
Abstract
Gastrointestinal cancers are a major threat to humans nowadays, due to their high incidence and mortality rates. The early detection of GI cancers was the key to prevention and treatment. Metabolomic profiling and analysis of volatile biomarkers are new and promising screening tools for the diagnosis of several cancers. Metabolites are small molecules produced during cell metabolism that represent the functional status of cell/tissue/malignant phenotype. Studies on biofluid metabolomics (serum, urine, plasma) are emerging fast on detecting new biomarkers for early diagnosis of cancer diseases and grasp a great promise for diagnostic applications. Volatile Organic Compounds (VOCs) signify diverse volatile metabolites which can be able to emit and diagnose in urine, breath, sweat, and feces. Nowadays, there is an increasing interest in the use and evaluation of VOCs with emerging analytical technologies in the diagnosis of GI cancer. With the advent of novel technologies in clinical diagnosis, metabolome analysis is an effective tool for metabolite profiling of biological processes in cells/tissues. This review emphasizes recent advancements in the identification of GI cancer biomarkers, particularly it focuses on metabolic markers and the emerging field of volatile biomarkers.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
1 Introduction
Gastrointestinal (GI) cancers are malignant with high mortality rates in the GI tract and accessory organs of digestion (Tillu and Nagaraju 2017). GI malignancies account for 30% of all cancer incidence and represent approximately 40% of tumor-related mortality globally. However, GI cancers are declining worldwide; however, it is even higher in Eastern Asia, mainly in China and Japan (Prathyusha et al. 2017). GI cancers have a high rate of mortality and morbidity due to a lack of defined risk factors, delayed diagnoses in their early stages leading to the progression of advanced stages with high recurrence (Tillu and Nagaraju 2017). Diagnosis in earlier stages considerably increases the prognosis by 95% in GI cancer patients (Xu et al. 2013). Esophagus, pancreatic, colorectal cancer (CRC), and gastric adenocarcinoma are among the top GI cancers in both incidence and mortality.
Several diagnostic tests are available for screening cancer, viz. upper and lower GI endoscopy-biopsy with pathological evaluation of tissue (Correa 2013; Thrumurthy et al. 2013), non-endoscopy-based balloon cytology, barium esophagram (Groome et al. 2008), image-based tests such as CT (computerized tomography) scan, Cytosponge, MRI (magnetic resonance imaging), cystoscopy, sigmoidoscopy, colonoscopy (Wild et al. 2010) and serological markers (Zhang et al. 2013, Patel and Ahmed (2015). Carcinoembryonic antigen (CEA) and fecal occult blood testing (FOBT) are currently in use for diagnosis of CRC with relatively low sensitivities and specificities (Ransohoff and Sox 2016). Nonetheless, all pragmatic approaches possess specific limitations in diagnosing imaging techniques. A major drawback is in some cases cancers endure undetected until malignant stages, in turn, affect the survival rate. The accuracy of endoscopy-biopsy screening and examination depends on collecting appropriate tissue biopsy which is a common clinical practice while a battery of serological marker tests was unsuccessful for screening or surveillance because of their low accuracy, sensitivity, and specificity. Many biopsy techniques are deliberate to be uncomfortable, inconvenient to patients, and are often underutilized by large segments of the population for a variety of reasons, such as access and patient burden (Oakley-Girvan and Davis 2017). Nonetheless, this necessitates the requirement for cost-effective, sensitive, reliable, accurate, noninvasive, patient-friendly screening tools for GI cancer detection which are currently not employed. Ascertaining specific biomarkers for detection of GI cancer in the benign stage (at onset) to ensure patient survival seems very promising.
Metabolites are small molecules produced during cell metabolism that represent the functional status of cell/tissue/malignant phenotype. The uncontrolled proliferation and altered metabolisms (glycolysis, TCA cycle, choline, and fatty acid metabolism) are important hallmarks of the malignant phenotype. These altered metabolisms result in a metabolic landscape that diverges significantly among cancer and normal cells. The goal of metabolomics studies captures this unique metabolic portrait as a label of cancer. Furthermore, a wide range of metabolic by-products is produced, comprising of a battery of organic compounds characterized by volatility at body temperatures, thus known as volatile organic metabolites/compounds (VOCs). Many VOCs are constantly produced in the body during various molecular pathways. VOCs are low molecular weight and volatile compounds detectable at low concentrations in biofluids, feces, and exhaled breath. Therefore, metabolites and VOCs can be highly informative regarding cell/tissue phenotype (Broza et al. 2018). Studies on biofluid metabolomics (serum, urine, plasma) and VOCs are emerging fast on detecting new biomarkers for early diagnosis of cancer diseases and grasp a great promise for diagnostic applications (Buck et al. 2017). Undoubtedly, several studies reported that specific regions of NMR and MS spectra differ among cancer patients and healthy controls (Patel and Ahmed 2015).
2 Metabolomic Analyses
Metabolic profiling involves two principal analytical procedures, viz. nuclear magnetic resonance (NMR) (Wang et al. 2017a, b) and mass spectrometry (MS) (Dettmer et al. 2007). Variations of NMR include high-resolution magic angle spinning (HR-MAS NMR) intended for tissue samples, 1H-NMR, 2D-NMR (HSQC and HMQC) techniques have been widely used in NMR-based metabolomics marker study (Emwas 2015). The chemical and physical diversity of molecules in biofluids, and alterations in ionic strength, pH, temperature, etc. may impede NMR analysis (Zhang et al. 2013). MS may be coupled directly to a chromatographic column such as gas chromatography-mass spectroscopy (GC-MS), liquid chromatography-mass spectroscopy (LC-MS), or capillary electrophoresis (CE-MS) (García et al. 2017) based on appliance. However, LC-MS is further ramified into ultra-performance mass spectroscopy (UPLC-MS) (Chen et al. 2019) or high-performance mass spectroscopy (HPLC-MS) (Zhao et al. 2006), and LC/MS/MS (liquid chromatography with tandem mass spectrometry). MS analysis can be performed using different ionization methods and mass analyzers (quadrupole time-off light (Q-TOF), Fourier transform ion cyclotron resonance (FTICR), and Orbitrap) for separation of ions of different masses and detection of molecular fragments based on mass-to-charge ratios (m/z). HPLC, coupled with electrospray ionization and Q-TOF (HPLC/ESI/Q-TOF-MS), was widely in use and documented to be beneficial clinically for early diagnosis of GI cancer due to precise qualitative analysis (Callejón-Leblic et al. 2016; Wang et al. 2017a, b).
Metabolome analysis was categorized into three major ways: targeted analysis, metabolic fingerprinting, and metabolite profiling (untargeted analysis). Untargeted analysis (metabolic profiling) usually emphasizes the measurement of levels of metabolites of all detectable metabolites in a given sample. NMR technique is widely in use for metabolomics fingerprinting (Emwas 2015). Metabolic fingerprinting reflects total metabolite fingerprint as a rare pattern illustrating a glimpse of the particular cell line or tissue metabolism. The targeted analysis emphasizes on the quantification and documentation of metabolites, of a specific metabolic pathway or direct product of drug administering or food intake. The metabolites involved in the study are usually predetermined, in targeted analysis, and the sample preparation is modified to diminish interference from other metabolites (Zhang et al. 2013). Djukovic and group employed targeted metabolite procedure to examine the role of nucleosides as cancer biomarkers in EAC (Esophageal Adenocarcinoma) using a serum-NMR technique (Djukovic et al. 2010).
Two main approaches have been developed that are used to assess VOCs in biological samples. Identification of the VOC spectrum allows one to study each compound separately and estimate the likelihood that it can serve as an individual biomarker of disease. One approach is based on analytical techniques such as GC-MS (Altomare et al. 2013), proton transfer reaction mass spectrometry (PTR-MS) (Jordan et al. 1995) and selected ion flow tube mass spectrometry (SIFT-MS) (Krilaviciute et al. 2015). Furthermore, the second approach is based on diverse chemically sensitive gas sensors that provide a total assessment of the mixture/profile of VOCs in a sample (Lourenço and Turner 2014).
Complex metabolite profiles obtained after analytical techniques were interpreted and characterized by multivariate pattern recognition statistical analysis, viz. (1) principle component analysis (PCA) (Wang et al. 2018), consensus PCA (CPCA), partial least square discriminant analysis (PLS-DA) (Nakajima et al. 2018), orthogonal signal correction (OSC), orthogonal partial least square discriminant analysis (OPLS-DA) (Li et al. 2013), and graded clustering analysis (GCA) (Wishart et al. 2016; Lai et al. 2018). XCMS is the most commonly used tool for metabolite profiling to analyze MS data by matching and nonlinear peak alignment. SIMCA-P is employed for multivariate data analysis (MVDA) by PLS, OPLS, and PCA analysis. MZmine 2 is a modular framework for visualizing, analyzing, and processing MS data. MetaboAnalyst is a web-based pipeline for statistical analysis, metabolomic data processing, and consequent functional elucidation. Notably, several additional tools also help in spectrometric data analysis. Davis et al. employed Mann–Whitney statistical analysis tool to correlate individual metabolite concentration among controls and EC patients (Davis et al. 2012).
3 Serum Metabolomics Signatures
Digestive tract malignant neoplasms are the most common reason for cancer-related mortality globally. Ikeda and hid co-workers reported more sensitive metabolites for diagnosis of GI cancer using analytical tools LC-MS, GC-MS, and NMR followed by PCA and PLS-DA statistical analysis. Their studies reported the metabolic differences among esophagus, gastric, and CRC cancer signifying the importance of different metabolisms in these cancers. Perhaps, these studies using multiple classifications analysis identify metabolite alteration levels namely malonic acid and l-serine is characteristic for EC. Alterations in concentrations of pyruvic acid and 3-hydroxy propionic acid is characteristic for gastric cancer while l-glutamine and glucuronic lactone signify colorectal cancer (Ikeda et al. 2012).
3.1 Esophagus and Stomach
Esophagus cancers are extremely malignant affecting the upper digestive tract with a 5-year survival rate in less than 15%. Zhang and colleagues (2013) analyzed the serum metabolic signatures of EC patients with healthy control using 1H NMR and UPLC based focused metabolic profiling. EC cells exhibited significant perturbations in glucose (reduced glucose and increased lactate levels in EC patients), lipids (apolipoproteins, LDL, VLDL, and unsaturated lipid were considerably reduced in the serum of EC patients), energy (serum creatinine and creatine concentrations were considerably elevated among EC patients), and amino acid metabolism. However, 12 biomarkers using NMR and 7 markers from UHPLC focused metabolomics were identified. Strikingly, the ketone bodies, viz. acetoacetate and β-hydroxybutyrate level were specifically elevated in EC patients’ serum suggesting a promoted β-oxidation. Amino acids (l-Tryptophan, l-Tyrosine, linoleic acid, and palmitic acid) have been identified to be modified in ESCC (Zhang et al. 2013). Wang et al. reported serum metabolites for the early-stage detection and discrimination among different stages of esophageal squamous cell carcinoma (ESCC) using nonparametric Kruskal–Wallis rank-sum test. Metabolites of glycerophospholipid, linoleic acid, and choline metabolism were to be found dysregulated in the ESCC population assessed to healthy individuals. Decreased trends of three biomarkers, namely dodecanoic acid, lysophosphatidic acid (LPA), and 4-lysophosphatidylcholines (LysoPC), reported being clear hallmarks for ESCC progression (Wang et al. 2016).
3.2 Colorectal Cancer (CRC)
CRC is one of the most prevailing cancer types globally with high morbidity and mortality. Uchiyama et al. reported serum metabolites for early-stage detection. Metabolome analysis was performed by CE-TOFMS for serum samples of CRC patients and controls followed by HCA and PCA statistical analysis and detected metabolites were plotted using VANTED software. Seventeen metabolites were reported to be correlated with CRC by elevation and 16 by downregulation in patients with adenoma in comparison with controls. Clustering identified upregulation of 7 and downregulation of 29 metabolites in stage I CRC, while upregulation of 11 and downregulation of 19 metabolites in stage II CRC. In stage III CRC, 5 metabolites reported to be upregulated whereas 39 downregulated; and in stage IV, 6 metabolites reported to be upregulated and 28 downregulated compared to normal controls. 3-hydroxybutyric acid was elevated in CRC stages and isovaleric acid, ornithine, benzoic acid, and the amino acids His, Lys, and Trp were downregulated. Of these, decanoic acid, octanoic acid (upregulated), histidine (downregulated), and benzoic acid exhibit significant correlation with all CRC stages. Benzoic acid is one of the metabolites that originated from procyanidins degradation by human gut microbiota. Benzoic acid was reported to be an excellent diagnostic marker to detect early and all the stages of CRC (Uchiyama et al.2017). Hata and his co-workers reported a promising serum biomarker GTA-446 (gastrointestinal tract acids) for primary CRC screening with the aim of early detection and to detect peoples at higher risk of CRC (Hata et al. 2017).
4 Plasma Metabolic Signatures
Plasma free amino acids (PFAA) are one of the most essential compounds for focused metabolomics as they play important physiological roles as elementary metabolites and metabolic regulators. Several studies reported that amino-acid levels were drastically declined in early-stage cancer populations, irrespective of subsequent progression. Particularly, significant reductions in the concentration of all amino acids were detected in both GC and CRC patients. Glutamine, tryptophan, histidine, proline, and ornithine amino acids were related to all types of cancer unveiled by univariate analysis (Miyagi et al. 2011).
4.1 Colorectal Cancer (CRC)
Cancers are characterized by diverse metabolic phenotypes due to alterations in key metabolic pathways, viz. glycolysis or tricarboxylic acid (TCA) cycle, etc. Geijsen et al. (2019) reported the correlation between plasma metabolites and colorectal cancer. Wang et al. reported a plasma metabolite marker for CRC diagnosis using a two-stage case-control study employing UPLC/Q-TOF MS/MS and PCA analysis. Glycochenodeoxycholate, l-Tryptophan, 13-OxoODE, IDP, and LysoPC (16:0), a five-biomarker panel, exhibited excellent diagnostic performance, favorable biological significance, and tumor specificity in Northeast China population. A six-biomarker panel of l-Phenylalanine, Linoleic acid, Citric acid, Inosine, Glycocholic acid, and LysoPC (14:0) showed the best extrapolation in diverse populations. Four metabolites (l-Tryptophan, Linoleic acid, Glycocholic acid, and LysoPC (16:0)) were ultimately recommended as the best combination with multiple advantages (Wang et al. 2018).
4.2 Esophagus and Stomach
In recent years, metabolomics studies on EC were performed by diverse analytical techniques to discover potential therapeutic markers. Liu et al. reported the metabolic profiling of ESCC by using UPLC-ESI-TOFMS and identified six upregulated molecules, namely phosphatidic acid, phosphatidylserine, phosphatidylethanolamine phosphatidylinositol, sphinganine 1-phosphate, and phosphatidylcholine. Furthermore, bile acid, lithocholic acid taurine conjugate reported being significantly upregulated whereas 5-β-cyprinol sulfate and desmosine/isodesmosine are downregulated in the plasma of ESCC patients (Liu et al. 2013).
5 Urinary and Fecal Metabolic Signatures
Urine is a biofluid usually used by metabolomics scientists, due to the collection of large volumes and patient-friendly.
5.1 Colorectal Cancer
Urine metabolic profiles were analyzed by Wang and his co-workers using 1H NMR along with OPLS-DA statistical validation by permutation analysis in comparison with healthy controls at stage I/II. They reported perturbation in amino acid (asparagine, alanine, cysteine, and phenylalanine), glycolysis, TCA cycle, choline (acetoacetate, guanidinoacetate), vitamin-B3 (Trigonelline), and urea metabolisms. Metabolites upregulated and downregulated at different stages were summarized in Table 5.1 (Wang et al. 2017a, b). Le Gall and his research group quantified fecal extracts from CRC patients and screened over 80 molecules using NMR. Furthermore, isobutyrate, branched-chain fatty acids (BCFA), valerate, isovalerate, and phenylacetate were reported to be upregulated while reduced concentrations of amino acids, methanol, sugars, and bile acids (lithodeoxycholate, cholate, and deoxycholate) in the fecal extracts of ESCC patients (Le Gall et al. 2019).
5.2 Esophagus and Stomach
Altered carbohydrates, amino acids, lipid, and ketone metabolisms were reported to be hallmarks for EC. Xu and his research group reported global urine metabolic profile of ESCC patients and healthy controls using LC-MS along with MVDA and reported 19 potential biomarkers related to perturbations of amino acids fatty acid β-oxidation and nucleotide metabolism. Metabolites upregulated and downregulated at different stages were summarized in Table 5.1 (Xu et al. 2016). Recently, studies are employing metabolomics technology to tissue, plasma, serum, and urine samples revealed alterations in choline, glucose, amino acid, fatty acid, linoleic acid, and energy metabolism in EC cells. These metabolites upregulation and downregulation reflected in blood samples of patients indicates the importance of these metabolisms in esophagus cancer progression and early detection.
6 Volatile Organic Compounds
VOCs are a diverse group of carbon compounds emitted from the human body that reflects the metabolic condition of the person detected in blood, breath, and excreted body fluids. Hundreds of different VOCs have been reported in cancer patients from different sources. Acids, ketones, alcohols, amines, aldehydes, O-heterocycles, N-heterocycles, VOCs, and other VSCs have been detected and quantified. However, concentrations of specific organic compounds in the exhaled breath of cancer patients are thought to be the result of oxidative stress, abnormal metabolic processes, or inability of biological systems to detoxify ROS (reactive oxygen species). Some VOCs are thought to originate from cancer cells as a result of abnormal metabolism that does not exist in healthy people (Oakley-Girvan and Davis 2017). Among several extraction procedures SPME (solid-phase microextraction) is a prevailing technique for sample preparation, sampling a wide range of analytes in breath and biological samples (Kim et al. 2019).
The four studies targeting to identify VOC in breath samples of CRC patients suggested diverse patterns of potential biomarkers were not completely matched, with an exemption of 1,3-dimethyl benzene reported by both Peng and Altomare groups individually (Peng et al. 2010; Altomare et al. 2013). Furthermore, 4-methyl octane was reported as a potential biomarker both by Altomare and Amal groups individually (Altomare et al. 2013; Amal et al. 2016). These diverse patterns possibly due to the involvement of different methods in sample collection and analysis. Wang et al. examined two different samples, of CRC patients i.e., exhaled breath and blood using SPME-GC-MS technique. Two different VOC patterns that did not fit each other probably due to different sample characteristics are reported. Remarkably, these authors identified reduced levels of 6-t-butyl-2,2,9,9-tetramethyl-3,5-decadien-7-yne in breath and blood sample. Kumar and his research group analyzed breath samples from 81 esophageal or gastric adenocarcinoma patients against 129 controls including benign upper gastrointestinal diseases, Barrett’s metaplasia, and normal upper GI tract. Twelve VOCs—hexanoic acid, pentanoic acid, methyl phenol, ethyl phenol, phenol, butanal, hexanal, pentanal, octanal, heptanal, decanal, and nonanal, were reported at extremely high levels in cancer groups compared to controls (Kumar et al. 2015). Kim and his co-workers employed SPME and 2D GC-MS to analyze 30 random plasma samples from CRC patients and reported five VOCs, among them 2,3,4-trimethylhexane (reduced) and 2,4-dimethylhept-1-ene (enhanced) were both lipid peroxidation products (Kim et al. 2019). Wang and his co-workers analyzed blood VOCs of SW620 CRC mice for a course of 12 and 26 days. They reported eight VOCs which progressively augmented with tumor growth (acetone, glycerol, arsenous acid, 2-heptanone, 4-nonanone, tris (trimethylsilyl) ester, butylated hydroxytoluene, l-alanine ethylamide (S)-, and 3-heptanone,4-methyl 2-dodecanone). The concentration of VOCs peaked at maximum tumor size and decreased promptly after tumor resection. Cyclotrisiloxane, hexamethyl was utilized by the tumor, and its concentration progressively reduced with the size of the tumor (Wang et al. 2019).
7 Nanomaterial-Based Breath Tests
Nanomaterial-based breath tests were first developed by Haick and co-workers that could categorize among different cancer types in exhaled breath, regardless of patients’ lifestyle, habits, gender, and other confounding factors. Xu et al. used GC-MS for chemical analysis of breath samples reported five VOCs (2-butoxy-ethanol, 2-propenenitrile, furfural, isoprene, and 6-methyl-5-hepten-2-one) elevated in gastric cancer and gastric ulcer patients. Three different DFA models were developed to achieve excellent discrimination among them (1) GC vs. benign gastric conditions, reported with 89% sensitivity; 90% specificity; (2) different stages of GC early-stage (I and II) and late-stage (III and IV), with 89% sensitivity; 94% specificity (Xu et al. 2013). Tong et al. reported four nanomaterial-based biomarkers in gastric cancer patients vs. healthy individuals 1,3-Dioxolan-2-one, Undecane, 2,3-Butanediol, 3,8-dimethyl- N,N-Dimethylacetamide Hexadecane while (p-hydroxyphenyl), 1,3-Dioxolane-2-methanol and 3,5-Decadien-7-yne, Phosphonic acid, 6-t-butyl-2,2,9,9-tetramethyl-1,6-Dioxacyclododecane-7,12-dione for carcinoma patients vs. gastric ulcer patients (Tong et al. 2017).
8 Integration of Metabolomic Networks
In the human body, most cancer cells exhibit hypoxic environment due to increased cell division at early stages resulting in increased aerobic and anaerobic glycolysis which is accompanied by disrupted TCA cycle and even other metabolisms creating a mutagenic phenotype. Tumor cells predominantly generate energy through glycolysis rather than oxidative phosphorylation via the TCA cycle, even in aerobic conditions (Warburg effect) (Armitage and Southam 2016). This results in the production of lactate in large amounts by the tumor and the anabolic synthesis of nucleotides, amino acids, and lipids. Lactate produced in large amounts is converted to glucose in liver via Cori cycle ends in acetyl Co-A accumulation and citrate upregulation (disruption of TCA cycle). If acetyl-CoA is not well utilized in TCA cycle, ketogenesis takes place and thus the accumulation of ketone bodies, viz. acetoacetate and β-hydroxybutyrate (Zhang et al. 2013). Increased glucose utilization favors energy metabolism, NADPH recycling to maintain serum creatine, creatinine, and glutathione levels for an optimal cellular redox status, respectively (Wang et al. 2013). Many blood amino acids downregulated in cancer patients indicate an increased demand for and overutilization of amino acids in tumor tissue. Altered fatty acid metabolism is also reported in cancer patient’s plasma, by reduced levels of several unsaturated lipids, VLDL, and LDL (Hasim et al. 2012). Wang et al. first reported the importance of essential fatty acids (linolenic acid) in proliferating tumor cells for the biosynthesis of prostaglandins and cell-membrane assembly and their metabolites as biomarkers (Wang et al. 2018). In summary, altered/disrupted metabolomic pathways comprise fluctuations in glycolysis, Cori cycle, TCA cycle, an amino acid (Alanine, Leucine, Valine, Isoleucine, 1-methylhistidine, and Glycoprotein), a ketone body, fatty acid (unsaturated lipids, VLDL, and LDL), energy metabolisms, and urea cycle. Metabolites accumulate in these pathways represent typical metabolic and VOC signatures in GI cancer patients.
9 Conclusion and Future Directions
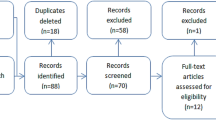
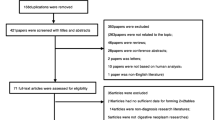
Currently available techniques for diagnosis and surveillance of GI cancers are expensive, invasive, and not suitable for early detection. Robust, low-cost, and noninvasive biomarkers to facilitate early screening, surveillance are scanty, indicating the necessity for the development of more efficient methods. In this sense, the metabolomics field emerged highly promising in the past few years, with large advancements in GI cancer diagnosis based on metabolites. Metabolic profiling has been used to find novel biomarkers for early detection of cancers. However, metabolomic analysis is a promising approach in cancer diagnosis, with certain constraints comprising necessity to evaluate existing metabolites, data redundancy, false discovery problems, and cost limitations endure major hurdles for metabolomics research. Issues related to sensitivity, specificity, and accuracy for biomarker detection must be dealt with to unleash metabolomics potential. Furthermore, the diagnostic accuracy of metabolic signatures needs to be established (Figs. 5.1 and 5.2).

Genomics to metabolomics

Schematic representation of metabolome profiling
References
Altomare DF, Di Lena M, Porcelli F, Trizio L, Travaglio E, Tutino M et al (2013) Exhaled volatile organic compounds identify patients with colorectal cancer. Br J Surg 100(1):144–150
Amal H, Leja M, Funka K, Lasina I, Skapars R, Sivins A et al (2016) Breath testing as potential colorectal cancer screening tool. Int J Cancer 138(1):229–236
Armitage EG, Southam AD (2016) Monitoring cancer prognosis, diagnosis and treatment efficacy using metabolomics and lipidomics. Metabolomics 12(9):146
Broza YY, Vishinkin R, Barash O, Nakhleh MK, Haick H (2018) Synergy between nanomaterials and volatile organic compounds for non-invasive medical evaluation. Chem Soc Rev 47(13):4781–4859
Buck A, Aichler M, Huber K, Walch A (2017) In situ metabolomics in cancer by mass spectrometry imaging. In: Advances in cancer research, vol 134. Academic, Cambridge, pp 117–132
Callejón-Leblic B, García-Barrera T, Grávalos-Guzmán J, Pereira-Vega A, Gómez-Ariza JL (2016) Metabolic profiling of potential lung cancer biomarkers using bronchoalveolar lavage fluid and the integrated direct infusion/gas chromatography mass spectrometry platform. J Proteome 145:197–206
Chen JL, Fan J, Yan LS, Guo HQ, Xiong JJ, Ren Y, Hu JD (2012) Urine metabolite profiling of human colorectal cancer by capillary electrophoresis mass spectrometry based on MRB. Gastroenterol Res Prac 2012:8
Chen J, Hou H, Chen H, Luo Y, Zhang L, Zhang Y et al (2019) Urinary metabolomics for discovering metabolic biomarkers of laryngeal cancer using UPLC-QTOF/MS. J Pharm Biomed Anal 167:83–89
Correa P (2013) Gastric cancer: overview. Gastroenterol Clin N Am 42:211–217
Davis VW, Schiller DE, Eurich D, Sawyer MB (2012) Urinary metabolomic signature of esophageal cancer and Barrett’s esophagus. World J Surg Oncol 10(1):271
Dettmer K, Aronov PA, Hammock BD (2007) Mass spectrometry-based metabolomics. Mass Spectrom Rev 26(1):51–78
Djukovic D, Baniasadi HR, Kc R, Hammoud Z, Raftery D (2010) Targeted serum metabolite profiling of nucleosides in esophageal adenocarcinoma. Rapid Commun Mass Spectrom 24(20):3057–3062
Emwas AHM (2015) The strengths and weaknesses of NMR spectroscopy and mass spectrometry with particular focus on metabolomics research. In: Metabonomics. Humana Press, New York, pp 161–193
García A, Godzien J, López-Gonzálvez Á, Barbas C (2017) Capillary electrophoresis mass spectrometry as a tool for untargeted metabolomics. Bioanalysis 9(1):99–130
Geijsen AJ, Brezina S, Keski-Rahkonen P, Baierl A, Bachleitner-Hofmann T, Bergmann MM et al (2019) Plasma metabolites associated with colorectal cancer: a discovery-replication strategy. Int J Cancer 145(5):1221–1231
Groome M, Lindsay J, Ross PE, Cotton JP, Hupp TR, Dillon JF (2008) Use of oesophageal stress response proteins as potential biomarkers in the screening for Barrett’s oesophagus. Eur J Gastroenterol Hepatol 20(10):961–965
Hasim A, Ma H, Mamtimin B, Abudula A, Niyaz M, Zhang LW et al (2012) Revealing the metabonomic variation of EC using 1 H-NMR spectroscopy and its association with the clinicopathological characteristics. Mol Biol Rep 39(9):8955–8964
Hata T, Takemasa I, Takahashi H, Haraguchi N, Nishimura J, Hata T et al (2017) Downregulation of serum metabolite GTA-446 as a novel potential marker for early detection of colorectal cancer. Br J Cancer 117(2):227
Ikeda A, Nishiumi S, Shinohara M, Yoshie T, Hatano N, Okuno T et al (2012) Serum metabolomics as a novel diagnostic approach for gastrointestinal cancer. Biomed Chromatogr 26(5):548–558
Jordan A, Hansel A, Holzinger R, Lindinger W (1995) Acetonitrile and benzene in the breath of smokers and non-smokers investigated by proton transfer reaction mass spectrometry (PTR-MS). Int J Mass Spectrom Ion Process 148(1–2):L1–L3
Kim S, Yin X, Prodhan MAI, Zhang X, Zhong Z, Kato I (2019) Global plasma profiling for colorectal cancer-associated volatile organic compounds: a proof-of-principle study. J Chromatogr Sci 57(5):385–396
Krilaviciute A, Heiss JA, Leja M, Kupcinskas J, Haick H, Brenner H (2015) Detection of cancer through exhaled breath: a systematic review. Oncotarget 6(36):38643
Kumar S, Huang J, Abbassi-Ghadi N, Mackenzie HA, Veselkov KA, Hoare JM et al (2015) Mass spectrometric analysis of exhaled breath for the identification of volatile organic compound biomarkers in esophageal and gastric adenocarcinoma. Ann Surg 262(6):981–990
Lai Z, Tsugawa H, Wohlgemuth G, Mehta S, Mueller M, Zheng Y et al (2018) Identifying metabolites by integrating metabolome databases with mass spectrometry cheminformatics. Nat Methods 15(1):53
Le Gall G, Guttula K, Kellingray L, Tett AJ, ten Hoopen R, Kemsley EK et al (2019) Correction: metabolite quantification of faecal extracts from colorectal cancer patients and healthy controls. Oncotarget 10(17):1660
Li F, Qin X, Chen H, Qiu L, Guo Y, Liu H et al (2013) Lipid profiling for early diagnosis and progression of colorectal cancer using direct-infusion electrospray ionization Fourier transform ion cyclotron resonance mass spectrometry. Rapid Commun Mass Spectrom 27(1):24–34
Liu R, Peng Y, Li X, Wang Y, Pan E, Guo W et al (2013) Identification of plasma metabolomic profiling for diagnosis of esophageal squamous-cell carcinoma using an UPLC/TOF/MS platform. Int J Mol Sci 14(5):8899–8911
Lourenço C, Turner C (2014) Breath analysis in disease diagnosis: methodological considerations and applications. Metabolites 4(2):465–498
Miyagi Y, Higashiyama M, Gochi A, Akaike M, Ishikawa T, Miura T et al (2011) Plasma free amino acid profiling of five types of cancer patients and its application for early detection. PLoS One 6(9):e24143
Monleon D, Morales JM, Barrasa A, Lopez JA, Vazquez C, Celda B (2009) Metabolite profiling of fecal water extracts from human colorectal cancer. NMR Biomed 22(3):342–348
Nakajima T, Katsumata K, Kuwabara H, Soya R, Enomoto M, Ishizaki T et al (2018) Urinary polyamine biomarker panels with machine-learning differentiated colorectal cancers, benign disease, and healthy controls. Int J Mol Sci 19(3):756
Oakley-Girvan I, Davis SW (2017) Breath based volatile organic compounds in the detection of breast, lung, and colorectal cancers: a systematic review. Cancer Biomark 21(1):29–39
Patel S, Ahmed S (2015) Emerging field of metabolomics: big promise for cancer biomarker identification and drug discovery. J Pharm Biomed Anal 107:63–74
Peng G, Hakim M, Broza YY, Billan S, Abdah-Bortnyak R, Kuten A et al (2010) Detection of lung, breast, colorectal, and prostate cancers from exhaled breath using a single array of nanosensors. Br J Cancer 103(4):542
Prathyusha AMVN, Raghu G, Bramhachari PV (2017) HIF-1α: its role in metastasis of oesophageal malignancy. In: Role of transcription factors in gastrointestinal malignancies. Springer, Singapore, pp 71–87
Ransohoff DF, Sox HC (2016) Clinical practice guidelines for colorectal cancer screening: new recommendations and new challenges. JAMA 315(23):2529–2531
Thrumurthy SG, Chaudry MA, Hochhauser D, Mughal M (2013) The diagnosis and management of gastric cancer. BMJ 347:f6367
Tillu H, Nagaraju GP (2017) YY1 and KLF4: their role in gastrointestinal malignancies. In: Role of transcription factors in gastrointestinal malignancies. Springer, Singapore, pp 3–15
Tong H, Wang Y, Li Y, Liu S, Chi C, Liu D et al (2017) Volatile organic metabolites identify patients with gastric carcinoma, gastric ulcer, or gastritis and control patients. Cancer Cell Int 17(1):108
Uchiyama K, Yagi N, Mizushima K, Higashimura Y, Hirai Y, Okayama T et al (2017) Serum metabolomics analysis for early detection of colorectal cancer. J Gastroenterol 52(6):677–694
Wang L, Chen J, Chen L, Deng P, Xiang P, Li M et al (2013) 1 H-NMR based metabonomic profiling of human esophageal cancer tissue. Mol Cancer 12(1):1
Wang J, Zhang T, Shen X, Liu J, Zhao D, Sun Y et al (2016) Serum metabolomics for early diagnosis of esophageal squamous cell carcinoma by UHPLC-QTOF/MS. Metabolomics 12(7):116
Wang Z, Lin Y, Liang J, Huang Y, Ma C, Liu X, Yang J (2017a) Nmr-based metabolomic techniques identify potential urinary biomarkers for early colorectal cancer detection. Oncotarget 8(62):105819
Wang D, Li W, Zou Q, Yin L, Du Y, Gu J, Suo J (2017b) Serum metabolomic profiling of human gastric cancer and its relationship with the prognosis. Oncotarget 8(66):110000
Wang M, Long Z, Tian J, Chen S, Sun H, Jian R, et al (2018) Plasma biomarkers for colorectal cancer diagnosis based on metabolomics
Wang G, Li Y, Liu M, Guo N, Han C, Liu D et al (2019) Determination of volatile organic compounds in SW620 colorectal cancer cells and tumor-bearing mice. J Pharm Biomed Anal 167:30–37
Wild N, Andres H, Rollinger W, Krause F, Dilba P, Tacke M, Karl J (2010) A combination of serum markers for the early detection of colorectal cancer. Clin Cancer Res 16(24):6111–6121
Wishart D, Mandal R, Stanislaus A, Ramirez-Gaona M (2016) Cancer metabolomics and the human metabolome database. Metabolites 6(1):10
Xu ZQ, Broza YY, Ionsecu R, Tisch U, Ding L, Liu H et al (2013) A nanomaterial-based breath test for distinguishing gastric cancer from benign gastric conditions. Br J Cancer 108(4):941
Xu J, Chen Y, Zhang R, He J, Song Y, Wang J et al (2016) Global metabolomics reveals potential urinary biomarkers of esophageal squamous cell carcinoma for diagnosis and staging. Sci Rep 6:35010
Yang Z, Liu Y, Ma L, Wen X, Ji H, Li K (2019) Exploring potential biomarkers of early stage esophageal squamous cell carcinoma in pre-and post-operative serum metabolomic fingerprint spectrum using 1H-NMR method. Am J Transl Res 11(2):819
Yue H, Wang Y, Zhang Y, Ren H, Wu J, Ma L, Liu S (2013) A metabonomics study of colorectal cancer by rrlc-qtof/ms. J Liq Chromatogr Relat Technol 36(4):428–438
Zhang X, Xu L, Shen J, Cao B, Cheng T, Zhao T et al (2013) Metabolic signatures of esophageal cancer: NMR-based metabolomics and UHPLC-based focused metabolomics of blood serum. Biochim Biophys Acta 1832(8):1207–1216
Zhao X, Wang W, Wang J, Yang J, Xu G (2006) Urinary profiling investigation of metabolites with cis-diol structure from cancer patients based on UPLC-MS and HPLC-MS as well as multivariate statistical analysis. J Sep Sci 29(16):2444–2451
Acknowledgments
The authors gratefully acknowledge UGC, Government of India, for financial support to AMVNP in the form of UGC-CSIR-JRF & SRF under the Grant No: F.No. 19-1/2015(SA-1).
Conflict of Interest
We declare we do not have any conflict of interest.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Prathyusha, A.M.V.N., Naidu, B.P., Veera Bramhachari, P. (2020). Metabolic Markers for Early Detection of Gastrointestinal Cancers. In: Veera Bramhachari, P., Neelapu, N. (eds) Recent Advancements in Biomarkers and Early Detection of Gastrointestinal Cancers . Diagnostics and Therapeutic Advances in GI Malignancies. Springer, Singapore. https://doi.org/10.1007/978-981-15-4431-6_5
Download citation
DOI: https://doi.org/10.1007/978-981-15-4431-6_5
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-15-4430-9
Online ISBN: 978-981-15-4431-6
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)