
Abstract
The development of fast, non-invasive and accurate diagnostics is of great importance in the medical field. Lasers, and optical spectroscopy and imaging techniques provide many new possibilities. Most frequently broad-band spectroscopic techniques are used for studying tissue constituents. Instead, the development of novel methods for monitoring free gas in situ using narrow-band laser spectroscopic techniques in the diagnostics of common infectious diseases and for the surveillance of pre-term infants is presented in this chapter. The gas in scattering media absorption spectroscopy (GASMAS) technique is used, relying on the fact, that the absorptive imprints of free gases are typically 10,000 times narrower than those due to the tissue itself. The work is in a translational process aiming at better diagnostics of common sinus and middle-ear infections (sinusitis and otitis) and for the management of the respiratory distress syndrome and necrotizing enterocolitis in premature infants.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Biophotonics deals with medical and biological applications of light from lasers, light-emitting diodes (LEDs) or classical light sources. As a research field it has expanded very rapidly. Recent reviews of the field include Refs. [1–5]. Many techniques deal with the study of biological samples on a microscopic level with the purpose of a fundamental understanding of function or for diagnostics of diseases. Other techniques address the study of larger areas of tissue in vivo, aiming at real-time classification of tissue and visualization of areas with pathological transformations. Fundamental interaction mechanisms of spectroscopic nature are discussed, e.g. in [6]. Laser light is also being used for therapeutical applications in laser surgery and other types on interventions. Some of these applications have a strong spectroscopic aspect, i.e. the choice of interaction wavelength is very important, e.g. in photodynamic therapy (see, e.g. [7]).
Biological tissue falls, from a basic physical classification scheme, into the area of condensed matter physics, which deals with solids and liquids. It is well known, that condensed matter shows only relatively broad spectroscopic features. Because of strong interaction between atoms and molecules the energy level structure becomes smeared, resulting in the corresponding spectra, generated in radiative transitions between such energy levels, to become relatively broad. Absorption, reflectance and fluorescence spectra rarely exhibit peaks narrower than 10 nm. Thus, lasers and other light sources do not need to be exceedingly well defined in frequency and linewidth, which facilitates the technical implementation of most biophotonics studies, while also leading to less sharp spectral “fingerprints” and associated reduced specificity in diagnostics.
In contrast, free gases, being little perturbed by interactions even at atmospheric pressures, exhibit very sharp spectral features, in absorption as well as emission. Accordingly, spectral lines of gases must be specified in wavelength to 6 significant digits, with the linewidth determined by Doppler broadening (typical thermal velocities are a millionth of the velocity of light) and pressure broadening, which is of the same magnitude.
This chapter deals with the monitoring of free gases in biophotonics. Laser sources with high wavelength definition are then required for high-resolution laser spectroscopy, and techniques developed for the study of atmospheric gases, e.g. in connection with pollution studies, are needed (see, e.g. [8]).
Free gas monitoring in connection with biophotonics basically deals with two aspects. The first one concerns extracorporal analysis of gases, in particular breath analysis. Here the monitoring is performed in a gas cell, which is filled with the sample of interest [9, 10]. A high sensitivity is needed, since gases, specific to certain diseases, are frequently in very low concentrations, requiring the use of multi-pass optical absorption cells or photoacoustic detection. Applications include the detection of certain types of malignant diseases, diabetes, renal failure, etc. Similar analysis related to, e.g. plant or insect respiration, is also being performed (see, e.g. [11, 12]).
The second type of free gas monitoring in biophotonics is a more recent one, and is the topic of the present chapter. Here we deal with free gas being studied in situ in living tissue, such as paranasal sinuses, the middle ear, lungs and intestines. The major difference from other types of optical gas measurements is, that we here deal with a situation, where massive scattering in the surrounding tissue causes two main problems which have to be dealt with:
-
1.
The optical pathlength through the gas becomes undefined; thus the Beer-Lambert law customarily used for gas concentration assessment is not applicable.
-
2.
Scattering and absorption in the surrounding tissue cause very strong attenuation of the detected light, even if the “tissue optical window” 600–1300 nm with comparatively low absorption by tissue constituents, is employed.
A new type of laser spectroscopy was developed to deal with these complications: Gas in scattering media absorption spectroscopy (GASMAS) [13]. It combines experience from the environmental monitoring field, where sensitive detection of sharp absorption lines in a non-scattering environment is employed, and the biophotonics field, where broad-band structures are studied in a heavily scattering context [14–16].
The lay-out of the present chapter is as follows. The medical background to in situ gas monitoring in the human body is given in the next section. Then, in Sect. 3 we present the basics of the GASMAS technique and how to overcome problems encountered in scattering media. Here also non-medical applications of the technique, e.g. in material sciences, food sciences and the pharmaceutical field are briefly mentioned. Then, in three following sections, specific applications to the human sinus cavities, to the management of middle-ear infection, and to the monitoring of neonatal children will be covered. Finally, in Sect. 7, conclusions and an outlook for the future are given.
2 Medical Background to In Situ Monitoring of Gas in the Human Body
We will here present some medical background to the studies presented in this chapter. We will first present the general requirements for medical diagnostics, then we will discuss the management of common infectious diseases such as sinuitis (sinus cavity inflammation) and otitis (middle ear inflammation) and the mounting threat of bacterial antibiotic resistance. Finally, we will describe monitoring of oxygenation with special emphasis on neonatal children needs.
2.1 Need for Fast and Non-invasive Detection, Monitoring and Characterisation
Before applying therapy a disease or a lesion has to be reliably monitored and characterised. Otherwise the therapy cannot be specifically directed. The majority of clinical cases can be handled with well established methods, sometimes referred to as gold standard methods, such as immuno/histopathology in oncology, and the use of the Polymerase Chair Reaction (PCR) or Petri dish bacteria growth, with or without antibiotics response study, for infectious diseases [17, 18]. Tumour detection relies mainly on ionising radiation based investigations, such as computed tomography, scintigraphy and positron emission tomography, but also on ultrasound and magnetic resonance imaging. However, very early only few cell layers thick lesions are not detectable by these techniques. Also in endoscopical investigations in hollow organs, there are situations when a tumour cannot be recognised or detected and thus no biopsy can be collected for further histopathological investigation [19–21]. These clinical situations are examples where it would be of value to develop complementary non-invasive laser/light based spectroscopy methods for more precise detection of the target of interest. Potentially attractive features of optical techniques include non-invasiveness, real-time presentation of findings and useful sensitivity and specificity [6, 22, 23]. A lot of translational research efforts have been pursued, and some important additions have been brought all the way from the laboratory to the clinic. These techniques include fluorescence detection for bladder carcinoma visualization [24], and the use of optical coherence tomography (OCT) for the monitoring of retinal disease [25].
Diagnostics based on free gases are in an early state of development but have substantial potential. We have mentioned spectroscopic monitoring of breath gases [9, 10]. GASMAS measures free gases in situ in the human body using high-resolution laser spectroscopy. While in principle many gases could be studied, in practice the studies are focussing on oxygen gas and water vapour, which have useful molecular transitions falling in the tissue optical window ranging from 600 to 1300 nm. The high concentration of these gases in the body compensates for the fact, that the transitions are quite weak. Since the light reaching the detector is faint due to scattering and absorption in the bulk tissue, trace gases presently fall outside the attainable realm.
Water vapour fills a confined volume at the saturation level as long as free water is present, which is always the case in living biological tissue. This is true irrespectively of what other gases are present. The detection of the sharp spectral signature of water vapour indicates that the detected light has passed a cavity filled with free gas. Generally speaking, a larger signal corresponds to a larger cavity, everything else being the same. The absence of a water vapour signal would indicate, that the cavity is instead filled with liquid, as is frequently the case for sinusitis and otitis.
Oxygen is a physiologically very important gas in the respiration. GASMAS can monitor the free oxygen gas in contrast to the common monitoring of the oxygen saturation in blood, where the relationship between oxyhaemoglobin and deoxyhaemaoglobin is monitored, e.g. by pulse oximeters [26]. We would like to emphasize the strong difference between oxygen bound to haemoglobin, which results in a broadband spectral imprint typical for condensed matter, and free oxygen molecules forming a constituent of the gas enclosed in a body cavity of varying size (sinuses or a lung alveolae). The local oxygen concentration can give information of the status at that particular site, while the oxygen saturation measured by classical oximetry gives a global value for the efficiency of the respiration. Broad-band measurements on blood include pulse oximetry, tissue viability monitoring and laser-Doppler flowmetry, techniques which assess the degree of oxygenation, blood volume and blood flow (see, e.g. [27, 28]).
Free oxygen gas concentration is also of interest to assess the ventilation of a cavity through the sinus ostia or through the middle ear Eustachian tube. A concentration close to ambient would indicate functioning ventilation pathways, while a low, or zero concentration in spite of free gas being present as judged from the water vapour signal, would indicate blocked passages and/or might carry information on the prevalence of aerobic/anaerobic bacteria.
2.2 Infectious Diseases and Antibiotics Resistance
The sinus cavities, most commonly the frontal and maxillary sinuses, which are normally air-filled cavities in the human cranium, often become the sites of infectious diseases [29, 30]. Sinusitis in adults is usually treated as bacterial infections even if it is well known, that most sinus infections are viral, and only a small proportion develops a secondary bacterial infection. In fact, only 10 % of the sinusitis exhibit bacterial origin and could be treated with antibiotics, since the remaining cases are related to viral or allergic reactions [31]. Due to decades of overprescription of antibiotics we have reached a point where bacteria become resistant to the standard therapy and more broad spectrum antibiotics have to be used [32–35]. Important to have in mind is also that the pharmaceutical industry is mostly not developing new antibiotics as it was during the period 1960–1980, which means that the availability of effective antibiotics is decreasing.
Acute middle ear infection (Acute Otitis Media, AOM) in small children is another very common infectious disease which most often is treated without more precise identification of the infectious agents [36–38]. The medical background to the high incidence of middle ear infection is the anatomy of the Eustachian tube, which at young age is horizontal and therefore has a slow release of fluid from the ear to the nasopharynx. Approximately 80 % of children below the age of 3 years have had an ear infection and up to 20–30 % have an average of 6 recurrencies below the age of 6 years. Although it is a fact that the majority of children with AOM (70–90 %) have spontaneous resolution within 7–14 days, there is an over prescription of antibiotics also for this disease [39]. A standard therapy for AOM is the antibiotic drug Amoxicillin. In some countries, e.g. China, it is now not effective any longer due to resistance that has been developed due to over prescription [35].
There is a need for more precise diagnosis so the bacterial cases can be separated from the others. One such possibility might be to use GASMAS to monitor the oxygen content in the sinus cavity and behind the ear drum. If a sinus cavity has a substantial content of oxygen there is a high probability that there is no bacterial infection. In the case of the small children with middle air infection there may be the same conditions regarding oxygen variation.
2.3 Respiratory Distress Syndrome and Necrotizing Enterocolitis in Pre-term Infants
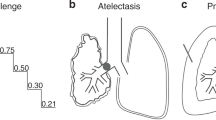
Another clinical specialty, where complementary techniques are needed is in neonatology for the preterm delivered infants. These children, born before gestation week 37 [40, 41], have an increased risk to develop the Respiratory Distress Syndrome (RDS) associated with immature organs [42, 43]. The lungs are not fully developed with surfactant lining in the alveoli. This leads to inhomogeneous lung function with partly fluid filled areas restricting the lung function. The most vulnerable organ that is at risk for damage is the brain. The therapy given to the small babies consists of artificial surfactant and continuous positive airway pressure support in an effort to keep the alveoli open and air filled. The follow-up of the treatment is X-ray based imaging and blood gases laboratory tests, the latter for a global measure of the oxygen saturation conditions. It is quite clear that efforts should be made to avoid ionizing radiation to the small babies, in particular knowing that the risk of developing a malignancy later in life is 10–15 times higher than for a 50-year old person exposed to the same dose [44]. With GASMAS there is a possibility to develop equipment which could provide a potential 24-h surveillance to follow the lung function, spatially resolved over the lung areas, and to provide instantaneous evaluation of the effectiveness of given treatment.
Pre-term children are also frequently subject to necrotizing enterocolitis (NEC), an acute inflammatory condition where part of the intestine becomes necrotic with risk of perforation [45–47]. Clearly, NEC is a very dangerous disease. The incidence ranges from 1 to 8 %, with the majority of all cases occurring for preterm children. NEC is a condition accompanied by strong gas release, making it a candidate for monitoring using GASMAS.
3 Basic Principles of Gas in Scattering Media Absorption Spectroscopy (GASMAS)
Many natural and man-made materials are porous, i.e. enclosures of gas are incorporated in the solid matrix material. Wood, polystyrene foam, ceramics, pharmaceutical preparations, fruits and other food stuffs come to mind. Pores are frequently small, on the micro- or even nanometer scale. When light propagates through a porous medium, it scatters at the interfaces where there is a step change in the index of refraction. If pores are abundant, multiple scattering occurs leading to a random walk for the photons. Clearly, propagation is only possible if the bulk material is reasonably transparent to light of the wavelength employed. The situation has similarities to the one encountered in atmospheric lidar (light detection and ranging) studies, where the light propagates in air, but encounters scattering aerosol particles [8]. If particles are abundant (like in clouds) multiple scattering occurs. In the DIAL (differential absorption lidar) variety, minor gas constituents, such as pollutants, are probed by changing the tuneable laser wavelength to sense the spectral imprint of the gas [48]. Reversely, in GASMAS, the gas inside the scattering pores is instead sensed. In both cases the fast spectral response for the gas imprint contrasted to the slow spectral variation due to the scattering particles is critically utilized. The situation for the two cases is schematically depicted in Fig. 1a and b, where (a) shows the multiple scattering lidar case (scattering particles in air) and (b) shows the GASMAS case, with scattering pores in a bulk material. Figure 1b shows a back-scattering GASMAS case whereas Fig. 1c depicts the GASMAS case for transillumination. Finally, Fig. 1d shows a GASMAS case, where a large cavity is surrounded by strongly scattering bulk material, such as in the case of a human sinus cavity. The lower part of the figure shows the intensity of the injected tuneable light as a function of wavelength (left), and the transmission spectrum after light diffusion through the scattering medium, with a very sharp free gas imprint (line-width around 10−3 nm or few GHz) superimposed on the slowly varying bulk material absorption spectrum.

Principles of GASMAS. a The multiple-scattering lidar case, with aerosol particles in air causing scattering; b the GASMAS case, where gas-filled pores in the bulk material cause scattering; back-scattering geometry; c same as case b, but signal observed in transillumination (transmission); d the GASMAS case with a single, large gas-filled cavity, surrounded by scattering material. Lower left shows the laser output as a function of wavelength; lower right shows the recorded spectrum after passage of the sample—a broad spectral undulation due to the slow frequency response of the bulk condensed matter material, and a super-imposed very sharp spectral imprint due to light passage through free gas
Since only weak light emerges diffusely from the sample, a large area photodiode or a photomultiplier tube, placed in close contact with the sample is used for the detection. Most frequently a tuneable diode laser with few mW output power is used as a light source, and the light is transported to the sample fibre-optically, to avoid signal contributions from the ambient air around the sample. Typical gases to be monitored are molecular oxygen, water vapour and carbon dioxide, with absorption bands, e.g. around 760, 935 and 2050 nm, respectively. Even if the effective path-length through gas is enhanced by the multiple scattering, the fractional gas imprint is frequently only of the order one per mile, since the NIR transitions used are quite weak or partly forbidden. This calls for the use of sensitive detection techniques, most frequently based on digital phase-sensitive (lock-in) detection. The diode laser is scanned by a current ramp, on which a fast sinusoidal modulation current is superimposed to sensitively detect the sudden strong slope of the sharp gas absorption imprint as a modulation in the detected light. The second harmonic of the signal is frequently monitored, since it is void of an off-set due to the ramped output power accompanying the laser output frequency scan. Experimental arrangements for GASMAS are presented, e.g. in [49–51]. By using individual modulation frequencies, the output of two diode lasers can be multiplexed and the emerging light from the sample can be collected by the same detector and de-multiplexed to yield data for two gases simultaneously. Problems with residual interference fringes in the detected signals can be handled by vibrating optical components and reference recording as discussed, e.g. in [52].
The absorptive imprint in light passing a gas is determined by the product of the gas concentration and the optical pathlength through the gas, as described by the Beer-Lambert law (see, e.g. Ref. [53]). It is highly desirable to determine the gas concentration in GASMAS measurements, but this is not straight forward because of the undefined optical pathlength through the scattering medium with a distribution of short and long pathlengths [49]. A convenient way to express the result of a GASMAS measurement is then to give the equivalent path-length Leq in a reference gas, normally ambient air, which would give rise to the same fractional absorptive imprint as recorded through the sample. A concentration determination would then require an independent measurement of the effective pathlength through the gas-containing pores. This can be achieved for the case of molecular oxygen by simultaneously measuring the signal from water vapour. When the air is saturated with water vapour (100 % humidity) the concentration of the gas is only determined by the temperature according to the Arden-Buck equation [54]. Since there is a wavelength difference between the absorption wavelengths for oxygen and water vapour, the procedure is only approximatively correct. The total effective pathlength through the medium, which is related to the pathlength through the gas alone can be measured with time-of-flight methods using pulsed lasers and single-photon correlation, or by the phase-shift method, employing swiftly modulated CW laser sources. Such approaches have been explored extensively as recently reviewed in [55]. An independent method, where gas concentrations can be determined without any knowledge of pathlength was recently introduced. Here the detailed absorption line shape, which depends on the collision partners and their concentrations, is analyzed [56].
Before discussing the medical diagnostics possibilities of GASMAS we will briefly mention other fields of application. Polystyrene foam was the first material studied by GASMAS [13, 49]. It is both highly porous and translucent and ideally suited for these types of studies. Wood has similar properties, although the material is highly anisotropic [57]. Wood was also used in studies of drying processes using GASMAS [58]. The technique has also been explored as a candidate for studies of archeological wood, such as water-logged material from historical ships [59, 60]. Many types of ceramics are translucent and have been studied by GASMAS, both with regard to pore-size assessment based on modification of the measured lineshapes due to frequent wall collisions in nano-porous materials [61–64] and as alignment-free multi-pass cells taking advantage of the path-length enhancement due to massive multiple scattering [65, 66]. Pharmaceutical tablets are of special interest to study with regards to porosity, controlled release etc. [67–69]. Fruits are also strongly porous and have been studied with regard to gas content and gas exchange [70–72], also related to the maturation and ripening processes [73]. Fruit storage in controlled atmosphere is a field of considerable interest (see, e.g. [74, 75]. The GASMAS technique is also very suitable for non-intrusive measurements on food packages and food-stuffs [76–78]. Modified atmosphere packaging (MAP) is widely applied [79, 80], and there is a great need to control the integrity of packages directly following processing, but also the current status of products on the shelf.
After this presentation of the principles of GASMAS and a brief review of non-medical applications we will now discuss specific applications to human sinus cavity monitoring, ear-infection diagnostics and neonatal children health care. A recent review paper discusses certain aspects of GASMAS studies on human subjects [16].
4 Monitoring of Paranasal Sinuses
The most easily accessible sinus cavities for optical probing are the maxillary and the frontal sinuses. Also the mastoideus bone, behind the outer ear, is readily accessible. A pure back-scattering measurement geometry, as indicated in Fig. 2a, is possible as demonstrated in our first study [81], which also was based on extensive measurements on scattering tissue phantoms. Backscattering yields weak gas signals since most of the light returns from the frontal bone structure without penetrating into the cavity. Better signals are obtained by injecting the light upwards from the upper part of the orbita and placing the detector towards the forehead. The maxillary sinuses can be probed from the outside in a similar way, with the injection and detection points separated by few centimeters and being on opposite sides of the cheek bone. A measurement scenario in shown in Fig. 3. By instead propagating the light from the inside of the mouth cavity and detecting the emerging scattered light on the cheek bone, the probability of detected photons having passed through the cavity is maximized leading to the highest signals received. Monte-Carlo simulations of photon propagation through sinuses surrounded by tissue provide understanding of the observations [82].

a Illustration of optical monitoring of gas in the frontal sinuses (MRI image of the last name author) b schematic diagram of the outer, middle and inner ear, with eardrum and Eustachian tube indicated (from Ref. [83])

GASMAS monitoring of sinus cavities (left) and of new-born baby lung (right). In both cases separated probes for the injection of narrow-band spectroscopic light and for detection of the weak light emerging from the tissue are employed
As an example, signals for maxillary sinuses in a patient with sinus problems (Fig. 4a) are compared with signals from a healthy volunteer in Fig. 4b. The partly blocked sinus yields a distinct oxygen signal, while the fully blocked sinus is characterized by the total absence of such a signal. The healthy volunteer presents with good signals in both sides [84]. A number of healthy volunteers were studied with regards to oxygen as well as water vapour, the best geometries were explored, and normalization of the oxygen signal on the water vapour signal (which reflects the size of the cavity) was demonstrated [85]. The encouraging results formed the basis for a clinical trial on patients remitted for skull CT imaging because of sinusitis problems. For 40 patients the frontal and the maxillary sinuses were also studied with GASMAS. Comparing the gas monitoring results with the CT evaluation of sinus status it was found that the sensitivity and specificity of the new method was to 93 and 61 %, and 94 and 86 % for the maxillary and frontal sinuses, respectively [86].

a MRI image of a patient with one maxillary sinus open and gas-filled while the other one is filled with liquid, corresponding to the GASMAS recording of oxygen in b, left. As a comparison, recordings for a volunteer with both maxillary cavities gas-filled is shown to the right (From [84]). c MRI image of a volunteer showing the mastoideus structures behind the ears. d GASMAS recording of oxygen gas in the mastoideus of a volunteer [88]
One interesting mode of measurements is to compare the recorded GASMAS signals for a particular patient with the historical values. Frequently, sinus problems are recurrent for certain patients. Clearly, it is important that the base-line values for a healthy patient are stable and reproducible. This has actually been demonstrated in a recent study [87].
Data for the mastoideus were also recorded for a number of patients. Figure 4c shows a transverse image at the level of the mastoideus—clear oxygen signals can be recorded as evidenced in Fig. 4d. Data from 31 mastoids showed, that the water vapour signal correlated with the size of the mastoideus with its porous structure [88].
We have found that it is possible to effectively study the ventilation, or lack of ventilation of the paranasal cavities by constantly observing the oxygen signal while flushing the nose with pure nitrogen gas through one nostril, under normal breathing through the mouth [85]. This provides additional diagnostic information on the status of sinus problems, and also allows an objective evaluation of the efficiency of anti-congestion sprays.
5 Diagnostics of Otitis Media
Monitoring of the middle ear is performed through the ear drum with the measurement probe inserted through the auditory passage. Given the geometry of the organ, as schematically shown in Fig. 2b, measurements in back-scattering seems to be the only viable choice. Such a geometry always leads to the risk of a substantial part of the light detected not having passed through the underlying gas, as discussed in connection with Fig. 2a. However, since the ear-drum is quite thin the situation is more favourable than in the case of the frontal sinuses. A probe with a central fiber for light injection surrounded by 6 fibres at a small separation from the injection point was constructed and found functional. So far only measurements on a middle ear phantom have been performed [83]. The phantom was constructed from a fish swim bladder, which was surrounded with gelatine prepared with titanium oxide scattering powder to mimic human tissue. Oxygen as well as water vapour signals could be readily detected from the cavity, which was prepared with some water left inside. Measurements mimicking middle ear ventilation through the Eustachian tube were performed and are illustrated in Fig. 5. To illustrate gas transport, the cavity was first filled with either pure oxygen or pure nitrogen, and a small hole was then made to allow the gas to equilibrate to ambient conditions. We note, that the water vapour signal is not affected by the procedure; 100 % humidity is maintained all the time. This illustrates the usefulness of using water vapour for referencing to allow determination of oxygen concentrations.

GASMAS recordings of ventilation of a human middle-ear phantom, constructed from a fish swim bladder surrounded by scattering material, mimicking human tissue. Oxygen and water vapour behind the phantom membrane is clearly detected by an optical probe operating in back-scattering mode. a shows the return of the cavity oxygen signal to ambient conditions following a filling with pure oxygen gas, while b shows the same process following filling with pure nitrogen gas. c and d instead monitor the water vapor behind the membrane—it can be seen that the signal from the moist cavity (100 % humidity) is unaffected by the ventilation, and thus can be useful for oxygen signal normalization purposes (from [83])
Reflectance measurements of the ear-drum were also performed, as previously demonstrated in [89]. The reflectance spectrum recorded with a compact fibre-based spectrometer gives an objective recording of the ear-drum, with a much better estimate of, e.g. erythema than attainable with the naked eye. Hopefully, a combination of reflectance and GASMAS data can provide a sharp diagnostics of middle ear infection. Measurements on healthy volunteers as well as patients suffering from otitis are planned.
6 Monitoring of Neonatal Children
As for the two other applications just discussed, our work aiming at improved diagnostics for neonatal children started with phantom studies [90]. Phantoms were constructed from fresh boar lung, which was placed between slabs of gelatine prepared to have optical properties similar to those of human tissue. The size of the phantoms was chosen to correspond to premature infants of different age. Good signals from oxygen as well as water vapour were obtained in back-scattering as well as transmission geometry. Nitrogen flushing of the boar lung resulted in a zero oxygen signal, while the water vapour signal remained unaffected. Encouraged by these results a pilot study on three healthy new-born infants was performed a illustrated in Fig. 3b with the equipment shown in Fig. 6 [91]. These children had a weight ranging from 3.9 to 4.3 kg, and were thus much larger than the intended patient group. Still it was possible to record good signals from water vapour, in particular from partly gas-filled intestines. Lungs also exhibited a signal for this gas, although considerably weaker, because of the thicker layer of tissue covering the gas-bearing structures. Data are shown for the three infants in Fig. 7 [91].

Experimental set-up for simultaneous monitoring of oxygen and water vapour signals, as illustrated for the case of neonatal infant monitoring. Two individual diode lasers are employed to generate the wavelengths needed for detection of the two types of molecules. By tagging the laser outputs by two different modulation frequencies a single transmitting probe and a single detector could be used in the measurements (from [91])

Panels a–c show recordings of water vapour present in gas pockets in the intestines of three new-born children. Likewise, panels d–f show signals from the lungs (from [91])
It was not possible to observe any oxygen signal in this first study, related to the fact, that oxygen signals are inherently weaker than water vapour signals, and also because of the low output power of the available oxygen diode laser. No oxygen signal is expected anyway from the intestines, while the lungs of course should exhibit oxygen gas. An ongoing clinical study employing a higher power oxygen laser and pursued on a larger number of new-born healthy children shows good oxygen signals from the lungs [92]. The hope is that a device providing spatially resolved information from different lung lobes could be achieved.
It should be noted that normal colic in small children is frequently caused by excessive gas in the intestines [93, 94]. A low-cost device monitoring the presence of gas in the belly, as manifested by the water vapour signal, could help parents to administer the relevant medication, e.g. Minifom.
7 Conclusion and Outlook
While the study of free gas in the human body is still in an early stage of development the results obtained so far can be considered to be promising. Common infectious diseases and the associated over-prescription of antibiotics constitute an important sector of the health-care system, and the work presented can hopefully provide contributions to this complex. Pre-term infants constitute a very vulnerable group of patients needing intense and costly care, and their well-being causes a lot of anxiety to parents. Any improvements in the early care could also substantially reduce later complications, worry and associated costs. A simple device for identifying a cause of colic in healthy small children could also be of substantial interest.
In future, more advanced applications of in situ monitoring of free gas in human tissue might include the discrimination between viable and necrotic tumours, and the detection of onset of caput necrosis following hip interventions, etc. The detection of minute signals due to small gas pockets related to such conditions clearly require more sophisticated equipment and would be reserved for specialized clinics.
In view of the early findings and the perspectives of the techniques developed it seems that continued research efforts are well motivated.
References
T. Vo-Dinh (ed.), Biomedical Photonics Handbook (CRC Press, Boca Raton, Florida, 2003)
J.G. Fujimoto, D.L. Farkas, Biomedical Optical Imaging (Oxford University Press, Oxford, 2009)
J. Popp, V.V. Tuchin, A. Chiou, S.H. Heinemann, Eds, Handbook of Biophotonics, Volumes 1–3 (Wiley-VCH 2011)
D.A. Boas, C. Pitris, N. Ramanujam, Handbook of Biomedical Optics (CRC Press, 2011)
H. Jelinkova, Ed. Lasers for Medical Application (Woodhead Publishing, 2013)
S. Svanberg, Laser spectroscopy in medical diagnostics, Chap. 10 in [5], pp. 286–324
K. Svanberg, N. Bendsoe, Photodynamic therapy for human malignancies with superficial and interstitial illumination, Chap. 25 in [5], pp. 760–778
S. Svanberg, LIDAR, Chap. 13.3 in F. Träger, Ed., Springer Handbook of Lasers and Optics, 2nd Edition (Springer, Heidelberg 2012), p. 1146
M.R. McCurdy, Y. Bakhirkin, G. Wysocki, R. Lewicki, F.K. Tittel, Recent advances of laser-spectroscopy-based techniques for applications in breath analysis. J. Breath Res. 1, 014001/1-12 (2007)
C. Wang, P. Sahay, Breath analysis using laser spectroscopic techniques: breath biomarkers, spectral fingerprints, and detection limits. Sensors 9, 8230 (2009)
S.M. Cristescu, S.T. Persijn, S. te Lintel Hekkert, F.J.M. Harren, Laser-based systems for trace gas detection in life sciences. Appl. Phys. B 92, 343 (2008)
D.D. Arslanov, M. Spunei, J. Mandon, S.M. Cristescu, S.T. Persijn, F.J.M. Harren, Optical parametric oscillator based infrared spectroscopy for sensitive molecular gas sensing. Laser Photonics Rev. 7, 188 (2013)
M. Sjöholm, G. Somesfalean, J. Alnis, S. Andersson-Engels, S. Svanberg, Analysis of gas dispersed in scattering solids and liquids. Opt. Lett. 26, 16–18 (2001)
M. Andersson, R. Grönlund, L. Persson, M. Sjöholm, K. Svanberg, S. Svanberg, Laser spectroscopy of gas in scattering media at scales ranging from kilometers to millimeters. Laser Phys. 17, 893 (2007)
S. Svanberg, Analysis of trapped gas—Gas in scattering media absorption spectroscopy. Laser Phys. 20, 68 (2010)
S. Svanberg, Gas in scattering media absorption spectroscopy—from basic studies to medical applications. Lasers Photonics Rev. 7, 779 (2013)
R. Saiki, S. Scharf, F. Faloona, K. Mullis, G. Horn, H. Erlich et al., Enzymatic amplification of beta-globin genomic sequences and restriction analysis for diagnosis of sickle cell anemia. Science 230, 1350 (1985)
D. Fredricks, D. Relman, Application of polymerase chain reaction to the diagnosis of infectious diseases. Clin. Infect. Dis. 29, 475 (1999)
D.Y. Graham, J.T. Schwartz, G.D. Cain, F. Gyorkey, Prospective evaluation of biopsy number in the diagnosis of esophageal and gastric carcinoma. Gastroenterol. 82, 228 (1982)
H. Sue-Ling, I. Martin, J. Griffith, D.C. Ward, P. Quirke, M.F. Dixon, A.T. Axon, M.J. McMahon, D. Johnston, Early gastric cancer: 46 cases treated in one surgical department. Gut 33, 1318 (1992)
H. Amin, L. Gilmour, S. Graham, X. Paterson-Brown, J. Terrace, T.J. Crofts, Gastric adenocarcinoma missed at endoscopy. J. R. Coll. Surg. Edinb. 47, 681 (2002)
S. Svanberg, Tissue diagnostics using lasers, in Lasers in Medicine, Chap. 6, ed. by R.W. Waynant (CRC Press, Baton Rouge 2002) pp. 135–169
S. Andersson-Engels, K. Svanberg, S. Svanberg, Fluorescence imaging in medical diagnostics, Chap. 10 in [1], pp. 265–305
S. Fickweiler, R.C. Krieg, H.G. Stepp, F. Hofstaedter, R. Knuechel, 5-aminolevulinic acid (ALA) mediated photodynamic therapy of bladder cancer cell lines. Proc. SPIE 3563, 143 (1999)
W. Drexler, J.G. Fujimoto (eds.), Optical Coherence Tomography: Technology and Applications (Springer, 2008)
J.P. Payne, J.P. Severinghaus (eds.), Pulse Oximetry (Springer, Heidelberg, 1986)
P. Rolfe, In vivo near-infrared spectroscopy. Ann. Rev. Biomed. Eng. 2, 715 (2000)
E. Krite Svanberg, P. Wollmer, S. Andersson-Engels, J. Åkeson, Physiological influence of basic perturbations assessed by non-invasive optical techniques in humans. Appl. Physiol. Nutr. Metab. 36, 946 (2011)
C. Bachert, K. Hormann, R. Mosges, G. Rasp, H. Riechelmann, R. Muller, H. Luckhaupt, B.A. Stuck, C. Rudack, An update on the diagnosis and treatment of sinusitis and nasal polyposis. Allergy 58, 176 (2003)
W. Fokkens, V. Lund, J. Mullol, European position paper on rhinosinusitis and nasal polyps 2007. Rhinol. Suppl. 20, 1–136 (2007)
I. Brook, Microbiology of sinusitis. Proc. Am. Thorac. Soc. 8, 90 (2011)
G.H. McCracken, Treatment of acute otitis media in an era of increasing microbial resistance. Pediatr. Infect. Dis. J. 17, 576 (1998)
S.F. Dowell, J.C. Butler, S.G. Giebink et al., Acute otitis media: management and surveillance in an era of pneumococcal resistance—a report from the drug-resistant streptococcus pneumonia therapeutic working group. Pediatr. Infect. Dis. J. 18, 1 (1999)
H. Goossens, M. Ferech, R. van der Stichele, M. Elseviers, ESAC project group. Outpatient antibiotic use in Europe and association with resistance: a cross-national database study, Lancet 365, 579 (2005)
P. Lee, Chief consultant at the EurAm clinic (Guangzhou, China (private communication), 2014)
S. Maxson, T. Yamauchi, Acute otitis media. Pediatr. Rev. 17(6), 191–195 (1996)
K. Ramakrishnan, R.A. Sparks, W.E. Berryhill, Diagnosis and treatment of otitis media. Am. Fam. Physician 76, 1650 (2007)
A.S. Lieberthal, A.E. Carroll, T. Chonmaitree et al., The diagnosis and management of acute otitis media. Pediatrics 131, 964 (2013)
R.M. Rosenfeld, D. Kay, Natural history of untreated otitis media. Laryngoscope 113, 1645 (2003)
M.M. Slattery, J. Morrison, Preterm delivery. Lancet 360, 1489 (2002)
R.L. Goldenberg et al., Epidemiology and causes of preterm birth. Lancet 371, 75 (2008)
L.B. Ware, M.A. Matthay, Medical progress – The acute respiratory distress syndrome. New Engl. J. Med. 342, 1334 (2000)
D.G. Sweet et al., European consensus guidelines on the management of neonatal respiratory distress syndrome in preterm infants—2013 update. Neonatol. 103, 353 (2013)
E.J. Hall, Lessons we have learned from our children: cancer risks from diagnostic radiology. Pediatr. Radiol. 32, 700 (2002)
R.M. Kliegman, A.A. Fanaroff, Nectrotizing enterocolitis. New Engl. J. Med. 310, 1093 (1984)
A.M. Kosloske, Epidemiology of necrotizing enterocolitis. Acta Paediatr. Suppl. 396, 2 (1994)
J. Pietz, B. Achanti, L. Lilien, E. Clifford Stepka, S. Ken Mehta, Prevention of necrotitizing enterocolitis in preterm infants: a 20-year experience. Pediatrics 119, 164 (2006)
S. Svanberg, Differential absorption lidar (DIAL), in Air Monitoring by Spectroscopic Techniques, M. Sigrist (ed.), (Wiley, N.Y. 1994), p. 85
G. Somesfalean, M. Sjöholm, J. Alnis, C. af Klinteberg, S. Andersson-Engels, S. Svanberg, Concentration measurement of gas imbedded in scattering media employing time and spatially resolved techniques. Appl. Optics 41, 3538–3544 (2002)
L. Persson, M. Lewander, M. Andersson, K. Svanberg, S. Svanberg, Simultaneous detection of molecular oxygen and water vapor in the tissue optical window using tunable diode laser spectroscopy. Appl. Opt. 47, 2028 (2008)
M. Lewander, Z.G. Guan, K. Svanberg, S. Svanberg, T. Svensson, Clinical system for non-invasive in situ monitoring of gases in the human paranasal sinuses. Opt. Express 13, 10849 (2009)
L. Persson, M. Andersson, F. Andersson, S. Svanberg, Approach to optical interference fringe reduction in diode-laser-based absorption spectroscopy. Appl. Phys. B 87, 523 (2007)
S. Svanberg, Atomic and Molecular Spectroscopy—Basic Aspects and Practical Applications, 4th edn. (Springer, Heidelberg, 2004)
A.L. Buck, New equations for computing vapor pressure and enhancement factor. J. Appl. Meteorol. 20, 1527–1532 (1996)
L. Mei, G. Somesfalean, S. Svanberg, Pathlength determination for gas in scattering media absorption spectroscopy. Sensors 14, 3871 (2014)
P. Lundin, L. Mei, S. Andersson-Engels, S. Svanberg, Laser spectroscopic gas concentration measurements in situations with unknown optical path length enabled by absorption line shape analysis. Appl. Phys. Lett. 103, 034105 (2013)
J. Alnis, B. Anderson, M. Sjöholm, G. Somesfalean, S. Svanberg, Laser spectroscopy on free molecular oxygen dispersed in wood materials. Appl. Phys. B 77, 691 (2003)
M. Andersson, L. Persson, M. Sjöholm, S. Svanberg, Spectroscopic studies of wood-drying processes. Opt. Express 14, 3641 (2006)
M. Karlsson, P. Lundin, L. Cocola, G. Somesfalean, S. Svanberg, I. Bargigia, C. D´Andrea, A. Nevin, A. Farina, A. Pifferi, R. Cubeddu, M. Orlandi, Non-invasive optical diagnosis of gases in wood, Shipwrecks 2011, Ed. M. Ek, ISBN 978-91-7501-142-4 (Vasa Museum, Stockholm 2011) p. 176
I. Bargigia, A. Nevin, A. Farina, A. Pifferi, C. D’Andrea, M. Karlsson, P. Lundin, G. Somesfalean, S. Svanberg, Diffuse optical techniques applied to wood characterization. J. Near Infrared Spectr. 21, 259 (2013)
T. Svensson, Z. Shen, Laser spectroscopy of gas confined in nanoporous materials. Appl. Phys. Lett. 96, 021107 (2010)
T. Svensson, M. Lewander, S. Svanberg, Laser absorption spectroscopy of water vapor confined in nanoporous alumina: wall collision line broadening and gas diffusion dynamics. Opt. Express 18, 16460 (2010)
C.T. Xu, M. Lewander, S. Andersson-Engels, E. Adolfsson, T. Svensson, S. Svanberg, Wall collision line broadening at reduced pressures: towards non-destructive characterization of nanoporous materials. Phys. Rev. A 84, 042705 (2011)
T. Svensson, E. Adolfsson, M. Burresi, R. Savo, C.T. Xu, D.S. Wiersma, S. Svanberg, Pore size assessment by high-resolution laser spectroscopy of wall collision line broadening of confined gases: experiments of strongly scattering nanoporous zirconia ceramics with fine-tuned pore sizes, Appl. Phys. B. doi:10.1007/S00340-012-5011-s (2012)
T. Svensson, E. Adolfsson, M. Lewander, C.T. Xu, S. Svanberg, Disordered, strongly scattering porous materials as miniature multi-pass gas cells. Phys. Rev. Lett. 107, 143901 (2011)
X.T. Lou, C.T. Xu, S. Svanberg, G. Somesfalean, Multi-mode diode laser correlation spectroscopy using gas-filled porous materials for pathlength enhancement. Appl. Phys. B 109, 453 (2012)
T. Svensson, L. Persson, M. Andersson, S. Svanberg, S. Andersson-Engels, J. Johansson, S. Folestad, Noninvasive characterization of pharmaceutical solids by diode laser oxygen spectroscopy. Appl. Spectr. 61, 784 (2007)
T. Svensson, M. Andersson, L. Rippe, S. Svanberg, S. Andersson-Engels, J. Johansson, S. Folestad, VCSEL-based oxygen spectroscopy for structural analysis of pharmaceutical solids. Appl. Phys. B 90, 345 (2008)
T. Svensson, E. Alerstam, J. Johansson, Stefan Andersson-Engels, Optical porosimetry and investigations of the porosity experienced by light interacting with porous media. Opt. Lett. 35, 1740–1742 (2010)
L. Persson, B. Anderson, M. Andersson, M. Sjöholm, S. Svanberg, Studies of gas exchange in fruits using laser spectroscopic techniques, in Proceedings of the Fruitic 05, Information and Technology for Sustainable Fruit and Vegetable Production, 543–552, Montpellier (September 2005)
L. Persson, H. Gao, M. Sjöholm, S. Svanberg, Diode laser absorption spectroscopy for studies of gas exchange in fruits. Lasers Opt. Engineering 44, 687 (2006)
U. Tylewicz, P. Lundin, L. Cocola, P. Rocculi, S. Svanberg, P. Dejmek, F. Gόmez Galindo, Gas in scattering media absorption spectroscopy (GASMAS) detected persistent vacuum in apple tissue after vacuum impregnation, Food Biophys. 10, 1483-011-9239-7 (2011)
H. Zhang, J. Huang, T.Q. Li, X.X. Wu, S. Svanberg, K. Svanberg, Studies for tropical fruit ripening using three different spectroscopic techniques. J. Biomed. Opt. 19, 067001 (2014)
M.L.A.T.M. Hertog, H.W. Peppelenbos, R.G. Evelo, L.M.M. Tijskens, Postharvest. Technol. Biol. 14, 335 (1998)
R.M. Beaudry, Postharvest Biol. Technol. 15, 293 (1999)
M. Lewander, Z.G. Guan, L. Persson, A. Olsson, S. Svanberg, Food monitoring based on diode laser gas spectroscopy. Appl. Phys. B 93, 619 (2008)
P. Lundin, L. Cocola, A. Olsson, S. Svanberg, Non-intrusive headspace gas measurements by laser spectroscopy—Performance validated by an intrusive reference sensor, J. Food Eng. http://dx.doi.org/10.1016/j.jfoodeng.2012.03.008 (2012)
M. Lewander, T. Svensson, S. Svanberg, A. Olsson, Non intrusive measurements of food and packaging quality. Packag. Technol. Sci. 24, 271 (2011)
I.L. Church, A.L. Parsons, Modied atmosphere packaging technology—A review. J. Sci. Food Agri. 67, 143 (1995)
C.A. Phillips, Review: Modified atmosphere packaging and its effects on the microbiological quality and safety of produce. Int. J. Food Sci. & Technol. 31, 463 (1996)
L. Persson, K. Svanberg, S. Svanberg, On the potential for human sinus cavity diagnostics using diode laser gas spectroscopy. Appl. Phys. B 82, 313 (2006)
L. Persson, E. Kristensson, L. Simonsson, S. Svanberg, Monte Carlo simulations of optical human sinusitis diagnostics. J. Biomedical Optics 12, 054002 (2007)
H. Zhang, J. Huang, T.Q. Li, S. Svanberg, K. Svanberg, Optical detection of middle ear infection using spectroscopic techniques—Phantom experiments, J. Biomed. Opt., doi: 10.1117/.jbo (2015)
L. Persson, M. Andersson, T. Svensson, K. Svanberg, S. Svanberg, Non-intrusive optical study of gas and its exchange in human maxillary sinuses. SPIE 6628, 662804 (2007)
L. Persson, M. Andersson, M. Cassel-Engquist, K. Svanberg, S. Svanberg, Gas monitoring in human sinuses using tunable diode laser spectroscopy, J. Biomed. Opt. 12, (5) (2007)
M. Lewander, S. Lindberg, T. Svensson, R. Siemund, K. Svanberg, S. Svanberg, Clinical study assessing information on the maxillary and frontal sinuses using diode laser gas spectroscopy. Rhinology 50, 26 (2011)
J. Huang, H. Zhang, T.Q L.i, H.Y. Lin, K. Svanberg, S. Svanberg, Assessment of human sinus cavity air volume using tunable diode laser spectroscopy, with application to sinusitis diagnostics, to appear (2015)
S. Lindberg, M. Lewander, T. Svensson, R. Siemund, K. Svanberg, S. Svanberg, Method for studying gas composition in the human mastoid cavity by use of laser spectroscopy, Annals of Otology, Rhinol. Laryngol. 121 (2012)
M. Sundberg, M. Peebo, P.A. Öberg, P.G. Lundquist, T. Strömberg, Diffuse reflectance spectroscopy of the human tympanic membrane in otitis media. Physiol. Meas. 25, 1473 (2004)
M. Lewander, A. Bruzelius, S. Svanberg, K. Svanberg, V. Fellman, Non-intrusive gas monitoring in neonatal lungs using diode laser spectroscopy: feasibility study. J. Biomed. Opt. 16, 127002 (2011)
P. Lundin, E. Krite Svanberg, L. Cocola, M. Lewander Xu, G. Somesfalean, S. Andersson-Engels, J. Jahr, V. Fellman, K. Svanberg, S. Svanberg, Non-invasive monitoring of gas in the lungs and intestines of newborn infants using diode lasers: feasibility study. J. Biomed. Opt. 18, 127005 (2013)
E. Krite Svanberg, P. Lundin et al., to appear
A. Morris, J.C. Wessel, E.B. Cobb, G.S. Jackson, J.R. Harrisand, A.C. Detwiler, Paroxysmal fussing in infancy, sometimes called colic. Pediatrics 14, 421 (1954)
D.W. Hide, B.M. Guyer, Prevalence of infant colic. Arch. Dis. Child. 57, 559 (1982)
Acknowledgments
The authors are grateful to a large number of colleagues and graduate students who collaborated in the development of biomedical applications of Gas in scattering media absorption spectroscopy. These persons include Mats Andersson, Stefan Andersson-Engels, L. Cocola, Vineta Fellman, Zuguang Guan, Jing Huang, Kjell Jonson, Emilie Krite Svanberg, Märta Lewander, Tianqi Li, Liang Mei, Sven Lindberg, Patrik Lundin, Linda Persson, Roger Siemund, Gabriel Somesfalean, Tomas Svensson, and Hao Zhang. The work was supported by the Swedish Research Council (VR), through a direct grant and a Linnaeus grant to the Lund Laser Centre, by the Lund University Medical Faculty, the Knut and Alice Wallenberg Foundation, and by the Guangdong Province Innovation Research Team Program (No. 201001D0104799318).
Author information
Authors and Affiliations
Corresponding authors
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer Science+Business Media Singapore
About this chapter
Cite this chapter
Svanberg, K., Svanberg, S. (2016). Monitoring Free Gas In Situ for Medical Diagnostics Using Laser Spectroscopic Techniques. In: Olivo, M., Dinish, U. (eds) Frontiers in Biophotonics for Translational Medicine. Progress in Optical Science and Photonics, vol 3. Springer, Singapore. https://doi.org/10.1007/978-981-287-627-0_10
Download citation
DOI: https://doi.org/10.1007/978-981-287-627-0_10
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-287-626-3
Online ISBN: 978-981-287-627-0
eBook Packages: EngineeringEngineering (R0)