
Abstract
Infectious diseases of the lower female genital tract include a variety of bacterial, viral, fungal, and parasitic infections that are commonly, but not exclusively, sexually transmitted. Sexually transmitted diseases (STDs) are a global public health issue and have serious impact on health care costs in the United States. The Centers for Disease Control and Prevention announced increasing numbers of reported STDs in recent years. Chlamydia, gonorrhea, and especially syphilis rates have increased dramatically over the past few years. Most infections of the lower female genital tract are diagnosed clinically, and tissue biopsies are rarely performed; however, it is important to be familiar with these entities and their histopathologic features to avoid misdiagnosis of these rather common infections. This chapter reviews clinical and pathologic presentations of common infections of the lower female genital tract, and incorporates the latest guidelines available for each entity. Human papillomavirus infection is briefly discussed under common sexually transmitted infections and generalized genital warts in patients with immunosuppression, and further reviewed in detail in other chapters. It also includes rare entities in the United States that should be considered in the differential diagnosis of patients with human immunodeficiency virus infection and vulvovaginal involvement by systemic infections in immunosuppressed individuals.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
3.1 Common Sexually Transmitted Infections
3.1.1 Trichomonas vaginalis
Trichomoniasis is the most common nonviral sexually transmitted disease (STD), caused by a motile flagellate parasitic protozoan, Trichomonas vaginalis (T. vaginalis) [1]. The parasite is typically pyriform, although in vivo amoeboid forms are occasionally identified. It has four anterior flagella, plus one recurrent flagellum that forms the undulating membrane [2, 3]. T. vaginalis infection only occurs in humans, and is more common in women, with estimated prevalence of 3.1% among women of reproductive age in the United States [4]. Higher rates of T. vaginalis infections have been reported among women 40 years and older (>11%). The infection is more prevalent among women with other STDs and human immunodeficiency virus (HIV) -infected individuals [5, 6].
Trophozoites of T. vaginalis are transmitted through sexual intercourse and attach to the mucosal surfaces of the lower urogenital tract. The organisms colonize the mucosa and release proteinases resulting in desquamation of the vaginal and cervical epithelia [7]. Trichomoniasis is associated with adverse outcomes of pregnancy, such as preterm labor or delivery of a low-birth weight infant [1, 5]. In addition, T. vaginalis may increase women’s risk of HIV acquisition and transmission [8].
Clinical features: The infection manifests with vulvovaginal pruritus and irritation, as well as frothy or yellow-green vaginal discharge. Cervical examination may reveal signs of cervicitis with punctate friability (strawberry cervix). Multiple studies have indicated that nearly half of the infected women are asymptomatic [3, 5, 7].
Diagnostic methods: Diagnosis can be made through a variety of techniques such as wet mount microscopy, culture, rapid antigen tests, polymerase chain reaction, and nucleic acid amplification test [1, 3]. Pap smears are not considered appropriate diagnostic or screening tests for T. vaginalis because of their poor sensitivity; however, if the organism is identified on liquid-based cervical smears, the specificity is high [8, 9].
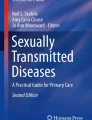
Microscopic findings: On histologic sections, the findings are nonspecific. The morphologic findings on cytology smears include identification of the pear-shaped organisms with eosinophilic cytoplasmic granules and eccentrically located vesicular nuclei (Fig. 3.1), clusters of neutrophils (polyballs), reactive nuclear changes with small perinuclear halos, and attachment of T. vaginalis to squamous cells [10, 11]. Leptothrix may be seen in association with T. vaginalis [11].

Papanicolaou-stained liquid-based smear depicts T. vaginalis, pear-shaped organisms with eosinophilic cytoplasmic granules and eccentric nucleus (arrows) and attachment of the organisms to squamous cells (white arrow)
Management: Concurrent treatment of the patient and all sex partners is curative and reduces transmission. First-line therapy consists of a single dose of metronidazole or tinidazole, as recommended by the United States Centers for Disease Control and Prevention (CDC) [12].
3.1.2 Molluscum Contagiosum
Molluscum contagiosum is a viral infection caused by a double-stranded DNA virus of the Poxviridae family, Molluscum contagiosum virus (MCV) . There are four known genotypes of MCV; type 1 is the most common form in healthy humans. The disease is more prevalent in children, transmitted by direct skin contact, and usually affects the exposed areas [13, 14]. In healthy young adults the disease is often transmitted sexually and lesions initially appear in genital area. However, the virus may be transmitted by casual contact or self-inoculation. Among HIV positive population, molluscum contagiosum is more common and can present as widespread lesions [13, 15].
Clinical features: MCV primarily infects the skin and follicular epithelium, presenting with single or multiple lesions in the epidermis. The lesions manifest as flesh-colored, raised, umbilicated papules or nodules (Fig. 3.2). Diagnosis is usually made by identification of skin lesions. Immunocompromised patients may present with atypical features including giant lesions (>1 cm), verrucous papules, or clusters of hundreds of small lesions [15, 16].

Molluscum contagiosum: (a, b) Single or multiple flesh-colored, raised, umbilicated papules or nodules. Microscopic findings characterized by (c) lobulated crater-shaped hyperplasia of the epithelium and inclusions of Molluscum contagiosum virus . Infected cells reveal (d) eosinophilic intracytoplasmic inclusions (molluscum bodies or Henderson-Patterson bodies) that displace the nucleus to the periphery
Microscopic Findings: Histologically, the molluscum lesions are characterized by lobulated endophytic hyperplasia of the epithelium with acanthotic epidermis. Eosinophilic intracytoplasmic inclusions, known as molluscum bodies or Henderson-Patterson bodies, are result of virus replication within the cytoplasm. As the inclusions enlarge, they compress the nucleus of infected cells to the periphery and acquire a basophilic appearance (Fig. 3.2) [17]. The epidermis ruptures as a result of pressure due to underlying proliferation and produces the characteristic white-yellow core. The surrounding dermis is relatively unremarkable with little or no inflammatory reaction; rarely the lesion ruptures in dermis and triggers an inflammatory response.
3.1.3 Herpes Simplex Virus
Genital herpes is a widespread sexually transmitted disease. It is the most common cause of genital ulcers in the United States, and is caused by the human herpes simplex virus (HSV). HSV is a double-stranded DNA virus from ubiquitous Herpesviridae family, and has two distinct types based on different envelope protein and antigen properties. Both types can cause genital herpes, a lifetime incurable infection. HSV-2 is the major cause of genital herpes; however, increasing numbers of genital ulcerations that are caused by HSV-1 in developed countries have been reported [18, 19]. The virus is transmitted through direct mucocutaneous contact with herpetic lesions or exposure to mucosal secretions during periods of viral shedding. Transmission occurs not only when lesions are visible, but also when lesions are not clinically apparent [20]. Asymptomatic viral shedding in the absence of detectable lesions is responsible for up to 70% of all HSV-2 infections [21]. A considerable number of HSV-2 seropositive individuals do not have a history of symptomatic genital herpes. Transmission of HSV from mother to child during pregnancy is uncommon and usually occurs at the time of labor and delivery; however, new infections acquired late in pregnancy carry a high risk for transmission to neonate [22].
Clinical features: Primary infections are usually asymptomatic and manifest with localized pain, tingling, or burning sensation at the site of exposure. Prodrome of systemic symptoms including headache, fever, malaise, dysuria, and lymphadenopathy is common. The virus damages the epithelium at the exposure site, causing eruption of vesicles within days. The vesicles rupture, resulting in erosion and ulceration, which heal without leaving scar. The virus travels by sensory nerve axons to the sacral ganglion and remains latent for the life of the host. Spontaneous or stress induced periodic reactivation of the virus manifests as mucocutaneous lesions [23]. HSV -1 induced infections are usually milder and recur 1–2 times a year, compared with HSV-2 infection causing 4–6 episodes of recurrence per year [19, 22]. Immunocompromised patients have an increased risk for extensive and recurrent HSV infection. Atypical presentations of genital herpes, including persistent ulcers and verrucous lesions, have been described in immunocompromised individuals [22, 24]. Another less common presentation of HSV in patients with immunodeficiency, known as “knife-cut sign,” appears as linear ulcers and fissures in intertriginous areas, such as the inguinal region, vulva, and other areas with folds [25]. Genital herpes is a common infection among human immunodeficiency virus type 1 (HIV-1)-infected patients, ranging from 50% to 90% in different affected populations [24]. Individuals with HSV infection are more prone to acquisition of HIV infection. HSV-2 prevents an effective immune response at the site of entry; furthermore complex interactions between HSV and host can affect HIV-1 replication [26].
Microscopic findings: The histology of herpes infections is very distinctive. Acantholysis, spongiosis, and ballooning degeneration of keratinocytes form intraepidermal and subepidermal vesicles. The keratinocyte nuclei show ground-glass appearance of nucleus with peripheral condensation of chromatin. Multinucleated cells show “molding” nuclei. The dermis shows polymorphous inflammation and leukocytoclastic vasculitis may be present. In late stages, vesicles rupture resulting in epithelial ulceration and crust [27]. Exophytic masses involving genital area associated with immunocompromised patients show pseudoepitheliomatous hyperplasia and can mimic cancer [28]. On cytology smears, herpes cytopathic effects present with the classic “3 Ms”: multinucleation, molding, and margination of chromatin (Fig. 3.3). Nuclei have a ground glass appearance due to accumulation of viral particles and eosinophilic intranuclear (Cowdry A) inclusions surrounded with a clear halo are variably present [11].

Herpes simplex virus infection: (a) Low power view of a herpetic ulcer, epithelial ulceration with multinucleated keratinocytes. (b) Intranuclear inclusions show ground-glass appearance, margination of chromatin, multinucleation, and nuclear molding . (c) Immunohistochemical stain for HSV2 highlights virus-infected cells. (d) Papanicolaou-stained smear portrays the classic “3 Ms” herpes cytopathic effect
Diagnostic methods: Diagnosis is made by nucleic acid amplification methods, including PCR assays or viral culture. Serologic tests that detect antibodies are available, but are not sensitive for differentiating acute and chronic infection. Direct immunofluorescence antigen staining is not recommended due to low sensitivity [23].
Differential diagnosis: Although HSV is the most common cause of genital ulcers in the United States, other ulcerative genital disease and the coexistence of other STDs must be considered. Other infectious etiologies such as chancroid and syphilis can be in differential diagnosis (Table 3.1). Noninfectious etiologies such as aphthous ulcers, Behçet syndrome, Stevens–Johnson syndrome, and Crohn’s disease can cause vulvar ulcers. Clinical presentation, involvement of other sites, and clinical course of the lesions, as well as laboratory tests are helpful in differentiating herpes from these systemic diseases [27, 29].
Management: Antiviral treatment of HSV infection with nucleoside analogues does not cure the infection, but rather aims for reducing recurrence and the risk of transmission. Treatment of recurrent episodes decreases the length of outbreaks and the severity of symptoms [23]. Daily dose of valacyclovir results in significant reduction in recurrence and viral shedding [28].
3.1.4 Gonorrhea
Clinical features: Gonorrhea is a common sexually transmitted infection caused by Neisseria gonorrhea, a gram-negative diplococcus. Gonorrhea is the second most commonly reported communicable disease [30]. Gonorrhea in women presents with urethritis, cervicitis , and vaginitis; however, a significant number of infected women are asymptomatic [30, 31]. The symptomatic patients present with pruritus, mucopurulant discharge, and urinary symptoms. Clinical exam may show friable cervix [31]. The infection can involve Bartholin’s glands , resulting in abscess formation [32]. Co-infection with Chlamydia is common. It is important to screen the women at high risk for STDs for gonorrhea because asymptomatic infections are common. Untreated gonorrhea, including asymptomatic infections, can progress to pelvic inflammatory disease and complications such as infertility and ectopic pregnancy [33].
Diagnostic methods: Microscopic findings are nonspecific as gonorrhea is not associated with marked inflammation [34]. Diagnosis can be made through a variety of techniques; by identifying intracellular organisms in gram-stained cervical smears, culture, and detection of antigen or nucleic acid in the sample. Nucleic acid amplification test (NAAT) has the highest sensitivity for detecting Neisseria gonorrhea [30]. Patients are treated by simultaneous ceftriaxone and azithromycin administration according to the current CDC guidelines [30].
3.1.5 Syphilis
Syphilis is a worldwide chronic infectious disease caused by spirochete Treponema pallidum. The primary mode of transmission is by sexual contact followed by vertical transmission from infected mother to child [35, 36]. Repeated oscillation in incidence of syphilis in the United States has been observed since 1940s, when penicillin was used to treat syphilis [37]. The rate of infection varies by population subgroups and is more common among people with limited access to health care and individuals with high-risk sexual behavior [35].
Clinical features: Acquired syphilis is divided into four stages (primary, secondary, latent, and tertiary), each present with different clinical manifestations. Venereal syphilis is acquired by direct penetration of spirochetes to the mucosa or skin during sexual contact [38]. The primary stage presents with a single chancre at the site of inoculation after an incubation period ranging from 10 to 90 days (an average of 3 weeks after exposure). Some cases show multiple primary lesions. The chancre in women most often occurs on the vulva, perineum, cervix, or oral mucosa and may be accompanied by painless regional lymphadenopathy. The skin lesion typically becomes indurated and progresses to a painless and non-purulent ulcer with clean base which heals spontaneously within 4–6 weeks [39, 40].
If untreated, T. pallidum disseminates throughout the body by hematogenous spread during the primary stage. Manifestations of secondary syphilis usually occur within 6–8 weeks of resolution of primary lesions [41]. Secondary syphilis may involve any organ but most commonly presents with disseminated heterogeneous mucocutaneous rash. The classic presentation includes generalized macular and papulosquamous skin eruption accompanied with systemic symptoms and generalized lymphadenopathy. Genital lesions are more common in women and range from macules and ulcerations to fleshy verrucous papules known as condylomata lata [40]. A variety of uncommon presentations such as nodular lesions and malignant lues (ulceronodular lesions) have been described [42,43,44].
In untreated patients, the lesions resolve over several weeks and the infection enters an asymptomatic “latent” stage. A subset of patients with latent infection progress to tertiary syphilis which may present with cardiovascular syphilis, neurosyphilis, and involvement of the skin, bones, or viscera with gumma [45, 46]. Vertical transmission of T. pallidum from mother to fetus may occur during pregnancy at any stage of infection, resulting in stillbirth or congenital syphilis. Syphilis and HIV coinfection is common, and the two diseases affect each other in several ways [47]. Clinical course of syphilis can be accelerated by HIV and result in atypical presentations and syphilis infection increases the risk of HIV transmission by breaking skin and mucosal barrier and increasing viral shedding [48,49,50].
Microscopic findings: Most primary lesions exhibit prominent endothelial swelling and proliferation with perivascular lymphoplasmacytic inflammation. The endothelial hyperplasia can result in endarteritis obliterans and subsequent ulceration. Epidermal hyperplasia and acanthosis is common [40, 51]. Secondary syphilis can demonstrate with a variety of histologic findings. Most cases show endarteritis, endothelial swelling, and interstitial and perivascular infiltrate in the dermis composed of lymphocytes, plasma cells, macrophages, and some neutrophils (Fig. 3.4). The epidermis shows variety of changes such as parakeratosis , exocytosis, spongiosis, and most frequently acanthosis [51,52,53]. Secondary syphilis skin lesions can demonstrate prominent lichenoid or psoriasiform features [54]. Condylomata lata show pronounced epithelial hyperplasia , elongated rete ridges, neutrophil exocytosis, and perivascular lymphoplasmacytic inflammation [54, 55]. Follicular microabscesses and pustules characterized by folliculocentric neutrophilic inflammation as well as patchy alopecia can occur [27]. Tertiary syphilis lesions often demonstrate dense lymphocytic and plasma cell infiltration of the dermis, granulomatous inflammation, and endarteritis obliterans [46, 54]. Silver stain or immunohistochemistry can be used to confirm the presence of Treponema within and around dermis vessels and in dermal–epidermal junction in primary and secondary stage lesions, and less commonly tertiary lesions. Non-treponemal spirochetes can cause false positive results [56].

Secondary syphilis: (a) Epidermal hyperplasia, acanthosis , and spongiosis with lymphoplasmacytic infiltrate in dermis. (b) Dermis demonstrates interstitial and perivascular lymphoplasmacytic infiltrate and vascular endothelial swelling and proliferation. (c) Warthin–Starry silver stain highlights spirochetes (arrows). (d) Immunohistochemical stain for Treponema highlights numerous spirochetes (Courtesy of Dr. Brian Hinds)
Diagnostic methods: Diagnosis can be made by detection of T. pallidum with dark field microscopy of primary or secondary lesions. Serologic testing is the main laboratory diagnostic method for secondary, latent, and tertiary syphilis; divided into non-treponemal and treponemal tests. Non-treponemal tests include the Venereal Disease Research Laboratory (VDRL) and the Rapid Plasma Reagin (RPR) which are useful for screening. Treponemal tests are used for confirming the infection and include the serum fluorescent treponemal antibody absorption test (FTA-ABS) and the microhemagglutination test for T. pallidum (MHA-TP) [39, 40]. Molecular detection of T. pallidum by PCR analysis have been developed and validated by some laboratories to detect the organism in serum, cerebrospinal fluid, amniotic fluid, lesion exudate, and fixed tissues [56, 57].
Differential diagnosis: Syphilis is called “great imitator” because it mimics the signs and symptoms of so many other diseases. Differential diagnoses of genital lesions in early syphilis include other infectious genital ulcer disease (chancroid , granuloma inguinale , lymphogranuloma venereum, and herpesvirus) Although, endothelial proliferation and perivascular lymphoplasmocytic inflammation are helpful hints to the diagnosis of syphilis. Secondary syphilis lesions can mimic inflammatory dermatoses such as lichen planus, eczema , psoriasis , and drug eruptions; however, involvement of deep dermis and predominance of plasma cells in the infiltrate is a clue for considering syphilis [41, 52]. In some cases dense inflammatory infiltrate may resemble lymphoma , but mixed population of inflammatory cells are in favor of a non-neoplastic process. Zoon’s vulvitis (plasmacytosis mucosae), a chronic inflammatory disease of unknown origin, demonstrates a band-like, dense mucosal infiltration of plasma cells admixed with lymphocytes and dilated dermal vessels. The absence of pronounced superficial and deep perivascular inflammation and vascular endothelial proliferation is helpful in differentiating these entities [27]. Condylomata lata can mimic verruca vulgaris and other conditions with epidermal hyperplasia . Granulomatous inflammation in later stages may simulate granuloma annulare, or other granulomatous diseases such as leprosy, tuberculosis , or sarcoidosis [27].
Management: According to CDC guidelines, primary, secondary, or early latent syphilis is cured by single intramuscular injection of long-acting Benzathine penicillin G (2.4 million units). Three doses of long-acting Benzathine penicillin G, administered intramuscularly at weekly intervals, are recommended for treatment of late latent syphilis. Treatment will kill the syphilis bacterium and prevent further damage, but will not repair existing damages [58].
3.1.6 Chancroid
The prevalence of chancroid has declined in the United States, but still occurs in developing countries. It is caused by the fastidious gram-negative coccobacillus called Haemophilus ducreyi [59, 60]. The transmission occurs by sexual contact and the incubation period is approximately 10 days [61, 62].
Clinical features: Clinically, it presents as tender erythematous papule that progresses into pustular stage, and then rupture to form single or multiple small genital ulcers (measuring 1–2 mm in diameter) that are painful, soft with purulent exudate, and can form coalescent lesions with ragged borders. Association with tender, suppurative, usually unilateral, inguinal lymphadenopathy (buboes formation) reinforces the diagnosis. The genital ulcers seen in chancroid can increase the transmission and acquisition of HIV infection, like in infections by herpes and syphilis. Differential diagnosis includes syphilis and herpes simplex [60, 62, 63].
Diagnostic methods: The diagnosis of chancroid is challenging, and the definitive diagnosis is achieved by identification of H. ducreyi on culture, which is considered the “gold standard” method. Multiplex PCR is not FDA approved, but available and validated in clinical laboratories [63].
Microscopic findings: Histology of the ulcers exhibit three distinct zones, from surface to depth, as follows: exuberant necrosis intermixed with neutrophils, erythrocytes, and fibrin; granulation tissue associated with degeneration and thrombosis of vessels; and dense lymphoplasmacytic infiltrate in the deep dermis (Fig. 3.5). Giemsa or gram stains may identify the bacteria at the surface of the lesion. Cytologic features of the ulcer’s exudate may show the bacteria in parallel chains (“school of fish”) [61, 62].

Chancroid ulcer with superficial fibrinopurulent exudate and necrotic debris associated with acute and chronic inflammatory cell infiltrate in dermis
Management: Patients are treated with antibiotics, and azithromycin and ceftriaxone regimen offers the advantage of single-dose therapy [60, 64].
3.1.7 Granuloma Inguinale (Donovanosis)
Klebsiella granulomatis (known as Calymmatobacterium granulomatis) is an intracellular gram-negative bacillus causative agent of granuloma inguinale (also called donovanosis or granuloma venereum). It is endemic in some tropical and developing areas, and very rare in the United States [65].
Clinical features: The disease presents as genital ulcers on vulva, vagina, or cervix that are painless, highly vascular (“beefy red appearance”) with rolled borders, and a friable bleeding base. Regional inguinal adenopathy is usually absent; however, subcutaneous granulomas (pseudobuboes) might occur. The incubation period is 1 week to 1 month after exposure. In addition to sexual contact, fecal contamination of the vulva or vagina has also been implicated. The ulcers can present in association with other sexually transmitted diseases or develop secondary superimposed bacterial infections. The lesions can spread and affect adjacent skin of perineum, thighs, and lower abdomen, and in severe cases may cause disfiguration of the genitals [59, 61, 62, 65].
Diagnostic methods: Smears of the lesion, stained by Wright or Giemsa, show mononuclear cells with numerous intracytoplasmic encapsulated ovoid bacteria (Donovan bodies). K. granulomatis is difficult to culture and the required specialized media is not available routinely. There are no FDA-cleared molecular tests for the detection of K. granulomatis DNA, but laboratories have developed and validated such tests. [63].
Microscopic findings: Histology of the lesion reveals an ulcer with central fibrinous exudate and necrosis, surround by pseudoepitheliomatous hyperplasia , underlay by granulation tissue with prominent vascularization and dense mixed inflammatory cell infiltrate (plasma cells and macrophages, predominantly). Histology sections stained with Warthin–Starry or Giemsa stains depict Donovan bodies found intracellularly (vacuoles of histiocytes) or extracellularly, which may appear as coccoid, coccobacillary, or bacillary organisms. The bipolar staining of the silver preparations confers the “safety pin” appearance of the bacteria. Electron microscopy may identify the organism within the phagosomes of macrophages [59, 62, 66].
Differential diagnosis includes nonhealing ulcers of squamous cell carcinoma , other STDs (chancroid , syphilis , and herpesvirus), infections caused by intracellular organism that affect histiocytes (leishmaniasis, histoplasmosis, and rhinoscleroma).
Management: The Centers for Disease Control and Prevention and the 2016 European guideline on donovanosis recommend treatment with azithromycin for at least 3 weeks and until all lesions have completely healed [59, 62, 65, 66].
3.1.8 Lymphogranuloma Venereum
Lymphogranuloma venereum (LGV) or lymphogranuloma inguinale is caused by the serotypes L1, L2, and L3 of Chlamydia trachomatis, an obligatory intracellular gram-negative bacterium [67]. The disease is more common in men, frequently found in tropical and subtropical areas of the world [68,69,70]. This sexual transmitted disease has a triphasic clinical presentation. The primary infection, after an incubation period of 3–30 days, presents with genital small painless papules, which become self-limiting ulcers, and frequently goes unnoticed. The secondary infection, after a few weeks, presents with regional lymphadenopathy and sometimes constitutional symptoms. The inguinal lymph nodes are more commonly involved in men, given the lymphatic drainage of the vagina and cervix is to the retroperitoneal rather than the inguinal lymph nodes. The “groove sign,” thought to be pathognomonic for LGV, refers to the presence of adenopathy above and below the inguinal ligament, occurs in 10–20% of cases. The lymph nodes become enlarged, tender (buboes formation), and may develop draining sinuses. The third phase of the disease, more common in women, consists of chronic pelvic lymphangitis with fibrosis of the genital tract that can lead to lymphatic obstruction, causing elephantiasis of the genitalia, fistulas, and strictures of vagina and rectum [62, 67, 71].
Diagnostic methods: The diagnosis of LGV is difficult given lack of specific clinical presentation and standardized laboratory assays for this pathogen. The clinical suspicion, epidemiologic information, and exclusion of other entities can guide the diagnosis. Specimens from infected sites can be tested for C. trachomatis by culture, direct immunofluorescence, or nucleic acid detection. PCR-based genotyping can be used to differentiate LGV from non-LGV C. trachomatis, but it is time consuming and not widely available. Chlamydia serology may help reach the diagnosis, but lacks specificity [72].
Microscopic Findings: The ulcers are rarely biopsied, given the absence of clinical presentation. Histology demonstrates dense underlying lymphoplasmocytic infiltrate, small foci of necrosis, and granulation tissue. The involved lymph nodes develop stellate abscesses with coalescence of necrotic foci surrounded by poorly formed palisade of epithelioid cells and histiocytes. Sinus formation also occurs. In later lesions, there is variable fibrosis. C. trachomatis has been identified by numerous stains in inguinal lymphadenitis as intravacuolar organisms in macrophages (measuring 0.2–2.0 μm in diameter) [59, 71].
Different diagnosis includes other causes of inguinal adenopathy in association with genital ulcers (syphilis , HSV-2, and chancroid ) or without ulcers (suppurative lymphadenitis caused by bacteria, cat-scratch disease, bubonic plague, tuberculous lymphadenitis, HIV infection, and lymphoma , among others) [59, 71].
Management: Medical therapy includes antibiotics (doxycycline is recommended), and aspiration of buboes to prevent the formation of sinus tract formation [67, 71].
3.1.9 Chlamydial Infection
Chlamydial infection is the most common sexually transmitted bacterial infection in the United States, caused by Chlamydia trachomatis, a gram-negative obligate intracellular pathogen [73]. C. trachomatis may involve lower urogenital tract (mainly endocervical mucosa), resulting in cervicitis , urethritis, and Bartholin’s glands infection [74]. Symptomatic infections present with mucopurulent vaginal discharge and dysuria, although the infection is often asymptomatic. Untreated infection may result in pelvic inflammatory disease and its associated complications, including infertility and ectopic pregnancy , even when the infection is asymptomatic [75, 76].
The microscopic findings are nonspecific, showing chronic inflammation and reactive changes in epithelial cells. In some cases, lymphoid follicles with well-formed germinal centers are reported [34]. Immunoperoxidase staining for C. trachomatis can identify endocervical cells containing chlamydial bodies [77]. Diagnosis is made by isolation of C. trachomatis through culture or by detection of antigen or nucleic acid in first-catch urine or vaginal/cervical swab specimens. NAATs have the highest sensitivity, therefore are the recommended tests for detecting C. trachomatis infection. The current CDC guidelines recommend antibiotics treatment by a single dose azithromycin or 7 days of doxycycline [73].
3.1.10 Human Papillomavirus
Human Papillomavirus (HPV) infection is one of the most common sexually transmitted diseases and is responsible for a large number of anogenital cancers and warts in the United States [78]. Most sexually active individuals become infected with HPV and the course of the disease is usually asymptomatic and self-limited. Numerous subtypes of the virus have been identified which are further classified as oncogenic (e.g., high-risk, HPV types 16 and 18) and nononcogenic (e.g., low-risk, HPV types 6 and 11). Vulvar HPV-related lesions will be briefly discussed in this chapter, and other HPV-associated diseases will be further detailed in other chapters. Common manifestations of HPV infection in vulvar region include condyloma acuminatum (HPV types 6, 11), verruca vulgaris (HPV type 2), and giant condyloma (discussed under Sect. 3.5) [54, 59, 78].
3.1.10.1 Condyloma Acuminatum
Condyloma acuminata are common lesions of the vulva, vagina, and perianal region in adults, most commonly associated with HPV 6 or 11. Transmission is by skin-to-skin contact, including sexual intercourse or any other contact involving the genital area, even in the absence of visible warts [78].
Clinical features: Codyloma acuminatum presents as single or multiple lesions (filiform, plaque-like, or flat) that are flesh-colored or pigmented, and may extend to the perineum and perianal areas. Condyloma acuminatum are usually painless, unless involved by secondary infection [54, 59, 78].
Microscopic findings: Condyloma acuminatum shows papillomatous epidermal hyperplasia with hyperkeratosis , parakeratosis , accentuation of the granular layer , prominent fibrovascular cores, and basal cell hyperplasia . The surface of the lesion may display koilocytosis with squamous cells showing binucleation or multinucleation, perinuclear vacuolization and irregular nuclear contour. Chronic inflammatory infiltrate may be present. Peculiar histologic findings are seen in condylomata treated with resin of podophyllin. The squamous epithelium can show nuclear enlargement, increased number of mitosis, apoptotic keratinocytes, and pallor of superficial cells (Fig. 3.6) [54, 59, 79].

Condylomata acuminatum: (a) Hyperplastic epidermis with acanthosis , parakeratosis , papillomatosis, prominent granular layer , and numerous koilocytes . (b) The koilocytes show irregular and wrinkled nuclei
Diagnostic methods: Diagnosis is usually made by clinical inspection. Biopsy can confirm the diagnosis, and it is indicated in immunocompromised patients, lesions that worsen during therapy, and concerning atypical lesions that are pigmented, indurated, ulcerated, fixed to the underlying tissue, and easily bleed [78].
Differential diagnosis: includes vulvar intraepithelial neoplasia , which shows prominent nuclear atypia (including nuclear pleomorphism and hyperchromasia), increased number of mitotic figures throughout the epithelium, and minimal maturation. Verrucous carcinoma is another differential diagnosis and displays minimal cytologic atypia, no koilocytosis, abundant keratin between papillae, and broad-based rete ridges with pushing margins. Long-standing condylomata lesions may lack koilocytosis and can resemble seborrheic keratosis [54, 59, 62]. Papillary immature metaplasia (PIM) has been described in the squamous columnar junction of the anus and cervix, and is a type of exophytic low-grade squamous intraepithelial lesion . However, it distinguishes from condyloma acuminatum by the presence of immature squamous cells on the surface of the filiform papillary projections of the lesion. PIM can be easily misdiagnosed as high-grade squamous intraepithelial lesion (HSIL) and awareness of this entity should be acknowledged. PIM lacks the nuclear atypia and conspicuous mitotic activity seen in HSIL. Immunostain for p16 is usually diffusely positive in HSIL, and negative in PIM [79,80,81].
Management: depends on the extent of the disease and identification of pathologic precancerous lesions. Certain antiviral therapy is not recommended, given that most lesions are self-limited. Excision, cryotherapy, and other types of ablation can be used. Lesions may also involute spontaneously within 1 year [78].
3.1.10.2 Verruca Vulgaris
Verruca vulgaris or common warts are usually seen in children and young adult and present as solitary, sometimes multiple, flesh-colored excrescences. They are usually asymptomatic, but can elicit pruritus, irritation, or bleeding. Microscopically, verruca vulgaris show a classic filiform surface architecture with parakeratosis , orthokeratosis, and hypergranulosis underlying a bland squamous epithelium with prominent papillary dermal vessels. The diagnosis is usually clinical. HPV genotyping can be used to differentiate verruca vulgaris from condyloma acuminatum in genital warts found in children, to assess for sexual abuse. The lesions can be excised or ablated (e.g., cryotherapy and electrocauterization) [54, 59].
3.1.11 Human Immunodeficiency Virus
The integrity of the vulvar and vaginal mucosal barrier is crucial in preventing pathogen invasion. The cellular immunity, microbiota, and mucus are some of the elements that maintain the intactness of tissue barrier. Mucosal inflammation increases the risk of HIV infection by elevating pro-inflammatory cytokines that disrupt the mucosa via neutrophil proteases activity, and increasing frequency of CD4+ T-cells, which are target cells of the virus. There is a high epidemiological association of STDs and HIV acquisition. Although the pathogenesis is unclear, HIV infection alters the integrity of the mucosal barrier and plays a role in acquisition of other STDs. Loss of Th17 cells is hypothesized to cause damage of the tight epithelial barrier allowing microbial translocation. In addition, HIV is capable of inducing inflammation by stimulating cells of the innate and adaptive immune system. Dysbiosis can also affect the immune cells in the mucosal surface and drive HIV infection. HIV-associated vulvar ulcers, without involvement of other pathogens are rare and few cases reported in literature describe the link between idiopathic vulvar ulcers and HIV infection that clinically present as multiple painful aphthous ulcers [59, 82,83,84,85].
3.2 Common Infections Not Typically Linked to Sexually Transmitted Diseases
3.2.1 Candida
Vulvovaginal Candidiasis (VVC) is a common infection of female genital tract. Candida albicans , an opportunistic yeast and a part of gastrointestinal tract flora, is responsible for 90% of VVCs [86]. Most of the remaining cases are caused by C. glabrata and C. tropicalis which are more resistant to treatment. Approximately 20–30% of asymptomatic women are carriers of candida in their lower genital tract. Epidemiologic data is limited due to the availability of over the counter treatment, yet it is estimated that up to 75% of women are affected at least once during their lives. Nearly 5–8% of women of reproductive age have recurrent vulvovaginal candidiasis [87].
VVC is not a sexually transmitted disease, but is more common in women who are sexually active. Risk factors for candida vulvovaginitis include pregnancy, diabetes mellitus, immunosuppression (e.g., HIV disease), and broad-spectrum antibiotic use [88, 89]. Menopausal women who receive exogenous estrogen replacement therapy are at higher risk of vulvovaginal candidiasis [90]. Studies have suggested that individuals with genetic factors such as nonsecretor phenotype of the ABO-Lewis blood group are at higher risk for recurrent VVCs [87, 91].
Clinical features: VC manifests by vulvar erythema, itching, irritation, and abnormal “cheese-like” or watery vaginal discharge. The infection can also result in candida intertrigo in inguinal region characterized by red lesions without central clearing and satellite rashes [91, 92].
Microscopic findings: On cytology smears, Candida organisms appear as eosinophilic yeast and pseudohyphae. Spearing of squamous cells, as if skewered by the pseudohyphae, is a frequent finding [11]. Histologic examination of vulva may show epidermal spongiosis, acanthosis , hyperkeratosis , and parakeratosis with subcorneal neutrophilic pustules (Fig. 3.7). Candida hyphae, pseudohyphae, and yeasts are highlighted by fungal stains (Grocott-Gomori methenamine silver stain or periodic acid–Schiff) in keratin layer [27].

Vulvovaginal candidiasis : (a) Vulvar epidermal spongiosis and associated dermal edema with Candida organisms and neutrophils in epidermis. (b) Epidermal parakeratosis with Candida pseudohyphae (arrow) and yeast in the thickened keratin layer. (c) Papanicolaou-stained cervical smear shows Candida pseudohyphae (arrow) and spearing of squamous cells
Diagnostic methods: Diagnosis is based on identifying the organism by wet preparation, potassium hydroxide microscopy, culture, or molecular DNA detection of Candida [86, 88]. The patients are treated by short-course topical azole drugs [89].
3.2.2 Dermatophytosis
Tinea cruris (jock itch) is a superficial dermatophyte infection involving groin, inner thighs, perianal area, and rarely vulva. Trichophyton rubrum is the most common causative organism [93]. The patient presents with pruritic, sharply demarcated, discolored rashes with erythematous scaly borders, and sometimes with vesicles and pustules [94]. Biopsy findings are usually nonspecific, showing epidermal acanthosis , parakeratosis , spongiosis, and fungal yeast and hyphae (Fig. 3.8) [27]. Contact with contaminated fomites, tight clothing, and conditions such as excessive sweating and obesity that provide increased temperature and moisture in skin folds are predisposing factors [95]. Tinea cruris can often be diagnosed by a KOH preparation or culture. This infection usually responds to topical treatment, but oral antifungals may be indicated for extensive disease [93].

Dermatophytosis: Epidermal hyperkeratosis and parakeratosis with fugal organisms in the thickened keratin layer on hematoxylin & eosin (a) and periodic acid–Schiff (b) stains
Deep dermatophytosis of the vulva is a rare infection mainly caused by T. mentagrophytes and Microsporum canis, most commonly affecting patients using topical steroids. Dermatophyte infection of the hair follicle and dermis evolves into scaly, erythematous plaques in vulva. The lesions may result in kerion formation or nodular granulomatous perifolliculitis, known as Majocchi’s granuloma. Biopsy shows inflammation, granulomatous perifolliculitis, or cellulitis and abscess formation with or without fungal hyphae [96,97,98].
3.2.3 Bacterial Vaginosis
Bacterial vaginosis (BV) is the most common vaginal infection in women of reproductive age, affecting up to 29% of women in the United States. It is a polymicrobial syndrome caused by shift in vaginal microbial flora as a result of reduction in the normal Lactobacilli and overgrowth of anaerobic and facultative bacteria [99]. Molecular-based techniques have identified multiple bacterial vaginosis-associated agents including Gardnerella species, Mobiluncus species, Atopobium species, and Mycoplasma hominis [100]. Recent studies confirm the key role of Gardnerella vaginalis (GV) in pathogenesis of BV [101].
The exact etiology and epidemiology of BV is not clear and the role of sexual transmission is debated, although considerable evidence shows a significant association between BV and sexual activity with new and multiple partners [102]. Recent studies have emphasized on the sexual transmission of GV and suggest BV is started when GV adheres to host epithelium and creates a biofilm community in the vaginal environment [101]. BV is a risk factor for acquiring various sexually transmitted diseases and increases the risk of pelvic inflammatory disease , preterm labor, chorioamnionitis, and endometritis [99]. Importantly, BV has been associated with an increased risk of HIV acquisition and transmission. Studies have shown that interaction between epithelial cells and BV-associated species resulted in upregulation of cytokines and secretion of HIV-enhancing proteins that increases susceptibility to HIV infection [103, 104].
Clinical features: The infection presents with thin, mal-odorous vaginal discharge without typical signs of inflammation. Many affected women are completely asymptomatic [102].
Microscopic findings: On cytology smears (Fig. 3.9), BV present with squamous cells covered by small coccobacilli obscuring the cell edges, known as clue cells . Lactobacilli are usually absent and background is clean in liquid-based smear, given no to minimal inflammatory response [11].

Liquid-based preparation reveal squamous cells covered with coccobacilli (“clue cells ”) suggestive of bacterial vaginosis
Diagnostic methods: The diagnosis is usually made by applying clinical criteria, measuring vaginal fluid pH (>4.5), a positive whiff test (production of a fishy odor after adding 10% potassium hydroxide to vaginal fluid), gram stain (substitution of gram-positive rods and lactobacilli by gram-negative and gram-variable organisms), or molecular DNA detection [105].
3.2.4 Folliculitis and Other Bacterial Infections of Skin and Soft Tissue
Hair bearing skin of labia majora and pubic area can be involved by superficial and deep folliculitis secondary to bacterial infection of the hair follicles by Staphylococcus aureus. Trauma due to removing hair by shaving or waxing and wearing tight underwear are predisposing factors. The clinical and histologic appearance are similar to folliculitis from other body sites, presenting with papules, pustules, and granulomatous inflammation (Fig. 3.10) [98]. Other less common pathogens include Pseudomonas aeruginosa (hot tub folliculitis), Malassezia, and dermatophytes [106,107,108]. Exfoliative toxins of S. aureus can result in vesicles and blisters in genital area [98].

(a, b) Folliculitis demonstrates mixed acute and chronic inflammation surrounding hair follicle with superficial ulcer
Vulvar cellulitis is bacterial infection of the dermis, usually caused by Streptococci group A and S. aureus, which affects the dermis in high-risk individuals including women with diabetes mellitus, obesity, pregnancy, and immunosuppression. This condition is often associated with fever, malaise chills, and nausea. Vulvar abscess formation often occurs due to progression of skin and hair follicle infections. These infections are often polymicrobial and Methicillin-resistant Staphylococcus aureus (MRSA) is the most common pathogen, isolated in 43–64% of cultures [32, 109,110,111,112,113,114]. Necrotizing fasciitis (or Fournier’s gangrene ) is a life-threatening progression of vulvar cellulitis that causes extensive necrosis of the subcutaneous tissue. Tissue debridement and surgical reconstruction are the most important course of treatment. Histopathologic examination (Fig. 3.11) shows extensive necrosis with fascia involvement, abscess formation, vasculitis, and microvascular thrombosis [110, 114].

Necrotizing fasciitis shows extensive necrosis with fascia involvement, abscess formation, vasculitis, and microvascular thrombosis
Bartholin gland obstruction and abscess formation affects approximately 2% of women. The infection is caused by mixed vaginal flora (Bacteroides, Escherichia coli, S. aureus) in nearly 80% of the cases; however, Neisseria gonorrhoea and rarely Chlamydia can cause this infection [32]. This condition presents with painful unilateral erythematous swelling in the vaginal introitus, and sometimes purulent discharge [32].
Periclitoral abscess is a rare condition with only few cases reported in literature. A significant number of these cases have occurred after local procedures, mostly after female circumcision [115,116,117]. In such cases, abscess formation is due to infected postsurgical inclusion cysts or less likely hematomas [116, 118]. Spontaneous periclitoral abscess formation without any previous surgery has been reported; however, due to rarity of this condition, association with specific causes and pathogens is unknown [116].
3.3 Infestations
3.3.1 Pediculosis Pubis
Pediculosis pubis (crab lice) is a highly contagious infestation caused by parasite Phthirus pubis. The disease is typically transmitted sexually; however, indirect infection through contact with infested objects is possible. Thirty percent of patients will have coexisting sexually transmitted disease. The crab louse is not a vector for systemic disease and commonly causes local symptoms by infesting pubic hair [119, 120].
Patients’ main complaint is of itch in the pubic area. The affected skin can show red papules at the site of lice bites (Fig. 3.12). The host DNA can be extracted from lice [119]. Light blue-gray macules (maculae ceruleae) on the lower abdomen and thighs are characteristic findings of established infestation due to deep dermal hemosiderin deposition. Secondary superimposed infection may occur as a result of scratching. The diagnosis is made by spotting the lice and nits (eggs) attached to the genital area hair (Fig. 3.12) [119,120,121,122].

Pediculosis pubis: (a) The affected skin shows red papules at the site of lice bites. (b) Lice and nits (eggs) attach to the genital area hair
3.3.2 Scabies
Scabies is a contagious skin infestation caused by a human mite, Sarcoptes scabiei var. hominis. The mite burrows into and lives in the stratum corneum of the skin, commonly in finger webs and wrists. Involvement of genitalia usually presents with intensely pruritic papular rash or eczematous lesions. The parasite is usually transmitted by direct skin-to-skin contact, but infection by infested bedding or cloths is possible. The diagnosis of scabies can sometimes be confirmed microscopically by presence of mites, eggs, or fecal material in skin biopsy or scraping. Skin biopsy (Fig. 3.13) usually demonstrates features of hypersensitivity dermatitis with epidermal spongiosis and perivascular inflammation in dermis, composed of lymphocytes and eosinophils [122, 123]. Crusted scabies, formerly known as Norwegian scabies, is a severe form of infestation usually seen in immunocompromised patients and rarely involves vulvar region. Patients characteristically develop generalized thick, hyperkeratotic lesions simulating psoriasis , drug eruptions, and eczemas [124].

Scabies : (a) The patient presents with pruritic papular rash or eczematous lesions. (b) Hyperparakeratotic, acanthotic epidermis with scabies mites (arrow)
3.4 Other Rare Infections
3.4.1 Epstein-Barr Virus
Genital ulceration is rarely caused by primary Epstein–Barr virus (EBV) infection. This condition, known as Lipschütz’s ulcer, is a non-sexually transmitted disease and primarily affects adolescent females (mean age of 14.5 years). Although several reports have outlined EBV shedding from genital tract secretions following acute systemic infection, genital ulceration caused by EBV are rarely described [125].
Patients typically present with one or multiple very painful ulcers, with purple-red irregular edges and clean or fibrinous base involving labia minora . Lymphadenopathy distant from the site of ulceration is common. Urinary symptoms such as dysuria and urine retention may be caused by the ulcers. Preceding prodromal systemic symptoms such as fatigue, headache, and low-grade fever are common and the majority of patients develop symptoms of mononucleosis [126]. The vulvar ulceration are more likely a manifestation of viremia and circulating infected B lymphocytes. The pathophysiology of ulceration is not clear; some believe a cytotoxic immune response to immune complex deposition triggers a type III hypersensitivity reaction, while others propose the ulcers are a manifestation of direct damage by EBV replication in the keratinocytes [125, 127]. Differential diagnoses include ulcerative STDs including HSV, chancroid , and syphilis.
Diagnosis is mainly clinical and based on excluding other causes of genital ulceration; confirmation can be made by detection of EBV-DNA by PCR examination of vulvar swabs or serologic evidence of acute EBV infection. The histologic findings are nonspecific, showing ulceration and underlying vasculitis with extensive mixed inflammatory cell infiltrate in dermis. This condition is self-limiting and ulcers usually resolve within 2–6 weeks without scarring [125].
3.4.2 Cytomegalovirus
Human Cytomegalovirus (CMV), a member of Herpesviridae family, is a ubiquitous virus that affects most of the world population. Immunocompetent hosts are generally asymptomatic or present with mononucleosis syndrome; however, it can cause life-threatening disease in immunocompromised patients. Like other members of Herpesviridae family, CMV establishes a lifelong latent infection of the host [128]. CMV can be identified in the cervix of up to 29% of women with normal cervical smears. The rate of CMV DNA detection in the cervical secretions has been as high as 66% in HIV-infected women [129, 130]. Symptomatic CMV infections of female genital tract are rare. Cases with anogenital ulcers and erosions have been reported in both healthy and immunocompromised patients [131, 132].
Histologically CMV is diagnosed by characteristic enlarged cells with large eosinophilic nuclear inclusions surrounded by a clear halo (owl’s eye) and intracytoplasmic granulations (Fig. 3.14). CMV inclusions are mainly found in the endocervical glandular epithelial cells and also in endothelial and mesenchymal cells [132]. In addition, CMV inclusions have rarely been detected in cervical smears [129]. When detected on cervical smears, CMV-infected cells are usually endocervical cells with characteristic large central eosinophilic inclusion with a prominent halo and small cytoplasmic basophilic inclusions [11].

Cytomegalovirus : (a) Epidermal hyperkeratosis and acanthosis with CMV inclusions in dermal vessels (arrows). (b) Characteristic “owl’s eye” inclusions in infected endothelial cells (arrow). (c) Immunohistochemical stain for CMV highlights the infected cells
3.4.3 Schistosomiasis
Schistosomiasis is an endemic parasitosis of countries in Africa, Middle East, South America, and Southeast Asia. Schistosoma haematobium, S. japonicum, and S. mansoni are the main species that infect humans, and are specific to certain geographic areas. The disease is acquired percutaneously by infection with cercariae found in contaminated freshwater of endemic areas. The inoculation of the cercariae can cause acute symptoms such as local dermatitis, and systemic prodromal symptoms, e.g., fever, headache, and cough. The adult schistosomes reside inside blood vessels of the human host’s body, and are usually seen in the superior mesenteric veins, the venous plexus of bladder, and rectal venules. The worm is able to move to different venous sites, and produces numerous eggs that can surface through the lumen of the intestines or the bladder urothelium, and be expelled. The eggs can also travel to different sites of the body and cause serious pathologies [133, 134].
Infection of the lower female genital tract by schistosomiasis may present as dermatitis of the vulvar skin caused by inoculation of the cercariae, or by an inflammatory reaction around the trematode’s eggs. Clinical presentation includes papules, plaques, ulcers, and/or extensive wart-like lesions that can be very similar to condyloma acuminata [59, 135, 136]. Schistosomiasis also affects the uterine cervix and causes rubbery papules, sandy patches, and neovascularization on the surface of the cervix. Histologically, the lesion encompasses mixed inflammatory cell infiltrate with neutrophils and eosinophils, worms or often calcified ova with adjacent granulomatous reaction, occasionally necrosis, and dense fibrosis (Fig. 3.15) [59]. In addition to biopsy of the lesions, the diagnosis can be made by detection of eggs in urine or feces, or serology testing. The later test has its limitations and cannot distinguish resolved versus active infection [133]. Female genital schistosomiasis has been proposed as a risk factor for HIV infection. However, no study was able to demonstrate a clear causality between the two entities, and confounding factors can also play a role in this association. Treatment of choice is the anti-helminthic praziquantel [133, 137,138,139,140].

Calcified Schistosoma ova (arrow) with adjacent mixed inflammatory cell infiltrate and multinucleated giant cells
3.4.4 Varicella Zoster
Varicella zoster virus (VZV) is a double-stranded DNA neurotropic human virus from Herpesviridae family. Primary infection with VZV causes chicken pox, a self-limited childhood disease presenting with disseminated vesicular rashes and fever. Shingles or herpes zoster is a result of reactivation of latent VZV, which establishes a dormant state in nerve ganglia after primary infection. Reactivation of VZV usually occurs in older adults and immunocompromised individuals, due to decreased immunity to the virus [141, 142].
Isolated herpes zoster of vulva is a rare cause of genital ulcers, triggered by reactivation of the VZV residing in sacral sensory ganglia [143, 144]. Lesions present with a prodrome of pain or burning sensation, followed by clusters of painful vesicles, pustules, and erosions in a dermatomal distribution. The lesions may be confused with herpes simplex; however, vulvar zoster is unlikely to recur in the same location or cross the midline. Post-herpetic neuralgia is a common complication and should be considered in vulvodynia patients [145]. Diagnosis can be made by detection of VZV from the lesions with culture, PCR, or direct Immunofluorescence assays (DFA). Biopsy samples are rarely taken which shows changes similar to HSV infection. Immunohistochemical staining can differentiate varicella zoster from herpes zoster .
3.4.5 Malakoplakia
Malakoplakia is an uncommon chronic inflammatory process, first described by Michaelis and Gutmann in 1902, which most commonly affects the urinary tract mucosa [146]. Female genital tract malakoplakia is rare and most reported cases describe vaginal involvement [146,147,148]. The pathogenesis of malakoplakia has not been fully elucidated, but several factors including microorganisms, abnormal immune response, and impaired macrophage function have been implicated [149]. Escherichia coli is found in majority of the cases; however, several organisms such as Mycobacterium tuberculosis , Proteus, and Staphylococcus aureus have been implicated [149].
Malakoplakia can present as mucosal plaques, nodules, and mass-like lesions which in some cases can mimic tumor [146, 148]. Microscopic examination shows sheets of large, granular histiocytes with eosinophilic to vacuolated cytoplasm containing granular basophilic periodic acid Schiff-positive, diastase-resistant inclusions and calcified Michaelis–Gutmann bodies. Michaelis–Gutmann bodies often exhibit a targetoid appearance and stain positively by Von Kossa (calcium) stain [149].
3.5 Vulvar Infections Associated with Immunosuppression
3.5.1 Generalized Genital Warts in Patients with Immunosuppression
Condylomata acuminata or anogenital warts are caused by HPV (90% is due to types 6 or 11) [78]. Patients with HIV infection or other causes of immunosuppression are prone to develop numerous and extensive lesions that are also more resistant to standard therapies [114, 150,151,152]. The reduction of CD8+ cytotoxic T-lymphocyte reactivity to HPV oncoproteins E6 and E7 (cell-mediated immunity) leads to inadequate elimination of the virus. Both transplant recipients and HIV-infected patients have been found to have a higher prevalence of high-risk HPV types. HIV patients have in particular HPV-16 type in their condylomata, which can be associated with foci of high-grade squamous intraepithelial lesions [59, 78, 114, 152].
Physical examination is sufficient for the diagnosis; however, biopsy of suspected wart can be used to confirm diagnosis and rule out malignancy. The histology of condilomata is the same as the lesions seen in immunocompetent individuals, and show acanthosis , dyskeratosis , parakeratosis , hyperkeratosis , papillomatosis, and a prominent granular layer . Koilocytosis is present in the superficial epithelial cells, and binucleated and multinucleated squamous cells are frequent findings (Fig. 3.6). Immunosuppressed patients are more likely to progress with dysplasia and invasive squamous cell carcinoma , regardless of the lesion’s site (vulva, vagina, cervix, anus, or perineal skin). Other type of malignant transformation of HPV infection to be considered in immunosuppressed population, although very rare, is giant condyloma acuminatum or Buschke–Lowenstein tumor (BLT), which is a low-grade squamous cell carcinoma that manifest as a large exophytic mass that can form fistulas, abscesses, and local neoplastic invasion. Histologically, BLT is very similar to condylomata, but tends to infiltrate deeper tissue layers with pushing infiltrating pattern. Malignant transformation to invasive carcinoma is determined by the presence of numerous mitotic figures and frank invasion. The CDC supports course of treatment for all patient with HPV infection, irrespective of their immune status [59, 62, 78, 153].
3.5.2 Tuberculosis
Tuberculosis rarely involves the lower female genital tract. The disease may affect the vulva, vagina, and cervix directly by coitus of a partner with genitourinary tuberculosis, or indirectly by secondary spread of tuberculosis from other sites. The most common primary source of the infection is pulmonary tuberculosis. However, genital tuberculosis of different sites such as fallopian tube and endometrium can also disseminate to the lower genital tract. Genital tuberculosis should be considered in patients with immunosuppression and latent tuberculosis, as well as in patients with active disease. Special attention should be drawn to immunocompromised patients with HIV infection, diabetes mellitus, corticosteroid use, end-stage renal disease, and to the patients treated by tumor necrosis factor-alpha inhibitors [59, 154].
Given the indolent course of the disease, the mycobacterium can reside in the tissue for an extended period before leading to clinical manifestation. Diagnosis can be made histologically with classical presentation of caseating granulomas characterized by central caseous necrosis, epithelioid histiocytes, and giant cells (Fig. 3.16). Ziehl–Neelsen stain can demonstrate the acid-fast Mycobacterium tuberculosis. Unfixed specimen should be considered for microbiologic testing. According to the patient’s immune response, caseous necrosis may be absent and the differential diagnosis includes foreign body giant cell granulomas (usually secondary to surgical procedures), lymphogranulomas venereum, schistosomiasis, sarcoidosis, granulomatous syphilis , and invasive cervical cancer. Diagnostic tests used for systemic tuberculosis, e.g., interferon-gamma assay, can also aid in the diagnosis of genital tuberculosis. Antituberculous therapy for genital disease follows the same guidelines used for pulmonary tuberculosis [154].

Tuberculosis involving dermis. (a, b) Caseating granulomas reveal central caseous necrosis, epithelioid histiocytes, and multinucleated giant cells. (c) AFB stain highlights mycobacteria in the granuloma (arrows)
3.5.3 Bacillary Angiomatosis
Bacillary angiomatosis (BA) is caused by two closely related gram-negative coccobacilli, Bartonella henselae and Bartonella quintana, and occurs primarily in immunocompromised patients. We are aware of three cases of vulvar BA reported in the literature. Clinical presentation is similar to BA cutaneous lesions of other sites, and appear as red-purple nodules with vascular formation that easily bleed with trauma. Histologic examination reveals vascular proliferations that are lined by prominent epithelioid endothelial cells in a background of lymphocytes, histiocytes, and neutrophils. Giemsa, Warthin–Starry, or Grocott-Gomori methenamine silver stain demonstrates hazy clumps of bacteria that characterize bacillary angiomatosis. Immunohistochemical techniques, culture, and polymerase chain reaction based methods have also been used to identify the organisms [62, 155,156,157]. Several antibiotics are effective against Bartonella infections, and macrolides are commonly used. Different diagnosis includes other vascular lesions such as pyogenic granuloma, Kaposi sarcoma, and cherry angioma, among others [62, 155].
References
Meites E. Trichomoniasis: the “neglected” sexually transmitted disease. Infect Dis Clin N Am. 2013;27(4):755–64.
Benchimol M. Trichomonads under microscopy. Microsc Microanal. 2004;10(5):528–50.
Schwebke JR, Burgess D. Trichomoniasis. Clin Microbiol Rev. 2004;17(4):794–803, table of contents.
Sutton M, Sternberg M, Koumans EH, McQuillan G, Berman S, Markowitz L. The prevalence of Trichomonas vaginalis infection among reproductive-age women in the United States, 2001–2004. Clin Infect Dis. 2007;45(10):1319–26.
Meites E, Gaydos CA, Hobbs MM, Kissinger P, Nyirjesy P, Schwebke JR, et al. A review of evidence-based care of symptomatic Trichomoniasis and asymptomatic Trichomonas vaginalis infections. Clin Infect Dis. 2015;61(Suppl 8):S837–48.
Van Der Pol B. Clinical and laboratory testing for Trichomonas vaginalis infection. J Clin Microbiol. 2016;54(1):7–12.
Harp DF, Chowdhury I. Trichomoniasis: evaluation to execution. Eur J Obstet Gynecol Reprod Biol. 2011;157(1):3–9.
Aslan DL, Gulbahce HE, Stelow EB, Setty S, Brown CA, McGlennen RC, et al. The diagnosis of Trichomonas vaginalis in liquid-based Pap tests: correlation with PCR. Diagn Cytopathol. 2005;32(6):341–4.
Lara-Torre E, Pinkerton JS. Accuracy of detection of Trichomonas vaginalis organisms on a liquid-based papanicolaou smear. Am J Obstet Gynecol. 2003;188(2):354–6.
Noel JC, Engohan-Aloghe C. Morphologic criteria associated with Trichomonas vaginalis in liquid-based cytology. Acta Cytol. 2010;54(4):582–6.
Nayar R, Wilbur DC. The Bethesda system for reporting cervical cytology: definitions, criteria, and explanatory notes. Cham: Springer; 2015. Available from: SpringerLink. Restricted to UC campuses https://doi.org/10.1007/978-3-319-11074-5.
Centers for Disease Control and Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, Division of STD Prevention. Trichomoniasis.
Shisler JL. Immune evasion strategies of molluscum contagiosum virus. Adv Virus Res. 2015;92:201–52.
Smith KJ, Yeager J, Skelton H. Molluscum contagiosum: its clinical, histopathologic, and immunohistochemical spectrum. Int J Dermatol. 1999;38(9):664–72.
Tyring SK. Molluscum contagiosum: the importance of early diagnosis and treatment. Am J Obstet Gynecol. 2003;189(3 Suppl):S12–6.
Gur I. The epidemiology of Molluscum contagiosum in HIV-seropositive patients: a unique entity or insignificant finding? Int J STD AIDS. 2008;19(8):503–6.
Ishikawa MK, Arps DP, Chow C, Hocker TL, Fullen DR. Histopathological features of molluscum contagiosum other than molluscum bodies. Histopathology. 2015;67(6):836–42.
Chentoufi AA, Benmohamed L. Mucosal herpes immunity and immunopathology to ocular and genital herpes simplex virus infections. Clin Dev Immunol. 2012;2012:149135.
Fatahzadeh M, Schwartz RA. Human herpes simplex virus infections: epidemiology, pathogenesis, symptomatology, diagnosis, and management. J Am Acad Dermatol. 2007;57(5):737–63; quiz 64–6.
Stanberry L, Cunningham A, Mertz G, Mindel A, Peters B, Reitano M, et al. New developments in the epidemiology, natural history and management of genital herpes. Antivir Res. 1999;42(1):1–14.
Money D, Steben M. No. 207-Genital herpes: gynaecological aspects. J Obstet Gynaecol Can. 2017;39(7):e105–e11.
Johnston C, Corey L. Current concepts for genital herpes simplex virus infection: diagnostics and pathogenesis of genital tract shedding. Clin Microbiol Rev. 2016;29(1):149–61.
Beauman JG. Genital herpes: a review. Am Fam Physician. 2005;72(8):1527–34.
Strick LB, Wald A, Celum C. Management of herpes simplex virus type 2 infection in HIV type 1-infected persons. Clin Infect Dis. 2006;43(3):347–56.
Cohen PR. The “knife-cut sign” revisited: a distinctive presentation of linear erosive herpes simplex virus infection in immunocompromised patients. J Clin Aesthet Dermatol. 2015;8(10):38–42.
Desai DV, Kulkarni SS. Herpes simplex virus: the interplay between HSV, host, and HIV-1. Viral Immunol. 2015;28(10):546–55.
Robboy SJ. Robboy’s pathology of the female reproductive tract. 2nd ed. Edinburgh: Churchill Livingstone/Elsevier; 2009. p. xxxviii, 1066 p.
Tangjitgamol S, Loharamtaweethong K, Thawaramara T, Chanpanitkitchot S. Vulvar pseudoepitheliomatous hyperplasia associated with herpes simplex virus type II mimicking cancer in an immunocompromised patient. J Obstet Gynaecol Res. 2014;40(1):255–8.
Groves MJ. Genital herpes: a review. Am Fam Physician. 2016;93(11):928–34.
Centers for Disease Control and Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, Division of STD Prevention. Gonorrhea. Available from: https://www.cdc.gov/std/tg2015/gonorrhea.htm.
Miller WC, Ford CA, Morris M, Handcock MS, Schmitz JL, Hobbs MM, et al. Prevalence of chlamydial and gonococcal infections among young adults in the United States. JAMA. 2004;291(18):2229–36.
Bora SA, Condous G. Bartholin’s, vulval and perineal abscesses. Best Pract Res Clin Obstet Gynaecol. 2009;23(5):661–6.
LeFevre ML, US Preventive Services Task Force. Screening for chlamydia and gonorrhea: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;161(12):902–10.
Kiviat NB, Paavonen JA, Wolner-Hanssen P, Critchlow CW, Stamm WE, Douglas J, et al. Histopathology of endocervical infection caused by Chlamydia trachomatis, herpes simplex virus, Trichomonas vaginalis, and Neisseria gonorrhoeae. Hum Pathol. 1990;21(8):831–7.
Peeling RW, Hook EW 3rd. The pathogenesis of syphilis: the Great Mimicker, revisited. J Pathol. 2006;208(2):224–32.
Radolf JD, Deka RK, Anand A, Smajs D, Norgard MV, Yang XF. Treponema pallidum, the syphilis spirochete: making a living as a stealth pathogen. Nat Rev Microbiol. 2016;14(12):744–59.
Shockman S, Buescher LS, Stone SP. Syphilis in the United States. Clin Dermatol. 2014;32(2):213–8.
Lafond RE, Lukehart SA. Biological basis for syphilis. Clin Microbiol Rev. 2006;19(1):29–49.
Carlson JA, Dabiri G, Cribier B, Sell S. The immunopathobiology of syphilis: the manifestations and course of syphilis are determined by the level of delayed-type hypersensitivity. Am J Dermatopathol. 2011;33(5):433–60.
Singh AE, Romanowski B. Syphilis: review with emphasis on clinical, epidemiologic, and some biologic features. Clin Microbiol Rev. 1999;12(2):187–209.
Baughn RE, Musher DM. Secondary syphilitic lesions. Clin Microbiol Rev. 2005;18(1):205–16.
Balagula Y, Mattei PL, Wisco OJ, Erdag G, Chien AL. The great imitator revisited: the spectrum of atypical cutaneous manifestations of secondary syphilis. Int J Dermatol. 2014;53(12):1434–41.
Cid PM, Cudos ES, Zamora Vargas FX, Merino MJ, Pinto PH. Pathologically confirmed malignant syphilis using immunohistochemical staining: report of 3 cases and review of the literature. Sex Transm Dis. 2014;41(2):94–7.
Requena CB, Orasmo CR, Ocanha JP, Barraviera SR, Marques ME, Marques SA. Malignant syphilis in an immunocompetent female patient. An Bras Dermatol. 2014;89(6):970–2.
Bittencourt Mde J, Brito AC, Nascimento BA, Carvalho AH, Drago MG. Nodular tertiary syphilis in an immunocompetent patient. An Bras Dermatol. 2016;91(4):528–30.
Rocha N, Horta M, Sanches M, Lima O, Massa A. Syphilitic gumma—cutaneous tertiary syphilis. J Eur Acad Dermatol Venereol. 2004;18(4):517–8.
Karp G, Schlaeffer F, Jotkowitz A, Riesenberg K. Syphilis and HIV co-infection. Eur J Intern Med. 2009;20(1):9–13.
Stevenson J, Heath M. Syphilis and HIV infection: an update. Dermatol Clin. 2006;24(4):497–507, vi.
Tobian AA, Quinn TC. Herpes simplex virus type 2 and syphilis infections with HIV: an evolving synergy in transmission and prevention. Curr Opin HIV AIDS. 2009;4(4):294–9.
Zetola NM, Klausner JD. Syphilis and HIV infection: an update. Clin Infect Dis. 2007;44(9):1222–8.
Engelkens HJ, ten Kate FJ, Vuzevski VD, van der Sluis JJ, Stolz E. Primary and secondary syphilis: a histopathological study. Int J STD AIDS. 1991;2(4):280–4.
Abell E, Marks R, Jones EW. Secondary syphilis: a clinico-pathological review. Br J Dermatol. 1975;93(1):53–61.
Flamm A, Parikh K, Xie Q, Kwon EJ, Elston DM. Histologic features of secondary syphilis: a multicenter retrospective review. J Am Acad Dermatol. 2015;73(6):1025–30.
Brown L. Pathology of the vulva and vagina. London: Springer, 2013. Available from: SpringerLink. Restricted to UC campuses https://doi.org/10.1007/978-0-85729-757-0.
Pandhi RK, Singh N, Ramam M. Secondary syphilis: a clinicopathologic study. Int J Dermatol. 1995;34(4):240–3.
Buffet M, Grange PA, Gerhardt P, Carlotti A, Calvez V, Bianchi A, et al. Diagnosing Treponema pallidum in secondary syphilis by PCR and immunohistochemistry. J Invest Dermatol. 2007;127(10):2345–50.
Grange PA, Gressier L, Dion PL, Farhi D, Benhaddou N, Gerhardt P, et al. Evaluation of a PCR test for detection of treponema pallidum in swabs and blood. J Clin Microbiol. 2012;50(3):546–52.
Centers for Disease Control and Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, Division of STD Prevention. Syphilis. Available from: https://www.cdc.gov/std/syphilis/default.htm.
Blaustein A, Kurman RJ, Ronnett BM. Blaustein’s pathology of the female genital tract. 6th ed. New York: Springer; 2011. 1246 p.
Centers for Disease Control and Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, Division of STD Prevention. Chancroid. Available from: https://www.cdc.gov/std/tg2015/chancroid.htm.
Sternberg SS, Mills SE, Carter D. Sternberg’s diagnostic surgical pathology, 2 vol., 5th ed. Philadelphia, PA: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2010 (xv, 418 pages, 83 unnumbered pages).
Weedon D, Strutton G, Rubin AI, Weedon D. Weedon’s skin pathology. 3rd ed. Oxford: Churchill Livingstone; 2010. 1041 p.
Joseph AK, Rosen T. Laboratory techniques used in the diagnosis of chancroid, granuloma inguinale, and lymphogranuloma venereum. Dermatol Clin. 1994;12(1):1–8.
Romero L, Huerfano C, Grillo-Ardila CF. Macrolides for treatment of Haemophilus ducreyi infection in sexually active adults. Cochrane Database Syst Rev. 2017;12:CD012492.
Centers for Disease Control and Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, Division of STD Prevention Donovanosis. Available from: https://www.cdc.gov/std/tg2015/donovanosis.htm.
O’Farrell N, Moi H. 2016 European guideline on donovanosis. Int J STD AIDS. 2016;27(8):605–7.
Centers for Disease Control and Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, Division of STD Prevention LGV. Available from: https://www.cdc.gov/std/tg2015/lgv.htm.
Isaksson J, Carlsson O, Airell A, Stromdahl S, Bratt G, Herrmann B. Lymphogranuloma venereum rates increased and Chlamydia trachomatis genotypes changed among men who have sex with men in Sweden 2004–2016. J Med Microbiol. 2017;66(11):1684–7.
Peuchant O, Touati A, Sperandio C, Henin N, Laurier-Nadalie C, Bebear C, et al. Changing pattern of Chlamydia trachomatis strains in lymphogranuloma venereum outbreak, France, 2010–2015. Emerg Infect Dis. 2016;22(11):1945–7.
Scieux C, Barnes R, Bianchi A, Casin I, Morel P, Perol Y. Lymphogranuloma venereum: 27 cases in Paris. J Infect Dis. 1989;160(4):662–8.
Collins L, White JA, Bradbeer C. Lymphogranuloma venereum. BMJ. 2006;332(7533):66.
Centers for Disease Control and Prevention. Recommendations for the laboratory-based detection of Chlamydia trachomatis and Neisseria gonorrhoeae—2014. MMWR Recomm Rep. 2014;63(RR-02):1–19.
Centers for Disease Control and Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, Division of STD Prevention. Chlamydia. Available from: https://www.cdc.gov/std/tg2015/chlamydia.htm.
Faro S. Chlamydia trachomatis infection in women. J Reprod Med. 1985;30(3 Suppl):273–8.
Haggerty CL, Gottlieb SL, Taylor BD, Low N, Xu F, Ness RB. Risk of sequelae after Chlamydia trachomatis genital infection in women. J Infect Dis. 2010;201(Suppl 2):S134–55.
O’Connell CM, Ferone ME. Chlamydia trachomatis genital infections. Microb Cell. 2016;3(9):390–403.
Edwards JM, Campbell AR, Tait A, Lusher M. Demonstration of Chlamydia trachomatis in colposcopic cervical biopsy specimens by an immunoperoxidase method. J Clin Pathol. 1991;44(12):1027–9.
Centers for Disease Control and Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, Division of STD Prevention. Warts. Available from: https://www.cdc.gov/std/tg2015/warts.htm.
Kurman RJ, International Agency for Research on Cancer, World Health Organization. WHO classification of tumours of female reproductive organs. 4th ed. Lyon: International Agency for Research on Cancer; 2014. 307 p.
Clavero O, McCloskey J, Molina VM, Quiros B, Bravo IG, de Sanjose S, et al. Squamous intraepithelial lesions of the anal squamocolumnar junction: histopathological classification and HPV genotyping. Papillomavirus Res. 2017;3:11–7.
Roberts JM, Cornall AM, Ekman D, Law C, Poynten IM, Jin F, et al. Papillary immature metaplasia of the anal canal: a low-grade lesion that can mimic a high-grade lesion. Am J Surg Pathol. 2016;40(3):348–53.
Anderson J, Clark RA, Watts DH, Till M, Arrastia C, Schuman P, et al. Idiopathic genital ulcers in women infected with human immunodeficiency virus. J Acquir Immune Defic Syndr Hum Retrovirol. 1996;13(4):343–7.
Burgener A, McGowan I, Klatt NR. HIV and mucosal barrier interactions: consequences for transmission and pathogenesis. Curr Opin Immunol. 2015;36:22–30.
Farcasanu M, Kwon DS. The influence of cervicovaginal microbiota on mucosal immunity and prophylaxis in the Battle against HIV. Curr HIV/AIDS Rep. 2018;15(1):30–8.
Nazli A, Chan O, Dobson-Belaire WN, Ouellet M, Tremblay MJ, Gray-Owen SD, et al. Exposure to HIV-1 directly impairs mucosal epithelial barrier integrity allowing microbial translocation. PLoS Pathog. 2010;6(4):e1000852.
Peters BM, Yano J, Noverr MC, Fidel PL Jr. Candida vaginitis: when opportunism knocks, the host responds. PLoS Pathog. 2014;10(4):e1003965.
Sobel JD. Vaginitis. N Engl J Med. 1997;337(26):1896–903.
Sobel JD. Vulvovaginal candidosis. Lancet. 2007;369(9577):1961–71.
Foxman B. The epidemiology of vulvovaginal candidiasis: risk factors. Am J Public Health. 1990;80(3):329–31.
Hoffmann JN, You HM, Hedberg EC, Jordan JA, McClintock MK. Prevalence of bacterial vaginosis and Candida among postmenopausal women in the United States. J Gerontol B Psychol Sci Soc Sci. 2014;69(Suppl 2):S205–14.
Mendling W, Friese K, Mylonas I, Weissenbacher ER, Brasch J, Schaller M, et al. Vulvovaginal Candidosis (excluding chronic mucocutaneous candidosis). Guideline of the German Society of Gynecology and Obstetrics (AWMF registry no. 015/072, S2k level, December 2013). Geburtshilfe Frauenheilkd. 2015;75(4):342–54.
Blostein F, Levin-Sparenberg E, Wagner J, Foxman B. Recurrent vulvovaginal candidiasis. Ann Epidemiol. 2017;27(9):575–82, e3.
Foster KW, Ghannoum MA, Elewski BE. Epidemiologic surveillance of cutaneous fungal infection in the United States from 1999 to 2002. J Am Acad Dermatol. 2004;50(5):748–52.
Ely JW, Rosenfeld S, Seabury Stone M. Diagnosis and management of tinea infections. Am Fam Physician. 2014;90(10):702–10.
Otero L, Palacio V, Vazquez F. Tinea cruris in female prostitutes. Mycopathologia. 2002;153(1):29–31.
Chang SE, Lee DK, Choi JH, Moon KC, Koh JK. Majocchi’s granuloma of the vulva caused by Trichophyton mentagrophytes. Mycoses. 2005;48(6):382–4.
Luchsinger I, Bosshard PP, Kasper RS, Reinhardt D, Lautenschlager S. Tinea genitalis: a new entity of sexually transmitted infection? Case series and review of the literature. Sex Transm Infect. 2015;91(7):493–6.
Sand FL, Thomsen SF. Skin diseases of the vulva: infectious diseases. J Obstet Gynaecol. 2017;37(7):840–8.
Koumans EH, Sternberg M, Bruce C, McQuillan G, Kendrick J, Sutton M, et al. The prevalence of bacterial vaginosis in the United States, 2001–2004; associations with symptoms, sexual behaviors, and reproductive health. Sex Transm Dis. 2007;34(11):864–9.
Malaguti N, Bahls LD, Uchimura NS, Gimenes F, Consolaro ME. Sensitive detection of thirteen bacterial vaginosis-associated agents using multiplex polymerase chain reaction. Biomed Res Int. 2015;2015:645853.
Schwebke JR, Muzny CA, Josey WE. Role of Gardnerella vaginalis in the pathogenesis of bacterial vaginosis: a conceptual model. J Infect Dis. 2014;210(3):338–43.
Kenyon C, Colebunders R, Crucitti T. The global epidemiology of bacterial vaginosis: a systematic review. Am J Obstet Gynecol. 2013;209(6):505–23.
Eade CR, Diaz C, Chen S, Cole AL, Cole AM. HIV-enhancing factors are secreted by reproductive epithelia upon inoculation with bacterial vaginosis-associated bacteria. Protein Pept Lett. 2015;22(8):672–80.
Mitchell C, Marrazzo J. Bacterial vaginosis and the cervicovaginal immune response. Am J Reprod Immunol. 2014;71(6):555–63.
Fredricks DN, Fiedler TL, Thomas KK, Oakley BB, Marrazzo JM. Targeted PCR for detection of vaginal bacteria associated with bacterial vaginosis. J Clin Microbiol. 2007;45(10):3270–6.
Bakardzhiev I, Chokoeva A, Tchernev G, Wollina U, Lotti T. Tinea profunda of the genital area. Successful treatment of a rare skin disease. Dermatol Ther. 2016;29(3):181–3.
Ramsey ML. Pseudomonas folliculitis associated with use of hot tubs and spas. Phys Sportsmed. 1989;17(5):150–62.
Zisova LG, Dobrev HP, Tchernev G, Semkova K, Aliman AA, Chorleva KI, et al. Tinea atypica: report of nine cases. Wien Med Wochenschr. 2013;163(23–24):549–55.
Bhide A, Nama V, Patel S, Kalu E. Microbiology of cysts/abscesses of Bartholin’s gland: review of empirical antibiotic therapy against microbial culture. J Obstet Gynaecol. 2010;30(7):701–3.
Cabrera H, Skoczdopole L, Marini M, Della Giovanna P, Saponaro A, Echeverria C. Necrotizing gangrene of the genitalia and perineum. Int J Dermatol. 2002;41(12):847–51.
Kilpatrick CC, Alagkiozidis I, Orejuela FJ, Chohan L, Hollier LM. Factors complicating surgical management of the vulvar abscess. J Reprod Med. 2010;55(3–4):139–42.
Kim TH, Seap B, Kim SA, Heo GE. Vulvar abscess caused by methicillin-resistant Staphylococcus aureus (MRSA) in a postmenopausal woman. J Menopausal Med. 2016;22(2):118–21.
Thurman AR, Satterfield TM, Soper DE. Methicillin-resistant Staphylococcus aureus as a common cause of vulvar abscesses. Obstet Gynecol. 2008;112(3):538–44.
Wood SC. Clinical manifestations and therapeutic management of vulvar cellulitis and abscess: methicillin-resistant Staphylococcus aureus, necrotizing fasciitis, Bartholin abscess, Crohn disease of the vulva, hidradenitis suppurativa. Clin Obstet Gynecol. 2015;58(3):503–11.
Dave AJ, Sethi A, Morrone A. Female genital mutilation: what every American dermatologist needs to know. Dermatol Clin. 2011;29(1):103–9.
Koussidis GA. Gynecologic rarities: a case of periclitoral abscess and review of the literature. Am J Obstet Gynecol. 2012;207(5):e3–5.
Rouzi AA. Epidermal clitoral inclusion cysts: not a rare complication of female genital mutilation. Hum Reprod. 2010;25(7):1672–4.
Gupta M, Saini V, Poddar A, Kumari S, Maitra A. Acquired clitoromegaly: a gynaecological problem or an obstetric complication? J Clin Diagn Res. 2016;10(12):QD10–1.
Markle W, Conti T, Kad M. Sexually transmitted diseases. Prim Care. 2013;40(3):557–87.
Ko CJ, Elston DM. Pediculosis. J Am Acad Dermatol. 2004;50(1):1–12; quiz 3–4.
Sangare AK, Doumbo OK, Raoult D. Management and treatment of human lice. Biomed Res Int. 2016;2016:8962685.
Chosidow O. Scabies and pediculosis. Lancet. 2000;355(9206):819–26.
Stamm AW, Kobashi KC, Stefanovic KB. Urologic dermatology: a review. Curr Urol Rep. 2017;18(8):62.
Bakos L, Reusch MC, D’Elia P, Aquino V, Bakos RM. Crusted scabies of the vulva. J Eur Acad Dermatol Venereol. 2007;21(5):682–4.
Hall LD, Eminger LA, Hesterman KS, Heymann WR. Epstein-Barr virus: dermatologic associations and implications: part I Mucocutaneous manifestations of Epstein-Barr virus and nonmalignant disorders. J Am Acad Dermatol. 2015;72(1):1–19; quiz 19−20.
Halvorsen JA, Brevig T, Aas T, Skar AG, Slevolden EM, Moi H. Genital ulcers as initial manifestation of Epstein-Barr virus infection: two new cases and a review of the literature. Acta Derm Venereol. 2006;86(5):439–42.
Haidari G, MacMahon E, Tong CY, White JA. Genital ulcers: it is not always simplex. Int J STD AIDS. 2015;26(1):72–3.
Griffiths P, Baraniak I, Reeves M. The pathogenesis of human cytomegalovirus. J Pathol. 2015;235(2):288–97.
McGalie CE, McBride HA, McCluggage WG. Cytomegalovirus infection of the cervix: morphological observations in five cases of a possibly under-recognised condition. J Clin Pathol. 2004;57(7):691–4.
Slyker J, Farquhar C, Atkinson C, Asbjornsdottir K, Roxby A, Drake A, et al. Compartmentalized cytomegalovirus replication and transmission in the setting of maternal HIV-1 infection. Clin Infect Dis. 2014;58(4):564–72.
Abou M, Dällenbach P. Acute cervicitis and vulvovaginitis may be associated with Cytomegalovirus. BMJ Case Rep. 2013;2013:bcr2013008884. https://doi.org/10.1136/bcr-2013-008884.
Choi YL, Kim JA, Jang KT, Kim DS, Kim WS, Lee JH, et al. Characteristics of cutaneous cytomegalovirus infection in non-acquired immune deficiency syndrome, immunocompromised patients. Br J Dermatol. 2006;155(5):977–82.
Centers for Disease Control and Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, Division of STD Prevention. Schistosomiasis. Available from: https://www.cdc.gov/parasites/schistosomiasis/index.html.
Christinet V, Lazdins-Helds JK, Stothard JR, Reinhard-Rupp J. Female genital schistosomiasis (FGS): from case reports to a call for concerted action against this neglected gynaecological disease. Int J Parasitol. 2016;46(7):395–404.
Richens J. Genital manifestations of tropical diseases. Sex Transm Infect. 2004;80(1):12–7.
Ricosse JH, Emeric R, Courbil LJ. [Anatomopathological aspects of schistosomiasis. A study of 286 pathological specimens (author’s transl)]. Med Trop (Mars). 1980;40(1):77–94.
Hegertun IE, Sulheim Gundersen KM, Kleppa E, Zulu SG, Gundersen SG, Taylor M, et al. S. haematobium as a common cause of genital morbidity in girls: a cross-sectional study of children in South Africa. PLoS Negl Trop Dis. 2013;7(3):e2104.
Kjetland EF, Ndhlovu PD, Mduluza T, Gomo E, Gwanzura L, Mason PR, et al. Simple clinical manifestations of genital Schistosoma haematobium infection in rural Zimbabwean women. Am J Trop Med Hyg. 2005;72(3):311–9.
Kleppa E, Klinge KF, Galaphaththi-Arachchige HN, Holmen SD, Lillebo K, Onsrud M, et al. Schistosoma haematobium infection and CD4+ T-cell levels: a cross-sectional study of young South African women. PLoS One. 2015;10(3):e0119326.
Poggensee G, Kiwelu I, Weger V, Goppner D, Diedrich T, Krantz I, et al. Female genital schistosomiasis of the lower genital tract: prevalence and disease-associated morbidity in northern Tanzania. J Infect Dis. 2000;181(3):1210–3.
John AR, Canaday DH. Herpes zoster in the older adult. Infect Dis Clin N Am. 2017;31(4):811–26.
Warren-Gash C, Forbes H, Breuer J. Varicella and herpes zoster vaccine development: lessons learned. Expert Rev Vaccines. 2017;16(12):1191–201.
Brown D. Herpes zoster of the vulva. Clin Obstet Gynecol. 1972;15(4):1010–4.
Philip KE, Goodman A, Pallawela SN, Sathia L, Webster DP. A not so simplex case of genital herpes. BMJ Case Rep. 2013;2013:bcr2013009993. https://doi.org/10.1136/bcr-2013-009993.
Cymerman RM, Kaplan Hoffmann R, Rouhani Schaffer P, Pomeranz MK. Vulvar infections: beyond sexually transmitted infections. Int J Dermatol. 2017;56(4):361–9.
Fishman A, Ortega E, Girtanner RE, Kaplan AL. Malacoplakia of the vagina presenting as a pelvic mass. Gynecol Oncol. 1993;49(3):380–2.
Chalvardjian A, Picard L, Shaw R, Davey R, Cairns JD. Malacoplakia of the female genital tract. Am J Obstet Gynecol. 1980;138(4):391–4.
Bhaijee F, Sebastian S, Lewin J. Vaginal malakoplakia: a benign mimic of pelvic malignancy in a postmenopausal female. Am J Clin Pathol. 2015;140:A171.
Yousef GM, Naghibi B, Hamodat MM. Malakoplakia outside the urinary tract. Arch Pathol Lab Med. 2007;131(2):297–300.
Yong M, Parkinson K, Goenka N, O’Mahony C. Diabetes and genital warts: an unhappy coalition. Int J STD AIDS. 2010;21(7):457–9.
Radja N, Lau R. Extensive genital warts associated with HTLV-I infection. Int J STD AIDS. 2004;15(3):202–3.
Gormley RH, Kovarik CL. Human papillomavirus-related genital disease in the immunocompromised host: part I. J Am Acad Dermatol. 2012;66(6):867.e1–14; quiz 81–2.
Werner RN, Westfechtel L, Dressler C, Nast A. Anogenital warts and other HPV-associated anogenital lesions in the HIV-positive patient: a systematic review and meta-analysis of the efficacy and safety of interventions assessed in controlled clinical trials. Sex Transm Infect. 2017;93(8):543–50.
Centers for Disease Control and Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, Division of STD Prevention. Available from: https://www.cdc.gov/tb/publications/guidelines/default.htm.
Centers for Disease Control and Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, Division of STD Prevention. Bartonella. Available from: https://www.cdc.gov/bartonella/clinicians/index.html.
Long SR, Whitfeld MJ, Eades C, Koehler JE, Korn AP, Zaloudek CJ. Bacillary angiomatosis of the cervix and vulva in a patient with AIDS. Obstet Gynecol. 1996;88(4 Pt 2):709–11.
Ramdial PK, Sing Y, Ramburan A, Dlova NC, Bagratee JS, Calonje E. Bartonella quintana-induced vulval bacillary angiomatosis. Int J Gynecol Pathol. 2012;31(4):390–4.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Science Press & Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Zare, S.Y., Leivo, M.Z., Chen, H., Walavalkar, V. (2019). Infectious Disorders of the Lower Genital Tract. In: Zheng, W., Fadare, O., Quick, C., Shen, D., Guo, D. (eds) Gynecologic and Obstetric Pathology, Volume 1. Springer, Singapore. https://doi.org/10.1007/978-981-13-3016-2_3
Download citation
DOI: https://doi.org/10.1007/978-981-13-3016-2_3
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-13-3015-5
Online ISBN: 978-981-13-3016-2
eBook Packages: MedicineMedicine (R0)