
Abstract
The temporal bone is a highly complex anatomical area affected by a heterogeneous group of diseases, mostly benign. Audiovestibular symptoms and facial paralysis are the most frequent clinical manifestations. Tools to study these patients include audiology tests, vestibular tests, and imaging studies. This chapter focuses on the anatomical landmarks useful to perform the most frequent temporal bone procedures, from a mastoidectomy to an infratemporal fossa approach. Endoscopic anatomy is also reviewed. Hearing loss, CSF leak, vestibular dysfunction, and facial nerve lesion are complications of these approaches. A multidisciplinary team including an ENT surgeon, a neurosurgeon, a neurophysiologist, and a head and neck surgeon is recommended to perform the most complex procedures.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
16.1 Introduction
To fully understand the three-dimensional anatomy of the temporal bone is one of the most challenging tasks a head and neck surgeon faces. The temporal bone also stands out for the variety of pathology affecting it. It is merely impossible to discuss extensively all the diseases and tumours affecting this anatomical region and their surgical management in a single book chapter. This chapter intends to help the reader comprehend the most common surgical approaches to treat the diseases and tumours that affect the lateral skull base more frequently.
It is important to mention that these approaches are largely designed for adult patients because such lesions are more common in this population. Nevertheless, the development of cochlear implants has radically increased the number of young children undergoing temporal bone surgery, a population that implies unique challenges [1].
Specimen dissection is perhaps the most valuable tool to properly identify surgical landmarks and eventually perform increasingly complex approaches in the diseased ear; therefore, the reader is encouraged to attend the laboratory as often as possible. Besides a solid knowledge of temporal bone anatomy and its variants, having adequate otologic instruments and properly preparing and positioning the patient are crucial steps for a safe procedure.
16.2 Surgical Pathology of the Temporal Bone
Most patients undergoing temporal bone surgery are afflicted by benign pathology, which can be inflammatory, traumatic, congenital, idiopathic, or neoplastic. Cardinal symptoms of temporal bone disease are hearing loss, otorrhea, facial paralysis, pain, and vestibular manifestations. Unilateral facial paralysis and pain that do not respond to treatment or are unproportioned to the signs observed during the physical exam should draw suspicion of malignant disease.
16.2.1 Benign Pathology
16.2.1.1 Chronic Otitis Media with Cholesteatoma
Cholesteatoma is defined by the presence of squamous epithelium in the middle ear. It is a benign pathology, but it is locally invasive and has a destructive nature. It can be congenital or more often acquired. Congenital cholesteatomas are usually discovered during a routine physical exam. In contrast, patients with acquired cholesteatoma tend to have a long history of otorrhea and conductive hearing loss. Most patients seek medical attention when hearing loss interferes with social activities; tinnitus is another common cause of consult. During the physical exam, tympanic membrane retraction and/or perforation, scutum and/or ossicular chain erosion, foul-smelling discharge, and an encapsulated white lesion full of greasy keratinaceous debris are common signs [2]. An aural polyp may also be found, and its presence should raise suspicion of malignant disease. Despite a slow growth rate, cholesteatomas frequently get infected and can lead to intratemporal and intracranial complications. Diagnosis is clinical, but audiometric testing is essential to evaluate the degree of conductive hearing loss and to identify sensorineural hearing loss, which might alert the surgeon of a labyrinthine fistula. Bone erosion is a classic feature of cholesteatoma, but beyond diagnostic confirmation, the real value of computed tomography (CT) scanning is its ability to determine the extent of disease, rule out complications, identify anatomical variants, and make a differential diagnosis with neoplastic disease [3, 4]. Treatment is essentially surgical, and the main goal is to eradicate the disease. Canal wall down procedure is the most effective to remove the matrix, but functional results are poor [5]. The use of endoscopes and the possibility to perform sequential magnetic resonance with diffusion-weighted imaging have allowed surgeons to perform less extensive surgeries with good results [6,7,8].
16.2.1.2 Temporal Bone Fracture with Facial Nerve Palsy
Adult patients with a temporal bone fracture have a 7–10% risk of developing a facial nerve injury; the risk is closer to 3% amongst children. The most common site of injury is the perigeniculate region, followed by the second genu. The tympanic and mastoid portions of the facial nerve may also be affected [9].
To decide between conservative and surgical management, the two main factors to consider are the time of onset (immediate vs. delayed) and the severity of injury (complete vs. partial). With regard to the time of onset, paralysis is immediate in 27% of cases, while in the remaining 73% facial motion will be normal at initial evaluation and paralysis installs 1–16 days later. Paralysis is complete in 25% of cases [10].
Surgical decompression should be considered in cases of immediate-onset complete facial nerve paralysis. Cases of complete paralysis in which the onset of paralysis is unknown should be treated as immediate. The selection of patients for surgical management is controversial, as 63% of patients with immediate-onset complete facial nerve paralysis will recover with high-dose steroids. If the nerve has suffered an unrecoverable injury, the outcome after conservative management is poor; hence, performing electrodiagnostic tests is paramount for selecting those patients that will benefit from surgery. Electroneurography (ENoG) is performed 3–14 days after injury, to allow Wallerian regression to take place. Two weeks after the onset of paralysis, electromyography (EMG) is preferred. Surgery is recommended if ENoG shows more than 90% of facial nerve degeneration or EMG fails to reveal voluntary motor unit potentials and only shows fibrillation potentials [11].
Ideally, surgery should be performed within the first weeks after trauma [12]. Other authors consider it appropriate to perform surgery during the first 2 months [13]. A translabyrinthine approach is preferred in patients with total hearing loss. In those with residual hearing, there is some controversy on the extension of the procedure. Alternatives are to perform a limited exploration based on clinical evaluation and imaging or to perform a total facial nerve exploration and decompression by a middle fossa and transmastoid/supralabyrinthine approach [9, 14]. When compared to the transmastoid approach, the middle fossa approach allows better exposure of the geniculate ganglion, the greater superficial petrosal nerve, and the tympanic segment of the facial nerve. The middle fossa approach also enables the identification of the labyrinthine segment, while the transmastoid approach does not. Currently, the surgical management of Bell’s palsy is controversial.
16.3 Sensorineural Hearing Loss and Cochlear Implant Surgery
Cochlear implant (CI) surgery is the most remarkable progress in otology in the twentieth century, allowing rehabilitation of patients who received little or no benefit from hearing aids. Bilateral severe or profound neurosensorial hearing loss continues to be the most frequent indication. Outstanding results and rapid technological advances have widened the selection criteria for candidacy, in both children and adults [15]. One of the major changes in selection criteria concerns the tendency to lower the age of CI surgery, in response to evidence showing that an early diagnosis and implantation allow for better language development. In 1990, the U.S. Food and Drug Administration (FDA) considered that the minimum age for CI surgery was 2 years old. Currently, the FDA approves CI surgery in 1-year-old children, and several centres worldwide support CI surgery in younger children [1]. Those implanted younger than 1 year of age represent a surgical challenge due to higher possibilities of intraoperative bleeding, facial nerve injury, and device migration. Difficulties to evaluate response to hearing aids and an increased anaesthetic risk should also be considered.
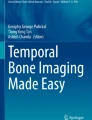
Electrode insertion through the round window is the preferred technique for cochlear implantation. The preferred approach is to perform a simple mastoidectomy followed by a posterior tympanotomy (Fig. 16.1). The main risk associated with this classic approach is facial nerve injury; the current rate is less than 1%.

CI insertion through the round window, incus (1), incus buttress (2), lateral semicircular canal (3), facial nerve (white line), round window (black arrow)
Anatomical variations like cochlear ossification, chronic otitis media, and cochlear malformation were considered a contraindication to CI. However, possible auditory benefits of cochlear implantation have led surgeons to develop alternatives to the standard technique. Non-mastoid approaches, including suprameatal, transcanal, and pericanal approaches, have been developed to reduce the risk of facial nerve and chorda tympani injuries and are useful tools in the context of cochlear malformations or unfavourable facial recess anatomy. Nevertheless, non-mastoid approaches are not ideal when the goal is hearing preservation, as most require creating a cochleostomy or providing a limited angle to the round window precluding a non-traumatic insertion [16]. The previous techniques might be contraindicated in patients with an open cavity in the context of chronic otitis media. In these complex cases, the middle fossa approach is a valid alternative for CI surgery [17].
16.4 Vestibular Disorders
Injury to the peripheric vestibular system may manifest with a myriad of symptoms, such as vertigo, dizziness, or chronic imbalance. These symptoms may or may not be triggered by postural changes and visual or auditory stimuli. Vestibular symptoms frequently present themselves with auditory and vegetative symptoms. Clinicians should suspect central vestibular system pathology if these are absent or if focal neurological symptoms are present, especially in the context of an acute vestibular syndrome. An aetiologic diagnosis is challenging and requires a careful history and a specific battery of tests, which are not included in the purpose of this chapter. Surgical management of peripheral vestibular disorders is needed in the minority of cases, yet surgery is a valuable resource in selected cases. Menière’s disease and superior semicircular canal dehiscence are two examples of the role of surgery for vestibular disorders.
16.4.1 Ménière’s Disease
Ménière’s disease is a well-known cause of episodic vestibular syndrome. It consists of recurrent episodes of spontaneous vertigo usually associated with unilateral fluctuating sensorineural hearing loss (SNHL), tinnitus, and aural fullness. Specific diagnostic criteria have been proposed by the Bárány Society [18]. The exact cause of Ménière’s disease is still a matter of discussion; nevertheless, endolymphatic hydrops seems to play a role in pathogenesis. Treatment options for intractable Ménière’s disease are endolymphatic sac surgery, intratympanic gentamicin, vestibular neurectomy, and labyrinthectomy with simultaneous cochlear implantation [19, 20]. Endolymphatic sac surgery is a specific procedure for Ménière’s disease, intended to control endolymph flow and stabilize the disease. After a series of studies by a Danish group suggesting that endolymphatic sac surgery was comparable to simple mastoidectomy with a considerable placebo effect, the procedure fell from favour [21, 22]. Re-evaluation of data found inconsistencies in Thomsen’s study, and endolymphatic sac surgery has proven to have better control of vertigo than mastoidectomy [23]. In a systematic review published by Sood and colleagues, both sac decompression and mastoid shunt procedures were effective at controlling vertigo in the short term (between 12 and 24 months of follow-up) and long term (>24 months) in at least 75% of patients with recalcitrant Ménière’s disease [24]. Since endolymphatic sac surgery can preserve inner ear function and hearing, some suggest that it should be the first strategy for intractable Menière’s disease [25]. Nevertheless, controversy regarding the efficacy of endolymphatic sac surgery remains, and a systematic review concluded that high-quality evidence on the matter is still lacking [26]. Hearing preservation with intratympanic gentamicin and vestibular neurectomy is comparable, but the latter is associated with better control of vertigo. Yet, the simplicity of intratympanic gentamicin has reduced the number of patients treated surgically [27].
16.4.2 Superior Semicircular Canal Dehiscence
Superior semicircular canal dehiscence (SCCD) consists of a bony defect in the roof of the superior semicircular canal (SSC). Minor was the first to describe the relationship between the anatomical defect of the temporal bone and a third window phenomenon [28]. Vertigo induced with loud sounds and/or pressure changes, egophony, tinnitus, chronic disequilibrium, and mild conductive hearing loss are frequent symptoms. Clinical diagnosis based on clinical manifestations is elusive, as symptoms can be vague, and SCCD is frequently mistaken with otosclerosis, perilymphatic fistulae, and otosyphilis, amongst others. Patients with SCCD have bone conduction hyperacusis and intact tympanic reflexes, while patients with otosclerosis do not. CT is necessary to confirm the anatomic defect, and slices should be thin (0.5 mm) with reconstructions in the planes of Stenvers and Pöschl (Fig. 16.2a, b). Yet, most patients with anatomic dehiscence will be asymptomatic. Moreover, in the face of a patient with an anatomic defect and symptoms, surgeons should also bear in mind that the otovestibular symptoms might not be explained by dehiscence. This is relevant when selecting surgical candidates, as surgical treatment of SCCD is highly effective for severe vestibular symptoms in well-selected patients, but then in many cases, it implies a medial fossa approach. Vestibular evoked myogenic potential (VEMP) testing can offer a 91% sensitivity and 96% specificity for diagnosing SCCD, and they are also valuable for follow-up and assessing surgical outcomes [29].

(a) CT scan of superior semicircular canal dehiscence (black arrowhead), (b) CT scan of superior semicircular canal dehiscence (white arrowhead) in Pöschl plane
16.5 Benign Tumours of the Temporal Bone
Tumours affecting the temporal bone, especially malignant ones, are rare. Amongst benign neoplasms, the most common histologic types are adenomas, paragangliomas, schwannomas, and mesenchymal tumours like lipoma, chordoma, hamartoma, and bone-related neoplasms.
To perform an extensive revision of temporal bone tumours escapes the scope of this chapter. We will only mention the most representative lesions, with emphasis on their surgical management.
16.5.1 Middle-Ear Glandular Neoplasms: Adenoma, Neuroendocrine Adenoma, and Carcinoid Tumours
Adenoma and its variant, the neuroendocrine adenoma, are rare benign neoplasms. They are not easily distinguishable from carcinoid tumours. Literature is characterized by heterogeneous terminology, making it difficult to find standardized reports amongst centres. Adenomas, neuroendocrine adenomas, and carcinoid tumours are currently considered primary low-grade glandular neoplasms with metastatic potential and have epithelial and/or neuroendocrine differentiation [30].
The most frequent symptoms are aural fullness and mild hearing loss, most often conductive. Otoscopy shows a retrotympanic mass with no distinctive traits. On CT, they are a well-circumscribed, soft-tissue mass without bone erosion. On MRI, they show a low-to-intermediate intensity on T1 with enhancement after administration of gadolinium and high intensity on T2-weighted images [31].
Since the clinical presentation and the imaging tests are not specific, the diagnosis depends on histologic and immunohistochemical examination. Based on immunohistochemical markers and the presence of metastasis, Saliba proposed a classification of middle-ear glandular neoplasms (Table 16.1).
Treatment is surgical resection; the procedure depends on the extension. When the ossicular chain is involved, it should be removed to reduce recurrence. The rate of recurrence is 18–22% in those patients in whom the removal of the ossicles was not performed [33]. Long-term follow-up is recommended.
16.5.2 Vestibular Schwannoma and Other Cerebellopontine Angle Neoplasms
Vestibular schwannoma (VS), previously known by the confusing name of “acoustic neuroma”, is a benign, slow-growing neoplasm arising from the Schwann cells of the vestibulocochlear nerve. The vestibular branches are affected in 95% of cases. They represent 6% of all intracranial tumours and 80–90% of all cerebellopontine angle (CPA) neoplasms. 90% are unilateral, and the most frequent clinical presentation is asymmetric sensorineural hearing loss and/or tinnitus. Differential diagnosis of a CPA mass is made with meningioma, epidermoid cyst, facial nerve haemangioma, and facial nerve schwannoma (FNS) [31].
Imaging studies are useful to differentiate VS from other CPA masses. VS is typically T1-isointense and T2-hyperintense and enhances homogeneously with contrast (Fig. 16.3). Meningiomas are also enhancing lesions but have a broad dural base and are isointense to grey matter on T1 and T2, and epidermoid cysts show diffusion restriction. FNS involving the CPA and/or the internal acoustic segment of the facial nerve is indistinguishable from a VS unless it extends to the labyrinthine segment [34]. MRI is also helpful for prognosis, as VS with cystic changes is associated with more rapid growth, a deeper hearing loss, and an unfavourable surgical outcome [31].

Vestibular schwannoma MRI, (a) T1-weighted, vestibular schwannoma (VS), (b) T2-weighted, cochlea (arrow), lateral semicircular canal (arrowhead), (c) T1 post gadolinium
Treatment options of VS include watchful waiting with MRI, surgical resection, and stereotactic surgery. Treatment selection depends on tumour size, growth rate, symptoms, patient’s age and preference, and the centre’s resources.
The goal of surgery is tumour control with as little morbidity as possible, preserving facial nerve function and, if feasible, hearing. Hence, subtotal resection with long-term surveillance is currently a valid alternative to preserve function. The approach is selected according to preoperative hearing, tumour size, and tumour location. Plausible approaches are the middle fossa, the retrosigmoid, and the translabyrinthine. The translabyrinthine approach is only suitable when the patient does not have a useful hearing. If hearing preservation is intended, the retrosigmoid or the middle fossa approaches are preferred. The middle fossa is indicated for small lateral tumours with less than 1 cm of CPA component and retrosigmoid for medial VS with a larger CPA component [35].
16.5.3 Temporal Bone Paraganglioma
Temporal bone paragangliomas (TBP) are benign vascular tumours that arise from neural crest cells. They are rare, with an incidence of 1 case per 1,000,000 habitants per year [36]. Despite their rarity, they are the most common middle-ear benign neoplasms. TBP may be further classified into tympanic and jugulare paraganglioma. Tympanic paraganglioma (TP) develops from paraganglion cells in the tympanic plexus associated with Jacobson’s (IX) and Arnold’s (X) nerves, and jugulare paraganglioma (JP) from adventitia of the jugular bulb. Nevertheless, these lesions share histologic characteristics, epidemiology, and large tumours that will eventually affect both the mesotympanic area and the jugular fossa, making it clinically irrelevant to determine where the lesion first started. Hence, we find the umbrella term jugulotympanic paraganglioma more useful. Most cases are unilateral and sporadic, present in the fourth or fifth decade of life, and are three times more frequent in women. The classic clinical presentation of lesions affecting the tympanic cavity is unilateral conductive hypoacusis, pulsatile tinnitus, and aural fulness. Large tumours may affect cranial nerves VII, IX, X, XI, and XII; affection of the lower nerves indicates jugular fossa compromise. Small tumours might be asymptomatic. A pulsatile, vascular, and retrotympanic mass is the characteristic otoscopic finding. Unlike paragangliomas located in the abdomen, lesions in the skull base are seldom related to catecholamine release. Less than 5% undergo malignant transformation; malignancy is defined by the presence of metastasis. The two main systems of classification are the Glasscock-Jackson classification [37], which proposed one classification system for TP and another for JP, and the Fisch classification, which includes both [38]. We consider that the classification proposed by Fisch is more practical, as it helps the surgeon to decide surgical management regardless of the site of origin of the paraganglioma.
The diagnostic protocol should include a thorough neurological examination, nasopharyngolaryngoscopy, audiology, and imaging tests with and without contrast. Angiography and embolization 24–72 h before resection should be considered in Fisch C and Fisch D tumours (Fig. 16.4). Measurement of catecholamines is not recommended in all patients, but the clinician should carefully look for symptoms suggesting the presence of a secretory neoplasm. Due to the small number of cases, management is controversial. Radiotherapy, surgical excision, and wait and scan are the three main treatment alternatives. The selection of treatment depends on the patient’s age, comorbidity, tumour size and growth, preoperative hearing and cranial nerve status, and presence of bilateral disease.

Embolization of glomus jugulare, (a) angiography before embolization, (b) angiography after embolization, vascular tumour (black arrow)
Surgical resection is the preferred modality of treatment for small TBP, especially for small TP that can be resected through a transcanal approach. Fisch B tumours can be removed by a transmastoid approach; according to tumour size, a canal wall up or a subtotal petrosectomy might be necessary [39]. For resection of larger tumours (Fisch C and D), Fisch described the infratemporal approach, which requires an anterior transposition of the facial nerve in 70% of cases. In Fisch’s series, 85% of patients had a preserved facial nerve function 2 years after surgery. In the same series, preservation of cranial nerves IX, X, XI, and XII was difficult to achieve [38]. Due to the higher morbidity to resect Fisch C and D tumours, some authors rather leave macroscopic disease and irradiate if growth is observed during follow-up. This alternative is associated with better local control and fewer complications than complete surgical resection [40]. Others have described cranial nerve preservation techniques like the intrabulbar dissection technique [41] or modifications of the infratemporal Fisch approach [42]. Radiotherapy is reserved for the elderly, as it increases the risk of malignant tumours and cerebrovascular accidents [40].
16.6 Malignant Neoplasms
Malignant neoplasms of the temporal bone are rare; they represent less than 0.2% of all tumours of the head and neck [43]. The estimated incidence of malignant tumours is close to 1 case per 1,000,000 inhabitants per year.
These tumours include lesions of the skin of the pinna that invade the temporal bone, primary tumours of the external auditory canal, middle ear or the petrous apex, and secondary tumours. Secondary tumours result from either distant metastasis or direct infiltration; the latter accounts for most cases of temporal bone malignancies [44]. Carcinomas of the breast, lung, and prostate are the main locations of primaries that cause distant metastasis affecting the temporal bone. Direct infiltration is typical from carcinomas of the periauricular skin and the parotid; infiltration from temporomandibular and advanced nasopharyngeal neoplasms may also occur [45]. Primary malignancies are represented by acinic cell carcinoma, adenocarcinoma, adenoid cystic carcinoma, basal cell carcinoma, chondrosarcoma, osteosarcoma, squamous cell carcinoma (SCC), and haemato-lymphoid tumours.
Differential diagnosis differs widely between adult and paediatric patients. For instance, SCC accounts for 60–80% of temporal bone malignancies in adults; meanwhile in children, rhabdomyosarcoma is the most common malignancy [46]. The main risk factors are sun exposure and a history of radiotherapy to treat another head and neck malignancy. Chronic otitis media and infection with papillomavirus have also been associated with the development of malignancy [43].
16.6.1 Squamous Cell Carcinoma of the Temporal Bone (SCCTB)
SCCTB is an aggressive malignancy (Fig. 16.5). Initial symptoms like otorrhea, pain, hypoacusis, and bleeding are non-specific, leading to a delayed diagnosis and a poor outcome. Non-resolving otitis externa should raise suspicion of malignancy.

Squamous cell carcinoma of the temporal bone arising in the right pinna (white arrow)
Preoperative imaging with a CT is essential for staging; it can detect bone erosion of 2 mm or greater. It is recommended to extend it to the chest for evaluation of distant metastasis. MRI is complementary and allows evaluation of perineural spread and intracranial involvement. An alternative to rule out distant metastasis is to perform a PET scan from the skull base to the lower extremities [47].
Unlike most carcinomas, the staging system for temporal bone carcinoma proposed by the American Joint Committee on Cancer (AJCC) is not widely used. The modified University of Pittsburgh staging system is the most accepted in literature (Table 16.2) [48]. According to Moody et al. (2000), the 2-year overall survival (OS) rates were 100% for T1 tumours, 80% for T2, 50% for T3, and 7% for T4 [49]. In a retrospective review including 11 studies and 195 patients, the 5-year OS rates based on the same system were 94.1% for T1, 80.8% for T2, 62.5% for T3, and 46.3% for T4. Two ominous signs are facial nerve paresis and dural infiltration, and as shown in Table 16.2, the presence of either classifies the tumour as a T4 lesion. Dural infiltration is the strongest negative factor affecting survival. A study concluded that the predictive performance of the modified Pittsburgh staging system is acceptable [50]. Mortality most often results from uncontrolled locoregional recurrence rather than from distant metastasis [51].
The mainstay treatment is surgical resection with or without radiotherapy (RT). Post-operative RT is recommended in T2, T3, and T4 tumours. Primary radiation is an alternative for T1 tumours. Definitive chemoradiotherapy (CRT) may be appropriate for cases with unresectable tumours or distant metastasis.
Sleeve resection, lateral temporal bone resection (LTBR), subtotal temporal bone resection (STBR), and total temporal bone resection (TTBR) are the different techniques designed to treat temporal bone malignancies. Sleeve resection does not include resection of the bony external auditory canal and is only suitable for the management of low-grade tumours. The minimal procedure for the management of SCC is an LTBR, and it is recommended for T1 and T2 lesions. For T3 and T4 lesions, STBR or TTBR is a recommended alternative; nevertheless, TTBR is a very morbid procedure, and survival benefit has not been proven. Curative surgery when dura is infiltrated is doubtful, because despite resection the rate of recurrence is high, and survival is poor. Therefore, even when resection is technically possible, palliation may be a reasonable alternative.
Superficial parotidectomy is indicated when the tumour infiltrates the gland, and it has a prophylactic role in T3 and T4 lesions. Neck dissection is indicated only with curative intent.
16.7 Investigation Tools for Temporal Bone Diseases
Investigation tools for temporal bone diseases have had impressive development. The numbers of tests available to the clinician may be overwhelming, and the detail of each test is beyond the scope of this chapter. Tests can be divided into three major groups: audiology tests, vestibular tests, and imaging.
16.7.1 Diagnostic Audiology
When evaluating hearing in adults, a pure-tone audiogram is the screening test of choice. This simple test allows the surgeon to determine the hearing threshold of the patient before and after surgical treatment, and it is also useful for differential diagnosis. Nevertheless, it is only suitable to determine hearing acuity and type of hearing loss. Then, audiometry should be complemented with speech discrimination tests. Patients with sensorineural hearing loss demonstrate lower scores on speech discrimination tests than expected from the audiogram. Pure-tone audiogram and speech discrimination tests require the patient’s cooperation; when this is not possible, objective tests like otoacoustic emissions, auditory steady-state response, and auditory brainstem response are valuable alternatives. Tympanometry and stapedial reflexes are simple and useful tools to evaluate middle-ear function.
16.7.2 Vestibular Tests
Parallel to the complexity of vestibular physiology is the number of tests available for the evaluation of vestibular function. The goal of vestibular testing is to identify the presence of a balance disorder, locate the lesion, and evaluate the residual function and the possibility of recovery. The main tests to consider are videonystagmography (VNG), video hit impulse test (vHIT), posturography, and vestibular evoked myogenic potential (VEMP).
VNG has replaced electronystagmography and is currently the most used method for recording eye movements. It comprises a series of subtests that assess the function of the vestibular end organs and the central vestibulo-ocular pathways. The caloric test is one of the subtests of the VNG; it was the main test to assess peripheral vestibular function. Currently, the caloric test is being replaced by vHIT, because it is a quick, innocuous test that evaluates the vestibular-ocular reflex (VOR) of the six SCCs independently, and results are more reliable [52]. Posturography evaluates the ability of the patient to maintain balance and analyses the specific contribution of the three major systems involved: vestibular, visual, and somatosensory. Finally, VEMP testing is a method used mainly in tertiary reference centres and in research. It has an increasing role for diagnosing peripheral vestibular disorders, especially for diagnosis and follow-up of SCCD, and for follow-up of intratympanic gentamicin treatment in patients with Menière’s disease (Fig. 16.6). Their role in the topographic diagnosis of central disorders is under research [53].

VEMP in a patient with semicircular superior canal dehiscence; note the amplitude and low threshold
16.7.3 Imaging
A high-resolution computed tomography (HRCT) of the temporal bone is the workhorse imaging study for temporal bone disease. It is an important preoperative investigation tool for cholesteatoma surgery, temporal bone fracture, middle-ear glandular neoplasms, TBP, SCCD, and malignant neoplasms (Fig. 16.7). It is useful to confirm the diagnosis of SCCD and essential for staging of SCCTB. In cholesteatoma, temporal bone fracture, TBP, and neoplasms, it is helpful to determine the disease extent and identify the presence of anatomical variants and potentially dangerous difficulties such as a high-riding jugular bulb, a low-lying dura, facial canal dehiscence, erosion of tegmen, or semicircular canal erosion, consequently assisting surgeons in elaborating a surgical plan [54]. The use of contrast is necessary if there is a concern of a vascular mass or clinical assessment suggests an abscess. Angiography and embolization should be considered for large jugular paragangliomas. MRI is the main tool for the evaluation of non-osseous components. Hence, it is useful for the assessment of VIII cranial nerve in candidates of cochlear implantation, evaluation of CPA neoplasms, facial nerve neoplasms, and lesions with dural extension or exposure. The use of DWI-MRI has reduced the number of second-look surgeries in patients with cholesteatoma. In contrast to most head and neck neoplasms, ultrasound has a limited role in the evaluation of temporal bone diseases. It might be useful for the evaluation of periauricular cystic lesions. Nuclear medicine studies are used for diagnosis and follow-up of skull base osteomyelitis, a major differential diagnosis of SCCTB. Finally, PET or PET/CT may be used for the assessment of temporal bone masses or nodal metastases.

CT scan in a patient with a middle-ear neoplasm
16.8 Anatomical Landmarks and Surgical Procedures
16.8.1 Surgical Approaches and Incisions
Every incision used in otologic surgery should create broad access to the surgical field, allow a direct extension to adjacent anatomical areas, permit the use of adjacent skin as a free or pedicled flap, and provide an acceptable cosmetic result [55].
Depending on the approach chosen, different incisions can be used. The postauricular, transcanal, and endaural incisions are the most common, as they allow a posterior, transmeatal, and anterior approach. Each approach has advantages and limitations and should be chosen based on the location and extension of the disease.
16.8.2 Postauricular Incision
A postauricular incision allows a great surgical exposure and harvest of temporalis fascia. It is useful for tympanoplasty, in cases of anterior tympanic membrane perforations in patients with prominent anterior wall canals, and it is the workhorse incision for transmastoid approaches.
Postauricular incisions can be performed either on the postauricular sulcus or 0.75–1.0 cm posterior to it (into the hairline). The incision should begin at the highest level of the helix and must extend to the mastoid tip, always taking into account the descending segment of the facial nerve, which exits from the stylomastoid foramen between the mastoid tip and styloid process (Fig. 16.8). It is essential to keep in mind that in paediatric patients, the facial nerve is more superficial [56].

Retroauricular incision in the right ear
After cutting through the skin and subcutaneous tissue, the auricular muscles are generally divided to access and incise the periosteum overlying the mastoid bone. Depending on the surgery, a small amount of temporalis fascia may be harvested, but the underlying muscle must be left intact [57].
16.8.3 Transmeatal Incisions
This approach is appropriate for otologic procedures limited to the tympanic membrane and posterior tympanic compartment (e.g. stapedectomy, tympanoplasty).
The transmeatal incision consists of two vertical incisions made in the external auditory canal (EAC) skin, starting from the annulus at the 6 and 12 o’clock positions (along the tympanomastoid and tympanosquamous suture lines). These incisions extend radially and are connected by a third horizontal semilunar incision in the medial or external third of the ear canal (Fig. 16.9) [58]. The canal skin and tympanic membrane (tympanomeatal flap) are elevated together up to the tympanic annulus, granting access to the middle-ear space.

Transmeatal incision, endoscopic view of left ear. (a) First vertical incision (black arrowheads), annulus (red arrowheads), flap knife (grey arrow), umbo (1), short process of the malleus (2). (b) Second vertical incision (black arrowheads), horizontal incision (white arrowheads), round cutting knife (grey arrow), annulus (grey line), umbo (1), short process of the malleus (2)
16.8.4 Endaural Incisions
These incisions, described by Lempert in 1938, are external to the meatus and expand the surgical field [59]. In some cases, an anterior canal bulge can hide the anterior half of the tympanic membrane and therefore is necessary to make an endaural incision to improve exposure. It is indicated for most tympanoplasties and some mastoidectomies.
The first part of the incision (Lempert I) is made in a semi-circumferential way between 6 and 12 o’clock on the back wall of the EAC at the bony cartilaginous junction. This intercartilaginous incision is prolonged vertically between the helix and tragus (Lempert II) to obtain a wider posterior flap that gives a better exposure to the mastoid cortex. The incision could be extended down (Lempert III) enough to retract soft tissue and fully expose the cortex and tip of the mastoid (Fig. 16.10).

Endaural incisions: Lempert types I, II, and III
16.8.5 Incisions for the Middle Fossa Approach and Infratemporal Fossa Approach
There are two main types of incision for a middle fossa approach, each designed for a different flap. When using an anterior/inferiorly based skin flap, the incision starts anterior to the tragus, extends posteriorly to the temporal region, turns superiorly 5–6 cm, and turns anteriorly again reaching the temporal hairline, making an “S” shape. This is also known as a question mark incision. For the posteriorly based skin flap, the incision starts behind the temporal hairline, extends anteriorly for 6.0 cm, turns superiorly for 6 cm, and turns posteriorly again for 6 cm, in the shape of a rounded box. Other alternatives are to simply extend a retroauricular incision anteriorly following the hairline or to do a vertical preauricular incision (Fig. 16.11). The skin incision for the infratemporal fossa approach is a neck extension of the C-shaped retroauricular incision.

Incisions for the middle fossa approach, anterior extension of a C-shaped retroauricular incision (1), preauricular incision for an anterior based flap (2), vertical linear preauricular incision (3), incision for a posterior based flap (4)
16.9 Anterior Atticotomy
In an anterior atticotomy, only the posterior superior bone portion of the EAC, known as scutum, is removed. The procedure is used in limited attic cholesteatomas since the scutum is the first bony structure to be eroded.
After making an endaural or postauricular approach, the superior and posterior bone portion of the canal is exposed, and the lateral epitympanic wall is removed with a burr until a thin layer of bone is left over the ossicles [60]. This layer is then removed using curettes to expose the tegmen tympani and ossicular chain. Once the procedure is finished, the defect can be reconstructed with a cartilage graft or autologous bone [58].
16.10 Transmastoid Approaches
The mastoidectomy is often performed for chronic otitis media with and without cholesteatoma. It is the initial step for several otologic procedures, including cochlear implantation, endolymphatic sac decompression, and most presigmoid approaches to the lateral skull base [61].
In 1873, Schwartze and Eysell published a paper describing for the first time the mastoidectomy procedure [62]. They highlighted the importance of finding and exposing the mastoid antrum as one of the key steps during the procedure [63]. The surgery starts in the lateral surface of the mastoid bone by drilling the cortical bone to expose the mastoid air cells. Thorough anatomical knowledge is an essential prerequisite of mastoid surgery [64]. Mastoidectomies are classified as either “wall up” or “wall down” depending on whether the posterior wall of the EAC is maintained.
16.10.1 Canal Wall Up (Intact Canal Wall) Mastoidectomy
Under microscopic vision and using a round cutting burr with continuous suction-irrigation, drilling is initiated along the linea temporalis (the lowest point of the middle fossa dura). A second line is drilled perpendicular to the previous one, tangent to the posterior margin of the EAC, behind the spine of Henle (small bony prominence anterior to the supramastoid pit at the posterosuperior margin of the bony EAC) [65]. These drill lines outline a triangular area posterior to the EAC, whose apex lies over the lateral semicircular canal, known as the MacEwen triangle (Fig. 16.12) [66].

Anatomical landmarks for mastoidectomy. Right temporal bone specimen, linea temporalis (LT), spine of Henle (H), posterior margin of the EAC (PoEAC), line representing the approximate location of the sigmoid sinus (SS), MacEwen triangle (MT)
Drilling is done in this area until air cells appear, removing cortical bone and thinning the posterior wall of the EAC. The superior limit is the tegmen mastoideum (level of the temporal line), and the anterior limit is the root of the zygomatic process [67]. Identifying the dura is often a meaningful step during mastoidectomy, as it represents an important anatomical landmark [68]. The bone should be drilled away evenly, orienting the surgical instrument parallel to the patient’s skull to avoid inadvertent damage to the ossicular chain. During this step of the dissection, the most important landmark is the sigmoid sinus, which is identified by its bluish colour and thin bony plate [58]. The sigmoid sinus and the tegmen mastoideum meet in an angle known as the sinodural angle (Citelli’s angle). Drilling is continued toward the mastoid tip, removing cells from the digastric ridge area. The facial nerve exits at the stylomastoid foramen, immediately anterior to the digastric ridge. Knowledge of this area is essential when performing mastoid surgery [69]. In case of extensive mastoid pneumatization, neighbouring structures like the dura of the middle and posterior cranial fossae, the sigmoid sinus, and the facial nerve may lack a bony hull, making them prone to injury [68]. The dissection is continued medially reaching Körner’s septum, a thick plate of bone that represents the persistence of the petrosquamous suture line, which divides the mastoid process into a superficial squamous portion and a deep petrous portion [70, 71]. This structure is removed to reach the mastoid antrum, the largest air cell in the mastoid cavity, connected to the posterior epitympanum via the aditus ad antrum (Fig. 16.13) [61].

Right mastoidectomy and antrum
Once identified, sculpt the EAC and tegmen toward the root of the zygoma to fully visualize the rest of the tegmen and the short process of the incus inside the fossa incudis. The horizontal semicircular canal (one of the most critical landmarks), characterized by its compact and ivory-coloured bone coat, should be identified at this point (Fig. 16.14) [72].

Identification of the incus; note that the bone at the horizontal or lateral semicircular canal, the relationship of the canal, and the short process of the incus with the second genu of the facial nerve are noteworthy
In case the incus is not visible, drilling is done anteriorly and inferior to the tegmen dura; this region has the widest distance between the ossicles and the tegmen tympani. The surgeon should remain superficial to the horizontal semicircular canal to avoid damage to adjacent structures. Figure 16.15 shows an intact canal wall mastoidectomy.

Canal wall up mastoidectomy, tegmen (T), sinodural angle (SDA), sigmoid sinus (SS), incus (I), posterior wall of external auditory canal (PoEAC), horizontal semicircular canal (1), posterior semicircular canal (2), fallopian canal (3), superior semicircular canal (4)
16.10.2 Canal Wall Down Mastoidectomy
Canal wall down mastoidectomies are indicated when the disease is extensive enough to cause damage to the posterior wall of the EAC or when there is a suboptimal visualization of the cavity and no certainty of complete eradication of the cholesteatoma. This procedure, also known as radical mastoidectomy, requires a complete mastoidectomy plus removal of the posterior superior osseous canal wall, exteriorizing the mastoid into the ear canal to form a single cavity [61]. In most cases, it is necessary to remove the ossicles affected by cholesteatoma, taking extreme care when manipulating the stapedius footplate. It is essential to drill superficial to the facial nerve and superficial to the semicircular canal; the objective is to create smooth transitions between the floor of the EAC and the mastoid cavity (single cavity). If the Eustachian tube is modified or the tympanic membrane or the mucosa of the middle ear or the ossicular chain is preserved, the procedure is referred to as a modified radical mastoidectomy.
16.10.3 Posterior Tympanotomy
A posterior tympanotomy is indicated in cholesteatoma eradication procedures (intact canal wall mastoidectomy), cochlear implantation, and middle-ear hearing device implantation [73]. It grants access to the middle ear and enables the surgeon to operate in the hypotympanum, the sinus tympani, and the region of the round window without lifting the tympanic membrane. This technique generates an opening between the facial nerve and the posterior wall of the EAC, in a region called the facial recess, which is a triangular area limited by the incudal buttress (superior), the vertical segment of the facial nerve (posterior), and the chorda tympani (anterior) (Fig. 16.16) [74].

Posterior tympanotomy: Anatomical landmarks, right ear, facial recess area outlined by a triangle: borders are the incus buttress, upper mastoid segment of the facial nerve, and chorda tympani
The facial nerve is carefully skeletonized at the mastoid genu to avoid exposure of the nerve sheath; the nerve and blood vessels can be seen through bone [58]. After identifying the chorda-facial angle, the chorda tympani are followed superiorly into the middle-ear space, thereby creating the opening of the facial recess (Fig. 16.17).

Opened facial recess, incus (T), incus buttress (IB), posterior wall of the external auditory canal (PoEAC), incudo-stapedial joint (IST), horizontal semicircular canal (HSC), mastoid facial nerve (MFN), round window (black arrowhead)
16.11 Endolymphatic Sac Decompression
Endolymphatic sac decompression is performed in patients with Menière’s disease that do not respond to medical treatment. The surgery starts with a simple mastoidectomy and identification of the posterior and horizontal semicircular canals, using Donaldson’s imaginary line as a reference. This line can be drawn along the horizontal semicircular canal, intersecting perpendicularly the posterior semicircular canal. The endolymphatic sac is posterior and inferior to this intersection and can be identified as a white and dense thickening of the dura (Fig. 16.18). After properly identifying the sac, it is opened and drained. A valve from the endolymphatic space to either the mastoid or the subarachnoid space can be inserted (shunt procedure).

Endolymphatic sac anatomy, surgical landmarks of endolymphatic sac, sigmoid sinus (SS), horizontal semicircular canal (1), posterior semicircular canal (2), distribution of facial nerve (red line), Donaldson’s line (blue line), triangle outlining the hard angle (blue triangle), approximate location of endolymphatic sac (ES)
16.12 Subtotal Petrosectomy
Indications of subtotal petrosectomy are chronic otitis media with or without cholesteatoma, meningoencephalic herniation, cerebrospinal fluid leak, and temporal bone tumours, amongst others. The most frequent indication is still infections of the temporal bone with necrosis, as it is a useful technique to debride as much bone as possible with preservation of facial function and cochlear reserve.
A wide retroauricular incision or a question mark incision is made in the skin, to expose the temporal muscle and mastoid process. The temporalis muscle is elevated anteriorly off the skull, and the muscle will be used later for the reconstruction. A mastoidectomy is performed; the semicircular canals, sigmoid sinus, posterior fossa dura, middle fossa dura, and vertical portion of the facial nerve are skeletonized; and the ossicles are removed with exception of the footplate of the stapes (Fig. 16.19). The sigmoid sinus is followed medially to the facial nerve to the jugular bulb performing a fallopian bridge technique. An elevator is used to remove the bone pieces from the sigmoid sinus and middle and posterior fossa. Classically, the concept of subtotal petrosectomy included removal of all cell tracts of the temporal bone, including antral, infralabyrinthine, pericarotid, retrosigmoid, retrofacial, retrolabyrinthine, supralabyrinthine, and supratubal cells. Currently, it is considered that the amount of temporal cells drilled is determined by the extent of the disease and is possibly more limited when the indication of surgery is cochlear implantation [75].

Canal wall down mastoidectomy, right mastoidectomy with skeletonization of facial nerve and semicircular canals. Tegmen (T), sinodural angle (SDA), sigmoid sinus (SS), epitympanum (E), Eustachian tube (ET), promontorium (Pr), tympanic facial nerve (TFN), mastoid facial nerve (MFN), area of the jugular bulb (JB), horizontal semicircular canal (1), posterior semicircular canal (2), superior semicircular canal (3)
When the petrosectomy is finished, the ET is obliterated with muscle or bone wax, and the temporalis muscle is divided into its anterior third to rotate a muscular flap underneath the temporal lobe and over the mastoid cavity defects. An alternative is to obliterate the cavity with abdominal bone. Finally, the temporal bone flap is repositioned, and the EAC is closed by everting meatal skin and suturing it.
16.13 Translabyrinthine Approaches
Through this approach, it is possible to reach the internal auditory canal (IAC), the posterior cranial fossa, and the cerebellopontine angle, without disturbing the integrity of the external auditory canal and tympanic cavity. This approach is suitable for the resection of CPA tumours without serviceable audition, endolymphatic sac tumours, management of vestibular disorders, and trigeminal neuralgia. A great advantage of this approach is that there is less retraction of the cerebellar mass in comparison with others, decreasing the risk of dysmetria and thrombosis of the sigmoid sinus.
A simple mastoidectomy with skeletonization of the sigmoid sinus and tegmen and exposure of the mastoid antrum and lateral semicircular canal is performed. When the bone over the sigmoid sinus and the posterior fossa is thin enough, a Freer elevator is used to retract the sigmoid sinus posteriorly. It is possible to leave a small island of bone above the sinus to protect it from the retractor, commonly known as Bill’s island. The mastoid emissary vein is transected and coagulated with bipolar cautery. If the sigmoid sinus is vulnerated, bleeding can be stopped with gentle pressure and by applying a haemostatic agent. The superior aspect of the jugular bulb must be skeletonized because it marks the inferior portion of the dissection. The posterior limit of dissection is the sigmoid sinus, while the superior limit is the superior petrosal sinus. Malleable retractors are placed between the posterior and middle fossa dura, then the drilling begins until the superior petrosal sinus, and the vertical segment of the facial nerve is identified. With the posterior fossa retraction, a tether can be seen indicating the position of the endolymphatic duct; it can be transected with an 11 blade scalpel, and then the retractor is advanced till the porus acusticus is identified.
The labyrinthectomy is performed using a diamond burr to extend the vestibule’s opening posteriorly toward the ampulla of the posterior semicircular canal (the ampullated ends of the superior and horizontal semicircular canals open into the anterior vestibule, which is medial to the horizontal segment of the facial nerve) (Fig. 16.20).

Drilling of semicircular canals, right mastoid, tegmen (T), sigmoid sinus (SS), mastoid facial nerve (FN), horizontal semicircular canal (HSC), common crus (CC), ampulla of posterior semicircular canal (APSC)
The medial wall of the vestibule contains the spherical recess and the elliptical recess; the former contains the saccule and the latter the utricle (Fig. 16.21). The vestibule marks the location of the fundus of the IAC; therefore, the surgeon must continue drilling the temporal bone parallel to the posterior fossa dura to find the porus acusticus that lies deeper than the fundus. When the porus acusticus is identified, superior and inferior troughs must be drilled and traced to the vestibule; it is important to keep the dura intact especially in the superior trough because the facial nerve could be displaced, especially when the indication of the procedure is a CPA tumour.

Vestibule, right vestibule, elliptical recess (ER), spherical recess (SR), mastoid facial nerve (NF), superior semicircular canal (SSC)
When thinning the bone near the fundus, the surgeon must drill in a more lateral position, compared to the medial position taken when working with the porus acusticus. When the bone is thinned, it should be carefully removed starting along the inferior dura of the IAC, then along the transverse crest, and at last along the superior portion of the IAC (Fig. 16.22). The transverse crest divides the fundus of the IAC in an upper part, containing the facial nerve and the superior vestibular nerve, and a lower part containing the inferior vestibular nerve and the cochlear nerve.

Transverse crest, right mastoid after drilling of semicircular canals, mastoid facial nerve (FN), transverse crest (blue arrow), inferior vestibular nerve (IVN), superior vestibular nerve (SVN). Note that vestibular nerves are located posteriorly and hence are more superficially encountered than the facial and cochlear nerves in the translabyrinthine approach
The dura is opened after removing the bone completely. Once the dura is opened, stimulation of the posterior portion of the tumour is done to locate the facial nerve. Then, a window in the surface of the tumour is performed to start debulking the tumour afterwards, and the capsule is removed in pieces. Subsequently, the dura of the IAC is opened to remove this part of the tumour, the superior and inferior vestibular nerves must be transected at the fundus, and resection of the tumour is completed. Open petrous apex cells must be plugged with bone wax, the aditus ad antrum is closed with fascia or dural substitute, and then the cavity is obliterated with abdominal fat.
16.14 Transcochlear Approach
It is an anteromedial extension of the translabyrinthine approach in which the cochlea is drilled out and the external ear canal is closed in a blind sac. This approach is indicated for cases where hearing preservation will not be attempted; it allows a wider exposure to the posterior fossa, ventral brainstem, and central skull base.
After exposing the dura over the IAC, the incus is removed, the facial nerve is exposed from the geniculate ganglion to the stylomastoid foramen, the greater superficial petrosal nerve (GSPN) is transected, and the facial nerve is transposed posteriorly so that the facial canal, petrous apex, and cochlea are drilled away until the edge of the clivus is reached exposing the inferior petrosal sinus and the petrous carotid. Since the facial nerve is transposed for greater exposure, a House-Brackmann grade III–IV facial palsy can be expected.
The transotic approach is similar to the transcochlear approach, with the difference that the facial nerve is kept in its bony canal and the EAC is closed in a blind sac.
16.15 Presigmoid-Retrolabyrinthine Approach
This approach can combine supra- and infratentorial craniotomy and a range of mastoid and labyrinthine resections. This approach provides access to the sigmoid sinus, presigmoid posterior fossa dura, and middle fossa dura. It can be useful to perform a vestibular neurectomy, microvascular decompression surgery, and resection of small CPA tumours that do not involve the internal third of the IAC.
With the presigmoid-retrolabyrinthine approach, the surgeon performs a “minimal mastoidectomy” that exposes the presigmoid dura, which is opened to gain access to the cerebellopontine angle (CPA). A Bill’s island can be used to reject the sigmoid sinus posteriorly and have a wider exposure (Fig. 16.23). A more extensive degree of exposure is achieved by skeletonizing the semicircular canals and the vertical portion of the facial nerve.

Presigmoid-retrolabyrinthine approach, left mastoid, posterior external auditory canal (PoEAC), tegmen (T), Bill’s island (BI), opened presigmoid dura (black arrow), close up to posterior semicircular canal after opening the dura (black star)
In a partial labyrinthectomy, usually the superior and posterior semicircular canals are drilled away with preservation of the lateral canal. The surgeon must keep in mind that hearing loss is likely to happen with this approach. Removing the posterior canal gives access to the posterior fossa and the superior canal to the middle fossa and petrous apex. This approach is mostly used to treat acute infections with intracranial complications such as sigmoid sinus thrombosis, epidural abscess, and subdural abscess.
16.16 Middle Cranial Fossa
Through this approach, it is possible to access the petrous apex, the IAC, and the posterior cranial fossa by retracting the temporal lobe. It can be useful to perform a vestibular neurectomy, resection of a lesion involving the geniculate and pregeniculate area of the facial nerve, management of a meningoencephalocele and SCCD, and resection of small schwannomas with acceptable audition preservation (lesions should not extend more than 1 cm medially into the CPA) and lesions involving the trigeminal nerve. However, temporal lobe retraction can cause injuries such as contusions, strokes, cerebral oedema, seizures, CSF leak, and injury to the carotid artery.
The skin, temporoparietal fascia, temporalis muscle, and periosteum are elevated by a single flap to expose the temporal squama to drill a sufficient temporal craniotomy (5 cm × 5 cm) centred over the zygomatic root; an endoscope can be used to reduce the size of the craniotomy. The middle fossa dura is separated from the bone flap using an elevator; this bone must be preserved for repairing the craniotomy at the end of the surgery. A Freer or a Joseph elevator can be used to elevate the dura off the temporal floor in a posterior-to-anterior manner, and the first landmark is the middle meningeal artery. If a larger exposure is needed, the middle meningeal artery can be divided to allow exposure to the posterior fossa. The next relevant anatomic structure is the arcuate eminence, which is absent in cases of SCCD (Fig. 16.24).

Dehiscent superior semicircular canal viewed from a middle fossa approach, facial nerve (black arrow)
The structure encountered next is the GSPN. While elevating the dura, the GSPN should be carefully identified to decrease the risk of injuring the geniculate ganglion, which is dehiscent in up to 15% of the patients [76]. Relevant anatomical references to locate the IAC are the GSPN and the arcuate eminence. The axis of the IAC intersects a 120° angle formed by the axis of the SSC and the GSPN. Others locate the IAC only relying on the arcuate eminence, as the axis of the IAC runs along an imaginary line located at a 60° angle from the axis of the SSC. The IAC and posterior fossa are reached by drilling away the petrous bone preferably medially, near the porus acusticus, though a diverse amount of techniques have been described [77]. The facial nerve and the superior vestibular nerve are the first nerves encountered when the IAC is opened; they are divided by Bill’s bar (Fig. 16.25).

Facial and superior vestibular nerves in the IAC, facial nerve (FN), superior vestibular nerve (SVN)
16.17 Infratemporal Fossa (IFT) Approach: Type A
This approach provides great exposure of the sigmoid sinus, jugular bulb, internal jugular vein, and internal carotid artery. It is used for tumours such as jugular paraganglioma, jugular foramen neuroma, jugular foramen meningioma, large parotid tumours of the deep lobe with infratemporal fossa extension, large schwannomas of the facial nerves, and lesions of the lower cranial nerves (IX, X, XI, and XII) [78].
The open approach to the ITF was classically described by Fisch, which is delineated into three types [79]. The type A approach provides exposure of the infralabyrinthine temporal bone and jugular foramen and is useful for the management of glomus jugulare tumours, neuromas, and meningiomas. The type B approach exposes the petrous apex and midclivus, including the horizontal ICA, which facilitates resection of chordomas and extensive cholesterol granulomas. The type C approach extends the exposure to the parasellar region, cavernous sinus, and foramen rotundum and permits resection of nasopharyngeal carcinomas and angiofibromas. All three variations lie within the domain of the neuro-otologist and involve mastoidectomy, facial nerve dissection and transposition, and obliteration of the Eustachian tube, middle ear, and external auditory canal with a resulting permanent conductive hearing loss.
To perform a type A IFT approach, a C-shaped retroauricular incision is performed and extended into the neck to the anterior border of the sternocleidomastoid (SCM) muscle. Dissection proceeds to expose the mastoid process, the parotid gland, and the digastric muscle. The SCM muscle is released from the mastoid process and retracted posteriorly, and then the mastoid tip is drilled away. The digastric muscle is divided and retracted anteriorly to drill the bone inferior to the sigmoid sinus. The lower cranial nerves, the carotid artery, and the jugular vein are identified and wrapped loosely with rubber slings.
A mastoidectomy with preservation of the ear canal wall is performed. The bone from the inferior portion of the sigmoid sinus is removed, and the facial nerve is followed down to the stylomastoid foramen to identify its main trunk. A facial recess approach extended inferiorly is performed, the chorda tympani nerve must be divided, and the ossicular chain should be kept intact. By skeletonizing the facial nerve, it is possible to gain access to the jugular bulb medially and open the hypotympanum to remove the tumour that has grown from the jugular foramen (Fig. 16.26). If a canal wall down mastoidectomy is performed, then the ear canal is transected and closed in a blind sac; the posterior wall is drilled away; the incudo-stapedial joint is separated; the tympanic membrane, malleus, and incus are removed; the Eustachian tube is plugged with muscle; and the anterior wall of the canal must be drilled to remove the epithelial remnants. Alternatively, to the fallopian bridge technique, rerouting of the facial nerve could be performed to gain more access to the jugular bulb.

Infratemporal fossa approach, type A, left mastoid. The facial nerve (FN) and the sigmoid sinus (SS) have been skeletonized, the surgeon is using a diamond burr to expose the jugular bulb
The venous flow to the sigmoid sinus is blocked by packing Surgicel between the bone of the sinus. The internal jugular vein is divided and ligated in the neck (Fig. 16.27), then the sinus wall is opened to expose the jugular bulb, and bleeding is controlled with Surgicel, cottonoid pledges, and pressure to occlude the inferior petrosal sinus collaterals and the condylar emissary vein. Complete removal of the tumour within the bulb is achieved.

Ligature of internal jugular vein: the internal jugular vein has been ligated in the left neck, and regurgitation of the jugular bulb is evident. Cottonoids have been placed to collapse the sigmoid sinus. Distal end of the internal jugular end (1), cephalic end of the internal jugular vein (2), jugular bulb (3), facial nerve (4)
16.18 Surgery for Squamous Cell Carcinoma: Temporal Bone Resection
Depending on the extension of the disease, the SCC of the temporal bone should be treated with a lateral temporal bone resection (LTBR), a subtotal temporal bone resection (STBR), or a total temporal bone resection (TTBR). The LTBR is performed en bloc through an extended facial recess approach, which implies the sacrifice of the chorda tympani. The EAC, tympanic membrane, malleus, and incus are removed, while the facial nerve and inner ear are entirely preserved. Depending on tumour spread, additional procedures should be considered, such as parotidectomy, partial mandibulectomy, and a modified neck dissection.
When malignancy has extended to the middle ear, dissection is extended depending on tumour spread. Starting with an en bloc LTBR, drilling continues medially into the otic capsule and petrous temporal bone till negative margins are attained. If the facial nerve is involved, it should be resected until a negative frozen section is achieved. The internal carotid artery is preserved. Nevertheless, the internal jugular vein and the internal carotid artery should be identified and controlled in the neck.
Finally, in TTBR, resection extends to involve the petrous apex, the sigmoid sinus, and possibly the petrous segment of the internal carotid artery. Internal carotid artery resection should only be considered in patients who have shown tolerance to ischaemia after performing a balloon test occlusion. Since TTBR has significantly higher morbidity compared with STBR, and a survival benefit has yet to be proven, selection of therapy should be carefully discussed with the patient and a multidisciplinary team. Reconstruction with mastoid cavity obliteration is especially relevant in patients undergoing post-operative radiotherapy.
16.19 Endoscopic Ear Surgery
Endoscopic ear surgery (EES) is a novel technique used to address middle ear and tympanic membrane pathology, including cholesteatoma, tympanic membrane perforation, and ossicular pathology. Some surgeons have used it to treat lesions like paragangliomas, meningiomas, and schwannomas [80]. This technique allows for an excellent surgical exposition using a transcanal approach, avoiding mastoidectomies and external incisions altogether. Due to its recent introduction, the surgeon must acquire a unique perspective on the anatomy of the middle ear. The most important structures and landmarks for this endoscopic procedure are given below.
16.19.1 Protympanum
The protympanic space lies anteriorly to the mesotympanum and inferiorly to the anterior epitympanic space. The anterior limit consists of the cochleariform process, the tensor fold, and the tensor tympani, while the posterior limit is marked by the promontory. The tympanic portion of the Eustachian tube is found in the protympanum and measures 11–12 mm in diameter. Above and medially to the Eustachian tube opening runs the internal carotid artery, which can be dehiscent in some cases. Knowledge of this area is important because cholesteatoma can hide in this region [81].
16.19.2 Epitympanum
The epitympanic space is a pneumatized portion of the temporal bone superior to the mesotympanum. It is divided from the latter by the epitympanic diaphragm. This last structure consists of three malleal ligamental folds (anterior, lateral, and posterior), the posterior incudal ligamental fold, and two membranous folds (the tensor fold and the lateral incudo-malleal fold) together with the malleus and incus [82]. From this anatomical point of view (using an angled 30° endoscope), it is possible to classify the epitympanum into two different compartments: a larger posterior compartment and a smaller anterior compartment. The posterior epitympanic space contains the incudo-malleolar joint, a crucial landmark during the transcanal endoscopic approach [81, 83].
16.19.3 Retrotympanum
The spaces surrounding the mesotympanum are complex because of the dimensions and details of the air cells [82]. Nevertheless, Marchioni et al. described four regions in the retrotympanum: the posterior sinus, sinus tympani, sinus subtympanicus, and facial recess [81]. These spaces are limited by the pyramidal eminence and three bony ridges, the ponticulum, subiculum, and funiculum. The ponticulum connects the pyramidal process to the promontory. The subiculum extends from the posterior lip of the round window to the styloid eminence. The funiculum marks the end of the retrotympanum and connects the anterior lip of the round window to the hypotympanic air cells. The posterior recess is a small space between the pyramidal eminence and the posterior crus of the stapes. The sinus tympani are located between the ponticulum and subiculum. The sinus subtympanicus is located below the sinus tympani, between the subiculum and funiculum [84]. Finally, the facial recess is located lateral to the pyramidal eminence.
The depth of the sinus tympani is significant because the deeper it is, the more difficult it is to achieve complete removal of cholesteatoma. Abreu et al. have classified the depth of the sinus tympani into three types as follows: small (type A), deep (type B), and deep with a posterior extension (type C) (Fig. 16.28) [84].

Classification of sinus tympani, promontory (PR), sinus tympani (ST), facial nerve (Nf). (Adapted from Abreu et al. (2015) Endoscopic Ear Surgery: Principles Indications and Techniques [84])
16.19.4 Hypotympanum
It is the inferior compartment of the tympanic cavity, located anteriorly and inferiorly to the retrotympanum. Its inferior limit is formed by the floor of the tympanic cavity and jugular bulb; its upper limit is a virtual plane passing through the styloid eminence and continuing to the inferior margin of the EAC. The hypotympanum floor has an irregular surface due to osseous trabeculae and small irregular tympanic cells [82].
16.20 Complications, Challenges, and Prognosis
Possible complications of transmastoid procedures include recurrent infection, wound dehiscence, dysgeusia, hearing loss, vestibular deficit, and facial palsy. Canal wall down procedures are more morbid. CFS leak and intracranial infection like meningitis could occur in those procedures when the internal ear is manipulated, or the dura is opened. Failure of the device is a relatively common complication of cochlear implant surgery. Due to the extent of the IFT approach, possible complications are hearing loss, facial palsy, lower CN (IX, X, XI, XII) palsy, internal carotid artery bleeding, and venous infarction with intracranial hypertension.
Due to the deleterious impact on the patient’s quality of life, facial palsy is a highly feared complication by the surgeon and the patient. Fortunately, its incidence is low due to higher anatomical knowledge and neuromonitoring. Preservation of hearing, vestibular function, and patients’ ability to perform aquatic activities after temporal bone surgery remain a challenge in different situations, mainly after surgery of chronic otitis media with cholesteatoma. Currently, not only the complete removal of disease but also the preservation of functional status and quality of life are of outermost relevance. Technology advances in imaging techniques and use of endoscopes have achieved excellent control of disease with appropriate functional preservation in selected patients. Indications for cochlear implantation surgery continue to expand, making the surgeon face special situations such as cochlear ossification, implantation after cholesteatoma, and other challenges. The prognosis of temporal bone diseases and tumours mainly depends on the aetiology, location, and size of the lesion.
16.21 Conclusion
The temporal bone is a complex anatomical area, affected by a large number of benign and sinister diseases. Strong anatomical knowledge is essential to reduce complications; technological advances and working with a multidisciplinary team are also appropriate measures for the management of patients with temporal bone diseases. Novice surgeons should properly identify surgical landmarks and eventually perform increasingly complex approaches.
References
Cosetti M, Roland JTJ. Cochlear implantation in the very young child: issues unique to the under-1 population. Trends Amplif. 2010;14(1):46–57. https://doi.org/10.1177/1084713810370039.
Castle JT. Cholesteatoma pearls: practical points and update. Head Neck Pathol. 2018;12(3):419–29. https://doi.org/10.1007/s12105-018-0915-5.
Gulati M, Gupta S, Prakash A, Garg A, Dixit R. HRCT imaging of acquired cholesteatoma: a pictorial review. Insights Imaging. 2019;10(1):92. https://doi.org/10.1186/s13244-019-0782-y.
Kalra VK. Aural polyp is not always due to chronic otitis media (COM): preoperative computed tomographic scan is good pointer for sinister lesions. Indian J Otolaryngol Head Neck Surg. 2018;70(4):505–9. https://doi.org/10.1007/s12070-018-1482-5.
Karamert R, Eravcı FC, Cebeci S, Düzlü M, Zorlu ME, Gülhan N, et al. Canal wall down versus canal wall up surgeries in the treatment of middle ear cholesteatoma. Turk J Med Sci. 2019;49(5):1426–32. https://doi.org/10.3906/sag-1904-109.
Bakaj T, Zbrozkova LB, Salzman R, Tedla M, Starek I. Recidivous cholesteatoma: DWI MR after canal wall up and canal wall down mastoidectomy. Bratislavske lekarske listy. 2016;117(9):515–20. https://doi.org/10.4149/BLL_2016.
Hu Y, Teh BM, Hurtado G, Yao X, Huang J, Shen Y. Can endoscopic ear surgery replace microscopic surgery in the treatment of acquired cholesteatoma? A contemporary review. Int J Pediatr Otorhinolaryngol. 2020;131:109872. https://doi.org/10.1016/j.ijporl.2020.109872.
Orhan KS, Çelik M, Polat B, Aydemir L, Aydoseli A, Sencer A, et al. Endoscope-assisted surgery for petrous bone cholesteatoma with hearing preservation. J Int Adv Otol. 2019;15(3):391–5. https://doi.org/10.5152/iao.2019.7212.
Gordin E, Lee TS, Ducic Y, Arnaoutakis D. Facial nerve trauma: evaluation and considerations in management. Craniomaxillofac Trauma Reconstr. 2015;8(1):1–13. https://doi.org/10.1055/s-0034-1372522.
Diaz RC, Cervenka B, Brodie HA. Treatment of temporal bone fractures. J Neurol Surg B Skull Base. 2016;77(5):419–29. https://doi.org/10.1055/s-0036-1584197.
Vajpayee D, Mallick A, Mishra AK. Post temporal bone fracture facial paralysis: strategies in decision making and analysis of efficacy of surgical treatment. Indian J Otolaryngol Head Neck Surg. 2018;70(4):566–71. https://doi.org/10.1007/s12070-018-1371-y.
Xie S, Wu X, Zhang Y, Xu Z, Yang T, Sun H. The timing of surgical treatment of traumatic facial paralysis: a systematic review. Acta Otolaryngol. 2016;136(12):1197–200. https://doi.org/10.1080/00016489.2016.1201862.
Abbaszadeh-Kasbi A, Kouhi A, Ashtiani MTK, Anari MR, Yazdi AK, Emami H. Conservative versus surgical therapy in managing patients with facial nerve palsy due to the temporal bone fracture. Craniomaxillofac Trauma Reconstr. 2019;12(1):20–6. https://doi.org/10.1055/s-0038-1625966.
Johnson F, Semaan MT, Megerian CA. Temporal bone fracture: evaluation and management in the modern era. Otolaryngol Clin N Am. 2008;41(3):597–618. https://doi.org/10.1016/j.otc.2008.01.006.
Szyfter W, Karlik M, Sekula A, Harris S, Gawęcki W. Current indications for cochlear implantation in adults and children. Otolaryngologia polska (Pol Otolaryngol). 2019;73(3):1–5. https://doi.org/10.5604/01.3001.0013.1000.
Santa Maria PL, Gluth MB, Yuan Y, Atlas MD, Blevins NH. Hearing preservation surgery for cochlear implantation: a meta-analysis. Otol Neurotol. 2014;35(10):e256–69. https://doi.org/10.1097/MAO.0000000000000561.
Lesser JCC, de Brito Neto RV, de Souza Queiroz Martins G, Bento RF. Cochlear implantation through the middle fossa approach: a review of related temporal bone studies and reported cases. Int Arch Otorhinolaryngol. 2017;21(1):102–8. https://doi.org/10.1055/s-0036-1582266.
Lopez-Escamez JA, Carey J, Chung W-H, Goebel JA, Magnusson M, Mandalà M, et al. Diagnostic criteria for Menière’s disease. J Vestib Res. 2015;25(1):1–7. https://doi.org/10.3233/VES-150549.
Perkins E, Rooth M, Dillon M, Brown K. Simultaneous labyrinthectomy and cochlear implantation in unilateral Meniere’s disease. Laryngoscope Investig Otolaryngol. 2018;3(3):225–30. https://doi.org/10.1002/lio2.163.
Kitahara T. Evidence of surgical treatments for intractable Meniere’s disease. Auris Nasus Larynx. 2018;45(3):393–8. https://doi.org/10.1016/j.anl.2017.07.016.
Thomsen J, Bonding P, Becker B, Stage J, Tos M. The non-specific effect of endolymphatic sac surgery in treatment of Meniere’s disease: a prospective, randomized controlled study comparing “classic” endolymphatic sac surgery with the insertion of a ventilating tube in the tympanic membrane. Acta Otolaryngol. 1998;118(6):769–73.
Bretlau P, Thomsen J, Tos M, Johnsen NJ. Placebo effect in surgery for Menière’s disease: nine-year follow-up. Am J Otol. 1989;10(4):259–61.
Pillsbury HC 3rd, Arenberg IK, Ferraro J, Ackley RS. Endolymphatic sac surgery. The Danish sham surgery study: an alternative analysis. Otolaryngol Clin N Am. 1983;16(1):123–7.
Sood AJ, Lambert PR, Nguyen SA, Meyer TA. Endolymphatic sac surgery for Ménière’s disease: a systematic review and meta-analysis. Otol Neurotol. 2014;35(6):1033–45. https://doi.org/10.1097/MAO.0000000000000324.
Welling DB, Nagaraja HN. Endolymphatic mastoid shunt: a reevaluation of efficacy. Otolaryngol Head Neck Surg. 2000;122(3):340–5. https://doi.org/10.1067/mhn.2000.101575.
Devantier L, Schmidt JH, Djurhuus BD, Hougaard DD, Händel MN, Liviu-Adelin Guldfred F, et al. Current state of evidence for endolymphatic sac surgery in Menière’s disease: a systematic review. Acta Otolaryngol. 2019;139(11):953–8. https://doi.org/10.1080/00016489.2019.1657240.
de Lourdes Flores García M, de la Llata Segura C, Lesser JCC, Pianese CP. Endolymphatic sac surgery for Ménière’s disease—current opinion and literature review. Int Arch Otorhinolaryngol. 2017;21(2):179–83. https://doi.org/10.1055/s-0037-1599276.
Minor LB, Solomon D, Zinreich JS, Zee DS. Sound- and/or pressure-induced vertigo due to bone dehiscence of the superior semicircular canal. Arch Otolaryngol Head Neck Surg. 1998;124(3):249–58. https://doi.org/10.1001/archotol.124.3.249.
Welgampola MS, Myrie OA, Minor LB, Carey JP. Vestibular-evoked myogenic potential thresholds normalize on plugging superior canal dehiscence. Neurology. 2008;70(6):464–72. https://doi.org/10.1212/01.wnl.0000299084.76250.4a.
Zan E, Limb CJ, Koehler JF, Yousem DM. Middle ear adenoma: a challenging diagnosis. AJNR Am J Neuroradiol. 2009;30(8):1602–3. https://doi.org/10.3174/ajnr.A1534.
Touska P, Juliano AF-Y. Temporal bone tumors: an imaging update. Neuroimaging Clin N Am. 2019;29(1):145–72. https://doi.org/10.1016/j.nic.2018.09.007.
Saliba I, Evrard AS. Middle ear glandular neoplasms: adenoma, carcinoma or adenoma with neuroendocrine differentiation: a case series. Cases J. 2009;2(3):1–8. https://doi.org/10.1186/1757-1626-2-6508.
Leong K, Haber MM, Divi V, Sataloff RT. Neuroendocrine adenoma of the middle ear (NAME). Ear Nose Throat J. 2009;88(4):874–9.
Mundada P, Purohit BS, Kumar TS, Tan TY. Imaging of facial nerve schwannomas: diagnostic pearls and potential pitfalls. Diagn Intervent Radiol (Ankara, Turkey). 2016;22(1):40–6.
Lin EP, Crane BT. The management and imaging of vestibular schwannomas. Am J Neuroradiol. 2017;38(11):2034–43.
Düzlü M, Tutar H, Karamert R, Karaloğlu F, Şahin MM, Göcek M, et al. Temporal bone paragangliomas: 15 years’ experience. Braz J Otorhinolaryngol. 2016;84:58–65. https://doi.org/10.1016/j.bjorl.2016.11.001.
Jackson CG, Glasscock ME 3rd, Harris PF. Glomus tumors. Diagnosis, classification, and management of large lesions. Arch Otolaryngol (Chicago, Ill: 1960). 1982;108(7):401–10. https://doi.org/10.1001/archotol.1982.00790550005002.
Oldring D, Fisch U. Glomus tumors of the temporal region: surgical therapy. Am J Otol. 1979;1(1):7–18.
Moe KS, Li D, Linder TE, Schmid S, Fisch U. An update on the surgical treatment of temporal bone paraganglioma. Skull Base Surg. 1999;9(3):185–94. https://doi.org/10.1055/s-2008-1058145.
Jansen TTG, Kaanders JHAM, Beute GN, Timmers HJLM, Marres HAM, Kunst HPM. Surgery, radiotherapy or a combined modality for jugulotympanic paraganglioma of Fisch class C and D. Clin Otolaryngol. 2018;43(6):1566–72. https://doi.org/10.1111/coa.13216.
Al-Mefty O, Teixeira A. Complex tumors of the glomus jugulare: criteria, treatment, and outcome. J Neurosurg. 2002;97(6):1356–66. https://doi.org/10.3171/jns.2002.97.6.1356.
de Brito R, Cisneros Lesser JC, Lopes PT, Bento RF. Preservation of the facial and lower cranial nerves in glomus jugulare tumor surgery: modifying our surgical technique for improved outcomes. Eur Arch Otorhinolaryngol. 2018;275(8):1963–9. https://doi.org/10.1007/s00405-018-5026-0.
Lionello M, Stritoni P, Facciolo MC, Staffieri A, Martini A, Mazzoni A, et al. Temporal bone carcinoma. Current diagnostic, therapeutic, and prognostic concepts. J Surg Oncol. 2014;110(4):383–92. https://doi.org/10.1002/jso.23660.
Gidley PW, DeMonte F. Temporal bone malignancies. Neurosurg Clin N Am. 2013;24(1):97–110. https://doi.org/10.1016/j.nec.2012.08.009.
Franciszek B. Benign and malignant tumours of the ear and temporal bone. In: Rozylo-Kalinowska I, Orhan K, editors. Imaging of the temporomandibular joint. Cham: Springer; 2019. https://doi.org/10.1007/978-3-319-99468-0_18.
da Silva AP, Breda E, Monteiro E. Malignant tumors of the temporal bone—our experience. Braz J Otorhinolaryngol. 2016;82(4):479–83. https://doi.org/10.1016/j.bjorl.2015.09.010.
Beyea JA, Moberly AC. Squamous cell carcinoma of the temporal bone. Otolaryngol Clin N Am. 2015;48(2):281–92. https://doi.org/10.1016/j.otc.2014.12.003.
Arriaga M, Curtin H, Takahashi H, Hirsch BE, Kamerer DB. Staging proposal for external auditory meatus carcinoma based on preoperative clinical examination and computed tomography findings. Ann Otol Rhinol Laryngol. 1990;99(9 Pt 1):714–21. https://doi.org/10.1177/000348949009900909.
Moody SA, Hirsch BE, Myers EN. Squamous cell carcinoma of the external auditory canal: an evaluation of a staging system. Am J Otol. 2000;21(4):582–8.
Nabuurs CH, Kievit W, Labbé N, Leemans CR, Smit CFGM, van den Brekel MWM, et al. Evaluation of the modified Pittsburgh classification for predicting the disease-free survival outcome of squamous cell carcinoma of the external auditory canal. Head Neck. 2020;42(12):3609–22. https://doi.org/10.1002/hed.26424.
Morita S, Mizumachi T, Nakamaru Y, Sakashita T, Kano S, Hoshino K, et al. Comparison of the University of Pittsburgh staging system and the eighth edition of the American Joint Committee on Cancer TNM classification for the prognostic evaluation of external auditory canal cancer. Int J Clin Oncol. 2018;23(6):1029–37. https://doi.org/10.1007/s10147-018-1314-3.
Halmagyi GM, Chen L, MacDougall HG, Weber KP, McGarvie LA, Curthoys IS. The video head impulse test. Front Neurol. 2017;8:258. https://doi.org/10.3389/fneur.2017.00258.
Venhovens J, Meulstee J, Verhagen WIM. Vestibular evoked myogenic potentials (VEMPs) in central neurological disorders. Clin Neurophysiol. 2016;127(1):40–9. https://doi.org/10.1016/j.clinph.2014.12.021.
Ng JH, Zhang EZ, Soon SR, Tan VYJ, Tan TY, Mok PKH, et al. Pre-operative high resolution computed tomography scans for cholesteatoma: has anything changed? Am J Otolaryngol. 2014;35(4):508–13. https://doi.org/10.1016/j.amjoto.2014.02.015.
Marquet JFE. Surgery and pathology of the middle ear. In: Marquet JFE, editor. Proceedings of the international conference on ‘The Postoperative Evaluation in Middle Ear Surgery’ held in Antwerp on June 14–16, 1984. 1st ed. Dordrecht: Springer; 1985. p. 424.
Shekhar C, Bhavana K. Aesthetics in ear surgery: a comparative study of different post auricular incisions and their cosmetic relevance. Indian J Otolaryngol Head Neck Surg. 2007;59(2):187–90. https://doi.org/10.1007/s12070-007-0057-7.
Barrett G, Koecher S, Ronan N, Whinney D. Patient satisfaction with postaural incision site. Int J Otolaryngol. 2014;2014:851980. https://doi.org/10.1155/2014/851980.
Brackmann DE, Shelton C, Arriaga MA. Otologic surgery. 3rd ed. Philadelphia: Saunders/Elsevier; 2010.
Lempert J. Endaural, antauricular surgical approach to the temporal bone: principles involved in this new approach; summary report of 1,780 cases. Arch Otolaryngol. 1938;27(5):555–87. https://doi.org/10.1001/archotol.1938.00650030568004.
Pennings RJE, Cremers CWRJ. Postauricular approach atticotomy: a modified closed technique with reconstruction of the scutum with cymbal cartilage. Ann Otol Rhinol Laryngol. 2009;118(3):199–204. https://doi.org/10.1177/000348940911800307.
Isaacson B. Anatomy and surgical approach of the ear and temporal bone. Head Neck Pathol. 2018;12(3):321–7. https://doi.org/10.1007/s12105-018-0926-2.
Schwartze E. Ueber die künstliche Eröffnung des Warzenfortsatzes. Archiv für Ohrenheilkunde. 2005;7:157–62.
Bento RF, de Oliveira Fonseca AC. A brief history of mastoidectomy. Int Arch Otorhinolaryngol. 2013;17(2):168–78. https://doi.org/10.7162/S1809-97772013000200009.
Aslan A, Mutlu C, Celik O, Govsa F, Ozgur T, Egrilmez M. Surgical implications of anatomical landmarks on the lateral surface of the mastoid bone. Surg Radiol Anat. 2004;26(4):263–7. https://doi.org/10.1007/s00276-004-0235-1.
Yilmazer R, Baskadem Yilmazer A, Hoffer ME, Eshraghi AA, Telischi FF, Angeli SI. A new technique to find the facial nerve and recess by using the short process of the incus and the spine of Henle as landmarks: incus-spine angle. Acta Otolaryngol. 2018;138(11):1051–6. https://doi.org/10.1080/00016489.2018.1504168.
Comrie JD. Section of the history of medicine. Br Med J. 1927;2(3474):205–10. https://doi.org/10.1136/bmj.2.3474.205.
Goycoolea MV. Mastoid and tympanomastoid procedures in otitis media: classic mastoidectomy (simple, modified, and radical) and current adaptations; open-cavity, closed-cavity, and intact-bridge tympanomastoidectomy. Otolaryngol Clin N Am. 1999;32(3):513–23. https://doi.org/10.1016/S0030-6665(05)70149-3.
Luers JC, Hüttenbrink K-B. Surgical anatomy and pathology of the middle ear. J Anat. 2016;228(2):338–53. https://doi.org/10.1111/joa.12389.
Irugu DVK, Singh A, Kumar R. Morphometry of the digastric ridge and its significance for mastoid surgeries—a cadaveric study. Ear Nose Throat J. 2021;100(6):NP296–8. https://doi.org/10.1177/0145561319870491.
Toros SZ, Karaca CT, Habeşoğlu TE, Noşeri H, Ertugay CK, Naiboğlu B, et al. Is there a relation between mastoid aeration and Körner’s septum? Eur Arch Otorhinolaryngol. 2010;267(10):1523–6. https://pubmed.ncbi.nlm.nih.gov/20480369/
Przewoźny TT, Kosiński A, Markiet K, Sierszeń W, Kuczkowski J, Kuryłowicz J, et al. Körner’s septum (petrosquamosal lamina): the anatomical variant or clinical problem? Folia Morphol. 2020;79(2):205–10. https://doi.org/10.5603/FM.a2019.0079.
Williamson SL, Rini DA. In: Francis HW, Niparko JK, editors. Temporal bone dissection guide. 2011th-1st ed. Stuttgart: Georg Thieme Verlag; 2011. Available from: http://www.thieme-connect.de/products/ebooks/book/10.1055/b-002-74277.
Bittencourt AG, Burke PR, de Souza Jardim I, de Brito R, Tsuji RK, de Oliveira Fonseca AC, et al. Implantable and semi-implantable hearing AIDS: a review of history, indications, and surgery. Int Arch Otorhinolaryngol. 2014;18(3):303–10. https://doi.org/10.1055/s-0033-1363463.
Arnoldner C, Lin VYW, Chen JM. Cortical mastoidectomy. In: Manual of otologic surgery. Vienna: Springer; 2015. p. 5–13. https://doi.org/10.1007/978-3-7091-1490-2_2.
Prasad SC, Roustan V, Piras G, Caruso A, Lauda L, Sanna M. Subtotal petrosectomy: surgical technique, indications, outcomes, and comprehensive review of literature. Laryngoscope. 2017;127(12):2833–42. https://doi.org/10.1002/lary.26533.
Cruz OLM, Tedeschi H, Rhoton AL Jr. In: Flint PW, Haughey BH, Robbins KT, Thomas JR, Niparko JK, Lund VJ, et al., editors. Cummings otolaryngology—head and neck surgery. Philadelphia: Elsevier Health Sciences; 2014. p. 2662–70. https://doi.org/10.1016/B978-1-4557-4696-5.00173-1.
Angeli S. Middle fossa approach: indications, technique, and results. Otolaryngol Clin N Am. 2012;45(2):417–38. https://doi.org/10.1016/j.otc.2011.12.010.
Schick B, Dlugaiczyk J. Surgery of the ear and the lateral skull base: pitfalls and complications. GMS Curr Top Otorhinolaryngol Head Neck Surg. 2013;12:Doc05. https://doi.org/10.3205/cto000097.
Fisch U. Infratemporal fossa approach to tumours of the temporal bone and base of the skull. J Laryngol Otol. 1978;92(11):949–67.
Marchioni D, Rubini A, Nogueira JF, Isaacson B, Presutti L. Transcanal endoscopic approach to lesions of the suprageniculate ganglion fossa. Auris Nasus Larynx. 2018;45(1):57–65. https://doi.org/10.1016/j.anl.2017.03.006.
Marchioni D, Molteni G, Presutti L. Endoscopic anatomy of the middle ear. Indian J Otolaryngol Head Neck Surg. 2011;63(2):101–13. https://doi.org/10.1007/s12070-011-0159-0.
Isaacson G. Endoscopic anatomy of the pediatric middle ear. Otolaryngol Head Neck Surg. 2014;150(1):6–15. https://doi.org/10.1177/0194599813509589.
Marchioni D, Alicandri-Ciufelli M, Mattioli F, Nogeira JF, Tarabichi M, Villari D, et al. From external to internal auditory canal: surgical anatomy by an exclusive endoscopic approach. Eur Arch Otorhinolaryngol. 2013;270(4):1267–75. https://doi.org/10.1007/s00405-012-2137-x.
Abreu JPS, Alicandri-Ciufelli M, Artioli FL, Ayache S, Badr-El-Dine MMK, Cunsolo EM, et al. Endoscopic ear surgery. In: Presutti L, Marchioni D, editors. Principles, indications, and techniques. Stuttgart: Georg Thieme Verlag; 2015. Available from: http://www.thieme-connect.de/products/ebooks/book/10.1055/b-003-121086.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Ramírez Arroyo, G., Tella Vega, C., Monroy Llaguno, D.A., Cisneros Lesser, J.C. (2022). Temporal Bone Diseases and Tumours and Its Related Surgery. In: Mat Lazim, N., Mohd Ismail, Z.I., Abdullah, B. (eds) Head and Neck Surgery : Surgical Landmark and Dissection Guide. Springer, Singapore. https://doi.org/10.1007/978-981-19-3854-2_16
Download citation
DOI: https://doi.org/10.1007/978-981-19-3854-2_16
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-19-3853-5
Online ISBN: 978-981-19-3854-2
eBook Packages: MedicineMedicine (R0)