
Abstract
Recently, lumbar interbody fusion by unilateral biportal endoscopy (UBE lumbar interbody fusion [ULIF]) has been developed and published by several studies that have demonstrated its various advantages compared with conventional PLIF/TLIF. ULIF is as effective as conventional PLIF/TLIF in terms of the fusion rate and clinical outcomes. Individual advantages of ULIF over conventional PLIF/TLIF include: (1) reduced intraoperative bleeding, (2) less postoperative back pain, (3) meticulous endplate preparation under endoscopic view, (4) magnified and clear surgical view, (5) less paraspinal muscle injury, and (6) achieve direct neural decompression of central and foraminal stenosis. However, in order to safely and effectively perform ULIF, there are several surgical tips that need to be taken into account at each stage of ULIF. This chapter aims to describe the surgical techniques and tips of ULIF.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Gold standard techniques such as transforaminal lumbar interbody fusion (TLIF) or posterior lumbar interbody fusion (PLIF), conventionally used for the treatment of degenerative lumbar spinal disease, have disadvantages, such as postoperative back pain as well as paraspinal muscle atrophy due to paraspinal muscle dissection or retraction [1, 2].
Recently, a technique for lumbar interbody fusion by unilateral biportal endoscopy (UBE lumbar interbody fusion [ULIF]) has been developed and published by several studies that have demonstrated its various advantages compared with conventional PLIF/TLIF, while reporting competent clinical outcomes as well as fusion rates [3,4,5,6]. In this technique, independent movement of the surgical instruments and endoscope is possible because the working portal, and not the working cannula, is utilized for surgical instruments [3]. Consequently, direct neural decompression of the central and foraminal stenosis is possible with less limitation of movement and vision [3, 7]. As the cage is inserted through the working portal, and not through the working cannula, large-sized cages can be inserted into the intervertebral space [3]. Moreover, ULIF can provide a familiar surgical view and high magnification/clearing by continuous irrigation for safe and effective surgery [5]. Additionally, ULIF can achieve meticulous endplate preparation and reduce the probability of bony endplate injury, which can be confirmed under endoscopic view [5, 7]. Furthermore, because of ULIF’s advantageous minimal invasiveness, patients have less postoperative back pain [3,4,5].
In order to safely and effectively perform ULIF, there are surgical tips that need to be taken into account at each stage of the procedure. This chapter aims to describe the surgical technique of ULIF.
2 Indications and Contraindications
The indications of ULIF are similar to those for conventional PLIF/TLIF.
The indications for ULIF are as follows:
-
1.
Grade 1 or 2 degenerative or isthmic spondylolisthesis
-
2.
Central or foraminal stenosis with instability
-
3.
Recurrent disc herniation
The contraindications for ULIF are as follows:
-
1.
High-grade spondylolisthesis (grade 3 or 4)
-
2.
Spinal deformity
-
3.
Vertebral fractures
-
4.
Spondylodiscitis
3 Special Instruments
Most of the instruments used during ULIF are similar to other surgeries by UBE. However, some instruments specially designed for ULIF are also available and could be safe.
-
1.
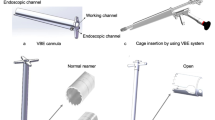
Semi-tubular retractor: Semi-tubular retractor keep continuous fluid output and guide the instrument to the operation field during operation (Fig. 12.1a). In addition to semi-tubular retractor, a working sheath can also be used to keep continuous fluid output.
-
2.
Hook radiofrequency probe: It is used for coagulation of focal epidural vessels or annulotomy (Fig. 12.1b).
-
3.
Funnel and Funnel pusher: Insertion of bone graft is performed through a specialized bone graft funnel (Fig. 12.1c).
-
4.
Serial dilator bars (11 mm, 13 mm, 15 mm): Prior to cage insertion, serial dilatation of paraspinal muscle can be achieved by using bar dilators to make it easier for insertion of the cage (Fig. 12.1d).
-
5.
Specilized root retractor: Thecal sac and nerve root can be protected with a specialized root retractor during cage insertion, which is anchored at lower vertebral body edge (Fig. 12.1e).
-
6.
Endplate removers: Specialized various angles of endplate removers are useful for endplate preparation, especially in contralateral side (Fig. 12.1f).


Special instruments for lumbar interbody fusion by unilateral biportal endoscopy. Semi-tubular retractor (a), hook radiofrequency probe (b), funnel and funnel pusher (c), serial dilator bars (d), specialized root retractor (e), endplate removers (f)
4 Anesthesia and Position
Patients are prepared in the prone position under general or epidural anesthesia. Generally, the left side is preferred for a right-handed spine surgeon, as it becomes easy to take surgical instruments from the nurse. However, in the case of high lordotic angle of surgical level, such as L5–S1 level, or when direct neural decompression of right foraminal stenosis is needed, right-side approach is a better alternative.
5 Surgical Steps
5.1 Skin Marking and Making Portal
Once the patient is positioned, intraoperative fluoroscopy is used to confirm the level of operation. Lower endplate line of upper vertebral body should be parallel under C-arm fluoroscopy guidance. The docking point is identified by using an anteroposterior view of C-arm fluoroscopy as the lower part of the cranial lamina. Two incisions are made, about 3 cm apart, with the center being the lower part of the cranial lamina at the midline of the proximal and distal pedicles. A transverse skin incision is made cranially for the endoscopic portal; another skin incision is made caudally for the working portal (Fig. 12.2a). Skin incisions may need to be further lateral and wide in obese patients. Each incision will be used for percutaneous pedicle screw insertion at the end of operation. If multi-level fusion is planned, the cranial endoscopic portals can be used in the working portal for the next-level ULIF.

Skin incision and docking point on the fluoroscopic anteroposterior view. The docking point (white circle) is the lower part of the cranial lamina. Two skin incisions (white line) are made about 3 cm apart, with the center being the lower part of the cranial lamina at the midline of the proximal and distal pedicles (dotted line) (a). The positioning of the endoscope and surgical instruments with semi-tubular retractor through each portal. A photo in the surgical field (b), fluoroscopic view (c)
Once the skin incision is made, the 15-blade is used to make incision in the lumbosacral fascia, enough to insert the serial tube dilators and the endoscopic sheath. After the fascia is opened, the serial tube dilators and the endoscopic sheath, which make triangulation, are placed at the target lamina. Triangulation of the endoscope and surgical instruments with semi-tubular retractor is crucial to visualize the surgical field and to manipulate the instruments with less motion and vision limitation (Fig. 12.2b, c). Using the muscle detacher, the surgeon is able to feel the base of the spinous process as well as the cranial lamina and the facet joint.
5.2 Initial Working Space and Bone Working (Fig. 12.3 and Video 12.1)
After positioning the endoscope and the semi-tubular retractor through each portal, the initial working space is made under endoscopic guidance. Once soft tissue overlying the cranial lamina is coagulated using RF probe, the inferior edge of the cranial lamina and the interlaminar space is identified (Fig. 12.3a). At this point, ipsilateral laminotomy can be performed by using round cutting burr or Kerrison punch. It is preferable not to use a burr, but rather to use Kerrison punch or osteotome to collect the auto bone for bone grafting. Typically, the ligamentum flavum (LF) is left as a protector to avoid neural injury or dural tear until bone working is finished. Laminotomy of the cranial lamina should be performed until exposure of cranial end of the LF (Fig. 12.3b, c). After finishing ipsilateral laminotomy, the inferior articular process (IAP) of the upper vertebra is removed by multiple osteotomies to save the autograft material (Fig. 12.3d, e). If the size of the bone chip is large, it may be difficult to remove through working portal or may cause paraspinal muscle injury. After satisfactory bone working is performed at the ipsilateral side, the bone working is done toward the contralateral side.


Serial sequence endoscopic images of the bone working. The surgical anatomy is first noticed in the inferior edge of the cranial lamina and the interlaminar space (a). Anatomical landmark for cranial bone working. The dotted line indicates cranial end of the ligamentum flavum of ipsilateral side (b) and contralateral side (c). Removal of inferior articular process by osteotome (d) and identification of the articular surfaces of superior articular process (e). Removal of the base of the spinous process for contralateral decompression. The dotted line indicates midline (f). Removal of inferior articular process by osteotome at contralateral side (g)
A contralateral decompression can be performed through sublaminar approach; the base of the spinous process and contralateral lamina are removed utilizing a round cutting burr or osteotome (Fig. 12.3f). It is important to sufficiently remove the base of spinous process to obtain working space because the base of the spinous process interrupts the manipulation of the endoscope and the surgical instruments. The contralateral facectectomy through sublaminar approach provides release, which helps in reduction of spondylolisthesis and making lordosis (Fig. 12.4a). When the IAP is caudally removed with an osteotome from the tip of IAP, the facet joint surface can be confirmed (Fig. 12.3g). When the facet joint osteophytes are prominent or greater reduction of spondylolisthesis is required, two new portals are created on the contralateral side to perform total removal of IAP (Fig. 12.4b).

Two types of contralateral facectectomy in lumbar interbody fusion by UBE. Contralateral facectectomy through sublaminar approach (a). When the facet joint osteophytes are prominent or greater reduction of spondylolisthesis is required, two new portals are created on the contralateral side to perform total removal of IAP (b)
5.3 Partial Removal of Superior Articular Process and Identification of Disc Space (Fig. 12.5 and Video 12.2)
After removing the superficial layer of ipsilateral LF, the upper portion of the caudal lamina and medial aspect of the superior articular process (SAP) could be identified (Fig. 12.5a, b). The upper portion of the caudal lamina is partially removed with Kerrison punch, continuing along the medial margins of the SAP and detachment of the deep layer of the LF (Fig. 12.5c). The medial aspect of SAP should be removed sufficiently to make space for insertion of the cage. Inadequate resection of SAP could induce retraction-related neurapraxia when the cage is inserted. When the distance from lateral margin of thecal sac to the remaining ledge of the SAP is at least 8 mm, the cage can be safely placed without retraction-related neurapraxia (Fig. 12.5d). Once the deep layer of ipsilateral LF is partially removed, the lateral margin of thecal sac, ipsilateral traversing nerve root, pedicle of lower vertebra, and disc space could be identified (Fig. 12.5e). We do not attempt to fully expose the ipsilateral exiting nerve root before cage insertion because this helps to protect the exiting nerve root from neural injury during cage insertion.


Endoscopic images showing the sequential steps of partial removal of superior articular process and identification of disc space. Detachment of the superficial layer of ligamentum flavum from caudal lamina (a). Exposure of the upper portion of the caudal lamina and medial margin of the superior articular process (white dotted curved line) (b). The upper portion of the caudal lamina is partially removed with Kerrison punch, continuing along the medial margins of the superior articular process (white dotted curved line) (c). When the distance from lateral margin of thecal sac to the remaining ledge of the SAP (double-ended arrow) is at least 8 mm, the cage can be safely placed (d). Identification of ipsilateral traversing nerve root, pedicle of lower vertebra, and disc space could be identified (e)
5.4 Annulotomy and Endplate Preparation (Fig. 12.6 and Video 12.2)
After exposing the ipsilateral disc space, epidural vessels above the annulus are coagulated. Annulotomy can be performed using hook RF probe with attention to protecting the thecal sac and nerve root (Fig. 12.6a). Then, Kerrison punch is used to remove the annulus fibrosus, making the disc space more release (Fig. 12.6b). The nucleus pulposus and cartilaginous endplate are removed using a combination of angled endplate removers and pituitary forceps. Meticulous endplate preparation is crucial for good arthrodesis, and special care should be taken to remove most of the cartilaginous endplate without bony endplate injury, which can prevent the subsidence of the cage into the vertebral body. Detachment of the cartilaginous endplate from the bony endplate can be performed by utilizing a variety of angled endplate removers (Fig. 12.6c). Care should be taken to adequately remove disc material and cartilaginous endplate at the contralateral side, so that the cage is able to be inserted at the contralateral side. With the help of angled endplate removers and curved pituitary forceps, contralateral endplate preparation could be achieved under endoscopic guidance. Using the 30° scope allows more endplate preparation at contralateral side. Generally, about 70%–80% of the disc space could be prepared for fusion with ULIF. In patients with high-grade spondylolisthesis or significant disc narrowing, it may be difficult to perform endplate preparation and cage insertion. In such cases, upper edge of lower vertebral body is removed with an osteotome to obtain a larger entry (Fig. 12.6d). By having a magnified endoscopic view, surgeons can make sure when the meticulous endplate preparation is complete (Fig. 12.6e).

Endoscopic images showing the steps in order of annulotomy and endplate preparation. Annulotomy using hook radiofrequency probe (a). Kerrison punch is used to remove the annulus fibrosus, making the disc space more release (b). The cartilaginous endplate can be detached from the bony endplate using endplate remover (c). Removal of upper edge of lower vertebral body (dotted circle) using an osteotome, which aids in easier cage insertion and prevents exiting root injury (d). Confirmation of meticulous endplate preparation (e)
5.5 Bone Grafting and Cage Insertion (Fig. 12.7 and Video 12.3)
When placing bone graft or inserting the cage, fluid should be stopped to prevent loss of bone chip by continuous irrigation. After sufficient endplate preparation, insertion of bone graft is performed using specialized bone graft funnel, which is checked on fluoroscopy (Figs. 12.1c and 12.7a, b). Autologous and allogenous bone grafts can be compacted into the anterior portion of the disc space through specialized bone graft funnel. Prior to cage insertion, dilatation of paraspinal muscle can be achieved by using bar dilators to make it easier for insertion of the cage (Figs. 12.1d and 12.7c). Under fluoroscopic guidance during cage insertion in ULIF, a blind space is made; thecal sac and nerve root can be protected with a specialized root retractor, anchored at lower vertebral body edge (Figs. 12.1e and 12.7d, e). The cage is then placed transversely using a cage impactor with the aid of fluoroscopy (Fig. 12.7f). Cage should be located between the anterior portion of the disc space on the lateral fluoroscopic image, and centrally place on the anteroposterior fluoroscopic image, which provides segmental lordosis. After insertion of the cage, Gelfoam is applied to the annulotomy site to reduce loss of bone graft and bleeding from the bony endplate (Fig. 12.7g).


Intraoperative images showing the sequential steps of bone grafting and cage insertion. Bone grafts can be compacted into the anterior portion of the disc space through specialized bone graft funnel. A photo in the surgical field (a), Lateral fluoroscopic images (b). Prior to cage insertion, dilatation of paraspinal muscle can be achieved by using bar dilators to make it easier for insertion of the cage (c). Thecal sac and nerve root can be protected with a specialized root retractor (asterisk) during cage insertion, which is anchored at lower vertebral body edge. Endoscopic view (d), Lateral fluoroscopic images (e). Serial sequence fluoroscopic images of the insertion of the cage (f). Gelfoam is placed to reduce loss of bone graft and bleeding from the bony endplate (g)
5.6 Completion of Central and Foraminal Decompression (Fig. 12.8 and Video 12.3)
After finishing the insertion of the cage, the remaining LF is removed to finalize decompression. Once the plane between the dural sac and LF is dissected with freer elevator, the RF probe can be used to detach the LF along the remaining body edge. This technique allows the LF to be removed in an en bloc fashion, and minimizes the usage of Kerrison punch, thereby reducing the risk of a dural tear or neural injury. After removing the LF at the contralateral side, we could identify the contralateral side disc space and traversing nerve root and then complete the central decompression (Fig. 12.8a).

Confirmation of central and foraminal decompression under endoscopic guidance. Contralateral traversing nerve root (a), ipsilateral exiting nerve root (b), and contralateral exiting nerve root (c)
If direct neural decompression is required in the ipsilateral and contralateral exiting nerve root, it can be done after placing the cage. In the case of an ipsilateral foraminotomy, the exiting nerve root can be identified by removing the foraminal ligament (Fig. 12.8b). Then, palpate the upper vertebral pedicle and remove the inferior aspect of transverse process and the tip of SAP following the exiting nerve root. Decompression of the contralateral exiting nerve root could also be performed using the contralateral sublaminar approach. When the tip of the SAP on contralateral side is removed with a curved osteotome or curved Kerrison punch and then the foraminal ligament is removed, the contralateral exiting nerve root can be identified (Fig. 12.8c). The nerve root and thecal sac can be identified by good pulsation, which is the end point of decompression.
5.7 Insertion of Postoperative Drainage and Percutaneous Pedicle Screw Fixation
Jackson–Pratt surgical drain (100 cc) is required after operation to prevent postoperative hematoma. As the drain’s line is irritated when the pedicle screw is inserted, Jackson–Pratt surgical drain is inserted through a subcutaneous tunnel created at the medial side of the caudal skin incision. Two ipsilateral incisions are performed for percutaneous pedicle screw insertion. The ULIF is completed with percutaneous pedicle screws.
5.8 Postoperative Care
The patient is mobilized with physical activity the first day after the operation. Postoperative standing radiographs and MRI should be checked on the second day after surgery, which will show the placement of the cage and neural decompression in detail. Jackson–Pratt surgical drain is removed 1 or 2 days postoperatively.
6 Illustrated Cases
6.1 Case 1 (Fig. 12.9)
A 56-year-old female patient complained of pain in both legs and neurological intermittent claudication for 2 years. Simple lateral radiography showed degenerative spondylolisthesis of L4–5 (Fig. 12.9a). Preoperative MRI showed central stenosis with spondylolisthesis at L4–5 level (Fig. 12.9b, c). We performed the ULIF via left-sided approach. Postoperative lateral radiography presented good reduction of spondylolisthesis (Fig. 12.9d). Postoperative MRI T2-weighted images showed improvement in decompressive status of central stenosis (Fig. 12.9e, f). The patient’s symptoms significantly resolved after surgery.

Images of a 56-year-old woman with both buttock and radiating pain. Preoperative lateral radiography showed degenerative spondylolisthesis of L4–5 (a). Preoperative MR images show central stenosis with spondylolisthesis at L4–5 level (sagittal: b, axial: c). Postoperative lateral radiography and sagittal T2-weighted MRI presented good reduction of spondylolisthesis (d and e). Postoperative axial T2-weighted MRI show enough decompression with minimal paraspinal muscle damage (f)
6.2 Case 2 (Fig. 12.10)
A 71-year-old male patient suffered from right side dominant radicular pain in both legs and neurological intermittent claudication for 1 year. Simple lateral radiography showed isthmic spondylolisthesis at L5–S1 (Fig. 12.10a). The patient’s preoperative T2-weighted sagittal and axial MRI is shown in Fig. 12.10b–d. There was bilateral foraminal stenosis with isthmic spondylolisthesis at L5–S1. The patient underwent ULIF via right-side approach. Postoperative lateral radiography shows good reduction of spondylolisthesis (Fig. 12.10e). Postoperative MRI confirmed that both exiting roots of L5 were well decompressed (Fig. 12.10f–h). He had a significant reduction in radicular leg pain after surgery.

Images of a 71-year-old man with claudication and radicular pain. Preoperative lateral radiography showed isthmic spondylolisthesis of L5-S1 (a). Preoperative MR images show bilateral foraminal stenosis on L5-S1 (sagittal: b (Right) and c (left), axial: d). Postoperative lateral radiography presented complete reduction of spondylolisthesis (e). Postoperative axial T2-weighted MRI shows well decompression of bilateral foraminal stenosis (sagittal: f (right) and g (left), axial: h)
7 Complications and Management
7.1 Dural Tear
Most cases of dural tear can be controlled by fibrin collagen patch (TachoComb). Since most of them are not large enough to suture directly dural tears can be repaired by the application of a fibrin collagen patch (TachoComb) and bed rest for 5 to 7 days. Nonetheless, if dural tear is larger than 10 mm, dural defect should be repaired by suture directly under endoscopy or by conversion to microscopic surgery.
7.2 Postoperative Hematoma
Bleeding from the removed bone is controlled by applying bone wax. Bleeding from the epidural vessels can be coagulated using a hook RF probe. Hemostatic agents, such as soluble hemostatic gauze (WoundClot) or Gelfoam, are useful to control bleeding from hidden bleeding focus. After insertion of the cage, Gelfoam is applied to the annulotomy site to reduce bleeding from the bony endplate. Jackson–Pratt surgical drain (100 cc) is required after operation to prevent postoperative hematoma for 1 or 2 days. If there are neurological symptoms due to postoperative hematoma, hematoma can be removed by UBE using previous portals.
7.3 Fluid-Induced Complications
Headache, neck stiffness, seizure, and retroperitoneal fluid collection are some of the fluid-related complications; therefore caution is important for fluid output as UBE is a fluid medium surgery, and so the fluid-induced complications can be prevented by utilizing a semi-tubular retractor (Fig. 12.1a).
7.4 Cage Subsidence/Retropulsion
When placing the cages, injury of the bony endplate can cause cage subsidence. This complication can be avoided with careful endplate preparation under endoscopic guidance, especially in osteoporosis patients. Using a freer elevator or endplate remover rather than using a currette for endplate preparation may reduce endplate injury. The risk of cage retropulsion is reduced by placing the cage transversely without endplate injury, as well as by performing compression of the pedicle screws while locking the screws.
7.5 Neural Injury
Prevention is the best way to avoid neural injury. It is recommended not to use sharp instruments such as curettes or knife. Also, the RF probe should be used with much caution around neural structures. When using RF probe around the neural structures, surgeons should use it against neural structure with low power. The LF is left as a protector to avoid neural injury until bone working is finished. When the distance from lateral margin of thecal sac to the remaining ledge of the SAP is at least 8 mm, the cage can be safely placed without retraction-related neurapraxia. In placing the cage, thecal sac and nerve root can be protected with a specialized root retractor under fluoroscopic guidance, which reduces the possibility of retraction-related neurapraxia.
8 Surgical Tips and Pitfalls
-
1.
In general, spine surgeons are familiar with left-side approach, but in case of high lordotic angle of surgical level such as L5–S1 level, or when direct neural decompression of right foraminal stenosis is needed, right-side approach is more suitable.
-
2.
When a contralateral decompression can be performed through sublaminar approach, it is important to sufficiently remove the base of the spinous process to obtain working space because the base of the spinous process obstructs the placement of the endoscope and the surgical instruments.
-
3.
The contralateral facectectomy through sublaminar approach provides release, which helps in reduction of spondylolisthesis and making lordosis.
-
4.
When the facet joint osteophytes are prominent or greater reduction of spondylolisthesis is required, two new portals are created on the contralateral side to perform total removal of IAP.
-
5.
As inadequate resection of the medial aspect of SAP can induce neural injury during insertion of the cage, the distance from lateral margin of thecal sac to the remaining ledge of the SAP should be at least 8 mm.
-
6.
When the cage is inserted into the disc space, we do not attempt to fully expose the ipsilateral exiting nerve root because this helps to protect the exiting nerve root.
-
7.
Care should be taken to adequately perform endplate preparation at the contralateral side, so that the cage is able to be inserted from the contralateral side with larger fusion surface area.
-
8.
With the help of angled endplate removers, curved pituitary forceps, and 30° scope, contralateral endplate preparation could be achieved under endoscopic guidance.
-
9.
During endplate preparation, careful attention should be paid not to injure the bony endplate or the anterior longitudinal ligament.
-
10.
In patients with a high-grade spondylolisthesis or significant disc narrowing, removal of upper edge of lower vertebral body using an osteotome aids in easier cage insertion and prevents exiting root injury.
-
11.
It is necessary to avoid continuous irrigation during insertion of bone graft and the cage, in order to prevent bone chip loss.
-
12.
An appropriate cage is inserted under fluoroscopic guidance with a specialized root retractor, which is anchored at lower vertebral body edge, to protect the exposed thecal sac and traversing nerve root.
-
13.
After cage insertion, cage is placed with a cage impactor to ensure it is located in the anterior and central portion of the disc space. To make segmental lordosis, it should be put on the stronger anterior ring apophysis rather than on the soft central cancellous portion.
-
14.
Gelfoam is applied to the annulotomy site to reduce loss of bone chip and bleeding from the bony endplate.
References
Gejo R, Matsui H, Kawaguchi Y, Ishihara H, Tsuji H. Serial changes in trunk muscle performance after posterior lumbar surgery. Spine (Phila Pa 1976). 1999;24(10):1023–8.
Lee KH, Yue WM, Yeo W, Soeharno H, Tan SB. Clinical and radiological outcomes of open versus minimally invasive transforaminal lumbar interbody fusion. Eur Spine J. 2012;21(11):2265–70.
Park MK, Park SA, Son SK, Park WW, Choi SH. Clinical and radiological outcomes of unilateral biportal endoscopic lumbar interbody fusion (ULIF) compared with conventional posterior lumbar interbody fusion (PLIF): 1-year follow-up. Neurosurg Rev. 2019;42(3):753–61.
Heo DH, Park CK. Clinical results of percutaneous biportal endoscopic lumbar interbody fusion with application of enhanced recovery after surgery. Neurosurg Focus. 2019;46(4):E18.
Kim JE, Yoo HS, Choi DJ, Park EJ, Jee SM. Comparison of minimal invasive versus biportal endoscopic transforaminal lumbar interbody fusion for single-level lumbar disease. Clin Spine Surg. 2021;34(2):E64–71.
Kang MS, You KH, Choi JY, Heo DH, Chung HJ, Park HJ. Minimally invasive transforaminal lumbar interbody fusion using the biportal endoscopic techniques versus microscopic tubular technique. Spine J. 2021;21(12):2066–77.
Heo DH, Hong YH, Lee DC, Chung HJ, Park CK. Technique of biportal endoscopic transforaminal lumbar interbody fusion. Neurospine. 2020;17(Suppl 1):S129–S37.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
1 Electronic Supplementary Material
Initial working space, ipsilateral and contralateral bone working (MP4 66566 kb)
Partial removal of superior articular process, identification of disc space, annulotomy, and endplate preparation (MP4 96271 kb)
Bone grafting, cage insertion, completion of central and foraminal decompression (MP4 59209 kb)
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Park, M.K., Son, S.K., Choi, S.H. (2022). Lumbar Interbody Fusion by Unilateral Biportal Endoscopy. In: Heo, D.H., Park, C.W., Son, S.K., Eum, J.H. (eds) Unilateral Biportal Endoscopic Spine Surgery. Springer, Singapore. https://doi.org/10.1007/978-981-16-8201-8_12
Download citation
DOI: https://doi.org/10.1007/978-981-16-8201-8_12
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-16-8200-1
Online ISBN: 978-981-16-8201-8
eBook Packages: MedicineMedicine (R0)