
Abstract
The diagnosis of intrauterine adhesions (IUAs) and Asherman’s syndrome has always been challenging. The development of diagnostic techniques and the raised awareness of the condition have led to a more reliable diagnosis and management of this intrauterine pathology. In this chapter, we summarize how to make the diagnosis of IUAs and Asherman’s syndrome, starting from the clinical suspicion, the first-level techniques (ultrasound scan), and the second-level ones for confirmation (hysteroscopy, or when this is not available, hysterosalpingography, sonohysterography, and magnetic resonance imaging). In particular, we highlight the key diagnostic elements for each step of the diagnostic process to suggest a specific flowchart to follow.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
5.1 Introduction
The diagnosis of intrauterine adhesions (IUAs) and Asherman’s syndrome has always been challenging [1, 2]. To date, the development of diagnostic techniques and the raised awareness of the condition have led to a more reliable diagnosis and management of this intrauterine pathology [3].
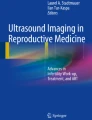
Hysteroscopy has been recognized as the gold standard for both the diagnosis and treatment of intrauterine adhesions, allowing clear visualization of the uterine cavity [4,5,6,7,8]. Nevertheless, the correct diagnostic flowchart (Fig. 5.1) for both IUAs and Asherman’s syndrome should start from clinical suspicion and ultrasonography and, therefore, confirmation by hysteroscopy or, when hysteroscopy is not available, by other diagnostic techniques such as hysterosalpingography (HSG), sonohysterography (SHG), or magnetic resonance imaging (MRI) [1].

Flowchart for the diagnosis of intrauterine adhesions and Asherman’s syndrome
5.1.1 Clinical Suspicion
IUAs can be asymptomatic or symptomatic [3]. Usually, women can refer no symptoms as well as menstrual disorders, including infrequent, mild, or no bleeding, reduced days of menstruation, dysmenorrhea, and, very rarely, heavy menstrual bleeding [9, 10]. In particular, menstrual bleeding is not strictly linked to the severity and location of adhesions [11]. Patients could complain of secondary infertility as the initial symptom, which is associated with Asherman’s syndrome in approximately 40% of women [12]. In this regard, it has been hypothesized that disturbed endometrial vascularization, due to adhesions, could lead to implantation failure; in addition, embryo implantation could be impaired due to mechanical impediments (partially or totally obliterated uterine cavity) [13].
The vaginal examination does not provide reliable information regarding the potential presence of IUAs, so the diagnosis should rely first of all on an accurate and detailed clinical history collection to rule out other possible causes of secondary amenorrhea/hypomenorrhea/menstrual irregularities and/or infertility, as well as identify risk factors for IUAs such as intrauterine curettage, uterine embolization, B-lynch sutures, abdominal/hysteroscopic myomectomy, genital tuberculosis, or surgical treatment of Müllerian anomalies [14,15,16,17,18,19,20,21]. After clinical history collection, ultrasonography represents the first step to investigate IUAs.
5.1.2 Ultrasonography
Ultrasonography should be used routinely as the first diagnostic tool, although the skill of the operator affects the diagnostic accuracy of the technique [22]. Intrauterine adhesions can be focused as transversal bands of myometrial tissue that cross the uterine cavity and connect the opposing uterine walls. Usually, bands have the same or augmented echogenicity of the surrounding myometrium and vary in length and thickness [23].
In the case of mild adhesions, endometrium should be clearly visible, and thin echogenic bands should be visualized inside a distended uterine cavity. The more the syndrome is severe, the most the bands should be rigid and thick, with hypoechogenic material between them. In the case of severe adhesions, the uterine cavity could be found morphologically irregular with a loss of endometrial echo [24].
A typical endometrial pattern is represented by “skip lesions”: interruptions of the endometrial layer by means of several hypoechoic areas, which are images of accumulated menstrual blood or detached endometrium [9].
The operator should be aware that if the internal cervical orifice is obliterated, the uterine cavity may be distended by menstrual blood and debris. Transversal bands are often not visible [22]. In case of significant IUAs, the endometrium could appear thin (atrophic) because of low estrogenic responsiveness that usually is restored after IUA divisions [22].
Nevertheless, data published so far are not robust enough to lead to an agreement about the sensitivity of ultrasonography for the diagnosis of IUAs and Asherman’s syndrome [25, 26]. To date, although the evolution of 3D and 4D ultrasonography has somehow improved the diagnostic accuracy with respect to the “classic” 2D scan [27, 28], further trials are needed to assess their efficacy in terms of sensitivity, specificity, and positive and negative predictive values.
5.1.3 Hysteroscopy
Hysteroscopy is a feasible, safe, and cost-effective diagnostic and therapeutic option for IUAs and Asherman’s syndrome [29,30,31,32]. During hysteroscopy, adhesions can be generally described in several ways: thin or subtle bands or stripes without vascularization that connect two opposite walls, or agglutinations of the walls that are able to completely or partially obliterate the uterine cavity [22]. It is essential for the operator to carefully define the number, location, extension, and structure of adhesions, as follows:
-
A.
Number: the number of synechiae inside the cavity
-
B.
Location of adhesions: central or marginal
-
B1.
Central: columnar shaped bands attached to two opposite walls of the uterine cavity with blazed ends
-
B2.
Marginal: sickle-shaped bands able to obliterate the uterine wall partially; the uterine cavity appears asymmetrical in shape
-
B1.
-
C.
Extension: mild, moderate, or severe
If the synechiae completely obliterate the cavity, this appears narrow and assumes a tubular-shaped conformation. In the case of Asherman’s syndrome (severe synechiae in association with dysmenorrhea and changes in menstrual patterns), only fibrous tissue could be seen, with just poor irregular endometrial bridges linked in between.
-
D.
Structure and consistency: identify which tissue is predominant (mucosal, muscular, or fibrous)
-
D1.
Mucosal: similar to the healthy physiological endometrium, easy to resect, delicate, laminar, without vascularization or specific structure.
-
D2.
Muscular: structured with an axis of muscular tissue covered by a thin line of endometrium surrounded by glandular outlets.
-
D3.
Fibrous: those synechiae are composed primarily of connective tissue, which can be easily differentiated from normal endometrium; they appear white and translucent, with no vascularization and mainly surrounded by atrophic endometrium.
-
D1.
It is important for the operator to schematically categorize adhesions using a specific classification system. To date, several classification systems are being routinely used by gynecologists [29,30,31, 33, 34]; however, there is no evidence supporting the superiority of one over the others [1]. The first classification was developed by March et al. in 1978 [29]. This classification divides IUAs into three groups according to extension in mild, moderate, and severe (Table 5.1). Among the other classification systems, there are those developed by Valle and Sciarra in 1988 [31], by Donnez and Nisolle in 1994 [35], and by the American Fertility Society in 1998 [34], which is to date the most used worldwide.
5.1.4 Other Diagnostic Techniques
HSG using contrast dye has a sensitivity of 75–81%, a specificity of 80%, and a positive predictive value of 50% compared to hysteroscopy for diagnosis of IUAs [22, 26, 36]. Using HSG, synechiae were indirectly referred to as filling defects and irregularly in-between-shaped spaces in images, with clear margins and homogeneous opacity. When severe IUAs are suspected, the uterine cavity would appear reduced in volume and distorted in shape with occluded tubes in the majority of cases [37]. Compared to hysteroscopy, HSG has been reported to have a similar sensitivity, although a large number of false-positive findings are considered a limitation to its use [26, 36].
SHG, also called saline infusion sonography (SIS) or gel infusion sonography (GIS), was found to be as effective as HSG, with both reported to have a sensitivity of 75% and a positive predictive value of 43% for SHG or SIS/GIS and 50% for HSG, compared to hysteroscopy [26, 38].
MRI has also been evaluated for the diagnosis of IUAs; nevertheless, the high cost of the procedure does not justify its routine use for diagnosis of IUAs and Asherman’s syndrome [39, 40].
Key Points
-
1.
Secondary infertility as an initial symptom is associated with Asherman’s syndrome in approximately 40% of women.
-
2.
Menstrual disorders, such as mild or no bleeding, reduced days of menstruations, and dysmenorrhea, could also be associated.
-
3.
The most common risk factors for Asherman’s syndrome are previous intrauterine curettage, uterine embolization, B-lynch sutures, abdominal/hysteroscopic myomectomy, genital tuberculosis, or surgical treatment of Müllerian anomalies.
-
4.
The vaginal examination does not provide reliable diagnostic information for Asherman’s syndrome.
-
5.
After an initial assessment by medical history, an ultrasound scan should be considered the first diagnostic step.
-
6.
At the ultrasound scan, intrauterine adhesions can be focused as transversal bands of myometrial tissue that cross the uterine cavity and connect the opposing uterine walls. Usually, bands have the same or increased echogenicity of the surrounding myometrium and can vary in length and thickness.
-
7.
The more the syndrome is severe, the most the bands should be rigid and thick, with hypoechogenic material between them. In the case of severe adhesions, the uterine cavity could be found morphologically irregular with a loss of endometrial echoes.
-
8.
After an ultrasound scan, the confirmation of Asherman’s syndrome is recommended by hysteroscopy, describing the following elements: number, location, extension, structure, and consistency of adhesions.
-
9.
To date, there is no evidence supporting the use of one classification system of intrauterine adhesions over the others, although the most used worldwide was developed by the American Fertility Society.
-
10.
Magnetic resonance imaging is not cost-effective for the diagnosis of intrauterine adhesions.
References
Dreisler E, Kjer JJ. Asherman’s syndrome: current perspectives on diagnosis and management. Int J Women’s Health. 2019;20:191–9.
Zupi E, Centini G, Lazzeri L. Asherman syndrome: an unsolved clinical definition and management. Fertil Steril. 2015;104:1380–1.
Hanstede MMF, Van Der Meij E, Goedemans L, Emanuel MH. Results of centralized Asherman surgery, 2003–2013. Fertil Steril. 2015;104:1561.e1–8.e1.
Khan Z, Goldberg JM. Hysteroscopic management of Asherman’s syndrome. J Minim Invasive Gynecol. 2018;25:218–28.
Bougie O, Lortie K, Shenassa H, Chen I, Singh SS. Treatment of Asherman’s syndrome in an outpatient hysteroscopy setting. J Minim Invasive Gynecol. 2015;22:446–50.
Amer-Cuenca JJ, Marín-Buck A, Vitale SG, La Rosa VL, Caruso S, Cianci A, Lisón JF. Non-pharmacological pain control in outpatient hysteroscopies. Minim Invasive Ther Allied Technol. 2020;29(1):10–9. https://doi.org/10.1080/13645706.2019.1576054.
Kriseman M, Schutt A, Appleton J, Pillai A, George V, Zarutskie PW. A novel ultrasound-guided technique for hysteroscopic adhesiolysis in high-risk patients. J Ultrasound Med. 2019;38:1383–7.
Laganà AS, Vitale SG, Muscia V, et al. Endometrial preparation with dienogest before hysteroscopic surgery: a systematic review. Arch Gynecol Obstet. 2017;295:661–7.
Yu D, Wong YM, Cheong Y, Xia E, Li TC. Asherman syndrome - one century later. Fertil Steril. 2008;89:759–79.
Salazar CA, Isaacson K, Morris S. A comprehensive review of Asherman’s syndrome: causes, symptoms and treatment options. Curr Opin Obstet Gynecol. 2017;29:249–56.
March CM. Management of Asherman’s syndrome. Reprod BioMed Online. 2011;23:63–76.
Tsui KH, Te Lin L, Cheng JT, Teng SW, Wang PH. Comprehensive treatment for infertile women with severe Asherman syndrome. Taiwan J Obstet Gynecol. 2014;53:372–5.
Azizi R, Aghebati-Maleki L, Nouri M, Marofi F, Negargar S, Yousefi M. Stem cell therapy in Asherman syndrome and thin endometrium: stem cell-based therapy. Biomed Pharmacother. 2018;102:333–43.
Song D, Liu Y, Xiao Y, Li TC, Zhou F, Xia E. A matched cohort study comparing the outcome of intrauterine adhesiolysis for Asherman’s syndrome after uterine artery embolization or surgical trauma. J Minim Invasive Gynecol. 2014;21(6):1022–8. https://doi.org/10.1016/j.jmig.2014.04.015.
Vitale SG, Sapia F, Rapisarda AMC, et al. Hysteroscopic morcellation of submucous myomas: a systematic review. Biomed Res Int. 2017;2017:6848250.
Zhu R, Gan L, Wang S, Duan H. A cohort study comparing the severity and outcome of intrauterine adhesiolysis for Asherman syndrome after first- or second-trimester termination of pregnancy. Eur J Obstet Gynecol Reprod Biol. 2019;238:49–53.
Gilman Barber AR, Rhone SA, Fluker MR. Curettage and Asherman’s syndrome-lessons to (re-) learn? J Obstet Gynaecol Can. 2014;36:997–1001.
Di Spiezio SA, Gencarelli A, Vieira MDC, Riemma G, De Simone T, Carugno J. Differentiating a rare uterine lipoleiomyoma from uterine perforation at hysteroscopy: a scary story. J Minim Invasive Gynecol. 2019;27(1):9–10. https://doi.org/10.1016/j.jmig.2019.04.020.
Laganà AS, Alonso Pacheco L, Tinelli A, Haimovich S, Carugno J, Ghezzi F, Mazzon I, Bettocchi S. Management of asymptomatic submucous myomas in women of reproductive age: a consensus statement from the global congress on hysteroscopy scientific committee. J Minim Invasive Gynecol. 2019;26:381–3.
Alonso Pacheco L, Laganà AS, Ghezzi F, Haimovich S, Azumendi Gómez P, Carugno J. Subtypes of T-shaped uterus. Fertil Steril. 2019;112:399–400.
Alonso Pacheco L, Laganà AS, Garzon S, Perez Garrido A, Flores Gornes A, Ghezzi F. Hysteroscopic outpatient metroplasty for T-shaped uterus in women with reproductive failure: results from a large prospective cohort study. Eur J Obstet Gynecol Reprod Biol. 2019;243:173–8. https://doi.org/10.1016/j.ejogrb.2019.09.023.
Amin TN, Saridogan E, Jurkovic D. Ultrasound and intrauterine adhesions: a novel structured approach to diagnosis and management. Ultrasound Obstet Gynecol. 2015;46:131–9.
Leone FPG, Timmerman D, Bourne T, et al. Terms, definitions and measurements to describe the sonographic features of the endometrium and intrauterine lesions: a consensus opinion from the International Endometrial Tumor Analysis (IETA) group. Ultrasound Obstet Gynecol. 2010;35:103–12.
Naftalin J, Jurkovic D. The endometrial-myometrial junction: a fresh look at a busy crossing. Ultrasound Obstet Gynecol. 2009;34:1–11.
Fedele L, Bianchi S, Dorta M, Vignali M. Intrauterine adhesions: detection with transvaginal US. Radiology. 1996;199:757–9.
Soares SR, Dos Reis MMBB, Camargos AF. Diagnostic accuracy of sonohysterography, transvaginal sonography, and hysterosalpingography in patients with uterine cavity diseases. Fertil Steril. 2000;73:406–11.
Knopman J, Copperman AB. Value of 3D ultrasound in the management of suspected Asherman’s syndrome. J Reprod Med Obstet Gynecol. 2007;52:1016–22.
Laganà AS, Ciancimino L, Mancuso A, Chiofalo B, Rizzo P, Triolo O. 3D sonohysterography vs. hysteroscopy: a cross-sectional study for the evaluation of endouterine diseases. Arch Gynecol Obstet. 2014;290:1173–8.
March CM, Israel R, March AD. Hysteroscopic management of intrauterine adhesions. Am J Obstet Gynecol. 1978;130:653–7.
Hamou J, Cittadini E, Perino A. Diagnosis and management of intrauterine adhesions by microhysteroscopy. Acta Eur Fertil. 1983;14:117–23.
Valle RF, Sciarra JJ. Intrauterine adhesions: hysteroscopic diagnosis, classification, treatment, and reproductive outcome. Am J Obstet Gynecol. 1988;158:1459–70.
Pabuçcu R, Urman B, Atay V, Ergün A, Orhon E. Hysteroscopic treatment of intrauterine adhesions is safe and effective in the restoration of normal menstruation and fertility. Fertil Steril. 1997;68:1141–3.
Aboul Nasr AL, Al-Inany HG, Thabet SM, Aboulghar M. A clinicohysteroscopic scoring system of intrauterine adhesions. Gynecol Obstet Investig. 2000;50:178–81.
Buttram VC, Gomel V, Siegler A, DeCherney A, Gibbons W, March C. The American Fertility Society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, Mullerian anomalies and intrauterine adhesions. Fertil Steril. 1988;49:944–55.
Donnez J, Nisolle M. Hysteroscopic adhesiolysis of intrauterine adhesions (Asherman syndrome). Hysteroscopy: An Atlas Laser Oper. Laparosc; 1994.
Dalfó AR, Úbeda B, Úbeda A, Monzón M, Rotger R, Ramos R, Palacio A. Diagnostic value of hysterosalpingography in the detection of intrauterine abnormalities: a comparison with hysteroscopy. Am J Roentgenol. 2004;183:1405–9.
Ahmadi F, Siahbazi S, Akhbari F, Eslami B, Vosough A. Hysterosalpingography finding in intrauterine adhesion (Asherman’s syndrome): a pictorial essay. Int J Fertil Steril. 2013;7:155–60.
Salle B, Gaucherand P, De Saint Hilaire P, Rudigoz RC. Transvaginal sonohysterographic evaluation of intrauterine adhesions. J Clin Ultrasound. 1999;27:131–4.
Letterie GS, Haggerty MF. Magnetic resonance imaging of intrauterine synechiae. Gynecol Obstet Investig. 1994;37:66–8.
Bacelar AC, Wilcock D, Powell M, Worthington BS. The value of MRI in the assessment of traumatic intra-uterine adhesions (Asherman’s syndrome). Clin Radiol. 1995;50:80–3.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Laganà, A.S., Garzon, S., Riemma, G., Vitale, S.G. (2021). Diagnosis: Patient Evaluation (Flowchart). In: Manchanda, R. (eds) Intra Uterine Adhesions. Springer, Singapore. https://doi.org/10.1007/978-981-33-4145-6_5
Download citation
DOI: https://doi.org/10.1007/978-981-33-4145-6_5
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-33-4144-9
Online ISBN: 978-981-33-4145-6
eBook Packages: MedicineMedicine (R0)