
Abstract
Pigmented villonodular synovitis (PVNS), also known as giant cell tumor in the joint, is a special synovial disease that is mostly diffuse and sometimes localized, much like a tumor [1]. The etiology of pigmented villonodular synovitis is unknown, but monoclonal evidence suggests that it is a tumor-derived disease. It can occur in young or old patients and the symptoms are caused by massed in the joint. The knee joint is the most likely joint to be involved, as well as the shoulder, elbow, hip, and ankle. The manifestation of poly articular involvement has also been reported in some cases. Typical symptoms are joint pain, swelling, and repeated effusion, with not necessarily a history of trauma, due to synovial bleeding and inflammation within the joint. It often presents as a knee locking, sometimes misdiagnosed as a popliteal cyst. Pigmented villonodular synovitis can cause bone erosion, the formation of bone cysts or collapse.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Principles of Treatment of Villonodular Synovitis
Pigmented villonodular synovitis (PVNS), also known as giant cell tumor in the joint, is a special synovial disease that is mostly diffuse and sometimes localized, much like a tumor [1]. The etiology of pigmented villonodular synovitis is unknown, but monoclonal evidence suggests that it is a tumor-derived disease. It can occur in young or old patients and the symptoms are caused by masses in the joint. The knee joint is the most likely joint to be involved, as well as the shoulder, elbow, hip, and ankle. The manifestation of poly articular involvement has also been reported in some cases. Typical symptoms are joint pain, swelling, and repeated effusion, with not necessarily a history of trauma, due to synovial bleeding and inflammation within the joint. It often presents as a knee locking, sometimes misdiagnosed as a popliteal cyst. Pigmented villonodular synovitis can cause bone erosion, the formation of bone cysts or collapse.
In general, PVNS presents synovial villous hyperplasia or nodular changes, and different patients may be dominated by villous morphology or nodular morphology. The synovial lesion shows “stool” change in color, with yellow, brown, and black color interlacing. Under arthroscopy, the typical change is to have purplish black vascular shadows within the brownish yellow villi. Histologically, PVNS is like giant cell tumor of the tendon sheath. The lesion showed round synovial-like cell proliferation, with inflammatory cells scattered in the middle, and sometimes osteoclast-type multinucleated giant cells, xanthoma cells, and so on.
Surgical resection is the best treatment for localized PVNS, with postoperative recurrence rate of 0–15% [2, 3]. Localized lumps can be removed arthroscopically. Arthroscopic surgery is less advantageous than open surgery to treat localized PVNS. Because the diseased tissue is removed by nibbling under arthroscopy, it is easy to cause the implantation and diffusion of the diseased tissue. Although the open resection is slightly more invasive, the overall removal of the mass has a significant benefit in preventing recurrence.
There is no fundamental treatment for diffused PVNS. Current treatments include surgical excision, cryotherapy, in vitro radiotherapy, radionuclide synovectomy (internal radiation therapy), immunotherapy, and targeted therapy, but none of these methods can ensure the removal of all diseased cells, so recurrence cannot be avoided. At present, the commonly used treatment is still surgical resection. The purpose of intraoperative freezing therapy is to destroy the diseased tissues, but it may cause necrosis of normal tissues, cartilage damage, transient nerve paralysis, etc., mainly because the freezing depth and range are not easy to control. External tubular radiotherapy may cause skin reaction, joint stiffness, poor wound healing, malignant transformation of tumor and even fracture. It should only be used as an auxiliary measure and should be used with caution for young people [4]. Radioactive synovectomy is the injection of radioactive material into the joint to destroy the diseased tissue, but collateral damage to normal tissue is inevitable and, in some cases, can lead to serious complications of articular cartilage, bone, and soft tissue. The effectiveness of immunotherapy has not been demonstrated in much clinical practice. Because of the tumor origin of PVNS, targeted therapy has been attempted, but the effectiveness and harm of this treatment need to be further explored. If the bone in the joint is severely damaged, joint replacement can be performed. However, joint replacement alone does not treat PVNS. Although synovial resection is performed during joint replacement, recurrence is inevitable and can result in premature failure of the prosthesis.
It is difficult to determine whether open or arthroscopic surgery is superior to the other for synovium resection [5, 6]. With both methods, the recurrence rate of diffuse cases ranged from 8% to 50%. The benefits of arthroscopic surgery are faster recovery and the avoidance of trauma of open surgery [7, 8]. The disadvantages are that the lesions are cleaned and excised in the middle, which may lead to the diffusion of localized lesions and implantation at surgical approaches, and the extra-articular lesion cannot be excised. In the case of exceptionally large lesion volume, especially nodular lesion, arthroscopic resection is inefficient or even impossible in terms of time.
The advantage of open surgery is that a large or whole lesion can be removed, which can save operation time. It has been reported that arthrotomy combined with cryotherapy can achieve good results. However, it is still quite challenging to thoroughly remove the synovium in the posterior compartment of the knee through the popliteal approaches. If the range of motion exercises cannot be carried out immediately after the operation, joint adhesion will cause dysfunction.
There is no prospective study to compare these techniques because the number of cases each surgeon receives is limited. In addition, these two surgical methods have corresponding indications, so it is impossible to only perform intra-articular surgery for the study of patients with pathological tissue mass outside the joint [9]. In general, arthroscopic synovial excision is recommended if the lesion is confined to the joint. If there is diseased tissue mass outside the joint, especially in the popliteal fossa, the diseased tissue inside the joint should be cleaned under arthroscopy, followed by an additional popliteal incision to remove the extra-articular masses [10, 11]. Sometimes, the synovial tissue is seriously fibrotic, it is difficult to clear with an arthroscopic shaver, the joint needs to be cut open to do synovium excision within the joint.
We believe that the advantages of synovectomy under arthroscopy are mainly reflected in the removal of diseased tissue from the posterior compartments of the knee. It is one of the necessary methods to remove the diseased tissues outside the joint by posterior side incision of the knee joint. However, it is particularly difficult to remove the lesions in the posterior joint of the knee through this approach, mainly because of the deep location and the obstruction of the medial and lateral head of the gastrocnemius muscle and the neurovascular structures. However, arthroscopic resection of the posterior compartment of the knee by posteromedial and posterolateral approaches is easy and thorough. The anterior lesions of the knee rarely spread beyond the joint, and arthroscopic resection has the advantage of minimally invasive; however, for synovitis mainly with nodular degeneration, the efficiency of arthroscopic resection is very low, so limited joint resection is recommended.
Preoperative Preparation
Patients with PVNS present with joint hemorrhage or effusion after minor trauma. Localized lesions often present with articular interlock, and both types cause limited range of motion. It is generally difficult to palpate a mass unless there is an invasion outside the joint. Extra-articular invasion occurs in the popliteal fossa. In severe cases, severe degenerative joint disease may occur.
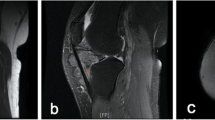
In the early stage of PVNS, no positive findings can be found by plain radiography. Some patients may find floating patella due to joint effusion. In severe cases, cystic changes may occur in the bone surrounding the cartilage. On MRI, PVNS is characteristic. On T1 and T2 weighted images, distinct soft tissue mass shadows with high and low signals can be observed, except in severe rheumatoid arthritis, where this unique MRI appearance is characteristic of PVNS and is due to the interlaced distribution of proliferative tissue with fluid and fat. The lesion is not confined to the joint but occurs between and outside the joint capsular fibers. An MRI examination must be performed before surgery to help make a clear diagnosis and make a surgical plan.
Surgical Procedures of Arthroscopic Synovectomy for Diffused PVNS of the Knee
It is more difficult to perform subtotal synovial resection for PVNS under arthroscopy than general arthroscopic surgery because the increase in biological tamping affects the field of vision. In addition, the removal of nodular tissue by shaver is inefficient. The operation requires a tourniquet, which requires a combination of anteromedial, anterolateral, supralateral patellar, posteromedial, posterolateral, and other arthroscopic approaches, and requires a posterior septum resection.
Clearing the Anterior Compartment and the Medial and Lateral Joint Space
The shaver is inserted alternately through the high anterolateral and anteromedial approaches to clear the intercondylar notch and the synovium tissue on the surface of the anterior and posterior cruciate ligaments and the most anterior part of the posterior septum are removed (Fig. 8.1).

The anterior compartment and the femoral notch are derided (Arthroscopic view of the left knee through the anterolateral portal). MFC medial femoral condyle, LFC lateral femoral condyle, ACL anterior cruciate ligament, PCL posterior cruciate ligament
All diseased synovial tissues in the anterior compartment, medial and lateral joint spaces of the knee are excised, including the site under the meniscus, especially the lateral meniscus (Fig. 8.2).

Photos indicting the diseased tissue under the medial meniscus (a) (Arthroscopic view of the medial compartment of the left knee through the anterolateral portal) and that under the lateral meniscus being removed (b) (Arthroscopic view of the lateral compartment of the left knee through the anteromedial portal). MFC medial femoral condyle, LFC lateral femoral condyle, MTC medial tibial condyle, LTC lateral tibial condyle, MM medial meniscus, LM lateral meniscus
Preliminary Debridement in Posteromedial Compartment
The knee is flexed at 60°, the arthroscope is inserted from the high anterolateral portal, through the space between the medial femoral condyle and the posterior cruciate ligament, to the posteromedial compartment. The knee is flexed further to more than 90° to expand the posteromedial compartment. Under arthroscopic observation, the standard posteromedial portal is created at the posteromedial corner of the knee, 1 cm above the joint line.
A shaver is inserted through the posteromedial portal to carry out preliminary debridement in the posteromedial compartment (Fig. 8.3), including the medial side of the posterior septum. The resection depth on the posterior wall of the posteromedial compartment should be controlled. The diseased synovial layer should be removed, and the fibrous layer of the joint capsule should be retained, to avoid nerve and blood vessel damage caused by too deep resecting. Visual blind areas such as the top, bottom, and inner corners of the posteromedial compartment are not cleaned for the time being.

Preliminary debridement in the posteromedial compartment (arthroscopic views and illustration of the posteromedial compartment of the left knee through the anterolateral portal). (a) Condition before the debridement. (b) Condition after debridement. (c) Illustration of the positions of the arthroscope and the instrument
Preliminary Debridement of the Posterolateral Compartment
The arthroscope is placed into the posteromedial compartment. The center of the medial side of the posterior septum is located and pressed against with the arthroscope. With the trocar in place, the arthroscope is replaced with the obturator. Then the set of trocar and obturator is passed through the posterior septum to the posterolateral compartment. The arthroscope is placed in to replace the obturator, namely to the posterolateral compartment through the posteromedial portal, posteromedial compartment, and the posterior septum. The posterolateral portal is created under observation. A shaver is placed in through the posterolateral approach for preliminary debridement (Fig. 8.4).

Preliminary debridement in the posterolateral compartment (arthroscopic views of the posterolateral compartment of the left knee through the posteromedial portal and the posterior septum). (a) Condition before the debridement. (b) Condition after debridement. LFC lateral femoral condyle
Removal of the Posterior Septum
The arthroscope is drawn back to the posteromedial compartment, and the shaver that has been inserted into the posterolateral compartment is inserted into the perforated part of the posterior septum following the arthroscope. The posterior septum is resected, including the synovium on the inner and outer surfaces and the fibrous adipose layer between them (Fig. 8.5).

Preliminary resection of the posterior septum (arthroscopic views and illustration of the posteromedial compartment of left knee through the posteromedial portal). (a) Condition before the removal of the posterior septum. (b) Condition after the removal of the posterior septum. (c) Illustration of the positions of the arthroscope and the instrument. MFC medial femoral condyle, LFC lateral femoral condyle, PS posterior septum
There is a small artery from outside the joint at the upper margin of the posterior septum. It should be cutoff and coagulated during the operation to avoid intractable hematoma. The posterior margin of the posterior septum is close to the popliteal articular structure, so attention should be paid to controlling the depth of synovectomy to avoid damage.
Complete Debridement in the Posterior Compartments
After removal of the posterior septum, the posteromedial and posterolateral compartments are connected. There is no blind area in the posterior compartments of the knee, which is convenient for further debridement operation. With arthroscopic monitoring alternately through the posteromedial and the posterolateral portals, the synovium of the posterior compartments is thoroughly removed, including the synovium excision at the top and bottom of the posterior compartments, as well as at the junction of the meniscus body and the posterior horn and other areas in the blind area of the conventional arthroscopic approaches.
Debridement of the Posterior Outlet of the Femoral Notch
The posterior outlet of the femoral notch can be divided into three parts: the space between the PCL and medial femoral condyle (Fig. 8.6), that between the ACL and the PCL (Fig. 8.7), and that between the ACL and the lateral femoral condyle (Fig. 8.8). The arthroscope is placed in for monitoring through the posterolateral portal, and the shaver is inserted through the anteromedial portal, and the synovium debridement is carried out at the three parts of the posterior outlet of the femoral notch, respectively.

Debridement between the posterior cruciate ligament and the medial femoral condyle at the posterior outlet (left knee). (a) Illustration of the position of the arthroscope and the to be debrided space. (b) Arthroscopic view of the posterior compartments of the left knee through the posterolateral portal. PS posterior septum, MFC medial femoral condyle, LFC lateral femoral condyle, PCL posterior cruciate ligament, MM medial meniscus

Debridement between the posterior and the anterior cruciate ligaments at the posterior outlet (left knee). (a) Illustration of the position of the arthroscope and the to be debrided space. (b) Arthroscopic view of the posterior compartments of the left knee through the posterolateral portal. PS posterior septum, MFC medial femoral condyle, LFC lateral femoral condyle, PCL posterior cruciate ligament, MM medial meniscus

Debridement between the anterior cruciate ligaments and the lateral femoral condyle at the posterior outlet (left knee). (a) Illustration of the position of the arthroscope and the to be debrided space. (b) Arthroscopic view of the posterior compartments of the left knee through the posterolateral portal. PS posterior septum, MFC medial femoral condyle, LFC lateral femoral condyle, PCL posterior cruciate ligament, MM medial meniscus
Debridement of the Medial and Lateral Gutter and Suprapatellar Pouch
The knee is changed into extension position, the arthroscope is inserted from the high anterolateral portal, the instruments are placed in from the anteromedial portal, and the medial gutter is debrided.
The supralateral patellar portal is created under monitoring, and the instruments are inserted through. Synovectomy in the lateral gutter is performed first and then in the supra patellar pouch. For patients with excessive suprapatellar pouch, an additional proximal supralateral patellar portal should be adopted, which is closer to the site than the standard supralateral patellar portal, to perform total synovial resection.
Thorough synovial debridement often results in the separation of the meniscus from nearby tissue, especially the lateral meniscus from the joint capsule. For posterior horn separation, the meniscus and the joint capsule are closed by all inside repair. For the separation of body and anterior horn from the capsule, the meniscus is reduced and sutured in an inside to outside or outside-in manner.
During the synovectomy, electrocoagulation and hemostasis are performed on the obvious bleeding sites. Drainage is placed in the posterior compartments and suprapatellar bursa respectively, and the incision is closed. For the relevant extra-articular lesions, the final excision is performed through open procedure. The affected limb is fully bandaged with an elastic bandage.
Postoperative Rehabilitation
Drainage is removed 2 days after synovial resection under arthroscopy. The affected limb is bandaged with elastic bandage for 7 days after the operation, and the quadriceps muscle isometric contraction and straight leg raising training are performed immediately. Knee range of motion training is started one week after the operation. Knee range of motion is required to reach 90 degrees at 4 weeks after the operation and 120 degrees at 6 weeks after the operation. The patients with limited knee flexion are given manual release within 3 months after the operation. Pearls and pitfalls of arthroscopic synovectomy for diffused PVNS of the knee are listed in Table 8.1.
References
Fałek A, Niemunis-Sawicka J, Wrona K, Szczypiór G, Rzepecka-Wejs L, Cięszczyk K, Burdan M, Puderecki M, Burzec P, Marzec-Kotarska B, Szumiło J, Burdan F. Pigmented villonodular synovitis. Folia Med Cracov. 2018;58(4):93–104.
Matar HE, Acharya A. Localized pigmented Villonodular synovitis of the knee: outcomes of arthroscopic synovectomy. J Long-Term Eff Med Implants. 2019;29(2):101–4.
Simonetta R, Florio M, Familiari F, Gasparini G, Rosa MA. All-arthroscopic treatment of intra- and extra-articular localized Villonodular synovitis of knee. Joints. 2017;5(3):184–7.
Duan Y, Qian J, Chen K, Zhang Z. Necessity of adjuvant postoperative radiotherapy for diffuse pigmented villonodular synovitis of the knee: a case report and literature review. Medicine (Baltimore). 2018;97(3):e9637.
Quaresma MB, Portela J, Soares do Brito J. Open versus arthroscopic surgery for diffuse tenosynovial giant-cell tumours of the knee: a systematic review. EFORT Open Rev. 2020;5(6):339–46.
Noailles T, Brulefert K, Briand S, Longis PM, Andrieu K, Chalopin A, Gouin F. Giant cell tumor of tendon sheath: open surgery or arthroscopic synovectomy? A systematic review of the literature. Orthop Traumatol Surg Res. 2017;103(5):809–14.
Keyhani S, Kazemi SM, Ahn JH, Verdonk R, Soleymanha M. Arthroscopic treatment of diffuse pigmented Villonodular synovitis of the knee: complete synovectomy and septum removal-midterm results. J Knee Surg. 2019;32(5):427–33.
Chang JS, Higgins JP, Kosy JD, Theodoropoulos J. Systematic arthroscopic treatment of diffuse pigmented Villonodular synovitis in the knee. Arthrosc Tech. 2017;6(5):e1547–51.
Kim DE, Kim JM, Lee BS, Kim NK, Lee SH, Bin SI. Distinct extra-articular invasion patterns of diffuse pigmented villonodular synovitis/tenosynovial giant cell tumor in the knee joints. Knee Surg Sports Traumatol Arthrosc. 2018;26(11):3508–14.
Georgiannos D, Boutsiadis A, Agathangelidis F, Papastergiou S, Karataglis D, Bisbinas I. Arthroscopically-assisted mini open partial synovectomy for the treatment of localized pigmented villonodular synovitis of the knee. A retrospective comparative study with long-term follow up. Int Orthop. 2017;41(5):925–30.
Mollon B, Griffin AM, Ferguson PC, Wunder JS, Theodoropoulos J. Combined arthroscopic and open synovectomy for diffuse pigmented villonodular synovitis of the knee. Knee Surg Sports Traumatol Arthrosc. 2016;24(1):260–6.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 Henan Science and Technology Press
About this chapter

Cite this chapter
Zhao, J. (2022). Arthroscopic Treatment of Pigmented Villonodular Synovitis of the Knee. In: Zhao, J. (eds) Minimally Invasive Functional Reconstruction of the Knee. Springer, Singapore. https://doi.org/10.1007/978-981-19-3971-6_8
Download citation
DOI: https://doi.org/10.1007/978-981-19-3971-6_8
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-19-3970-9
Online ISBN: 978-981-19-3971-6
eBook Packages: MedicineMedicine (R0)