
Abstract
Transforaminal endoscopic thoracic discectomy (TETD) can minimize the incidence of postoperative spinal instability by minimizing resection of bone and joint tissue. It can be performed under the local anesthesia and has a faster recovery than open surgery.
The distance from the midline to the skin entry point can be calculated in the axial image of the MRI, usually 5–7 cm. An access angle of about 45–60 degrees is recommended for removal of the disc in the subarticular zone. A 70–80 degree angle is recommended to remove the disc in the foraminal zone. After approaching the disc space, internal discal decompression is performed using laser or forceps. After finding the annular tear point, the herniated disc can be easily removed. After removal of the herniated disc, full decompression can be confirmed by epidural pulsation. In addition, the working cannula can be a withdrawal to the annular window to directly check the ventral portion of the spinal cord to ensure complete decompression.
Transforaminal endoscopic thoracic discectomy with foraminoplasty under the local anesthesia could be an effective treatment method for the selected group of patients with thoracic disc herniation.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
Introduction
Thoracic disc herniation is rare compared with lumbar disc or cervical disc herniation, accounting for 0.25–0.5% of disc disease [1, 2]. However, the diagnosis of thoracic disc herniation is increasing with the development of diagnostic methods such as magnetic resonance image (MRI). Many patients with thoracic disc herniation have mostly no symptoms. Conservative treatment should be given preferentially to patients with symptoms without a severe neurological deficit. Patients with symptoms of thoracic disc herniation show various clinical presentations. Radical pain, motor symptom, sensory symptom, bladder symptom, or any of the above symptoms are associated with each other. In patients with symptomatic thoracic disc herniation, clinical manifestations can be dynamic and progression. Progressive myelopathy or voiding difficulty, lower limb motor weakness, patients with radiculopathy not responding to conservative therapy are candidates for decompression surgery [3, 4].
Kambin introduced the concept of posterior-lateral disc decompression in 1983 [5]. Endoscopic discectomies were developed into effective treatment methods for many herniated disc patients [6,7,8,9]. However, compared to open surgery, endoscopic decompression is difficult to apply for all forms of disc herniation due to its small operating field, limited equipment availability, and limited working mobility. Therefore, it is very important to establish an appropriate indication.
Transforaminal endoscopic thoracic discectomy (TETD) can minimize the incidence of postoperative spinal instability by minimizing resection of bone and joint tissue. It can be performed under the local anesthesia and has a faster recovery than open surgery. In addition, there is little traction on the nerve, which can reduce nerve edema, and it does not cause excessive nerve tissue exposure, thus minimizing postoperative neural adhesion. Indications for endoscopic discectomy are becoming increasingly widespread due to patient needs and the development of endoscopic devices.
Indication
Thoracic disc herniation can be classified as central, centro-lateral, or lateral depending on the location of the herniated disc [10, 11]. Because TETD is characterized by the foramen approach at the posterior lateral side, it can be applied to all soft thoracic disc herniations, regardless of location, from lateral to central herniation. Among them, paramedian or foraminal disc herniation can be removed more easily than central herniation because the target is reached immediately after approach. In the case of central herniation, it is safe to remove the extruded disc by accessing the subarticular zone, separating the dura and posterior longitudinal ligament, entering the disc, and removing the extruded disc.
TETD is not practically applicable to patients with calcified disc or hard disc herniation. The hard disc is defined as the disc containing calcification or ossification in the displaced portion of the herniated disc and is often associated with apophyseal osteophyte. Calcified discs are defined as calcification within the disc space, not inclusive of the disc space at the periphery of the disc space [12]. These are often adherent to surrounding nerve tissue. It is also difficult to remove the whole herniated disc by pulling a part of the hernia mass. For this reason, endoscopic treatment is difficult to obtain good treatment results for hard discs or calcified discs [1, 13].
Thoracic disc herniation usually occurs in the lower thoracic spine and is uncommon in the upper lumbar spine [14]. Because the thoracic vertebral body has a pear shape, it is possible to remove the extruded disc from the central portion to the foraminal portion, It can be applied to all thoracic levels. However, since the low thoracic spine has a large body size, the access can be made easier.
Thoracic disc herniation shows some intradural herniation [15, 16]. Epstein et al. [16] reported thoracic intradural herniation as 5% of all intradural herniation. Intradural herniation often shows severe adhesion between the dura and the posterior longitudinal ligament, often resulting in a dural defect. If intradural herniation is suspected on preoperative MRI, TETD is not appropriate.
Thoracic disc herniation is not exactly known for multiple level involvement. Bohlman et al. [17] reported that 3 out of 19 patients had multiple level involvement. Ross et al. [18] reported that 3 out of 13 patients had multiple level involvement. In thoracic disc herniation with multiple level involvement, open surgery may be more appropriate than TETD because the operation time including the approach is longer and the radiation exposure of the patient and the surgeon becomes larger.
Surgical Technique
Anesthesia and Position
Thoracic endoscopic decompression can be performed under local anesthesia. But it is recommended to have an anesthesiologist for sedation and pain control. Midazolam or fentanyl may be given intravenously to relieve pain and sedation during procedure. The degree of sedation is controlled to respond to the physician’s verbal command during the procedure. The patient is placed on the prone position under the guidance of fluoroscope.
Special Surgical Instrument
Unlike lumbar disc herniation, most patients with thoracic disc herniation require a foraminoplastic approach. Therefore, manual bone reamers, manual bone drills, or electrical endoscopic drills for foraminoplasty are essential for the procedure (Fig. 1). An endoscopic punch or laser is required to remove the ligamentum flavum, and endoscopic probe or scissor can be used for dissection between the spinal cord and the disc. For discectomy, forceps of various sizes and shapes are used.

Special surgical instrument used for foraminoplasty. (a) Manual bone drill. (b) Manual bone reamer. (c) Electrical endoscopic drill
Surgical Step
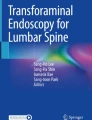
Preoperative MRI should be carefully checked to determine the appropriate skin entry point and approaching angle. The distance from the midline to the skin entry point can be calculated in the axial image of the MRI, usually 5–7 cm (Fig. 2). An access angle of about 45–60 degrees is recommended for removal of the disc in the subarticular zone. A 70–80 degree angle is recommended to remove the disc in the foraminal zone.

Preoperative MR image for determining the entry point
After determining the proper approach angle and skin entry point, insert an 18 gauge spinal needle using a fluoroscope.
In the anterior-posterior fluoroscopic view, the tip of needle is directed into the disc space, and in lateral view the tip of needle points toward the inferior portion of the superior articular process. Also in oblique view, the needle tip should be placed between the pedicle and the rib head (Fig. 3).

Transforaminal approach under the guidance of the fluoroscope. (a) Anterior-posterior fluoroscopic view; the tip of needle is directed to the disc space. (b) Lateral fluoroscopic view; introducer needle approaches the foramen along the undersurface of the superior articular process. (c) Oblique view; the needle is located between the pedicle and rib head
After touching the superior articular process, insert the needle into the foramen. The epidurogram is then performed using radiocontrast dye. Epidurograms can be used to identify the lateral margin of spinal cords, which can help access disc space safely. In addition, 2–3 ml of lidocaine 0.5% may be administered after the epidurogram, which may reduce the patient’s pain during the procedure (Fig. 4).

Epidurogram. (a) Lateral fluoroscopic view. Tip of needle is located in epidural space. (b) Anterior-posterior view. The lateral margin of the spinal cord can be identified
The needle is then inserted into disc space. The discogram confirms the extent of the herniated disc and observes whether concordant pain is caused (Fig. 5). And a guidewire is inserted into the epidural space through the needle. Enlarge the foraminal space by cutting the lateral aspect of the facet along the guidewire using a serial bone reamer (Fig. 6). In the fluoroscopic anterior-posterior image, bone work can be safely performed beyond the medial pedicular line to the lateral margin of the spinal cord identified after the epidurogram.

Discography. (a) Lateral fluoroscopic view. Extent of the disc herniation can be confirmed. (b) Anterior-posterior view. Tip of needle is located in the disc space beyond the lateral margin of the spinal cord

Schematic illustrations and fluoroscopic image of foraminoplasty. (a–d) Enlargement of the foraminal space by cutting the lateral aspect of the facet along the guidewire using a serial bone reamer
The thoracic vertebral body is a pear shape. Thus, the posterior vertebral body line of a lateral image does not indicate the anterior margin of the spinal cord. Therefore, the annulus should be touched during foraminoplasty before crossing the lateral margin of the spinal cord in the anterior-posterior image. After forminoplasty, obturator is introduced into the disc, and the working cannula is inserted into the disc space along the obturator.
Access using reamer can be difficult when the foramen is narrow with large pedicles or the transverse width of facet joint is wide. In this case, it is safe to approach the epidural space by placing the working cannula on the lateral portion of the facet joint, removing the upper part of the facet joint and pedicle using a drill, and then confirming the neural structure under direct endoscopic vision.
After approaching the disc space, internal discal decompression is performed using laser or forcep. After finding the annular tear point, the herniated disc can be easily removed.
After removal of the herniated disc, full decompression can be confirmed by epidural pulsation. In addition, the working cannula can be a withdrawal to the annular window to directly check the ventral portion of the spinal cord to ensure complete decompression.
After removing the working cannula, the subcritical suture is performed and the procedure is finished.
Postoperative Consideration
A neurological examination of the patient should be done immediately following the procedure. Neurological examination should confirm whether the symptom is improved and whether motor deficit has occurred. In addition, postoperative MR can be used to check for complete decompression of the lesion. The patient may be discharged after several hours of observation. At discharge, oral antibiotics are considered to prevent procedure related infection.
Case Illustration
Figure 7 a 43-year-old male presented with pain in thoracic area and sensory impairment in the right leg. Preoperative MR image demonstrated the herniated thoracic disc at T8/9. Endoscopic discectomy performed. Postoperative MR image revealed complete decompression of herniated disc.

Illustrative case. (a) Preoperative MR image showing thoracic herniated disc at T8/9. (b) Postoperative MR image showing complete decompression of herniated disc
Summary
Transforaminal endoscopic thoracic discectomy with foraminoplasty under the local anesthesia could be an effective treatment method for the selected group of patients with thoracic disc herniation.
References
Choi KY, Eun SS, Lee HY. Percutaneous endoscopic thoracic discectomy; Transforaminal approach. Minim Invas Neurosurg. 2010;53:25–8.
Baker JK, Reardon PR, Reardon MJ, et al. Vascular injury in anterior lumbar spine surgery. Spine. 1993;18:2227–30.
Lesoin F, Rousseaux M, Autricque A, et al. Thoracic disc herniations: evolution in the approach and indications. Acta Neurochir. 1986;80:30–4.
Rosenthal D, Rosenthal R, de Simone A. Removal of a protruded thoracic disc using mucrosurgical endoscopy: a new technique. Spine. 1994;19:1087–91.
Kambin P, Gellman H. Percutaneous lateral discectomy of the lumbar spine. Clin Orthop. 1983;174:172–32.
Yeung AT, Tsou PM. Posterolateral endoscopic excision for lumbar disc herniation: surgical technique, outcome, and complications in 307 consecutive cases. Spine. 2002;27:722–31.
Shin SH, Hwang BW, Keum HJ, et al. Epidural steroids after a percutaneous endoscopic lumbar discectomy. Spine. 2015;40:859–65.
Ahn Y, Lee SH, Park WM, et al. Percutaneous endoscopic lumbar discectomy for recurrent disc herniation: surgical technique, outcome, and prognostic factors of 43 consecutive cases. Spine. 2004;29:E326–32.
Birkenmaier C, Komp M, Leu HF, et al. The current state of endoscopic disc surgery: review of controlled studies comparing full-endoscopic procedures for disc herniations to standard procedures. Pain Physician. 2013;16:335–44.
Arce CA, Dohrmann G. Herniated thoracic disks. Neurol Clin. 1985;3:383–92.
Awwad EE, Martin DS, Smith KR Jr, et al. Asymptomatic versus symptomatic herniated thoracic discs: their frequency and characteristics as detected by computed tomography after myelography. Neurosurgery. 1991;28:180–6.
Fardon DF, Williams AL, Dohring EJ, et al. Lumbar disc nomenclature: version 2.0. Spine. 2014;4:1448–65.
Ruetten S, Komp M, Merk H, et al. Full-endoscopic interlaminar and transforaminal lumbar discectomy versus conventional microsurgical technique: a prospective, randomized, controlled study. Spine. 2008;33:931–9.
Videman T, Battie MC, Gill K, et al. Magnetic resonance imaging findings and their relationships in the thoracic and lumbar spine: insightes into the etiopathogenesis of spinal degeneration. Spine. 1995;20:928–35.
Patterson RH Jr, Arbit E. A surgical approach through the pedicle to protruded thoracic discs. J Neurosurg. 1978;48:768–72.
Epstein NE, Syrquin MS, Epstein JA, et al. Intradural disc herniations in the cervical, thoracic, and lumbar spine: report of three cases and review of the literature. J Spinal Disord. 1990;3:396–403.
Bohlman HH, Zdeblick TA. Anterior excision of herniated thoracic discs. J Bone Joint Surg Am. 1988;70:1038–47.
Ross JS, Perez-Reyes N, Masaryk TJ, et al. Thoracic disc herniation: MR imaging. Radiology. 1987;165:511–5.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 This is a U.S. government work and not under copyright protection in the U.S.; foreign copyright protection may apply
About this chapter

Cite this chapter
Shin, SH., Bae, J., Lee, SH. (2021). Transforaminal Endoscopic Thoracic Discectomy with Foraminoplasty. In: Lee, SH., Bae, J., Jeon, SH. (eds) Minimally Invasive Thoracic Spine Surgery. Springer, Singapore. https://doi.org/10.1007/978-981-15-6615-8_8
Download citation
DOI: https://doi.org/10.1007/978-981-15-6615-8_8
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-15-6614-1
Online ISBN: 978-981-15-6615-8
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)