BRCA1/2 variants are reported as a VUS [49,50,51,52]. In the large rearrangement tests and the family-specific variant tests for at-risk relatives, the testing results will be shown in one of two categories: absent (negative) or present (positive). Even if negative results are obtained, careful interpretation is indispensable because negative results do not necessarily eliminate the possibility of a hereditary susceptibility to cancer. There is also a possibility that cancer in the family might be associated with unknown hereditary factors that are undetectable by the genetic test performed. When VUS results are obtained, further analysis using samples from additional family members might be a clue to examine whether the variants co-segregate with cancer in the family [7].
12.5 Relationships Between BRCA1/2 Variants and Histological Properties of Hereditary Gynecological Malignancies
The prevalence of germline BRCA1/2 variants is known to be associated with frequencies of specific types of histology [11]. The most common histology type of ovarian cancer carrying BRCA variants is high-grade serous carcinoma, comprising about 70–80% of women with BRCA1/2 variants, while it is approximately 50% in sporadic controls or women without BRCA1/2 variants [53,54,55,56,57,58]. Endometrioid and mucinous carcinomas of the ovary account for a smaller population, which is a maximum of 6–12% among women carrying BRCA1/2 variants. In contrast, approximately 10–20% of people in the general population with wild-type germline BRCA present with these carcinomas. It is estimated that approximately 10–15% of women with pelvic serous carcinoma have pathogenic germline BRCA variants.
Serous carcinoma of pelvic malignancies is generally high-grade, a clinically aggressive type, and characterized as a type II tumor, which is frequently bilateral and is often found on the peritoneal surfaces at diagnosis [7, 59]. In BRCA-associated ovarian cancers, distinct molecular pathways of carcinogenesis, which are different from sporadic ovarian cancers, are associated with unique histopathologic subtypes [60]. According to the accumulated evidence through careful histopathologic analyses, such as of the resected fallopian tubes at the risk-reduction salpingo-oophorectomy from patients carrying BRCA germline variants, a hypothesis was established that the distal fimbria end may be a potential site for early-stage tubal carcinoma leading to advanced tumorigenesis of pelvic malignancies, including primary peritoneal carcinoma [61,62,63,64,65]. Many studies have clarified that noninvasive carcinoma arising in the fallopian tube is potentially able to metastasize without invading into the substantial stroma of the distal salpinx, and this character is analogous to superficial serous carcinoma of the endometrium [66]. Such early stages of serous carcinoma, termed as serous tubal intraepithelial carcinomas (STICs) in fimbria, are observed with ovarian carcinoma in over 70% of sporadic ovarian and peritoneal malignancies of high-grade serous carcinoma [67]. Therefore, it is hypothesized that STICs, which are detected in fimbria, would be a source of high-grade serous carcinoma in pelvic malignancies, regardless of the status of germline BRCA1/2.
Occult malignancy, a small in situ carcinoma, was originally described by Colgan et al. in the study of salpingo-oophorectomy specimens at a prevalence rate of 8.3% in 5 of 60 high-risk women carrying BRCA1/2 variants [61]. The incidence rate of occult carcinoma varies to some extent in study groups. Leeper et al., for example, reported that the occult carcinoma is observed in 17% (5 patients of 30) of BRCA1/2-variant positive women [68]. Paley et al. studied two BRCA1-positive patients with occult carcinoma in fallopian tubes and with positive peritoneal cytological malignancy, suggesting the micro-implantation potential of malignant cells in the peritoneum [69]. Another study by Agoff et al. showed that two of four cases of early fallopian tube carcinoma were positive for peritoneal cytology [70]. This leads to the central hypothesis that the inherited BRCA status is included as part of the cancer spectrum associated with STICs, which develops into fallopian tube carcinoma with a high potential to metastasize [66]. Depending on the location and the speed of tumor growth, the tumor might be mistakenly presumed as primary carcinomas of the ovary, peritoneum, or fallopian tube [60]. These are significant research outcomes by analyzing salpingo-oophorectomy specimens from pathogenic BRCA1/2 variant-positive women. These findings are also supported by the finding that almost all STICs showed positive staining for p53, which is similar to that of high-grade serous carcinoma. Small linear p53-positive foci, termed the p53 signature, are commonly detected in the distal fimbria of both BRCA-variant positive women and sporadic groups with early tubal cancer [71]. Another study analyzing 29 cases of pelvic serous carcinoma showed that STICs and concordant high-grade serous carcinoma were identical to the TP53 variant of ovarian carcinoma, which supports a clonal relationship between STICs and TP53 [72]. Although these data are not necessarily relevant to the germline status of BRCA1/2, this suggests that the p53 signature would be an early precursor of high-grade serous carcinoma [66]. The accumulated evidence obtained from analyses of fallopian tubes from BRCA-variant-positive women has strengthened the fact that the fimbria end may be an origin of pelvic malignancies. What is more obvious from this evidence is that BRCA variants are susceptible factors for a subset of serous carcinomas, which has a strong connection with the distal end of the fallopian tube.
12.6 Molecular Features and Diagnosis of Gynecological Malignancies with LS
Microsatellite instability (MSI) and DNA mismatch repair deficiency (MMR-D) are basic tools for screening LS. Latham et al reported that LS was identified in 16.3% of patients with MSI-high (MSI-H). Immunohistochemical staining of LS-positive MSI-H, including MSI-intermediate (MSH-I) tumors, demonstrated MMR-D in 98% of patients [74]. MSI-H status is generally concordant with a high tumor mutational burden (high TMB), but the converse is not always true. According to the study by Chalmers et al., 16% of high TMB (> 20 mutations/Mb) was classified as MSI-H, of which concordance is dependent on malignancy type [73]. High TMB and MSI-H are rarely detected in lung and skin carcinomas, while those two statuses are matched frequently in cases of gynecological malignancies, such as endometrial carcinoma including endometrioid carcinoma of the uterus [73] (Fig. 12.3).

The relationship between tumor mutation burden (TMB) and microsatellite instability (MSI). A majority (83%) of MSI-high (MSI-H) samples also had high TMB (TMB-H), while a smaller population (16%) in TMB-H was classified as MSI-H (panel a). Co-occurrence of MSI-H and TMB-H was observed at high incidence in gynecological malignancies, such as endometrial carcinoma of the uterus (panel b, asterisks). Adapted from Chalmers et al., Genome Medicine (2017) 9:34. doi: 10.1186/s13073-017-0424-2 © Zachary R. Chalmers et al.
The initial step of clinical screening for gynecological malignancies with LS is the selection of patients and families based on the revised Amsterdam criteria II, a clinical diagnostic criterion of hereditary nonpolyposis colorectal cancer (HNPCC)-associated malignancies, covering colorectal, endometrial, renal pelvic, ureteral, and small intestinal cancers [12] (Table 12.3). Endometrial and ovarian cancers are also listed as LS-associated tumors in the revised Bethesda Guidelines, which is a clinical screening criterion for individuals with HNPCC who should be tested for microsatellite instability (MSI) [75]. MSI is caused by mismatch repair deficiency and is characterized by insertion/deletion or alteration in the lengths of repetitive regions within DNA. Polymerase chain reaction (PCR)-based MSI screening is widely conducted using the Bethesda panel, a five-marker panel comprising two mononucleotide repeats, BAT25, BAT26, and three dinucleotide repeats of D2S123, D5S346, and D17S250, of which application is recommended by the National Cancer Institute, USA [76, 77]. If two or more of five markers show instability, for example, variable shifting in the wave patterns in capillary electrophoresis of fluorescent-adjunct and amplified fragments from tumor and unaffected tissue, those MSI statuses are called high-frequency MSI (MSI-H). In contrast, if a single or no marker out of five shows instability, it is termed as low-frequency MSI (MSI-L) or microsatellite status stable (MSS) [76]. In recent years, PCR-based methods using five mononucleotide markers (BAT25, BAT26, MONO27, NR21, and NR24, instead of the Bethesda panel) as well as next-generation sequencing (NGS) techniques have been developed to detect MSI status with high sensitivity and specificity. Quasi-monomorphic variation range (QMVR), in which PCR products from normal DNA are almost confined regardless of ethnicity, is applied to MSI testing using five mononucleotide markers. MSI status can therefore be determined using the mononucleotide marker panel without normal DNA analysis [78]. In the NGS technique by FoundationOne® CDx (Foundation Medicine, Inc., Cambridge, MA, USA), a tumor sequencing used in cancer precision medicine, the MSI status is designated based on the genome-wide analysis of 95 microsatellite loci. Approximately 90% of LS-associated endometrial cancers are estimated to show MSI-H [79], while nearly 30% of sporadic endometrial cancer cases are presumed to show MSI-H [80]. In contrast, in ovarian cancer, the MSI-H population ranges from 3 to 13%, while the prevalence rate of LS in ovarian cancer is estimated to be almost the same or less at 0.9–2.7% [74, 81,82,83].
Immunohistochemical (IHC) analysis of MMR protein expression has been conventionally and universally performed as the second step in the diagnosis of LS. IHC analysis is advantageous in the direct visual detection of altered MMR. MSH2 functions as a heterodimer with MSH6, forming a major MutSα complex or with MSH3 to form a minor MutSβ complex. MLH1 and PMS2 proteins function as stable heterodimers by forming a MutLβ complex that detects the short insertion–deletion loop of the mismatch structure. Loss of expression in both MSH2 and MSH6 is typically caused by germline variants. In contrast, loss of expression in both MLH1 and PMS2 indicates a germline alteration of MLH1 or somatic methylation of MLH1 promoter in sporadic cancers [14, 84]. To rule out sporadic MSI-H carrying epigenetic methylation of MLH1, BRAF V600E testing is applied based on the evidence that BRAF V600E is positive in approximately 40% of sporadic MSI-H colorectal cancers, while it is rarely observed in LS-associated colorectal cancer [85,86,87]. It must be noted that this is the case with colorectal cancer but not with endometrial cancer. The BRAF V600E test is not applicable to endometrial cancer in clinical practice [88, 89]. It should also be noted that the majority of MSI-H in gynecological malignancy is due to hypermethylation of the MLH1 promoter rather than germline variants of MMR genes.
The majority of LS-associated endometrial cancers are endometrioid carcinomas, most of which are found as Grade 1 of the International Federation of Gynecology and Obstetrics (FIGO). Other non-endometrioid carcinomas including clear cell carcinoma, serous carcinoma, and carcinosarcoma, which is known as malignant mixed Mullerian tumor (MMMT), have also been reported [90]. Mesenchymal tumors, such as leiomyomas, leiomyosarcomas, and other stromal tumors, are not associated with LS. The location of endometrial cancer in patients with LS is likely to be in the lower uterine segment (LUS), which is a rare site for sporadic endometrial carcinoma [91, 92].
12.7 Risk Assessment, Surveillance, and Prevention of Hereditary Gynecological Malignancies
While ovarian cancer is a relatively rare type of malignancy, in which the prevalence rate in the general population is as low as 1.3% (1 of 78) according to the statistics in the USA, the lifetime incidence of ovarian cancer increases to 39–58% in women carrying germline pathogenic BRCA variants, and it rises to 9–12% in women with germline MMR pathogenic variants according to a study in the USA [93]. Population-based, single institutional, or nationwide multicentric studies showed that the positive rates for germline BRCA variants are 11–15% in invasive ovarian cancer patients regardless of ethnicity [10, 11, 55, 94]. It is as much as 2% in invasive ovarian cancer cases, which are positive for germline MMR variants [83]. The positive rates may be increased in patients with early onset of ovarian cancer (before 40 years of age) [95]. Due to the genes inherited in an autosomal dominant manner, each child of a person with HBOC or LS carrying germline pathogenic mutations in BRCA1/2 or MMR genes has a 50% chance of having inherited causative variants, irrespective of gender. Appropriate surveillance following proper genetic testing at the right time point is important for the prevention of cancer development associated with inherited cancer syndromes.
12.7.1 Guideline Overview on BRCA1/2-Associated Gynecological Malignancies
Identifying women at high lifetime risk for ovarian cancer, due to germline variants relevant to the inherited syndromes, provide asymptomatic women with prevention opportunities, such as surveillance, chemoprevention, and risk-reducing surgery, by using a systematic tailored screening strategy [96]. Some medical societies recommend germline genetic testing for all women diagnosed with ovarian cancer. According to the American Society of Clinical Oncology (ASCO) Guidelines, published in 2020, it is strongly recommended that all women diagnosed with epithelial ovarian cancer should have germline genetic testing for BRCA1/2 and other ovarian cancer susceptibility genes, irrespective of their clinical features or family cancer history [97]. It is moderately recommended that women diagnosed with clear cell, endometrioid, or mucinous ovarian cancer should undergo somatic tumor testing for mismatch repair deficiency (dMMR) [97]. The National Comprehensive Cancer Network® (NCCN®) (NCCN) regularly updates its clinical practice guidelines in oncology (NCCN Clinical Practical Guidelines in Oncology® (NCCN Guidelines®)) which can link to NCCN.org. According to Version 1.2020 of NCCN Guidelines® for Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic, focusing on BRCA1/2 variant-positive management, clinical breast examination should be performed every 6–12 months, starting at the age of 25 years. Genetic counseling on risk-reducing mastectomy should include a discussion regarding the degree of protection, reconstruction options, and risks [98]. Risk-reducing salpingo-oophorectomy (RRSO) is recommended, which is typically performed between 35 and 40 years of age and upon completion of childbearing [98]. There is also a description regarding the management of RRSO, depending on the variant status of BRCA1/2. For patients with BRCA2 pathogenic/likely pathogenic variants, RRSO can be reasonably delayed until the age of 40–45 years, since the onset of ovarian cancer in patients with BRCA2 pathogenic/likely pathogenic variants is an average of 8–10 years later than in patients with BRCA1 pathogenic/likely pathogenic variants [98]. Salpingectomy alone, which is based on the detection of precursor lesions, including serous tubal intraepithelial carcinomas (STICs) in fimbria, is not standard of care for risk reduction [98]. Clinical trials of interval salpingectomy and delayed oophorectomy are ongoing. As a discretion option, transvaginal ultrasound (TVUS) combined with serum CA125 level may be considered for ovarian cancer screening for patients who have not elected RRSO [98]. In any case, education regarding signs and symptoms of cancers, especially those associated with BRCA pathogenic/likely pathogenic variants, is important for women (ovarian cancer) and men (male breast and prostate cancers) carrying these variants [98]. Symptoms of pelvic or abdominal pain, bloating, and increased abdominal girth are associated with ovarian cancer development. The US Preventive Services Task Force recommends that primary care clinicians assess women with a personal or family history of breast, ovarian, tubal, or peritoneal cancer or who have an ancestry associated with BRCA variants with an appropriate brief familial risk assessment tool [99]. Women with a positive result on the risk assessment tool should receive genetic counseling, and genetic testing at the indicated time points thereafter [99].
12.7.2 Surveillance and Prevention Strategy for LS-Associated Gynecologic Malignancies
A majority (e.g., 67% in Cancer Statistics 2017) of endometrial cancer patients show symptoms, such as vaginal bleeding, and are diagnosed at an early stage with disease confined to the uterus [100, 101]. The NCCN Guidelines® for Genetic/Familial High-Risk Assessment: Colorectal Version1.2020 recommend that women should be educated regarding the importance of prompt reporting and evaluation of any abnormal uterine bleeding or postmenopausal bleeding [26]. Endometrial biopsy is included as an option for the evaluation of these symptoms; a screening via endometrial biopsy every 1–2 years starting at age 30–35 years can be considered [26]. Hysterectomy may be considered as a risk-reducing surgery for endometrial cancer in at-risk women [26]. Schmeler et al. demonstrated that prophylactic hysterectomy with bilateral salpingo-oophorectomy is effective for preventing endometrial and ovarian cancer in women with LS [102]. Consideration and discussion on the risks and benefits of these risk-reduction agents, as well as patient education regarding the early symptoms of endometrial cancer, are important. Genetic counseling, which is a critical component in cancer risk assessment and helping clients make informed decisions, covers those procedures. As for ovarian cancer, there is no effective screening strategy so far. Transvaginal ultrasound for ovarian cancer screening with or without serum CA125 is not a routine recommendation since those modalities have not been shown to be sufficiently sensitive or specific as the screening of ovarian cancer. To conduct the referral to the genetic counseling at the right time point, including genetic testing, information regarding significant family history of the involved disease will be very important, especially for ovarian cancer.
12.8 Cancer Susceptibility Gene to Gynecological Malignancies Is Presumed Through Tumor Genomic Sequencing
Somatic genomic testing using next-generation sequencing (NGS) is becoming a common practice in clinical oncology, such as for the care of patients with advanced or metastatic cancer. The analysis of tumor genomes also has the potential to uncover germline variants as the underlying background information, called germline findings [103]. BRCA1/2 and MMR genes are important presumed germline genes among the minimum 59 listed genes whose disclosure is recommended by the statement of the American College of Medical Genetics and Genomics (ACMG) [104, 105]. The goal of the disclosure of those presumed germline pathogenic variants (PGPVs) is to identify and manage risks for selected highly penetrant genetic disorders that can be prevented and of which morbidity and mortality can be reduced through established interventions after confirmation as pathogenic germline variants (PGVs) [105]. Both BRCA1/2 and MMR are high-actionable cancer susceptibility genes (CSGs), which confer a predisposition to specific tumor types, such as breast, ovarian, or colon cancer. Even though pathogenic CGCs are detected in organs in which elevated risk of cancer is generally not conferred by those genes, the pathogenic variants of BRCA1/2 or MMR genes should be regarded as germline origin [106]. The NCCN Guidelines® for Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic Version 1.2021 introduces that BRCA1/2 germline genetic testing should be considered if a pathogenic or likely pathogenic variant is found through tumor profiling [76, 98]. The homologous recombination deficiency (HRD) status, due to deleterious variants of BRCA1/2, can be used for response prediction to poly(ADP-ribose) polymerase (PARP) inhibitor. Detection of somatic variants and subsequent confirmation as PGVs allows for a higher likelihood of responses to PARP inhibitors, as well as the effective chance of surveillance to prevent ovarian cancer, colon cancer, or other associated cancers in patients and relatives.
12.9 For Understanding of Hereditary Gynecological Malignancies
Web-based resources and links for HBOC with BRCA1 and BRCA2 variants and LS with MMR variants:
-
GeneReviews®: https://www.ncbi.nlm.nih.gov/books/NBK1116/
-
National Comprehensive Cancer Network (NCCN) Guidelines® for Detection, Prevention, & Risk Reduction: https://www.nccn.org
-
American Society of Clinical Oncology Guidelines: https://www.asco.org/research-guidelines
-
European Society of Medical Oncology (ESMO) Clinical Guidelines: Gynaecological Cancers: https://www.esmo.org/guidelines/gynaecological-cancers
-
U.S. Preventive Services Task Force Recommendation Statement: BRCA-Related Cancer: Risk Assessment, Genetic Counseling, and Genetic Testing: https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/brca-related-cancer-risk-assessment-genetic-counseling-and-genetic-testing
Book
-
Hereditary Gynecologic Cancer: Risk, Prevention and Management edited by Karen H. Lu, published in 2012 by Informa Healthcare, UK.
12.10 Conclusion
BRCA1/2-associated ovarian cancer and LS-associated endometrial cancer are representatives of hereditary gynecological malignancies. A better understanding of these symptoms as well as attention to significant family history provides women with opportunities to identify HBOC or LS, leading to the early detection of asymptomatic stages of ovarian cancer and prevention of secondary cancers. Owing to the progress of analytical technologies and risk-reducing modalities, we have unveiled the detailed mechanisms by which ovarian carcinogenesis and development occur. By identifying specific germline variants associated with gynecologic malignancies, unaffected family members, and relatives also have the opportunity to undergo predictive testing and surveillance. Recent advancements in cancer genomic analytical technology using next-generation sequencing are becoming a common modality that provides us with another opportunity to consider pathogenic variants presumed as germline origin, as well as other potential cancer susceptibilities, called germline findings. The utilization of inherited information, which is estimated through somatic genomic testing and germline analysis, is becoming more common and important in the management of gynecological malignancies.
References
Whittemore AS. Characteristics relating to ovarian cancer risk: implications for prevention and detection. Gynecol Oncol. 1994;55(3 Pt 2):S15–9.
Claus EB, Schildkraut JM, Thompson WD, Risch NJ. The genetic attributable risk of breast and ovarian cancer. Cancer. 1996;77(11):2318–24.
Walsh T, Casadei S, Lee MK, Pennil CC, Nord AS, Thornton AM, et al. Mutations in 12 genes for inherited ovarian, fallopian tube, and peritoneal carcinoma identified by massively parallel sequencing. Proc Natl Acad Sci U S A. 2011;108(44):18032–7.
Easton DF, Ford D, Bishop DT. Breast and ovarian cancer incidence in BRCA1-mutation carriers. Breast Cancer Linkage Consortium. Am J Hum Genet. 1995;56(1):265–71.
Antoniou A, Pharoah PD, Narod S, Risch HA, Eyfjord JE, Hopper JL, et al. Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case Series unselected for family history: a combined analysis of 22 studies. Am J Hum Genet. 2003;72(5):1117–30.
Hopper JL, Southey MC, Dite GS, Jolley DJ, Giles GG, McCredie MR, et al. Population-based estimate of the average age-specific cumulative risk of breast cancer for a defined set of protein-truncating mutations in BRCA1 and BRCA2. Australian Breast Cancer Family Study. Cancer Epidemiol Biomarkers Prev. 1999;8(9):741–7.
Petrucelli N, Daly MB, Feldman GL. Hereditary breast and ovarian cancer due to mutations in BRCA1 and BRCA2. Genet Med. 2010;12(5):245–59.
Gene Reviews [Internet]. https://www.ncbi.nlm.nih.gov/books/NBK1247. Accessed 15 Nov 2020.
Kuchenbaecker KB, Hopper JL, Barnes DR, Phillips KA, Mooij TM, Roos-Blom MJ, et al. Risks of breast, ovarian, and contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. JAMA. 2017;317(23):2402–16.
Hirasawa A, Imoto I, Naruto T, Akahane T, Yamagami W, Nomura H, et al. Prevalence of pathogenic germline variants detected by multigene sequencing in unselected Japanese patients with ovarian cancer. Oncotarget. 2017;8(68):112258–67.
Enomoto T, Aoki D, Hattori K, Jinushi M, Kigawa J, Takeshima N, et al. The first Japanese nationwide multicenter study of BRCA mutation testing in ovarian cancer: CHARacterizing the cross-sectionaL approach to Ovarian cancer geneTic TEsting of BRCA (CHARLOTTE). Int J Gynecol Cancer. 2019;29(6):1043–9.
Vasen HF, Watson P, Mecklin JP, Lynch HT. New clinical criteria for hereditary nonpolyposis colorectal cancer (HNPCC, Lynch syndrome) proposed by the International Collaborative group on HNPCC. Gastroenterology. 1999;116(6):1453–6.
Dunlop MG, Farrington SM, Nicholl I, Aaltonen L, Petersen G, Porteous M, et al. Population carrier frequency of hMSH2 and hMLH1 mutations. Br J Cancer. 2000;83(12):1643–5.
Sinicrope FA. Lynch syndrome-associated colorectal cancer. N Engl J Med. 2018;379(8):764–73.
Hampel H, Stephens JA, Pukkala E, Sankila R, Aaltonen LA, Mecklin JP, et al. Cancer risk in hereditary nonpolyposis colorectal cancer syndrome: later age of onset. Gastroenterology. 2005;129(2):415–21.
Aarnio M, Sankila R, Pukkala E, Salovaara R, Aaltonen LA, de la Chapelle A, et al. Cancer risk in mutation carriers of DNA-mismatch-repair genes. Int J Cancer. 1999;81(2):214–8.
Hendriks YM, Wagner A, Morreau H, Menko F, Stormorken A, Quehenberger F, et al. Cancer risk in hereditary nonpolyposis colorectal cancer due to MSH6 mutations: impact on counseling and surveillance. Gastroenterology. 2004;127(1):17–25.
Gruber SB. Thompson WD. A population-based study of endometrial cancer and familial risk in younger women. Cancer and Steroid Hormone Study Group. Cancer Epidemiol Biomarkers Prev. 1996;5(6):411–7.
Hampel H, Frankel W, Panescu J, Lockman J, Sotamaa K, Fix D, et al. Screening for Lynch syndrome (hereditary nonpolyposis colorectal cancer) among endometrial cancer patients. Cancer Res. 2006;66(15):7810–7.
Leenen CH, van Lier MG, van Doorn HC, van Leerdam ME, Kooi SG, de Waard J, et al. Prospective evaluation of molecular screening for Lynch syndrome in patients with endometrial cancer </= 70 years. Gynecol Oncol. 2012;125(2):414–20.
Dunlop MG, Farrington SM, Carothers AD, Wyllie AH, Sharp L, Burn J, et al. Cancer risk associated with germline DNA mismatch repair gene mutations. Hum Mol Genet. 1997;6(1):105–10.
Watson P, Vasen HFA, Mecklin JP, Bernstein I, Aarnio M, Jarvinen HJ, et al. The risk of extra-colonic, extra-endometrial cancer in the Lynch syndrome. Int J Cancer. 2008;123(2):444–9.
Nakamura K, Banno K, Yanokura M, Iida M, Adachi M, Masuda K, et al. Features of ovarian cancer in Lynch syndrome (Review). Mol Clin Oncol. 2014;2(6):909–16.
Bonadona V, Bonaiti B, Olschwang S, Grandjouan S, Huiart L, Longy M, et al. Cancer risks associated with germline mutations in MLH1, MSH2, and MSH6 genes in Lynch syndrome. JAMA. 2011;305(22):2304–10.
Stoffel E, Mukherjee B, Raymond VM, Tayob N, Kastrinos F, Sparr J, et al. Calculation of risk of colorectal and endometrial cancer among patients with Lynch syndrome. Gastroenterology. 2009;137(5):1621–7.
Referenced with permission from the NCCN Guidelines® for Genetic/Familial High-Risk Assessment: Colorectal Version 1.2020 © National Comprehensive Cancer Network, Inc. 2020. All rights reserved. Accessed 2 Aug 2020. Available online at www.NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way.
Plazzer JP, Sijmons RH, Woods MO, Peltomaki P, Thompson B, Den Dunnen JT, et al. The InSiGHT database: utilizing 100 years of insights into Lynch syndrome. Fam Cancer. 2013;12(2):175–80.
Niessen RC, Hofstra RM, Westers H, Ligtenberg MJ, Kooi K, Jager PO, et al. Germline hypermethylation of MLH1 and EPCAM deletions are a frequent cause of Lynch syndrome. Genes Chromosomes Cancer. 2009;48(8):737–44.
Kuiper RP, Vissers LE, Venkatachalam R, Bodmer D, Hoenselaar E, Goossens M, et al. Recurrence and variability of germline EPCAM deletions in Lynch syndrome. Hum Mutat. 2011;32(4):407–14.
Baglietto L, Lindor NM, Dowty JG, White DM, Wagner A, Gomez Garcia EB, et al. Risks of Lynch syndrome cancers for MSH6 mutation carriers. J Natl Cancer Inst. 2010;102(3):193–201.
Senter L, Clendenning M, Sotamaa K, Hampel H, Green J, Potter JD, et al. The clinical phenotype of Lynch syndrome due to germ-line PMS2 mutations. Gastroenterology. 2008;135(2):419–28.
Kempers MJ, Kuiper RP, Ockeloen CW, Chappuis PO, Hutter P, Rahner N, et al. Risk of colorectal and endometrial cancers in EPCAM deletion-positive Lynch syndrome: a cohort study. Lancet Oncol. 2011;12(1):49–55.
Win AK, Lindor NM, Winship I, Tucker KM, Buchanan DD, Young JP, et al. Risks of colorectal and other cancers after endometrial cancer for women with Lynch syndrome. J Natl Cancer Inst. 2013;105(4):274–9.
Win AK, Lindor NM, Jenkins MA. Risk of breast cancer in Lynch syndrome: a systematic review. Breast Cancer Res. 2013;15(2):R27.
Miki Y, Swensen J, Shattuck-Eidens D, Futreal PA, Harshman K, Tavtigian S, et al. A strong candidate for the breast and ovarian cancer susceptibility gene BRCA1. Science. 1994;266(5182):66–71.
Wooster R, Neuhausen SL, Mangion J, Quirk Y, Ford D, Collins N, et al. Localization of a breast cancer susceptibility gene, BRCA2, to chromosome 13q12-13. Science. 1994;265(5181):2088–90.
Zhang H, Tombline G, Weber BL. BRCA1, BRCA2, and DNA damage response: collision or collusion? Cell. 1998;92(4):433–6.
Hashizume R, Fukuda M, Maeda I, Nishikawa H, Oyake D, Yabuki Y, et al. The RING heterodimer BRCA1-BARD1 is a ubiquitin ligase inactivated by a breast cancer-derived mutation. J Biol Chem. 2001;276(18):14537–40.
Wang B, Matsuoka S, Ballif BA, Zhang D, Smogorzewska A, Gygi SP, et al. Abraxas and RAP80 form a BRCA1 protein complex required for the DNA damage response. Science. 2007;316(5828):1194–8.
Deng CX. BRCA1: cell cycle checkpoint, genetic instability, DNA damage response and cancer evolution. Nucleic Acids Res. 2006;34(5):1416–26.
Kolinjivadi AM, Sannino V, De Antoni A, Zadorozhny K, Kilkenny M, Techer H, et al. Smarcal1-mediated fork reversal triggers Mre11-dependent degradation of nascent DNA in the absence of Brca2 and stable Rad51 nucleofilaments. Mol Cell. 2017;67(5):867–81 e7.
Siaud N, Barbera MA, Egashira A, Lam I, Christ N, Schlacher K, et al. Plasticity of BRCA2 function in homologous recombination: genetic interactions of the PALB2 and DNA binding domains. PLoS Genet. 2011;7(12):e1002409.
Smith SA, Easton DF, Evans DG, Ponder BA. Allele losses in the region 17q12-21 in familial breast and ovarian cancer involve the wild-type chromosome. Nat Genet. 1992;2(2):128–31.
King TA, Li W, Brogi E, Yee CJ, Gemignani ML, Olvera N, et al. Heterogenic loss of the wild-type BRCA allele in human breast tumorigenesis. Ann Surg Oncol. 2007;14(9):2510–8.
Bryant HE, Schultz N, Thomas HD, Parker KM, Flower D, Lopez E, et al. Specific killing of BRCA2-deficient tumours with inhibitors of poly(ADP-ribose) polymerase. Nature. 2005;434(7035):913–7.
Farmer H, McCabe N, Lord CJ, Tutt AN, Johnson DA, Richardson TB, et al. Targeting the DNA repair defect in BRCA mutant cells as a therapeutic strategy. Nature. 2005;434(7035):917–21.
Lubinski J, Phelan CM, Ghadirian P, Lynch HT, Garber J, Weber B, et al. Cancer variation associated with the position of the mutation in the BRCA2 gene. Fam Cancer. 2004;3(1):1–10.
Struewing JP, Hartge P, Wacholder S, Baker SM, Berlin M, McAdams M, et al. The risk of cancer associated with specific mutations of BRCA1 and BRCA2 among Ashkenazi Jews. N Engl J Med. 1997;336(20):1401–8.
Frank TS, Deffenbaugh AM, Reid JE, Hulick M, Ward BE, Lingenfelter B, et al. Clinical characteristics of individuals with germline mutations in BRCA1 and BRCA2: analysis of 10,000 individuals. J Clin Oncol. 2002;20(6):1480–90.
Nielsen FC, van Overeem Hansen T, Sorensen CS. Hereditary breast and ovarian cancer: new genes in confined pathways. Nat Rev Cancer. 2016;16(9):599–612.
Lee JS, Oh S, Park SK, Lee MH, Lee JW, Kim SW, et al. Reclassification of BRCA1 and BRCA2 variants of uncertain significance: a multifactorial analysis of multicentre prospective cohort. J Med Genet. 2018;55(12):794–802.
Mesman RLS, Calleja F, Hendriks G, Morolli B, Misovic B, Devilee P, et al. The functional impact of variants of uncertain significance in BRCA2. Genet Med. 2019;21(2):293–302.
Werness BA, Ramus SJ, DiCioccio RA, Whittemore AS, Garlinghouse-Jones K, Oakley-Girvan I, et al. Histopathology, FIGO stage, and BRCA mutation status of ovarian cancers from the Gilda Radner Familial Ovarian Cancer Registry. Int J Gynecol Pathol. 2004;23(1):29–34.
Shaw PA, McLaughlin JR, Zweemer RP, Narod SA, Risch H, Verheijen RH, et al. Histopathologic features of genetically determined ovarian cancer. Int J Gynecol Pathol. 2002;21(4):407–11.
Pal T, Permuth-Wey J, Betts JA, Krischer JP, Fiorica J, Arango H, et al. BRCA1 and BRCA2 mutations account for a large proportion of ovarian carcinoma cases. Cancer. 2005;104(12):2807–16.
Rubin SC, Benjamin I, Behbakht K, Takahashi H, Morgan MA, LiVolsi VA, et al. Clinical and pathological features of ovarian cancer in women with germ-line mutations of BRCA1. N Engl J Med. 1996;335(19):1413–6.
Aida H, Takakuwa K, Nagata H, Tsuneki I, Takano M, Tsuji S, et al. Clinical features of ovarian cancer in Japanese women with germ-line mutations of BRCA1. Clin Cancer Res. 1998;4(1):235–40.
Berchuck A, Heron KA, Carney ME, Lancaster JM, Fraser EG, Vinson VL, et al. Frequency of germline and somatic BRCA1 mutations in ovarian cancer. Clin Cancer Res. 1998;4(10):2433–7.
Lim D, Oliva E. Precursors and pathogenesis of ovarian carcinoma. Pathology. 2013;45(3):229–42.
Crum CP, Drapkin R, Kindelberger D, Medeiros F, Miron A, Lee Y. Lessons from BRCA: the tubal fimbria emerges as an origin for pelvic serous cancer. Clin Med Res. 2007;5(1):35–44.
Colgan TJ, Murphy J, Cole DE, Narod S, Rosen B. Occult carcinoma in prophylactic oophorectomy specimens: prevalence and association with BRCA germline mutation status. Am J Surg Pathol. 2001;25(10):1283–9.
Shaw PA, Rouzbahman M, Pizer ES, Pintilie M, Begley H. Candidate serous cancer precursors in fallopian tube epithelium of BRCA1/2 mutation carriers. Mod Pathol. 2009;22(9):1133–8.
Kurman RJ, Shih IM. The origin and pathogenesis of epithelial ovarian cancer: a proposed unifying theory. Am J Surg Pathol. 2010;34(3):433–43.
Kurman RJ. Origin and molecular pathogenesis of ovarian high-grade serous carcinoma. Ann Oncol. 2013;24(Suppl 10):x16–21.
Vang R, Shih Ie M, Kurman RJ. Fallopian tube precursors of ovarian low- and high-grade serous neoplasms. Histopathology. 2013;62(1):44–58.
Callahan MJ, Crum CP, Medeiros F, Kindelberger DW, Elvin JA, Garber JE, et al. Primary fallopian tube malignancies in BRCA-positive women undergoing surgery for ovarian cancer risk reduction. J Clin Oncol. 2007;25(25):3985–90.
Kindelberger DW, Lee Y, Miron A, Hirsch MS, Feltmate C, Medeiros F, et al. Intraepithelial carcinoma of the fimbria and pelvic serous carcinoma: Evidence for a causal relationship. Am J Surg Pathol. 2007;31(2):161–9.
Leeper K, Garcia R, Swisher E, Goff B, Greer B, Paley P. Pathologic findings in prophylactic oophorectomy specimens in high-risk women. Gynecol Oncol. 2002;87(1):52–6.
Paley PJ, Swisher EM, Garcia RL, Agoff SN, Greer BE, Peters KL, et al. Occult cancer of the fallopian tube in BRCA-1 germline mutation carriers at prophylactic oophorectomy: a case for recommending hysterectomy at surgical prophylaxis. Gynecol Oncol. 2001;80(2):176–80.
Agoff SN, Garcia RL, Goff B, Swisher E. Follow-up of in situ and early-stage fallopian tube carcinoma in patients undergoing prophylactic surgery for proven or suspected BRCA-1 or BRCA-2 mutations. Am J Surg Pathol. 2004;28(8):1112–4.
Lee Y, Miron A, Drapkin R, Nucci MR, Medeiros F, Saleemuddin A, et al. A candidate precursor to serous carcinoma that originates in the distal fallopian tube. J Pathol. 2007;211(1):26–35.
Kuhn E, Kurman RJ, Vang R, Sehdev AS, Han G, Soslow R, et al. TP53 mutations in serous tubal intraepithelial carcinoma and concurrent pelvic high-grade serous carcinoma—evidence supporting the clonal relationship of the two lesions. J Pathol. 2012;226(3):421–6.
Chalmers ZR, Connelly CF, Fabrizio D, Gay L, Ali SM, Ennis R, et al. Analysis of 100,000 human cancer genomes reveals the landscape of tumor mutational burden. Genome Med. 2017;9(1):34.
Latham A, Srinivasan P, Kemel Y, Shia J, Bandlamudi C, Mandelker D, et al. Microsatellite instability is associated with the presence of Lynch syndrome pan-cancer. J Clin Oncol. 2019;37(4):286–95.
Umar A, Boland CR, Terdiman JP, Syngal S, de la Chapelle A, Ruschoff J, et al. Revised Bethesda Guidelines for hereditary nonpolyposis colorectal cancer (Lynch syndrome) and microsatellite instability. J Natl Cancer Inst. 2004;96(4):261–8.
Boland CR, Thibodeau SN, Hamilton SR, Sidransky D, Eshleman JR, Burt RW, et al. A National Cancer Institute Workshop on Microsatellite Instability for cancer detection and familial predisposition: development of international criteria for the determination of microsatellite instability in colorectal cancer. Cancer Res. 1998;58(22):5248–57.
Richman S. Deficient mismatch repair: Read all about it (Review). Int J Oncol. 2015;47(4):1189–202.
Bando H, Okamoto W, Fukui T, Yamanaka T, Akagi K, Yoshino T. Utility of the quasi-monomorphic variation range in unresectable metastatic colorectal cancer patients. Cancer Sci. 2018;109(11):3411–5.
Cook LS, Nelson HE, Stidley CA, Dong Y, Round PJ, Amankwah EK, et al. Endometrial cancer and a family history of cancer. Gynecol Oncol. 2013;130(2):334–9.
Peterson LM, Kipp BR, Halling KC, Kerr SE, Smith DI, Distad TJ, et al. Molecular characterization of endometrial cancer: a correlative study assessing microsatellite instability, MLH1 hypermethylation, DNA mismatch repair protein expression, and PTEN, PIK3CA, KRAS, and BRAF mutation analysis. Int J Gynecol Pathol. 2012;31(3):195–205.
Kobayashi K, Sagae S, Kudo R, Saito H, Koi S, Nakamura Y. Microsatellite instability in endometrial carcinomas: frequent replication errors in tumors of early onset and/or of poorly differentiated type. Genes Chromosomes Cancer. 1995;14(2):128–32.
Singer G, Kallinowski T, Hartmann A, Dietmaier W, Wild PJ, Schraml P, et al. Different types of microsatellite instability in ovarian carcinoma. Int J Cancer. 2004;112(4):643–6.
Malander S, Rambech E, Kristoffersson U, Halvarsson B, Ridderheim M, Borg A, et al. The contribution of the hereditary nonpolyposis colorectal cancer syndrome to the development of ovarian cancer. Gynecol Oncol. 2006;101(2):238–43.
Bellizzi AM, Frankel WL. Colorectal cancer due to deficiency in DNA mismatch repair function: a review. Adv Anat Pathol. 2009;16(6):405–17.
Herman JG, Umar A, Polyak K, Graff JR, Ahuja N, Issa JP, et al. Incidence and functional consequences of hMLH1 promoter hypermethylation in colorectal carcinoma. Proc Natl Acad Sci U S A. 1998;95(12):6870–5.
Koinuma K, Shitoh K, Miyakura Y, Furukawa T, Yamashita Y, Ota J, et al. Mutations of BRAF are associated with extensive hMLH1 promoter methylation in sporadic colorectal carcinomas. Int J Cancer. 2004;108(2):237–42.
McGivern A, Wynter CV, Whitehall VL, Kambara T, Spring KJ, Walsh MD, et al. Promoter hypermethylation frequency and BRAF mutations distinguish hereditary non-polyposis colon cancer from sporadic MSI-H colon cancer. Fam Cancer. 2004;3(2):101–7.
Kawaguchi M, Yanokura M, Banno K, Kobayashi Y, Kuwabara Y, Kobayashi M, et al. Analysis of a correlation between the BRAF V600E mutation and abnormal DNA mismatch repair in patients with sporadic endometrial cancer. Int J Oncol. 2009;34(6):1541–7.
Tanakaya K. Current clinical topics of Lynch syndrome. Int J Clin Oncol. 2019;24(9):1013–9.
Broaddus RR, Lynch HT, Chen LM, Daniels MS, Conrad P, Munsell MF, et al. Pathologic features of endometrial carcinoma associated with HNPCC: a comparison with sporadic endometrial carcinoma. Cancer. 2006;106(1):87–94.
Westin SN, Lacour RA, Urbauer DL, Luthra R, Bodurka DC, Lu KH, et al. Carcinoma of the lower uterine segment: a newly described association with Lynch syndrome. J Clin Oncol. 2008;26(36):5965–71.
Masuda K, Banno K, Hirasawa A, Yanokura M, Tsuji K, Kobayashi Y, et al. Relationship of lower uterine segment cancer with Lynch syndrome: a novel case with an hMLH1 germline mutation. Oncol Rep. 2012;28(5):1537–43.
https://www.cancer.org/cancer/ovarian-cancer/about/key-statistics.html. Accessed 15 Nov 2020.
Risch HA, McLaughlin JR, Cole DE, Rosen B, Bradley L, Fan I, et al. Population BRCA1 and BRCA2 mutation frequencies and cancer penetrances: a kin-cohort study in Ontario, Canada. J Natl Cancer Inst. 2006;98(23):1694–706.
Domanska K, Malander S, Masback A, Nilbert M. Ovarian cancer at young age: the contribution of mismatch-repair defects in a population-based series of epithelial ovarian cancer before age 40. Int J Gynecol Cancer. 2007;17(4):789–93.
Lancaster JM, Powell CB, Kauff ND, Cass I, Chen LM, Lu KH, et al. Society of Gynecologic Oncologists Education Committee statement on risk assessment for inherited gynecologic cancer predispositions. Gynecol Oncol. 2007;107(2):159–62.
Konstantinopoulos PA, Norquist B, Lacchetti C, Armstrong D, Grisham RN, Goodfellow PJ, et al. Germline and somatic tumor testing in epithelial ovarian cancer: ASCO guideline. J Clin Oncol. 2020;38(11):1222–45.
Referenced with permission from the NCCN Guidelines® for Guideline Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic Version.1.2021 © National Comprehensive Cancer Network, Inc. 2020. All rights reserved. Accessed 14 Sept 2020. Available online at www.NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way.
US Preventive Services Task Force, Owens DK, Davidson KW, Krist AH, Barry MJ, Cabana M, et al. Risk Assessment, Genetic Counseling, and Genetic Testing for BRCA-Related Cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2019;322(7):652–65.
Lu KH, Daniels M. Endometrial and ovarian cancer in women with Lynch syndrome: update in screening and prevention. Fam Cancer. 2013;12(2):273–7.
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Cancer J Clin. 2017;67(1):7–30.
Schmeler KM, Lynch HT, Chen LM, Munsell MF, Soliman PT, Clark MB, et al. Prophylactic surgery to reduce the risk of gynecologic cancers in the Lynch syndrome. N Engl J Med. 2006;354(3):261–9.
Li MM, Chao E, Esplin ED, Miller DT, Nathanson KL, Plon SE, et al. Points to consider for reporting of germline variation in patients undergoing tumor testing: a statement of the American College of Medical Genetics and Genomics (ACMG). Genet Med. 2020;22(7):1142–8.
Green RC, Berg JS, Grody WW, Kalia SS, Korf BR, Martin CL, et al. ACMG recommendations for reporting of incidental findings in clinical exome and genome sequencing. Genet Med. 2013;15(7):565–74.
Kalia SS, Adelman K, Bale SJ, Chung WK, Eng C, Evans JP, et al. Recommendations for reporting of secondary findings in clinical exome and genome sequencing, 2016 update (ACMG SF v2.0): a policy statement of the American College of Medical Genetics and Genomics. Genet Med. 2017;19(2):249–55.
Mandelker D, Donoghue M, Talukdar S, Bandlamudi C, Srinivasan P, Vivek M, et al. Germline-focussed analysis of tumour-only sequencing: recommendations from the ESMO Precision Medicine Working Group. Ann Oncol. 2019;30(8):1221–31.
Acknowledgments
This work was supported in part by Health Labour Sciences Research Grant (20EA1027), Foundation for Promotion of Cancer Research in Japan, and Daiwa Securities Health Foundation.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 The Author(s), under exclusive license to Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Yamamoto, H., Hirasawa, A. (2021). Hereditary Gynecological Malignancy and Molecular Features. In: Isonishi, S., Kikuchi, Y. (eds) Molecular Diagnosis and Targeting for Gynecologic Malignancy. Current Human Cell Research and Applications. Springer, Singapore. https://doi.org/10.1007/978-981-33-6013-6_12
Download citation
DOI: https://doi.org/10.1007/978-981-33-6013-6_12
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-33-6012-9
Online ISBN: 978-981-33-6013-6
eBook Packages: MedicineMedicine (R0)